
Abstract
Background:
According to a report from the WHO, an estimated 1.13 billion people worldwide have hypertension. Medication therapy management (MTM) service is a clinical service based on the theoretical and methodological framework of pharmaceutical care practice, which aims to ensure the best therapeutic outcomes for the patient by identifying, preventing, and resolving drug therapy problems (DTPs).
Purpose:
The goal of this study was to determine the impact of MTM on hypertension management in Ethiopia.
Methods:
A pre-post interventional study design was used. Descriptive statistics, linear regression, and logistic regressions were employed to present and analyze data.
Results:
The final analysis included 279 patients out of 304, with a 7.8% attrition rate. The prevalence of drug therapy problems (DTPs) reduced from 63.4% at baseline to 31.5% during the post-intervention phase. Polypharmacy (AOR = 2.46; 95% CI: 1.27-4.77) and complications (AOR = 0.52; 95% CI: 0.27-0.99) were substantially associated with DTPs at the start of the study. The MTM resulted in a significant reduction in mean systolic blood pressure (SBP) (AOR = 5.31, 95% CI (3.50-7.11), P < .001), as well as a significant increase (P < .001) in the number of study patients who reached a target BP. At the end of the MTM intervention, non-adherence was linked with DTP (AOR = 2.40; 95% CI: 1.33-4.334) and living outside Addis Ababa (AOR = 1.73; 95% CI: 1.38-1.88). On average, treatment satisfaction was 86.55% (+SD) 10.34.
Conclusion:
To resolve DTPs and improve clinical outcomes, the MTM service was critical. The majority of patients were found to be compliant with a high treatment satisfaction score.
Keywords
Introduction
Hypertension is the condition of persistent, non-physiologic elevation of systemic blood pressure (BP). It is typically defined as a resting Systolic BP (SBP) of 140 mm Hg or higher or Diastolic BP (DBP) of 90 mm Hg or higher following repeated examination or receiving therapy for the indication of BP-lowering. 1 It is a chronic condition that usually is treated with different anti-hypertensive drugs and lifestyle changes. Patients with hypertension often receive multiple medications2,3 and have different co-morbid chronic diseases that can lead to the occurrence of Drug Therapy Problems (DTPs). 4
DTPs are undesirable events experienced by the patient involving drug therapy that impede progress toward achieving the desired goals of therapy. 5 It includes unnecessary drug therapy, the need for additional drug therapy, ineffective drug therapy, adverse drug reaction, appropriate dosing, and non-adherence.5,6 In studies related to the determination of DTPs, the prevalence of DTPs has been reported to be high in patients with hypertension.7-10 DTPs among hypertensive patients could be the major contributors to poor health outcomes,4,7 lower health-related quality of life, 8 increase health care costs, and eroded public confidence in health care systems. 11
Hypertension is an important worldwide public health problem and the most preventable risk factor for cerebrovascular, cardiovascular, and kidney disease. 12 Genetic, environmental as well as important gene-environment interactions and behavioral factors influence the development of hypertension. 13 According to a report from the World Health Organization (WHO), an estimated 1.13 billion people worldwide have hypertension. 14 Different surveys of the prevalence of hypertension also indicate a growing global burden of the disease as it increases sharply with the growing pandemic of obesity, advancing age, and urbanization. 15
The trend of hypertension in Africa shows that it has risen from 55 million in 1990 to 130 million in 2010 and by 2030 expected to be 220 million. 16 A community-based survey from 9 regions of Ethiopia showed the overall prevalence of raised BP among the Ethiopian population aged 15 to 69 years to be 15.8%. The prevalence is higher in the urban population (19.7%) than rural (14.8%). 17 In Ethiopia, hypertension affects 19.6% of the population, and it is associated with high rates of morbidity and mortality. Ethiopia’s hypertension treatment appears to be lacking as only 4.5% of its hypertensive patients have their blood pressure under control.18,19 Some of the challenges and obstacles to managing hypertension in Ethiopia include inadequate resources for health care, inadequate quality of service, poor drug adherence, and a lack of information.19,20 Therefore, practical and efficient measures are needed to enhance Ethiopia’s hypertension outcomes. One such intervention is medication therapy management (MTM), MTM service is a clinical service based on the theoretical and methodological framework of pharmaceutical care practice, which aims to ensure the best therapeutic outcomes for the patient by identifying, preventing, and resolving DTPs.21-23
MTM is typically provided by pharmacists through Performing patient assessment and a comprehensive medication review (CMR); formulating a medication treatment plan, monitoring efficacy and safety of medication therapy; enhancing medication adherence through patient empowerment and education; and documenting and communicating MTM services to prescribers to maintain comprehensive patient care.24,25 MTM can help patients get the most benefit from their medications, prevent costly medication problems, and achieve optimal goals of medication therapy.21-23 MTM has also been shown to improve blood pressure management and reduce cardiovascular events in a number of settings. However, there is a lack of information regarding MTM’s impact on hypertension treatment follow-up, an important indicator of care quality and continuity.
This is the first study that we are aware of that evaluates the impact of an MTM service on the follow-up of hypertension medication in Ethiopia, a nation with limited resources and limited access to high-quality healthcare. 26 The study identifies several gaps, including limited research in low-resource settings, a lack of understanding of patient-centered outcomes, a lack of research on long-term impact, comparative effectiveness, and implementation strategies. The study aims to bridge these gaps by examining the sustainability and durability of the observed effects over an extended period, comparing the effectiveness of medication therapy management services with alternative interventions, and understanding factors influencing successful implementation. Addressing these gaps can contribute to the advancement of hypertension management knowledge and optimize care delivery in similar healthcare settings.
Materials and Methods
Study setting
The research has been carried out in Ethiopia at a centrally located referral hospital renal ambulatory clinic. The hospital is the country’s largest referral teaching hospital. The hospital’s outpatient clinics serve 500 000 patients annually and include 51 disciplines, sub-specializations, and super-specialties. The renal out-patient clinic functions 3 times per week serving 60 to 80 patients per session. Hypertensive patients account for the majority.
Study type and period
A one-group pre-post interventional study was conducted in 2 phases from July 2019 to April 2020. The first phase lasted 6 months of the intervention period and the second phase was a posted intervention study, which lasted for 4 months.
Study population
The study population involves all hypertensive patients visiting the renal ambulatory clinic of the hospital during the study period and who fulfilled the inclusion criteria. Patients who were ⩾18 years of age and those patients who were on antihypertensive drug treatment for at least 1 year were included. Those patients with any evidence of hypertensive urgency or emergency, serious renal, cardiac, or hepatic disease, pregnancy, dementia, or cognitive impairment, and those who refused to give informed consent were excluded.
Sampling method and sample size determination
The sample size was calculated using a single proportion formula with the assumption of a 5% margin of error, 95% confidence interval, and 55.6% prevalence of DTPs in patients with hypertension from the prior study. 11 The sample size was determined using an estimated population size of 1010 adult hypertensive patients based on the previous hypertensive patients’ attendance records at the renal ambulatory Clinic of the hospital. Using a single proportion formula, the sample size was determined to be 304 patients. A systematic random sampling method was used to recruit samples for the study on each day of the data collection process.
Intervention development and implementation
The MTM service was launched by creating a patient database: relevant previous medical and medication histories by data collectors. After the patient visited the physician, he/she met with the MTM pharmacist face-to-face for the Medication Therapy Review (MTR).
The clinical pharmacists identified medication-related needs of patients including indication, effectiveness, safety, and adherence. This was followed by an evaluation of the appropriateness of pharmacotherapy using various references and current practice guidelines. Micromedex drug interaction checker was used to identify the potential drug-drug interactions. With the aid of Micromedex medication interaction checkers, Pharmacists may identify and manage any drug interactions in their patients. They provide information on the severity, mechanism, start, clinical effects, and therapy of drug interactions in addition to references to support the advice. Micromedex drug interaction checkers are not a substitute for clinical expertise, but rather a support tool to enhance patient safety and quality of care.
Adverse drug reactions were also identified from the patient medical record and through interviews. Eventually, drug-related problems (DTPs) were listed and prioritized leading to the development of a pharmaceutical care plan. If any of the patients experienced DTP pharmacist identified its cause and classified it into different categories according to and prioritized DTPs for intervention. The MTM Pharmacist then created a pharmaceutical care plan to resolve the problem. The care plan might have necessitated the participation of patients, physicians, or both. If a pharmaceutical care plan involved patient participation to resolve DTP the pharmacist created a medication action plan (MAP) and directly communicated with the patient to resolve the identified problem. When the identified DTPs need the participation of prescribing physicians pharmaceutical care plan that involves physicians was prepared and communicated with them.
After communicating with physicians and patients to resolve DTPs and all necessary modifications were made to optimize drug therapy, a reconciled medication list was written and provided to the patient as a personal medication record (PMR). The status of the identified DTP was then recorded. An evidence-based brochure that was prepared in the Amharic language to increase patients’ knowledge of drug use and disease management was provided after counseling on all important issues related to therapy.
After each visit, patients were interviewed for progress, any new DTP, and counseled on their disease state and medication use. Unresolved issues from the prior sessions were also discussed. The pharmacist assessed the treatment care plan to monitor the patient’s adherence to the medication action plan and to establish new therapy goals when required. Finally, after 6 months of follow-up, outcomes of the pharmaceutical care (PC) provided for each patient were assessed. The assessment included DTP identification, medication adherence, and patient treatment satisfaction.
Data collection and management
Data collection instruments and procedures
Socio-demographic data, health information, and lifestyle factors, clinical characteristics, medication history were collected using questionnaires and data abstraction format (Supplemental Annex I). Blood pressure was measured using a sphygmomanometer at baseline and during each visit to monitor the efficacy of the medication and the goal of therapy achieved.
The Micromedex drug interaction tool lists the drug-drug interactions that occurred during patient assessment. The tool assigns a severity rating to each interaction, from contraindicated to minor. When analyzing the results, we considered the patient’s health, the availability of substitute medications, and the clinical importance of the interactions. We have also discussed the tool’s results and the pharmacists’ expertise with the physician to help patients and make the best clinical decision.
DTPs were identified and classified according to the Cipolle et al DTP classification tool which specifies 4 categories of DTP and 7 types of DTP and a specific cause for each DTP. 6 The level of adherence was assessed using the Morisky Green Levin Medication Adherence Scale (MGL) at the end of the intervention. Thus, patients were considered adherent if the score was ⩽2 and non-adherent if the score was >2 (Supplemental Annex II). A self-administered Treatment Satisfaction with Medicines Questionnaire (SATMED-Q) 17 was also used to measure patients’ treatment satisfaction after MTM service (Supplemental Annex III).
Data collector’s recruitment and training
Three nurses and one clinical pharmacist were recruited as data collectors. The training was given to the data collectors; to familiarize them with the study protocol, how to request informed consent from eligible participants, and to conduct a patient interview.
Data quality management
A pre-test was carried out on 5% of the sample at the outpatient department of Tirunesh Beijing General Hospital before commencing the patient recruitment process and data collection to check the completeness of the instruments. Based on the results obtained from the pre-test, an amendment was made to the assessment tools and ways of assessment. Appropriate training was also given to the data collectors. The principal investigator (PI) was closely supervising the data collection daily.
Data analysis
Data were coded and entered into SPSS version-25 statistical software for management and analysis. Descriptive analysis was computed as frequency and percent for categorical variables and mean and standard deviation (SD) for continuous variables. Both binary and multiple logistic regression analyses were performed. Independent variables having a P-value < .20 in the bivariate logistic regression analysis were entered into a multivariable logistic regression analysis to control the confounding effect.
A paired sample t-test was used to ascertain the significance of differences between the mean value of baseline and post-MTM SBP and DBP. The statistical significance of treatment satisfaction was determined using an independent t-test for mean values of 2 continuous variables and one-way analysis of variance (ANOVA) with post hoc analysis for mean values of more than 2 continuous variables. A 95% CI and P-value of <.05 were considered statistically significant for all data analyses.
The flow of study participants
A total of 304 patients meeting the previously described inclusion criteria were referred and recruited to the HTN MTM service using systematic random sampling after patients gave informed consent from July 2019 to April 2020. Out of this, 279 (92.7%) study participants completed the study and entered into the final analysis. Thus, the attrition rate was found to be 7.8% (Figure 1).

Flow diagram of patients with hypertension participating in MTM service study at ambulatory clinic of TASH, July 2019 to April 2020.
Results
Sociodemographic characteristics
Males and females were equally represented (50.5% females). The mean (SD) age of the study participants was 56.26 ± 11.75 years and 23.7% of them were ⩾65 elders. Most of the study participants were married (82.8%) and the majority of them were living within the study city (89.6%). Of the study’s participants, almost a quarter (26.2%) had completed secondary school, and 24.4% were employed. Half (53.8%) of the study participants were found to get their medication through third-party coverage (Table 1).
Socio-demographic characteristics of ambulatory hypertensive patients on follow-up clinic (n = 279).

Abbreviation: SD, standard deviation.
All participants who took part were literate. Thirty-three individuals did not hold a formal education, nonetheless. Secondary school refers to high school education, while tertiary-level education refers to college or university education.
The khat plant is found throughout East Africa and the Arabian Peninsula. 27 Khat contains stimulant chemicals that can cause increased talkativeness, alertness, excitement, and mild euphoria. 28 Khat chewing is part of some social and cultural traditions in the regions where the plant grows, but it is also associated with some health and legal risks. Chahat is used for social and cultural purposes despite its risks to health and legality. 29
Clinical characteristics and medication profile
Most of the study participants had a hypertension treatment duration of >10 years. Around 66.6% and 45.9% had experienced at least one co-morbid condition and complication, respectively; with diabetic Mellitus (DM) (31.2%) and nephropathy (35.4%) being the most common co-morbid condition and hypertension-related complication respectively. The mean (SD) number of medications was 3.70 (±2.00). The majority of them were prescribed dual therapy (39.1%). Calcium channel blockers (CCBs) were the most frequently prescribed class of drugs (69.9%) followed by angiotensin-converting enzymes (ACEIs) (54.1%) and diuretics (48.7%). Only 52.7% had controlled BP. The majority (73.1%) of the study participants had 1 to 2 MTM pharmacist visits and about 26.9% had 3 or more visits (Table 2).
Clinical characteristics of ambulatory hypertensive patients on follow-up clinic (n = 279).

Abbreviations: BMI, Body Mass Index; CKD, chronic kidney disease; DM, diabetic mellitus; HTN, hypertension; HHD, hypertensive heart disease; IHD, ischemic heart disease; MTM, Medication Therapy Management; PN, peripheral neuropathy; SD, standard deviation.
Heart failure, atrial fibrillation, peptic ulcer disease, valvular heart disease, Thyroid disorders, Psychiatric and Neurological disorders, infection, obesity, cancer.
Drug therapy problems
Prevalence and pattern
At baseline, a total of 260 DTPs were identified. Additionally, 27 DTPs were identified during follow-up. The prevalence of DTP at baseline was 63.4%. At the end of the study, at least one, DTP was identified among 88 patients; which makes a prevalence of 31.54% (Figure 2).
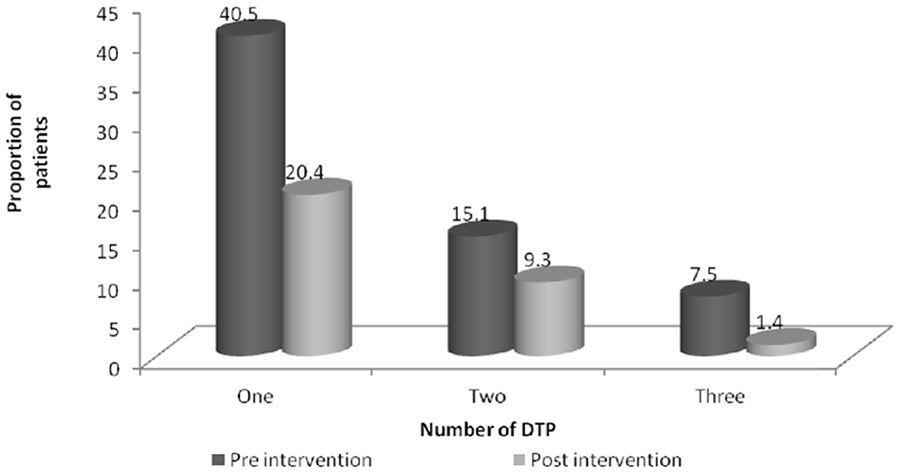
Pattern of DTPs among ambulatory hypertensive patients on follow-up clinic at TASH, Addis Ababa, Ethiopia, July 1, 2019 to April 30 2020 (n = 279).
There was a significant reduction in the proportion of patients with at least one DTP from 63.4% in the pre-intervention phase to 31.5% during the post-intervention phase (P < .05). The most encountered DTPs in the pre-intervention phase were non-adherence (n = 53, 20.38%) followed by ADR (n = 48, 18.46%) and the need for additional drug therapy (n = 47, 18%). On the other hand, the most encountered DTP in the post-intervention was ineffective drug therapy (n = 32, 26.66%) followed by the need for additional drug therapy (n = 31, 25.83%) and non-adherence (n = 19, 15.83%). Using the McNemars test, there was a statistically significant decline in the proportion of patients with overall DTP (P < .01) and each type of DTP from baseline to end of the study (P < .01) except for ineffective drug therapy (Table 3).
Type and proportion of DTPs among ambulatory hypertensive patients in follow-up clinic (n = 279).

McNamara chi-square test, DTP, drug therapy problems; MTM, Medication Therapy Management.
From a total of 287 identified DTPs, MTM service resolved 203 (70.73%) of them. Pharmaceutical care interventions were made for 161(56%) involving physicians. From these, 104 (64.5%) DTPs were accepted, 42 (26%) were partially accepted and 15 (9.3%) were rejected. The pharmaceutical care plan involving patient participation was 126 (43%). Ninety-nine (78.50%) of these were solved with the patient. The majority of them were about unnecessary OTC medication use, adherence enhancement, and ADR management.
Predictors of drug therapy problems
Different socio-demographic and clinical characteristics were considered for binary logistic regression analysis. The variables included in the bivariate analysis were age, sex, residency, education status, marital status, alcohol use, physical activity, chat chewing, co-morbidity, aspirin use, statin use, non-steroidal anti-inflammatory drug use, BP control, number of medications, duration of treatment, complication, health care cost coverage, and salt consumption. Depending on the result of binary logistic regression variables like age, sex, marital status, salt restriction, duration of treatment, presence of co-morbidity, presence of complication, number of medications, and BP control status were considered for multivariate analysis to determine predictors of DTP at baseline. After the provision of MTM service, the level of adherence and the number of MTM visits were also considered for binary and multivariate logistic analysis.
The result of the multivariate logistic analysis showed that several medications, the presence of complications, and salt restriction status were significantly associated with the occurrence of DTP at baseline. Accordingly, participants who took more than 5 medications were 2.5 times (AOR = 2.46 95% CI: 1.27-4.77) more likely to develop DTPs as compared to those taking less than 5 medications. Patients without hypertension-related complications were twice as likely to develop DTP than those who developed hypertension-related complications (AOR = 0.52 95% CI: 0.27-0.99). The status of salt restriction was also found to be associated with the occurrence of DTPs. The data showed a decreased risk of developing DTPs by half for samples who reported having restricted salt intake (AOR = 0.56 95% CI: 0.33-0.97) as compared to those who consumed without restriction.
At the end of the study, the presence of hypertension-related complications and the level of medication adherence were found to be significantly associated with experiencing DTPs. The risk of occurrence of DTP was lower approximately by 50% (AOR = 0.43 95% CI: 0.23-0.80) in patients with complications as compared to those without it. Moreover, the risk of DTPs was 70% times (AOR = 0.30, 95% CI: 0.14-0.69) lower in those patients with high adherence status as compared to participants with low adherence (Table 4).
Multivariate analysis of factors associated with drug therapy problems among ambulatory hypertensive patients on follow-up (n = 279).
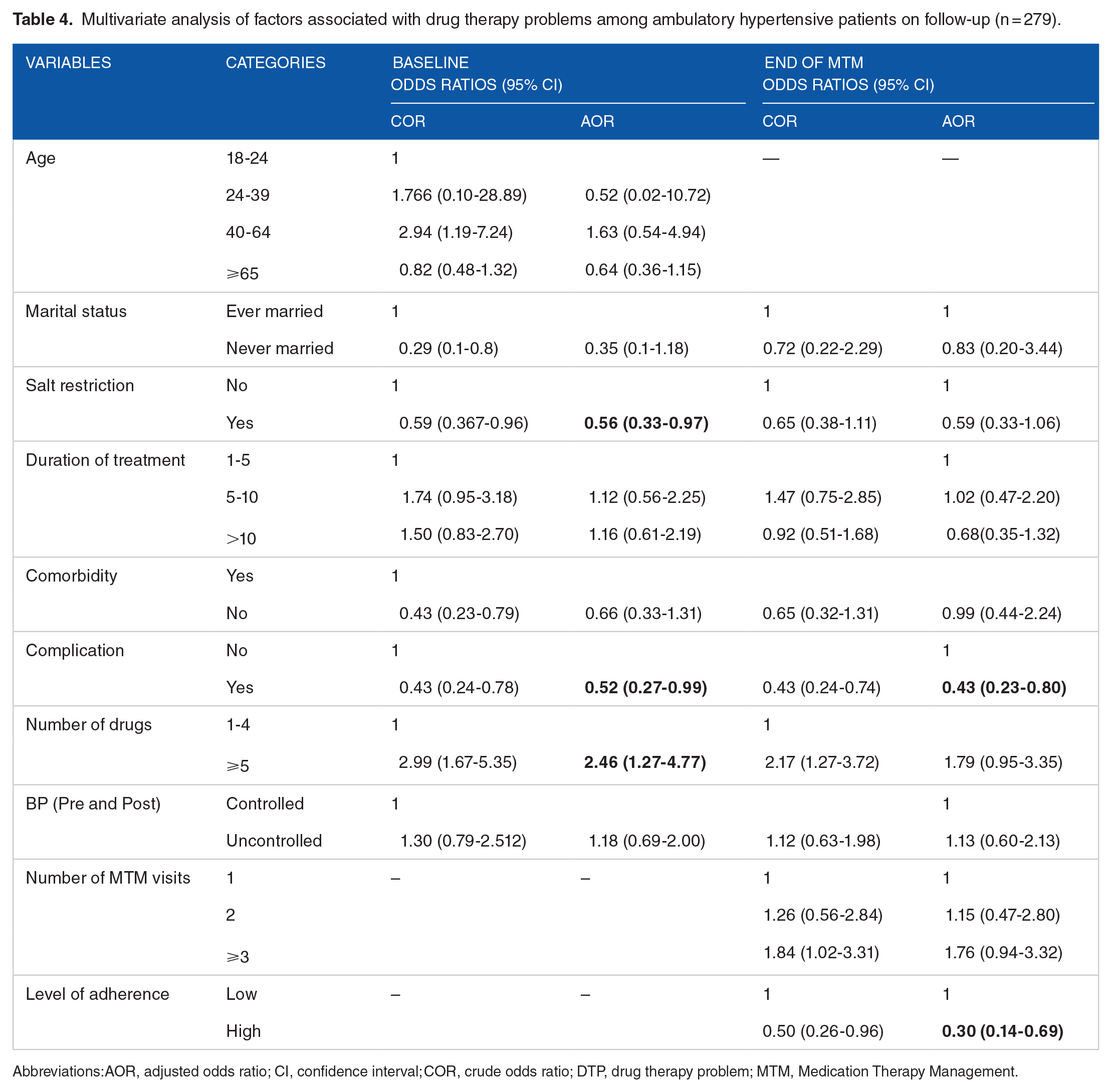
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; DTP, drug therapy problem; MTM, Medication Therapy Management.
A total of 103 (37%) potential DDIs have been observed out of which 5% were associated with serious drug interactions (Table 5).
The list of serious drug interactions observed in the study.

Changes in clinical outcomes
The mean SBP at baseline was 136.67 mmHg and this was decreased to 131.36 mmHg at the end of the study. Using paired t-test analysis the change in SBP was found to be significant (P < .001). The difference in DBP was not found to be statistically significant (P = .053) from the baseline (Table 6).
The mean systolic blood pressure and diastolic blood pressure of ambulatory hypertensive patients in follow-up clinic (n = 279).

Abbreviations: BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; MTM, Medication Therapy Management; SBP, systolic blood pressure.
The Proportion of patients with controlled BP was 52.70% at the beginning of the study and this was increased to 72.40% at the end of the study (P < .01). Likewise, we have also found a decreased proportion of patients with stage 1 and stage 2 hypertension from baseline to the end of the study. The proportion of stage-1 hypertension decreased from 36.52% to 20.95% while stage-2 hypertension decreased from 10.78% to 6.65% as depicted in Figure 3.

Blood pressure control status of ambulatory hypertensive patients on follow-up clinic at TASH, Addis Ababa, Ethiopia, July 2019 to April 2020 (n = 279).
Medication adherence status
According to the MGL medication adherence scale, after the implementation of the MTM service, 194 (69.5%) of patients were found to be adherent to their antihypertensive medications. Different socio-demographic and clinical characteristics were included in the univariate analysis and variables with P-value < .2 were further entered into multivariate analysis to identify the predictors of medication non-adherence.
Thus, the source of medication and residency was significantly associated with medication non-adherence. Patients who got their medication through third-party coverage were 90% times (AOR = 0.10; 95% CI: 0.01-0.77) less adherent than those buying their medications on a cash basis. Similarly, study participants who lived in the study city were 1.73 times more adherent (AOR = 1.73; 95% CI: 1.38-1.88) than those living outside the study city (Table 7).
Multivariate analysis of factors associated with medication adherence among ambulatory hypertensive patients in follow-up clinic (n = 279).

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; DTP, drug therapy problem; MTM, Medication Therapy Management.
Variables in bivariate analysis with P ⩽ .20 and ⩽.05 indicated by * and ** respectively.
Patient treatment satisfaction
The treatment satisfaction rate for all domains is described in Figure 4. According to the SATMED-Q score tool of treatment satisfaction, the overall mean score (SD) of treatment satisfaction was 86.55 ± 10.34.

Treatment satisfaction level following MTM intervention among ambulatory hypertensive patients on follow-up at TASH, Addis Ababa, Ethiopia, January 1 to April 30 (n = 279).
Predictors of patients’ treatment satisfaction
There was no statistically significant difference in general treatment satisfaction among patients’ age groups, sex, marital status, education level, employment status, Source of medication, residence, co-morbid condition, and duration of treatment. The presence of Poly-pharmacy, ADR, and complications was found to be significantly associated with treatment satisfaction (Table 8).
Relationship between treatment satisfaction and different characteristics of ambulatory hypertensive patients in follow-up clinic (n = 279).

Abbreviations: MTM, Medication Therapy Management; SD, standard deviation.
There was a significant difference in general treatment satisfaction among patients with DTP experiencing status. Accordingly, patients experiencing DTPs had a lower mean score as compared to those without it (F = 4.88; P = .002) for general treatment satisfaction. Significant differences among patients with different adherence statuses were found as patients with low adherence were less likely to be satisfied with their treatment (F = 0.84; P < .001). The median general satisfaction scores for those patients’ adherent and not adherent to antihypertensive medications were around 90 and 80, respectively (Figure 5).
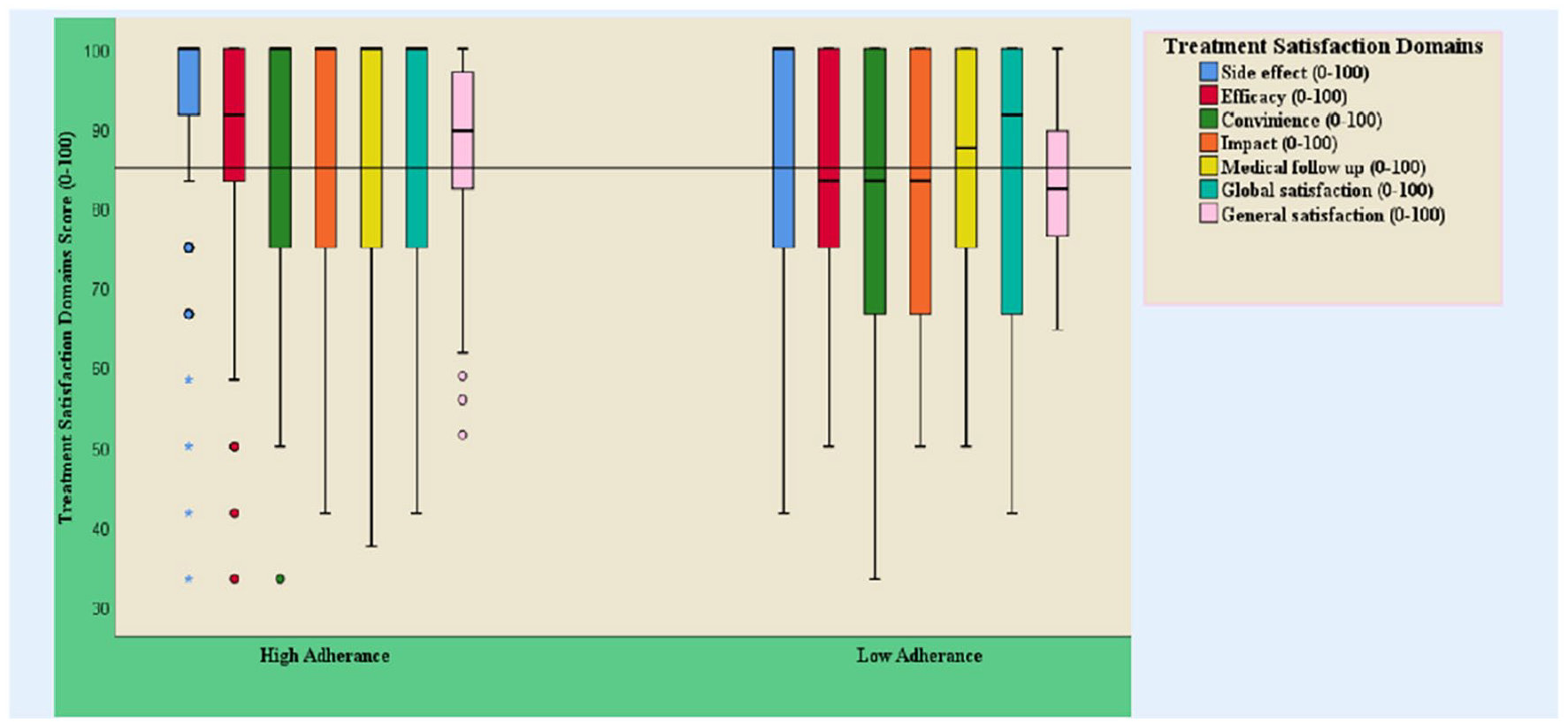
Box plot of association of all domains of treatment satisfaction with adherence status of ambulatory hypertensive patients on follow-up at TASH, Addis Ababa, Ethiopia, January April 2020 (n = 279).
Discussion
The study aimed to assess the impact of Medication Therapy Management (MTM) services on blood pressure control, medication adherence, Drug Therapy Problems (DTPs), and treatment satisfaction among hypertensive patients in Ethiopia, recognizing their high risk of developing DTPs due to multiple co-morbidities and poly-pharmacy.3,30 The identification and resolution of DTPs are critical healthcare contributions, as they compromise therapy goals and contribute to greater clinical, humanistic, and economic burdens. 8
The implementation of MTM services in the study resulted in the resolution of 70.73% of identified DTPs and a decrease in DTP prevalence from 63.4% at baseline to 31.54% at the end of the program. 3 Comparable rates were observed in Nigeria (69.23%), while higher rates were reported in England (86.7%) and the USA (78%), suggesting variations possibly influenced by factors such as healthcare infrastructure and study methodology.31,32 Factors contributing to higher DTP prevalence in low- and middle-income countries (LMICs) compared to high-income countries (HICs) include low health literacy, poor adherence, and limited access to healthcare and medications. 3
Physician acceptance of pharmacist recommendations in the study was 64.5%, consistent with rates reported elsewhere but lower than certain studies, potentially attributed to methodological differences and varying DTP classification systems.33-36 Reasons for rejection included concerns about drug availability, affordability, clinical experience, and distinguishing potential from actual DTPs.37,38
In conclusion, the study highlights the efficacy of MTM services in addressing DTPs among hypertensive patients in Ethiopia and underscores the importance of pharmacist involvement in community healthcare to enhance medication availability and optimize therapy outcomes.3,37,38
The study revealed that non-adherence to medications, Adverse Drug Reactions (ADRs), and the need for additional drug therapy were the most common types of Drug Therapy Problems (DTPs) at baseline, consistent with previous research.33,39 This pattern suggests patients’ lack of access to medications, poor knowledge about drugs, and the long-term complications of hypertension as contributing factors to DTP occurrence. 40
Pharmacist interventions primarily addressed doses too low, doses too high, and unnecessary DTPs, aligning with other studies reporting a lower substitution rate for ineffective drugs after pharmacist intervention.34,40 Specifically, the study highlighted concerns regarding the use of atenolol, a frequently prescribed beta-blocker for hypertension, due to its limited evidence for efficacy and safety compared to other antihypertensive medications.41-43
Several medications, complications related to hypertension, and salt consumption status were significantly associated with DTP occurrence at baseline, supporting earlier findings.7,10,44 Notably, the presence of hypertension-related complications emerged as a protective factor against DTPs, likely due to increased caution in medication management and enhanced clinician attention to patients with complications.44,45 These findings underscore the importance of educational interventions targeting disease management, complications, and medication adherence in hypertensive patients. 46
The study also noted a frequent occurrence of ADRs, potentially influenced by the high rate of significant cardiovascular drugs, highlighting the importance of identifying and managing Drug-Drug Interactions (DDIs) in hypertension management to prevent adverse outcomes and reduce healthcare costs. 47
The findings suggest several actionable measures to address hypertension management challenges. Clinical pharmacists could play a pivotal role in optimizing drug therapy by enhancing rational drug use and preventing ineffective drug therapy. 48 Furthermore, patient education and counseling to improve medication adherence and raise awareness about treatment goals and Adverse Drug Reactions (ADRs) are crucial. 49
Significant improvements were observed in mean systolic blood pressure (SBP) levels from baseline to the end of the study, with an increase in the proportion of patients achieving controlled blood pressure (BP). 18 Although these results were favorable compared to prior studies in Ethiopia and the USA, variations in intervention intensity, follow-up duration, and participant characteristics may account for discrepancies. 50 The study applied relaxed BP goals in accordance with national and international guidelines.51,52
Drug-Drug Interactions (DDIs) emerged as a major concern, with a considerable proportion of serious DDIs necessitating changes in prescribed drugs. 53 While a significant reduction in SBP was noted, the impact on diastolic blood pressure (DBP) was not significant, possibly influenced by baseline characteristics and intervention components.54-56 The sensitivity of SBP to interventions could be attributed to the higher prevalence of co-morbidities like Chronic Kidney Disease (CKD) and Diabetes Mellitus (DM), emphasizing the importance of tailored interventions for specific patient groups. 57
Medication adherence rates varied, with factors such as third-party medication coverage and urban residency influencing adherence levels. 58 However, the association between medication accessibility and adherence warrants further investigation, as it appears to be a multifaceted issue influenced by various factors.59-61
The study demonstrated high treatment satisfaction scores post-intervention, potentially attributable to increased health literacy, adherence rates, and reduced DTPs and ADRs.62,63 Importantly, treatment satisfaction was positively associated with medication adherence, highlighting the need to address patient concerns and safety issues during consultations to enhance adherence and overall treatment satisfaction.62,64-66
Limitation of the Study
The study has limitations due to its small sample size, short follow-up, limited generalizability, lack of randomization, and self-reporting adherence measurement, which could lead to regression to the mean and recall bias.
Conclusions
The provision of MTM service demonstrated the decreased prevalence of DTPs after 6 months of follow-up. Additionally, modest improvement in clinical outcomes such as average SBP and DBP with an increased proportion of patients who are at goal BP from baseline to the end of the study was found. Furthermore, a higher medication adherence rate and patient treatment satisfaction were reported by study participants after introducing the MTM service. Conjointly, this result will be valuable in the management of hypertension and could serve as a framework for further research on a similar topic.
Supplemental Material
sj-docx-1-cic-10.1177_11795468241274720 – Supplemental material for The Impact of a Medication Therapy Management Service on the Outcomes of Hypertension Treatment Follow-Up Care in an Ethiopian Tertiary Hospital: A Pre-Post Interventional Study
Supplemental material, sj-docx-1-cic-10.1177_11795468241274720 for The Impact of a Medication Therapy Management Service on the Outcomes of Hypertension Treatment Follow-Up Care in an Ethiopian Tertiary Hospital: A Pre-Post Interventional Study by Belachew Bulo, Minyahil Woldu, Alemseged Beyene, Desalew Mekonnen and Ephrem Engidawork in Clinical Medicine Insights: Cardiology
Supplemental Material
sj-docx-2-cic-10.1177_11795468241274720 – Supplemental material for The Impact of a Medication Therapy Management Service on the Outcomes of Hypertension Treatment Follow-Up Care in an Ethiopian Tertiary Hospital: A Pre-Post Interventional Study
Supplemental material, sj-docx-2-cic-10.1177_11795468241274720 for The Impact of a Medication Therapy Management Service on the Outcomes of Hypertension Treatment Follow-Up Care in an Ethiopian Tertiary Hospital: A Pre-Post Interventional Study by Belachew Bulo, Minyahil Woldu, Alemseged Beyene, Desalew Mekonnen and Ephrem Engidawork in Clinical Medicine Insights: Cardiology
Supplemental Material
sj-docx-3-cic-10.1177_11795468241274720 – Supplemental material for The Impact of a Medication Therapy Management Service on the Outcomes of Hypertension Treatment Follow-Up Care in an Ethiopian Tertiary Hospital: A Pre-Post Interventional Study
Supplemental material, sj-docx-3-cic-10.1177_11795468241274720 for The Impact of a Medication Therapy Management Service on the Outcomes of Hypertension Treatment Follow-Up Care in an Ethiopian Tertiary Hospital: A Pre-Post Interventional Study by Belachew Bulo, Minyahil Woldu, Alemseged Beyene, Desalew Mekonnen and Ephrem Engidawork in Clinical Medicine Insights: Cardiology
Footnotes
Acknowledgements
The authors would like to extend their gratitude to all the data collectors, participants, and staff members of the renal ambulatory clinic of TASH for their contributions to undertaking this research. We would also like to highlight that the paper is available through the Addis Abeba University repository system.
Author Contributions
BB: Data Curation, Formal analysis, Investigation, Writing—Original Draft, Writing—Funding acquisition; MA: Conceptualization, Methodology, Software, Review & Editing, Project administration, Supervision AB: Conceptualization, Methodology, Software, Review & Editing, Project administration, Supervision DM: Review & Editing, Supervision; EE: Conceptualization, Methodology, Supervision, Writing—Review & Editing, Funding acquisition.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The original funding source for conducting the research was sponsored by AAU. Part of the research was also sponsored by the MTM-AAU-2017-21 project.
Ethical Considerations
The Ethical Review Board of Addis Ababa University’s School of Pharmacy granted ethical clearance and approval for the study protocols (ERB/SOP/114/07/2019). Furthermore, we received approval to carry out the study at the clinic from the directors of the Renal Clinic and the Department of Internal Medicine. The Declaration of Helsinki’s guiding principles were followed in the conduct of the study.
Patient Consent
Prior to the commencement of data collection, all participants were informed about the study’s objectives, and their written consent was acquired. They were also made fully aware of their unrestricted right to withdraw from the study at any time. Strict protocols were put in place to protect confidentiality and privacy, such as purposefully avoiding identifiers and limiting access to data. Before participating in the trial, all patients—regardless of their educational background—provided written informed consent. During the recruitment procedure, individuals without formal education participated in literacy evaluations by reading consent forms translated into Amharic and writing their names in Geez or Ethiopic letters. This method ensured that participants without formal education understood the study material and gave independent written informed consent without the need for a legally authorized representative (LAR).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.