
Abstract
Prompt and effective chest compressions is the cornerstone cardiopulmonary resuscitation and has been found to improve cardiac arrest outcomes. Despite being rare, a wide variety of cardiac and pulmonary complications due to chest compressions have been identified. We present a case of a young, otherwise healthy female developing toxic shock syndrome and ultimately cardiac arrest requiring chest compressions found to cause right atrial and ventricular collapse on echocardiography.
Keywords
Introduction
Cardiopulmonary resuscitation (CPR) is lifesaving in cardiac arrest patients and begins with prompt and effective chest compressions. 1 Despite being the cornerstone of CPR, chest compressions have been found to cause a wide variety of cardiac and pulmonary complications including myocardial rupture, contusions, and pneumothorax. 2 We present a case of a young, otherwise healthy female developing toxic shock syndrome and ultimately cardiac arrest requiring chest compressions. Due to CPR, we find a rare complication of right atrial and ventricular collapse.
Case Presentation
A 42-year-old female with no medical history presented to the emergency department (ED) complaining of worsening shortness of breath. Three days prior she visited an urgent care center with similar complaints and was diagnosed with the influenza A virus and sent home. In the emergency department, she was in significant respiratory distress and was unable to speak in complete sentences due to increased work of breathing. Vital signs on presentation were a temperature of 106 degrees Fahrenheit, respiratory rate of 32 breaths per minute, heart rate of 128 beats per minute, blood pressure of 89/66 mm Hg, and oxygen saturation of 69% to 73% on room air. Laboratory testing revealed a troponin level of 0.02 ng/mL (normal value <0.04 ng/mL), lactic acid of 6.6 mmol/L (normal value 0.5-2.0 mmol/L), and procalcitonin level of 34.46 ng/mL (normal value <0.5 ng/mL).
Shortly after presentation she had pulseless electrical activity (PEA) on telemetry and advanced cardiac life support was initiated. She was emergently intubated and return of spontaneous circulation (ROSC) was achieved after 4 minutes of cardiopulmonary resuscitation (CPR). An emergent chest X-ray was obtained suggestive of a right sided lower lobe infiltrate and possible effusion (Figure 1). She was started on broad spectrum intravenous antibiotics with vancomycin and imipenem and blood cultures were sent. Due to persistent hemodynamic instability unresponsive to fluid resuscitation, she was started on norepinephrine, vasopressin, epinephrine, and phenylephrine to maintain and mean arterial pressure >65 mm Hg. Ventilator settings at this time were a rate of 24, tidal volume of 500, fraction of inspired oxygen of 100%, and positive end expiratory pressure of 12. A bedside ultrasound FAST exam was performed showing no free fluid but loculated fluid collection by the liver. An emergent 36-French chest tube was placed on the right side which yielded an immediate rush of air followed by 400 mL bloody fluid. Electrocardiogram at this time showed an accelerated junctional rhythm (ventricular rate of 104 beats per minute), without ST-segment elevations (Figure 2). A repeat chest X-ray was obtained to confirm chest tube placement and showed improvement of effusion in the right lung (Figure 3).

Chest X-ray after intubation showing right lower lobe infiltrates and effusions.

Electrocardiogram after ROSC showing accelerated junctional rhythm.
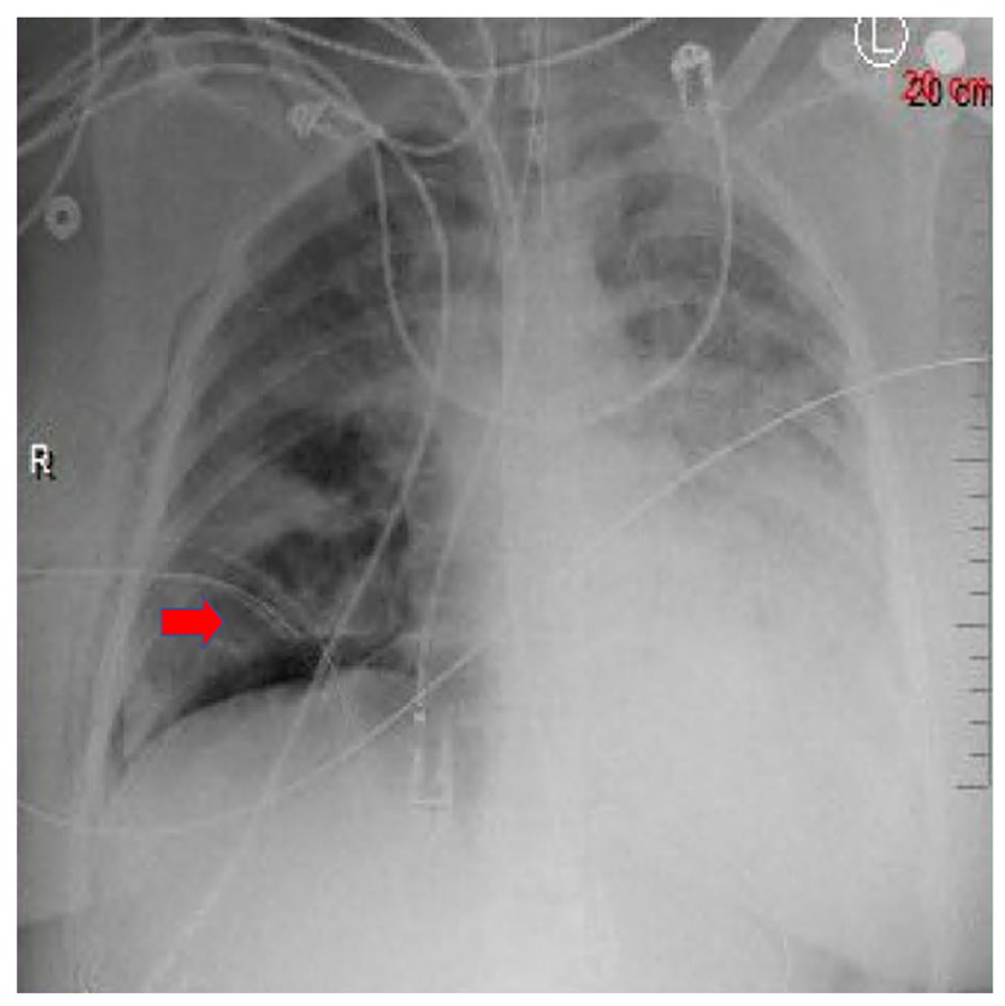
Chest X-ray showing placement of chest tube (red arrow) and improvement of effusion in the right lung. No fractures of the ribs were appreciated.
Within an hour, the patient had another episode of PEA and CPR was initiated for 2 minutes prior to achieving ROSC. Repeat laboratory testing was significant for a troponin level of 0.77 ng/mL. An emergent echocardiogram was performed after obtaining ROSC and showed an ejection fraction of 60% to 65% and a large mass extrinsic to the heart causing severe compression to the right ventricle and atrium (Figure 4). After stabilization, she was transferred to the intensive care unit for further management. The following day, her blood cultures grew gram Group A Streptococcus pyogenes and she was changed to an antibiotic regimen of penicillin G, 4 million units for 1 dose followed by 3 million units every 6 hours intravenously, and clindamycin 900 milligrams every 8 hours intravenously. She was also given 1 dose of 89 grams of intravenous immunoglobulin (1 gram per kilogram body mass) for suspected toxic shock syndrome leading to multiorgan failure. The following morning, she had another episode of PEA and, despite CPR and aggressive efforts, she ultimately succumbed to her condition.
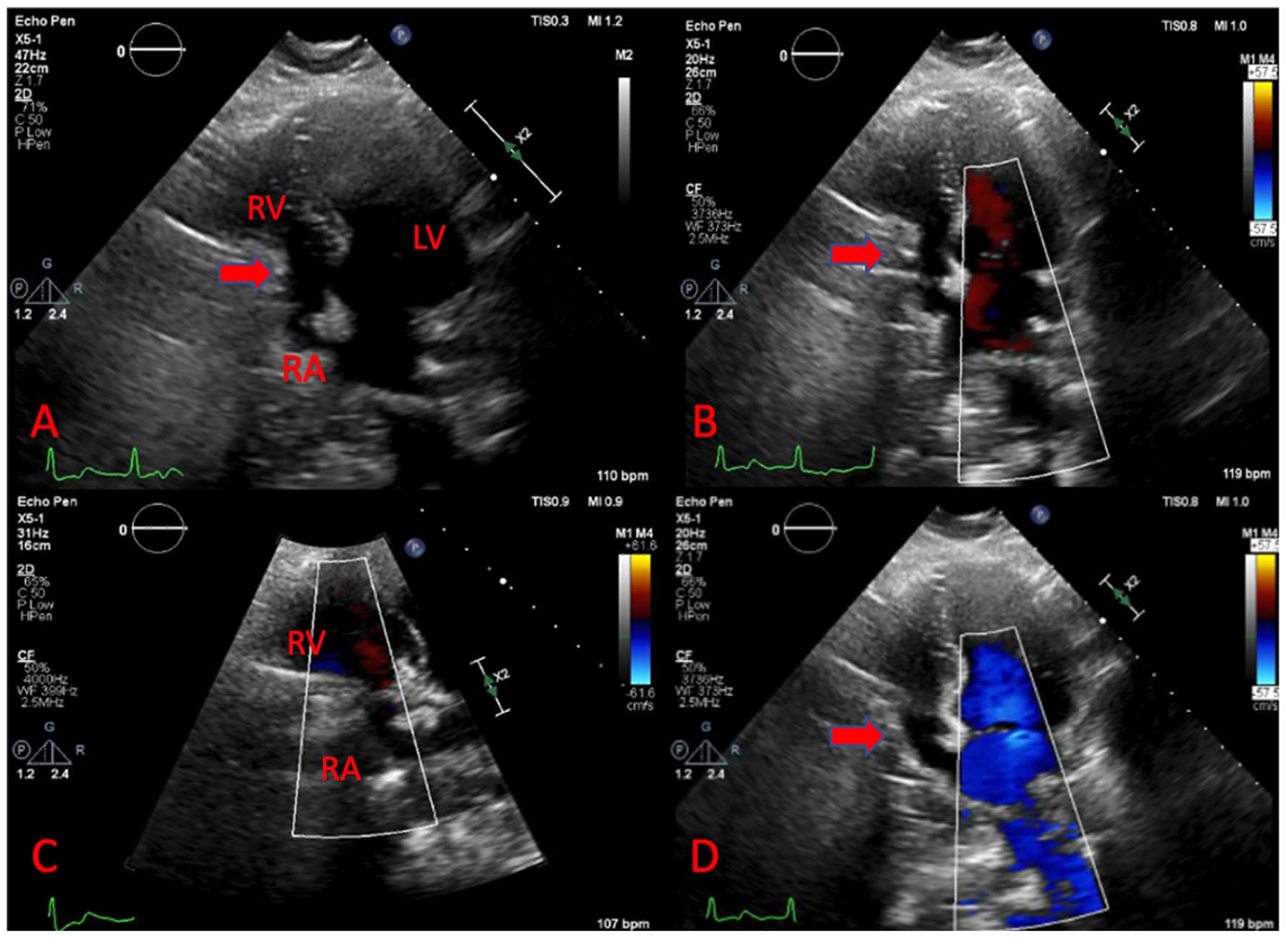
Echocardiogram showing right atrial and ventricular collapse after chest compressions and ROSC was achieved.
Discussion
The American Heart Association has developed guidelines expressing the importance of chest compressions in CPR. Despite the purposed benefit, only 22.3% to 25.5% of patients who have an in-hospital cardiac arrest survive. 3 In addition to a high mortality rate associated with cardiac arrest, chest compressions have been also found to cause a wide range of complications in up to 45% of cardiac arrest patients undergoing standard CPR. 2 Some more severe complications such as left and right ventricular collapse or rupture have also been reported after chest compressions.4,5
In our presented case of a young, otherwise healthy female, echocardiography after ROSC was obtained revealed both right atrial and ventricular collapse. While this phenomenon has previously been described in literature, cardiac rupture and chamber collapse as a complication of chest compressions has been rarely reported. 2 The mechanism of cardiac rupture or collapse post chest compressions is still not fully understood but has been suggested to be due to thoracic wall injuries such as rib and sternal fractures, cardiac tamponade, or a weakened myocardium.2,6,7 However, our patient did not have any fractures noted on chest X-ray and did not have cardiac tamponade or pericardial fluid collection appreciated on echocardiogram. Our patient likely suffered cardiac arrest due to multi-organ failure secondary to toxic shock syndrome from Group A Streptococcus. 8 The right-sided cardiac collapse could have also been due to the hemopneumothorax observed in this patient, confirmed by the rush of air and blood after chest tube placement. Hemopneumothorax can be a complication of chest compressions and if large enough can lead to pressure against the cardiac chambers. Treatment for cardiac chamber collapse usually revolves around the underlying cause such as pericardiocentesis in cardiac tamponade, cardiogenic shock management, or chest tube placement to resolve a hemothorax such as in our presented case.
Regardless of the cause, cardiac compression leading to chamber collapse can make resuscitation futile and can add to the already elevated morbidity and mortality. Bedside evaluation using ultrasound and echocardiography as done in this case after achieving ROSC can lead to prompt recognition of such chest compression complications.
Conclusion
Despite being an uncommon finding, it is important for healthcare providers to be aware of complications from chest compressions during CPR including cardiac rupture and chamber collapse. Prompt evaluation using bedside ultrasound and echocardiogram after patient stabilization could be used to detect these complications and allow for emergent management to prevent further morbidity and mortality.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Steven Douedi: Writing – original draft, review, and editing. Matthew Meleka – visualization, review and editing. Steven Daniels – visualization, review and editing. All authors have given final approval of this manuscript to be published.
Ethical Approval
The patient’s next of kin has given their informed consent to publish this case (including publication of images).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.