
Abstract
Introduction:
Hypertension is an important public health menace globally and in sub-Saharan Africa. The prevalence of hypertension is on the rise in low- and lower-middle-income countries (LMIC) such as Ghana. This rise led to the adoption of the May Measurement Month (MMM) initiative, a global blood pressure screening campaign. We aimed to create awareness and present the findings of the 2019 MMM screening campaign in the Ashanti region of Ghana.
Methods:
Ghana was 1 of 92 countries that participated in this global community-based cross-sectional study in May 2019. Participants (⩾18 years) were recruited by opportunistic sampling. The blood pressures of participants were measured 3 times and the mean of the last 2 was used for the analysis. Summary statistics were used to describe the data. Simple and multiple logistic regression models were used to determine the predictors of hypertension.
Results:
We screened 3080 participants with a mean age of 39.8 ± 16.8 years. The prevalence of hypertension was 27.3% among participants. Two-thirds of the hypertensives were unaware of their condition and only 49.5% of participants with a history of hypertension on medication were controlled. Predictors of hypertension in a multiple logistic regression were increasing age (OR = 1.05 (CI 1.04-1.06), P < .001) and high body mass index (OR = 1.06 (1.02-1.10), P = .005).
Conclusion:
The MMM initiative is highly commendable and of huge public health importance in LMICs like Ghana. Population-based health programs such as the MMM initiative is encouraged to shape appropriate public health policies to reduce the prevalence of hypertension.
Introduction
Globally, there is an increasing prevalence of hypertension with an increased incidence of its complications such as stroke, myocardial infarctions, heart failure, and chronic kidney disease. 1 According to the World Health Organization (WHO), hypertension is estimated to contribute to about 12.8% of the total of all deaths and 3.7% of total disability-adjusted life years (DALY). 1 This high prevalence can be attributed to population growth, aging populations, and unhealthy lifestyles. 1 Cardiovascular diseases affect approximately a third of the world’s adult population and are described as the world’s largest-ever pandemic. 2 The heart, brain, and kidneys are end organs complicated by uncontrolled hypertension. 3
Hypertension has many complications such as stroke, heart failure, kidney disease, retinopathy, peripheral vascular disease, and myocardial ischemia. 4 Indeed, the most common cardiac presentation at the emergency department in Ghana is driven by hypertension. 5 Hypertension is the leading cause of preventable deaths 6 and an important public health problem, particularly in sub-Saharan Africa. 7 The prevalence of hypertension is increasing in low- and middle-income countries(LMIC) but decreasing in high-income countries7,8 with about 80% of the attributable burden of hypertension globally occurring in LMIC. 9 The pooled prevalence of hypertension in Africa has increased from 19.7% in the 1990s to 30.8% in 2010. 8 According to a recent systematic review, the pooled prevalence of hypertension is now highest in Africa where it has a prevalence of 57% in older adults. 10 This burden is highest in people aged 45 to 69 years.9,10 Despite the high burden of hypertension in Africa, the awareness, treatment, and control are lowest in Africa, particularly in rural areas. 11
Hypertension remains an important cause of death in Ghana according to a systematic review. 12 According to the Ghana Demographic and Health Survey (GDHS) in 2014, hypertension has a prevalence of 13% amongst adults with 40.5% on treatment and only 23.8% of hypertension under control. 13 According to a survey by Dosoo et al in the middle belt of Ghana, less than half of hypertensives were aware of their condition with an overall hypertension prevalence of 28.1%. 14
The May Measurement Month (MMM) initiative was adopted by a group of doctors and public health personnel in Ghana for early detection for appropriate management to prevent complications. The May Measurement Month initiative, led by the International Society of Hypertension (ISH) and endorsed by the World Hypertension League (WHL) targets to screen 1% of the population in each participating country for hypertension. The prevalence of hypertension amongst participants determined during the global MMM campaign in 2018 was 33.4%. 15 Furthermore the prevalence determined during the global 2019 MMM campaign was 34% amongst participants with 23% of participants having untreated or poorly treated hypertension. 16
In Ghana, a total of 6907 participants were screened for hypertension with a prevalence of 34.1% in 2018. 17 The prevalence of hypertension in the Ashanti region of Ghana during the MMM 2019 survey is however not known. We, therefore, set out to report the findings of the MMM 2019 survey conducted in the Ashanti region of Ghana.
Methods
Study design and site
May Measurement Month 2019 is a global cross-sectional survey of adults aged 18 years and above who consented to participate in the screening exercise. Ghana was 1 of 92 countries to participate in this global awareness and screening campaign in May 2019.
This community-based cross-sectional study was conducted in the Kumasi metropolis of the Ashanti region of Ghana. The Ashanti region is one of the most populated of the 16 regions of Ghana. It is centrally located in the middle belt of Ghana. The Ashanti region has 530 health facilities. The Ghana Health Service operates 170 of these facilities, 281 are operated by private institutions, and 71 are operated by missions. 18 The region had a doctor-to-patient ratio of 1:7848. Kumasi, the economic and commercial hub of the region, is its capital and second-largest city in the country. Kumasi is located about 270 km north of Accra. It has a population density of 5552 persons per square kilometer. 18 Kumasi has the second-largest teaching hospital in Ghana, a regional hospital, and a host of district hospitals, clinics, and health care centers providing healthcare to all its inhabitants.
The survey was conducted from 1st to 31st May 2019 during the MMM campaign at 33 different screening sites. The screening sites included areas of mass public gathering including religious, social, and political events in May.
Study population
The study involved adults aged 18 years and above who consented to participate in the study. Participants were recruited via opportunistic sampling.
Data collection, processing, and analysis
The awareness campaign was organized before May in the whole metropolis via radio, television, and social media. Four hundred (400) volunteers were trained with training materials made available by the International Society of Hypertension (ISH). The study was coordinated by a team of researchers and health professionals. Data was collected on a simple and easy-to-understand questionnaire internationally standardized and provided by the ISH. Data collected included data on demography, medical history, and where possible, the weight and height were measured using a weighing scale and stadiometer respectively. Weight and height were estimated in places where volunteers were overwhelmed and measurement was not feasible. Blood pressures of participants were measured 3 times ideally by volunteers after following all recommended precautions.
Data collection was incomplete in some instances and as such, there was missing data for some variables which were not included in the analysis. We, therefore, used the term “respondents” for participants who responded to a specific question to account for the variations in denominators in some of the variables collected.
Hypertension was defined as systolic blood pressure ⩾140 mm Hg, or diastolic blood pressure ⩾90 mm Hg (mean of the second and third readings), or taking antihypertensive medication. All participants with systolic blood pressure higher than 140 mm Hg and/or diastolic blood pressure higher than 90 mm Hg were referred to the nearest hospital.
Data analysis
The data were analyzed using Stata/SE 14.0 statistical software (StataCorp. 4905 Lakeway Drive Station, Texas 77845, USA). Descriptive statistics were done for all variables and when normally distributed, continuous variables were expressed as means and standard deviations. Categorical variables were also expressed as percentages. Participants with normal blood pressure readings were compared with participants with high blood pressure readings as defined in this study. Simple logistic regression was done to identify the predictors of hypertension in the independent variables. The independent factors that were found to be statistically significant with P value of less than .05 were then included in the analysis and multiple logistic regression done to establish the predictors of raised blood pressure. The odds ratio and 95% confidence interval were determined for the independent variables including age, obesity, BM1, history of alcohol intake, history of hypertension in pregnancy and a known history of hypertension. These were expressed in tables after the analysis. A P-value of less than .05 was defined as statistically significant.
Ethical Considerations
Ethical approval was obtained nationally from the Ethics Review Committee of the Ghana Health Service before starting the awareness and screening campaign. Informed consent was also obtained from all participants.
Results
There were 3080 participants involved in the MMM 2019 campaign. The majority (76.2%) of the blood pressure measurements were done outdoors. The mean age of participants was 39.8 ± 16 years. There were 1835 (59.6%) females. The majority (84%) of participants had no prior participation in the MMM 2018 campaign. The majority (86.0%) of participants had no known history of hypertension and 90 (2.9%) had a history of diabetes mellitus. More than a quarter of respondents (27.9%) had never had their blood pressure checked. Many of the respondents with a history of hypertension were either on monotherapy (38.3%) or dual therapy (38%) for blood pressure control (Table 1).
Demographic and baseline characteristics of participants surveyed.

Abbreviations: BP, blood pressure; MMM, may measurement month; n, number; SD, standard deviation.
We found the prevalence of hypertension to be 27.3% among participants. This included respondents with a history of hypertension—430 (14.0%) and respondents with blood pressure measurements greater than or equal to 140/90 mm Hg—599 (21.3%) or both. Two-thirds of 397 (66.3%) of participants with high blood pressure measurements were unaware of their condition and only 149 (49.5%) of participants with history of hypertension on medication had their blood pressures controlled (Table 2). The mean body mass index (BMI) of participants was 26.0 ± 5.3 kg/m2. There were 859 (33.6%) participants who were overweight and 513 (20.1%) were obese. The mean heart rate was 79.1 ± 11.33 beats per minute and mean systolic and diastolic BP measurements were 123.9 ± 20.0 mm Hg and 77.1 ± 12.4 mm Hg respectively.
The examination findings of participants involved in the survey.
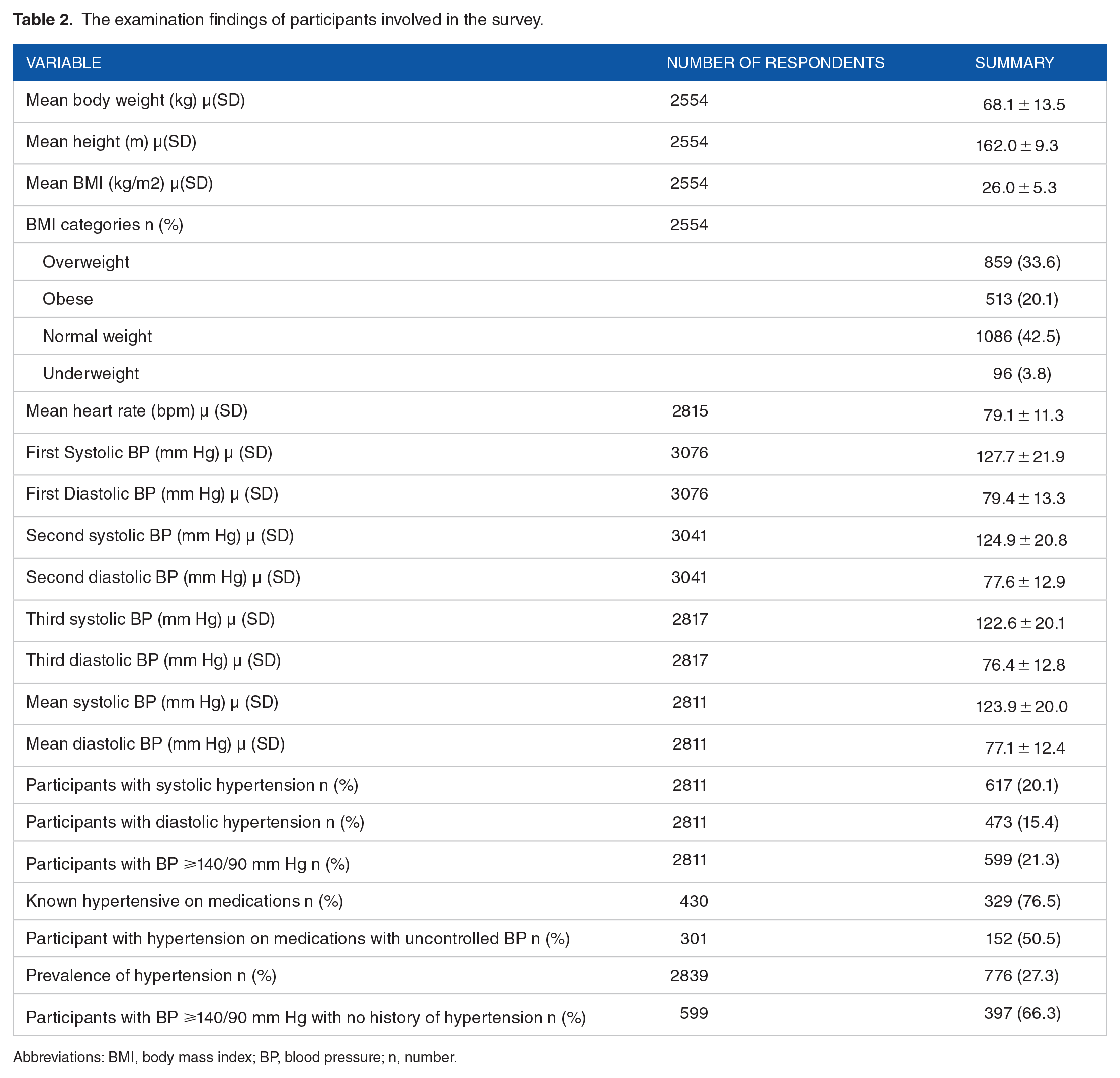
Abbreviations: BMI, body mass index; BP, blood pressure; n, number.
Analysis of those with a high blood pressure reading as compared to those with normal blood pressure showed that those with measured high blood pressure readings were significantly older than those with normal blood pressure (51.9 ± 16.0 vs 36.5 ± 15.7, P < .001). There was a significant association between those with high blood pressure concerning age, history of hypertension in pregnancy, obesity, and history of stroke as compared to participants’ normal blood pressure in the study (Table 3). The predictors of hypertension in a multiple logistic regression were increasing age (OR = 1.05 (CI 1.04-1.06), P < .001), history of hypertension (OR = 1.89 (CI 1.33-2.68) P < .001), and high body mass index (OR = 1.06 (1.02-1.10), P = .005) (Table 4).
Comparison of participants with high blood pressure with those with normal blood pressure.

Abbreviations: BP, blood pressure; kg, kilogram; m2, meter squared; n, number; ; SD, standard deviation; µ, mean.
Multiple logistic regression to determine predictors of hypertension after simple logistic regression.
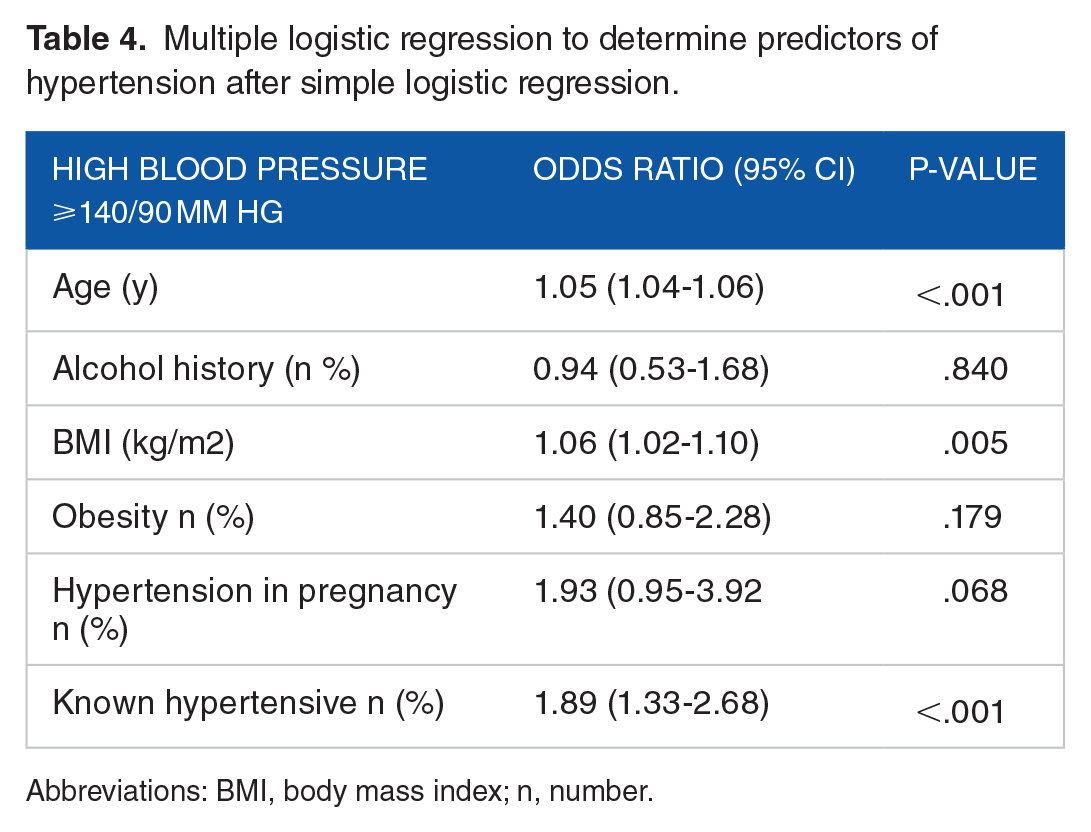
Abbreviations: BMI, body mass index; n, number.
Discussion
This was the second hypertension awareness campaign in the Ashanti region of Ghana after the debut campaign in the year 2018. We found that the prevalence of hypertension was 27.3% in 2019. Two-thirds of those with high blood pressure were unaware and about half of those with a history of hypertension target did not have optimum blood pressure readings.
The prevalence of hypertension in the Ashanti region was found to be higher than the Ghana national prevalence of 25.9% in MMM 2019 but lower than that global prevalence of 34.1% in MMM 2019. 19 Out of the total number of MMM 2019 participants with hypertension, only a third (33.7%) of them were aware of their status, this is less than the national average of 36.5% 19 and the global average of 58.7%. 15 These results indicate that there is a relatively higher prevalence of hypertension and a lower awareness level of the condition in the Ashanti region of Ghana compared to the national average. The factors that may contribute to this include the urban-rural disparities in hypertension prevalence and awareness within urban and more populated areas like the Ashanti region where higher prevalence but lower awareness of hypertension were recorded.
Over half (50.5%) of participants with hypertension on medication had poorly controlled blood pressures and this was higher than the reported global proportion of 31.7%. 16 Hypertension control in sub-Saharan Africa has proven to be the worst in the world. Poorly controlled blood pressures can be attributed to a host of factors; doctor-related, patient-related factors, and even poor public health policies. Lack of regular screening campaigns contributes to poor control of hypertension hence the relevance of blood pressure campaigns such as MMM. Poor awareness of hypertension as evidenced by this study can also contribute to poor BP control. Other factors that may contribute to poor control of BPs include lack of access to the various types of antihypertensives, significant comorbidities, poor adherence to treatment, and lack of governmental commitment among others.20-22
The present study found a strong positive association between hypertension and risk factors such as increasing age and increased BMI. Higher rates of hypertension are recorded in the aged compared to younger individuals. Increasing age is one of the non-modifiable risk factors for hypertension and is evidenced in this study. 23 Another very important risk factor for hypertension that was highlighted in this study was increasing BMI. 24 Obesity and increased BMI were identified as predictors of high blood pressure. Body mass index is a reflection of one’s lifestyle in most cases, elevated BMI has also been associated with a host of medical conditions including hypertension. Weight loss has been shown to significantly reduce blood pressure and some authors have suggested that it is causally associated with hypertension. BMI has been projected to rise exponentially in areas such as the Ashanti region with the urbanization of cities in sub-Saharan Africa (SSA) and the amplification and adoption of western lifestyles. 25 This can have damming effects on the health of the population as increasing BMI will become a major cardiovascular disease risk factor in SSA.
The MMM19 campaign has become increasingly relevant in the Ashanti region of Ghana as it brings to light the need for blood pressure awareness and screening campaigns, especially in urban areas.
Limitations
The campaign was mainly aimed at measuring the blood pressures of individuals and the convenient sampling used led to selection bias making the data less likely to be representative of the entire population. The research protocol was adopted from the International Society of Hypertension’s MMM protocol used worldwide. Data was not fully recorded for all participants, hence the total number of respondents for each specific data variable differed. Since it was not an interventional study, participants found to have raised blood pressures or even hypertensive urgencies or emergencies were not treated. However, participants found to be hypertensive were given lifestyle and dietary advice and referred to the nearest hospitals for expert care. In some cases, the weight and height of participants were estimated, this might reflect poorly on the measured BMI and its association with hypertension. Other possible risk factors for hypertension such as dietary salt intake and physical activity were not assessed by this study
Conclusion
This study highlights the enormity of the burden of hypertension in the Ashanti region of Ghana. The increased prevalence of this condition relative to the national and international average emphasizes the need for increasing blood pressure screening and awareness campaigns such as the MMM and supports calls for population-based strategies to address the burden of hypertension in Ghana.
Footnotes
Acknowledgements
We like to thank all our volunteers who dedicated their efforts to making this hypertension screening exercise an overwhelming success. We are most grateful for your support.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
All authors contributed in planning and data collection. EKT, OON, YAB, GO, LAP, EO and SOK drafted the initial manuscript. DA, FAK, EXA, OON designed the methodology. GJA, EXA, FAK, KAB, EO and MOA analyzed the data. All others contributed in review and additional contribution to the write up. All authors approved of the final version of manuscript and can affirm to the accuracy and integrity of the work
Ethical Approval
Ethical approval was obtained nationally from the ethics review committee of the Ghana Health Service in Accra-Ghana before the commencement of the national MMM campaign
Guarantor
Obed Ofori Nyarko