
Abstract
Introduction:
The debate remains open as to the difference in prevalence of mortality and occurrence of acute events in patients with Myocardial infarction with non-obstructive coronary arteries (MINOCA) and others with Myocardial infarction with coronary arteries disease (MI-CAD).
Methods:
We conducted a 2-year retrospective study for patients admitted for Acute coronary syndrome (ACS) to analyze the clinical and prognostic characteristics of patients with MINOCA versus MI-CAD. We defined 1-year all-cause mortality as the primary outcome, and the secondary outcome as a composite of 1-year readmission for myocardial infarction or acute heart failure (AHF).
Results:
Our study included 1077 patients, 95.3% with MI-CAD and 4.7% with MINOCA. At admission, 71.1% patient were diagnosed STEMI and 28.9% with NSTEMI. The difference between the 2 groups was found on age (P < .001), hypertension, diabetes with consecutive P-values of .007 and .001, as well as Ejection fraction (P < .001). For the outcomes studied, the difference was significant between the 2 groups for all events, and MINOCA patients had a better prognosis than MI-CAD patients, with adjusted hazard ratios (HR) for 1-year mortality (HR = 0.601 P = .004), for readmission for ACS (HR = 0.662; P = .002) and for readmission for AHF (HR = 0.539; P = .019).
Conclusion:
Despite the ambiguity in the genesis of MINOCA, the short- and long-term prognosis of these patients remains generally favorable.
Introduction
Myocardial infarction (MI) is pathologically described as myocardial cell death caused by persistent ischemia. As early as 10 to 15 minutes after the onset of ischemia, the first ultrastructural alterations can be seen, including depletion of cellular glycogen, relaxed myofibrils and disruption of the sarcolemma, 1 and using electron microscopy, mitochondrial abnormalities can be observed as early as 10 minutes after coronary occlusion, and are progressive. 2
Based on histological, clinical, prognostic and treatment-related characteristics, MI can be divided into 2 types 3 : Myocardial infarction with coronary arteries disease (MI-CAD), which is defined as a myocardial infarction with significant hemodynamic obstruction of 1 or more coronary arteries (>50%), 4 and the Myocardial infarction with non-obstructive coronary arteries (MINOCA) is a disease with several causes that is characterized by clinical evidence of MI and angiographically normal or minimally obstructive coronary arteries (<50% stenosis),5-8 and 10% of acute coronary syndrome (ACS) are caused by MINOCA. 9 In this work, we carried out an analysis of the clinical and prognostic characteristics of MINOCA versus MI-CAD.
Materials and Methods
Rationale and design of the study
A significant proportion of patients admitted with ACS with or without persistant ST-segment elevation have no significant coronary artery stenosis to explain the symptomatology, in which case we speak of myocardial infarction with no obstructive coronary artery (MINOCA). This is a recent entity and is still the subject of debate concerning the etiological work-up, in which cardiac MRI plays a pivotal role in recognizing the mechanism of ischemia, assessing the necrosis extent, and thus eliminating differential diagnoses such as myocarditis.10,11 In addition, the short- and long-term prognosis of these patients is still a research topic.
To this end, we conducted a 2-year monocentric retrospective study in our cardiac intensive care unit (CICU) for patients admitted for ACS to analyze the clinical and prognostic characteristics of patients with MINOCA versus MI-CAD.
Study population and data collection
We included all patients admitted for ACS with or without ST-segment elevation and in who coronary angiography had been performed. We defined an ACS as a patient who presented with chest pain with presumed new ECG electrical changes, associated with positive troponin levels changes. We excluded patients who died before coronary angiography was performed, as well as patients who refused coronary angiography, and patients with myocarditis at cardiac Magnetic Resonance Imaging (MRI; Figure 1).

Flow diagram for study participations.
All demographic, clinical, echocardiographic, angiographic data, as well as intra-hospital evolution and the evolution during the follow-up were obtained from patients’ electronic medical records.
Definition
We defined STEMI according to an association of chest pain presumed to be of coronary origin, with persistent ST-segment elevation or equivalent, and troponin elevation above 99 percentiles with coronary angiography occlusion or significant stenosis (>70% for coronary arteries and 50% for the left main).12,13
We defined NSTEMI as the association of chest pain of presumed coronary origin associated with dynamic ST-segment changes, and troponin elevation above 99 percentiles with significant coronary artery occlusion or stenosis (>70% for coronary arteries and 50% for the left main). 14
We defined MINOCA as the association of chest pain presumed to be of coronary origin and troponin elevation above the 99th percentile with the absence of significant stenosis on coronary angiography, excluding myocarditis or tako-tsubo cardiomyopathy.15,16
We defined AHF as any clinical presentation suggestive of left ventricular failure secondary to acute elevation of left ventricular filling pressures due to impaired systolic or diastolic function. 17
Outcomes study
We defined 1-year all-cause mortality as the primary outcome, and the secondary outcome as a composite of 1-year readmission for ACS or acute heart failure (AHF).
Statistical analysis
The categorical variables were reported as numbers and percentages, then Pearson’s chi-square test or Fisher’s exact test were used for comparison between the different groups. For continuous variables, normality was first analyzed using the Shapiro-Wilk test, then the variables were reported as mean and standard deviation (SD) or median and interquartile range and compared using the t-student test or non-parametric tests depending on whether or not the distribution was normal.
The primary and secondary outcomes was studied using a Cox proportional hazards regression model to estimate hazard ratios (HRs) and 95% confidence intervals (CIs), adjusting for variables described in the literature. Kaplan-Meier analysis was used to compare mortality rates and readmission for ACS or AHF between the different groups, with significance between groups being assessed by the log-rank test (Mantel-Cox). All P-values were calculated using 2-sided tests, and P-values less than .05 were considered statistically significant. All statistical analyses were performed using IBM SPSS version 26 (SPSS, Inc., Chicago, IL).
Ethical approval
This study did not require formal ethics approval. Access to patient data was authorized by the Mohammed VI University Hospital and approved by the head of department, given the retrospective design of this study. The requirement for patient consent was waived. Data anonymity was respected in accordance with national and international guidelines.
Results
(A) General characteristics (Table 1)
Our study included 1077 patients, 95.3% with MI-CAD (1025 patients) and 4.7% with MINOCA (52 patients). Males predominated between the 2 groups, with a total percentage of 74.7%. The MINOCA group was significantly younger, with a mean age of 53.15
Showing the general characteristics of patients according to MINOCA or MI-CAD.

The mean time from onset of symptoms to presentation was 12.34 hours, with no difference between the 2 groups. On admission, 1.9% had a systolic blood pressure (SBP)<90 mmHg, and 9.7% of patients had clinical signs of heart failure with a KILLIP class > II. For the admission diagnosis, 71.1% were considered STEMI and 28.9% NSTEMI. In the MINOCA group, 77% patients were considered STEMI and 23% patients NSTEMI.
On electrocardiography, persistent ST-segment elevation was found in 73.9%, ST-segment depression in 49.4%, and ST-segment elevation in AVR in 5.9%, with no difference between the 2 groups.
The mean ejection fraction calculated by trans-thoracic echocardiography was 47% in MINOCA and 53% in MI-CAD (P < .001). For left ventricular diastolic function, there was no difference between the 2 groups, and the same was observed for right ventricular systolic function.
In the MI-CAD group, the most frequent culprit artery was LAD (60.8%), followed by RCA (22%), LCX (15.4%) and LM (1.8%). Flow was restored in 525 patients, but 217 patients had TIMI 0 or TIMI I flow. Of these patients, PCI was performed in 742, surgery in 217, a conservative strategy in 66 and a pharmaco-invasive strategy in 245.
In the biological work-up, anemia (Hb < 10 g/dl) was found in 21.4%, inflammation with CRP>300mg/ml in 2.5%, with no significant difference for either parameter. However, acute kidney disease with (GFR < 30 ml/min/1.73 m2 and white blood cell count >12 000/mm3) were different between the 2 groups.
As for the outcome during hospitalization, 8.1% had presented acute heart failure, 5.7% a threatening arrhythmia, 7.4% a threatening conduction disorder, 1.2% a mechanical complication, 3.2% cardiogenic shock, and finally 1.7% had died during hospitalization, with no significant difference between the 2 groups for any of these events.
(B) Outcomes study (Table 2)
For the primary outcome, 47 events were observed with a total percentage of 4.4%: 46 (4.6%) events in the MI-CAD group and 1 (0.1%) event in the MINOCA group (P < .001). The Kaplein Meier survival analysis showed a significant difference between the 2 groups, with a log-rank test P-value of .023 (Figure 2).
Shows the difference between the 2 groups for primary and secondary outcomes endpoints.


Kaplan-Meier curve for all-cause mortality at 1 years according to MINOCA or MI-CAD.
For secondary outcomes, firstly, for readmission for ACS, 55 events were observed, that is, 5.1%: 54 events in the MI-CAD group (5%) and 1 event in the MINOCA group (0.1%) (P = .002), and for readmission for acute heart failure, 28 events were observed, that is, 2.6%: 27 events in the MI-CAD group (2.5%) and 1 event in the MINOCA group (0.1%) (P = .042). For the 2 secondary outcomes, the kaplein Meier analysis objective a significant difference between the 2 groups with consecutive log-rank test P-values of .033 and .035 (Figures 3 and 4).
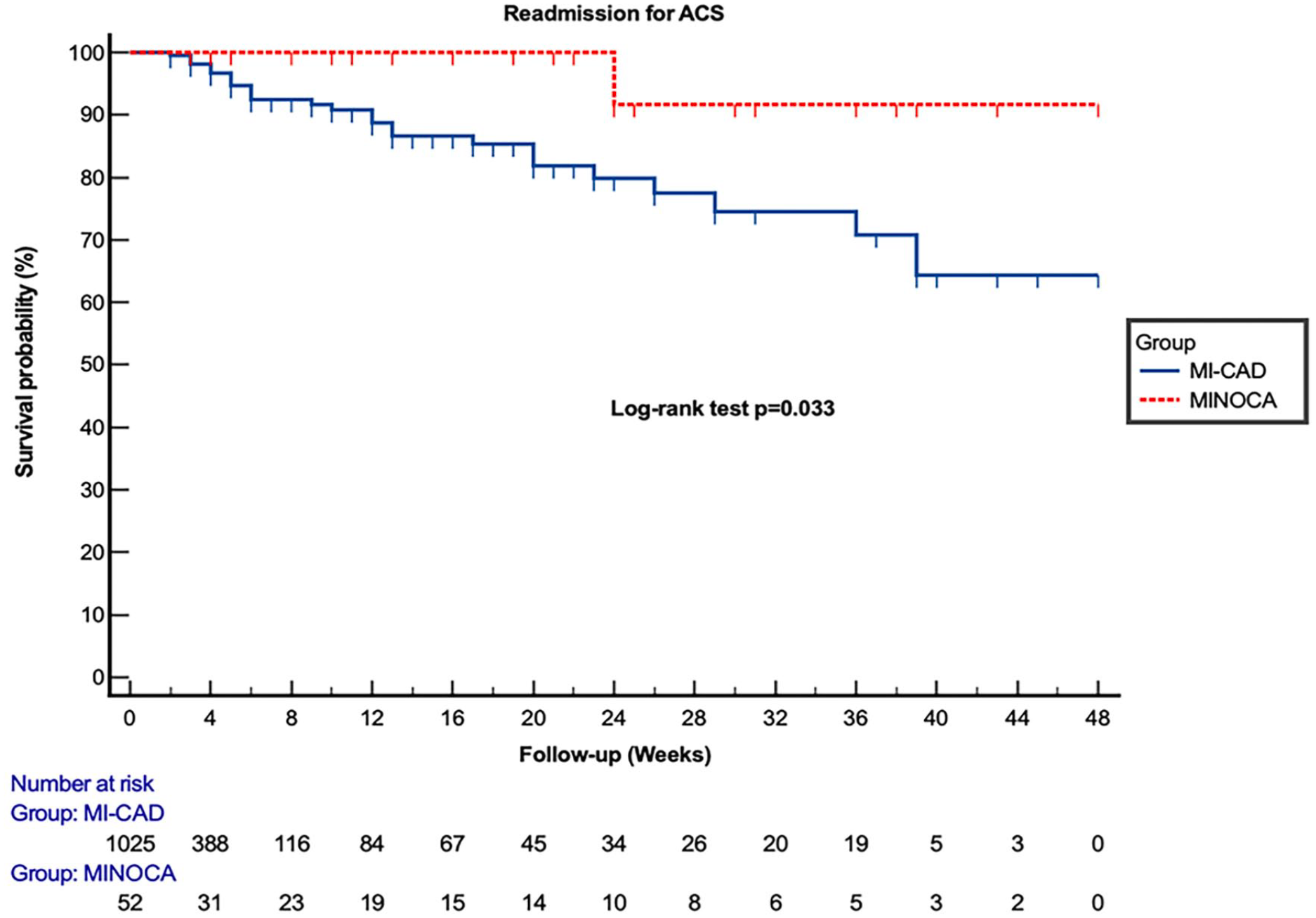
Kaplan-Meier curve for readmission for myocardial infarction at 1 years as a function of MINOCA or MI-CAD.
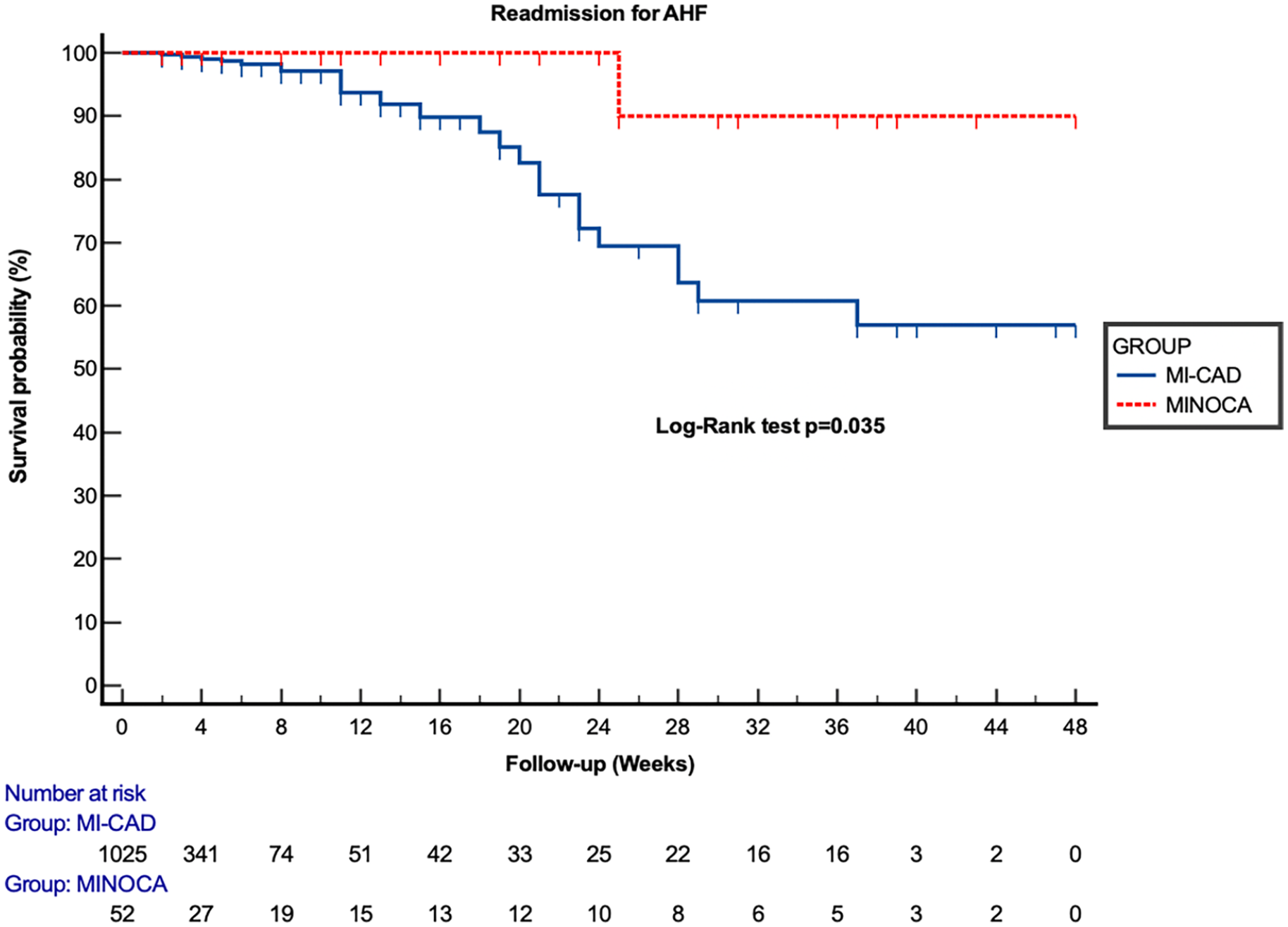
Kaplan-Meier curve for readmission for Acute heart failure at 1 years as a function of MINOCA or MI-CAD.
Multivariable analysis (Table 3)
Using Cox proportional hazards analysis, we found, firstly before adjustment, that patients in the MINOCA group had a better prognosis than the MI-CAD group, for all-cause 1-year mortality (HR = 0. 442; 95% CI 0.227-0.760; P = .041), a lower risk of readmission for ACS (HR = 0.297; 95% CI 0.316-0.821; P = .034), as well as for readmission for AHF (HR = 0.555; 95% CI 0.329-0.836; P = .045).
Cox proportional hazards analysis for the different outcomes studied for the MINOCA group versus MI-CAD before and after adjustment for (Age, arterial hypertension, diabetes, active smoking, EF < 40%, proximal LAD or LM as culprit artery, TIMI 0-I flow, CRP >300 mg and KILLIP > I at admission).

After adjustment for age, arterial hypertension, diabetes, active smoking, EF < 40%, proximal LAD or LM as culprit artery, TIMI 0-I flow, CRP >300mg and KILLIP > 1 at admission, the results remained significantly in favor of a better prognosis for MINOCA: (HR = 0. 601; 95% CI 0.281-0.853; P = .004) for 1-year all-cause mortality, (HR = 0.662; 95% CI 0.398-0.809; P = .002) for readmission for ACS and finally (HR = 0.713; 95% CI 0.539-0.902; P = .019) for readmission for AHF.
Discussion
The debate remains open as to the difference in prevalence of mortality and occurrence of acute events in patients with MINOCA and others with MI-CAD.18,19
In a meta-analysis of 28 publications on this topic was published in 2015 by Pasupathy et al showed that the prevalence of MINOCA was 6%, with a median age of 55 years, and that 40% of them were women. Compared with MI-CAD. patients, MINOCA patients were more often young and female, and less often had dyslipidemia. However, other cardiovascular risk factors were similar between the 2 groups. After 12 months, the all-cause mortality rate was lower in the MINOCA group (4.7%, 95% CI, 2.6%-6.9%) than in the MI-CADgroup (6.7%, 95% CI, 4.3%-9.0%). 20
In addition, as part of The ACUITY trial, Planer et al carried-out Propensity-Matched Analysis on 2422 patients diagnosed with SCA, of whom 2245 (91.9%) were with MI-CAD and 197 (8.1%) with MINOCA. For 1-month mortality, there was no difference between the 2 groups for all-cause mortality, but there was more recurrent myocardial infarction in the MI-CAD group (HR = 0.11 95% CI: 0.02, 0.82; P = .03). At 1 year, and paradoxically, overall mortality was significantly higher in the MINOCA group (5.2% vs 1.6%), with (HR = 3.44 95% CI: 1.05, 11.28 ; P = .04). Conversely, rates of recurrent myocardial infarction were significantly higher in patients with obstructive coronary artery disease (HR = 0.35 95% CI: 0.12, 0.98; P = .04). 21
In a large meta-analysis that included 36 932 patients after the selection of 44 studies, with at least a follow-up duration of more than 6months of patients with ACS. The duration of the study observation period was approximately 25 months, during which 1409 patients (3.8%) died, with an overall annual mortality rate of 2.0% (95% confidence interval [CI]: 1.5% to 2.4%), with significant heterogeneity (I2 = 80%, P < .001). After analyzing 26 of the selected studies that compared MINOCA patients with those suffering from myocardial infarction and obstructive coronary disease, they concluded that annual long-term total mortality rates were 2.2% for MINOCA patients and 5.0% for patients with obstructive coronary disease, with a significant difference (relative risk: 0.60, 95% CI: 0.46-0.78, P < .001). In addition, a meta-regression analysis showed that long-term mortality correlated directly with beta-blocker use during the follow-up period and the presence of ST-segment depression on the admission electrocardiogram, and inversely with normal ejection fraction and normal coronary arteries on angiography. 22
With the same objective of our study, Dreyer et al analyzed patients with MINOCA from the National Cardiovascular Data Registry (NCDRVR) CathPCI Registry, and among a total of 276 522 patients admitted for ACS 16 849 (5.9%) had MINOCA. The primary endpoint was major adverse cardiac events (MACE) defined as all-cause mortality, re-hospitalization for acute myocardial infarction (AMI), heart failure (HF) or stroke 12 months after AMI, and secondary endpoints included 12-month MACE components. Results showed that 12-month MACE rates (18.7% vs 27.6%) were significantly lower for MINOCA patients than for MI-CAD patients (P < .001). For the secondary endpoints, the rates of mortality (12.3% vs 16.7%), re-hospitalization for HF (5.9% vs 9.3%) and re-hospitalization for AMI (1.3% vs 6.1%), were always significantly lower for MINOCA versus MI-CAD. patients (P < .001). In multivariate analysis and after risk adjustment, MINOCA patients had a lower mortality rate than MI-CAD patients (P < .001). MINOCA patients had a lower risk of MACE (HR = 0.57, 95% CI 0.55-0.59), 12-month mortality after discharge (HR = 0.60, 95% CI 0.57-0.63) and a low rate of re-hospitalization for HF or AMI (HR = 0.89; 95% CI 0.86-0.91). 23
In another sense, and to determine the factors predictive of an unfavorable outcome in patients with MINOCA, Nordenskjöld et al conducted a 10-year observational study of 199 163 patients admitted for AMI. For MACEs defined as all-cause mortality, rehospitalization for acute infarction, ischemic stroke and heart failure, and after risk adjustment, the predictive factors found were advanced age, hypertension, diabetes, previous myocardial infarction or stroke, active smoking, peripheral vascular disease, reduced left ventricular ejection fraction, higher creatinine and lower total cholesterol levels, and for all-cause mortality, the independent predictive factors are almost the same as those for MACEs, in addition to the high level of CRP (C-reactive protein), and after the results of this analysis, we can deduce the similarity between the predictive factors of unfavorable evolution between MINOCA and MI-CAD. 24 And since patients with CAD-MI complicated by cardiogenic shock on admission are characterized by high short- and long-term mortality,25-27 KILLIP stage 1 was independently associated with high mortality, with a 3-fold higher risk of mortality (P = .001) and a 4-fold higher risk of hospitalization for heart failure (P = .003) in patient admitted for MINOCA. 3
To summarize, MINOCA remains an entity in its own right, and not negligible among patients admitted for ACS whose long-term prognosis is better than patients with MI-CAD, 28 although the predictive factors of an unfavorable outcome are almost similar, but the major difference in the pathophysiology of the 2 entities may explain this difference in prognosis. 29
Study Limitations
Our study has 3 main limitations: firstly, its observational nature; secondly, the number of patients included, although 1077 patients is a large number, it would be just as well to have a larger number, especially given the observational nature of the study; and thirdly, the limited follow-up time of 1 year. But despite these limitations, our results are very similar to those published in the literature.
Conclusion
MINOCA remains an entity of recent description, and its pathophysiological mechanisms are still the subject of debate, but despite this ambiguity, the prognosis of these patients in the short and long term remains generally favorable.
Footnotes
Acknowledgements
None
Author Contributions
A.B. developed the project idea, writing and revising the proofs.
M. I.writing and revising the proofs.
Z. B., N.I., and N.E. supervised the project.
All authors contributed to the article and approved the submitted version.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are available in the article and in its online supplementary material.
Ethical Approval
Not required
Consent to Publication
Not required