
Abstract
Background:
Coronary artery disease is the leading cause of mortality in India. There is scarcity of data on demographic profile and outcomes of acute coronary syndrome (ACS) in low socioeconomic status (SES) population of India.
Objectives:
This study was undertaken to determine the clinical presentation, management strategies, and in-hospital outcomes of ACS in low SES population.
Methods:
We conducted 1-year prospective observational cohort study of ACS patients admitted at Employees State Insurance Corporation unit of our tertiary care cardiac center. Clinical parameters, management strategies, and in-hospital outcomes of 621 patients enrolled during the study period from February 2015 to January 2016 were studied.
Results:
Mean age of patients was 56.06 ± 11.29 years. Majority (62%) of the patients had ST elevation myocardial infarction (STEMI), whereas Non-ST elevation acute coronary syndrome (NSTE-ACS) was seen in 38% of the patients. Median time from symptom onset to hospital admission was 285 min with wide range from 105 to 1765 min. Coronary angiography was performed in 81% of patient population. Single-vessel disease (SVD) was the most common pattern (seen in 43.3%) of coronary artery involvement with left anterior descending coronary artery (LAD) being the most frequently involved vessel (62.8%). Pharmaco-invasive approach was the preferred strategy. Overall percutaneous coronary intervention (PCI) rates were 59.1% (62.1% in STEMI and 54.2% in NSTE-ACS). Overall in-hospital mortality was 3.2%, being significantly higher in STEMI (4.2%) as compared with NSTE-ACS (1.7%).
Conclusions:
With implementation of evidence-based pharmacotherapy and interventions, outcomes comparable with developed countries can be achieved even in low SES populations of developing world.
Keywords
Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide, accounting for about 31% of global deaths. About three quarters of these deaths occur in low-income and middle-income countries. 1 Compared with the high-income countries, ischemic heart disease (IHD) in low- and middle-income countries is characterized by premature onset and high case fatality rate. 2 In India, CVD is responsible for about 27% of all deaths. The age-standardized death rate from CVD in India is 272 per 100 000 population as compared with global average of 235 per 100, 000 population.1,2
Various studies have shown that CVD mortality and morbidity have strong association with socioeconomic status (SES).3-7 Patients with low SES have higher mortality and morbidity rates as compared with those with high SES. This has been attributed both to higher prevalence and/or poor control of cardiac risk factors like hypertension, diabetes, smoking, and dyslipidemia; and to unequal access to medical facilities including invasive treatment. However, most of these studies have been from high-income countries. There have been few studies from low- and middle-income countries which have the highest burden of CVD, and these studies have shown inconsistent results.8,9
We had an opportunity to study the spectrum of acute coronary syndrome (ACS) in a low socioeconomic cohort population as 1 unit of our tertiary care center (Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bengaluru, India) is operating in ESIC (Employees’ State Insurance Corporation) Hospital premises, Bengaluru. ESIC hospitals in India provide exclusive cashless treatment to persons and their families insured under the scheme. ESIC act of Government of India is applicable to establishments (mostly nonseasonal factories) who employ 10 or more individuals with upper wage limit of each individual being Rs 21 000/month (305 US$/month). 10 In this article, we discuss the clinical characteristics, management strategies, and in-hospital outcomes of our cohort of low SES population.
Materials and Methods
Setting, study population, and operational definitions
This was a prospective observational descriptive cohort study conducted at ESIC unit of our tertiary care cardiac center. Methodology and results involving the comparison of diabetic and nondiabetic patients in this study has been published previously. 11 In brief, patient population consisted of consecutive ACS patients aged ⩾ 18 years who were referred to our center by the ESIC dispensaries located in the nearby geographic area and were admitted at our center. Patients were included in the study only if they belonged to low SES as assessed by Kuppuswamy classification. 12 Data were collected for a period of 12 months from February 2015 to January 2016. Patients were classified as having ST elevation myocardial infarction (STEMI) or Non-ST elevation acute coronary syndrome (NSTE-ACS) according to American College of Cardiology/American Heart Association (ACC/AHA) definitions.13,14 To ensure uniformity of data, standard definitions were used for the following:
Hypertension: self-reporting of physician diagnosis of hypertension and/or on antihypertensive medications, systolic blood pressure ⩾ 140 mm Hg, or diastolic blood pressure ⩾90 mm Hg.
Diabetes mellitus (DM): self-reporting of physician diagnosis of DM and/or on antidiabetic medications, fasting glucose levels > 126 mg/dL, or glycated hemoglobin levels > 6.5%.
Dyslipidemia: self-reporting of physician diagnosis of dyslipidemia and/or on treatment for dyslipidemia, high-density lipoprotein cholesterol (HDL) level < 40 mg/dL (men) or <50 mg/dL (women), and triglyceride level > 150 mg/dL, serum total cholesterol > 200 mg/dL or low-density lipoprotein cholesterol (LDL) level > 130 mg/dL.
Past history of IHD: prior typical angina, history of admission for ACS, prior percutaneous coronary intervention (PCI), or coronary artery bypass surgery (CABG).
Smoking: patients were considered as smokers if they reported any smoking/tobacco consumption within last 1 year of study enrollment.
Patients having concomitant valvular heart disease, cardiomyopathy, pericardial disease, and congenital heart disease were excluded from the study. Coronary angiography was performed using standard technique within 24 h of admission unless contraindicated. Coronary angiograms were analyzed by 2 expert cardiologists. Significant CAD (coronary artery disease) was defined as >50% diameter stenosis in a coronary artery which is at least 2 mm in diameter. Patients were accordingly classified as having single-vessel disease (SVD), double-vessel disease (DVD), or triple-vessel disease (TVD). 15 PCI and CABG were performed in eligible candidates as per standard practice and institutional protocol. Major adverse cardiovascular events (MACE) recorded in this study included in-hospital mortality, heart failure, cardiogenic shock, cardiac arrest, reinfarction, stroke, and major bleeding.
Ethical consideration
The study draft was approved by the institute’s ethics committee. Written informed consent was obtained from each patient. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Statistical analysis
Data were summarized as mean ± standard deviation (SD) if they were normally distributed; otherwise, they were summarized as the median (25th and 75th percentiles). Differences between groups were assessed using Chi-square or Fisher’s exact tests for categorical variables, student’s t-tests for continuous and normally distributed variables, and the Mann-Whitney U test for skewed variables. All analyses were considered significant at P < 0.05. The analysis was performed using SPSS software, version 23 (SPSS Inc., Chicago, IL, USA).
Results
A total of 651 eligible patients admitted with ACS were enrolled during the study period, 30 patients were excluded from the analysis due to incomplete data. Final data analysis was performed for 621 patients. Eighteen patients had 1 or more readmissions during the study period, and data from the index hospitalization was included in analysis in case of these patients.
Clinical characteristics and risk factors
Majority of the patients were men (75.8%). Overall mean age was 56.06 ± 11.29 years. Minimum age was 21 years and maximum was 97 years. Mean age in men was 54.5 ± 10.87 years, whereas in women, it was 60.97 ± 11.23 years (P = .000). Majority of the patients had STEMI (62%), whereas NSTE-ACS patients constituted 38% of the patient population. Median time from symptom onset to hospital admission was 285 min with wide range from 105 to 1765 min with no significant difference between STEMI and NSTE-ACS subgroups. Hypertension was the most common risk factor being present in 242 (39%) of the patient population. It was significantly more common in NSTE-ACS patients than in STEMI patients (50.4% vs 31.9%, P = .000). Diabetes was present in 231 (37.2%) of the patients being more common in NSTE-ACS than in STEMI (43.6% vs 33.2%, P = .009). Dyslipidemia was seen in 215 (34.6%) of the patients without any significant difference between STEMI and NSTE-ACS groups. Smoking was significantly higher in STEMI group (27.3%) than in NSTE-ACS (18.6%); P = .014. Majority of smokers were men (96.4%). Past history of IHD was more commonly present in NSTE-ACS group (39.8% vs 8.3%, P < .000).
Clinical characteristics and risk factor profile of the study population.
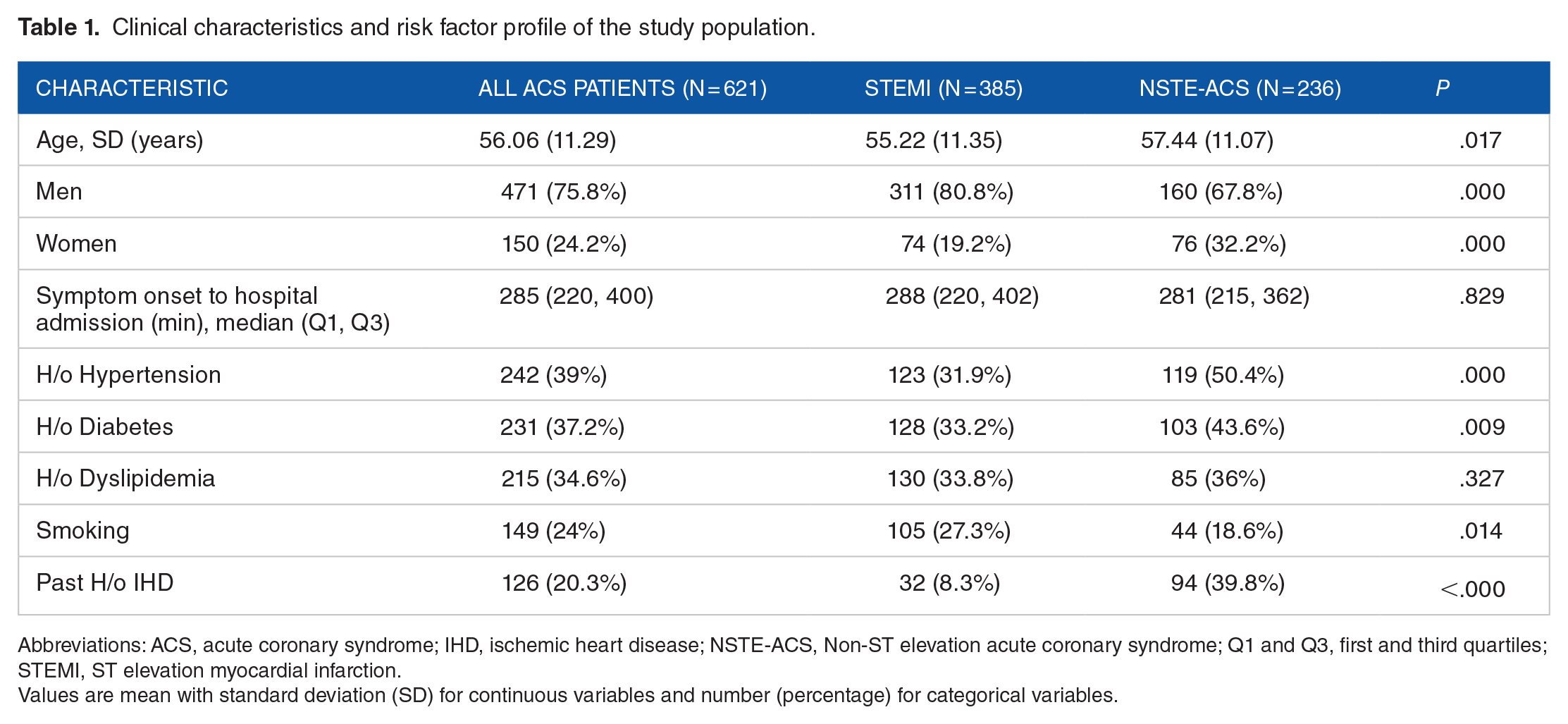
Abbreviations: ACS, acute coronary syndrome; IHD, ischemic heart disease; NSTE-ACS, Non-ST elevation acute coronary syndrome; Q1 and Q3, first and third quartiles; STEMI, ST elevation myocardial infarction.
Values are mean with standard deviation (SD) for continuous variables and number (percentage) for categorical variables.
Electrocardiographic profile
Electrocardiographically anterior wall myocardial infarction (MI) was the most common presentation in STEMI, being seen in 56.1% of the cases followed by inferior wall MI (35.3%). We also analyzed the prevalence of right bundle branch block (RBBB) and complete atrioventricular (AV) block in the patient population. The RBBB was seen in 9 patients (1.4%), all being STEMI. Complete AV block was also seen exclusively in STEMI (total 14 cases, 2.3%). Left bundle branch block (LBBB) was not analyzed separately as new-onset LBBB was considered as STEMI equivalent.
Angiographic profile of the patients
Out of 621 patients, 118 (19%) were managed noninvasively and 503 (81%) were subjected to selective coronary angiography within 24 h of admission. Most commons reasons for noninvasive management were deranged renal parameters, unwillingness of the patient, severe comorbidities limiting life expectancy, or moribund state. Normal epicardial coronaries or insignificant CAD was seen in 86 (16.9%) of the patients with no significant difference between STEMI and NSTE-ACS subgroups. The SVD was the most common pattern of coronary involvement and was seen in 218 (43.3%) of the patients. It was significantly more common in STEMI subgroup (49.5% vs 32.2%, P = .000). The DVD was seen in 103 (20.5%) of the patients with no significant difference between STEMI and NSTE-ACS subgroups. TVD was seen in 96 (19.1%) of the patients, being significantly more common in NSTE-ACS subgroup (29.4% vs 13.3%, P = .000). Left main coronary artery (LM) involvement was seen in 19 (3.8%) of the patient population. It was significantly more common in NSTE-ACS population (8.3% vs 1.2%, P = .000). The LAD was the most commonly involved vessel with significant stenosis being present in 316 (62.8%) of the overall ACS population. It was involved in 60.1% of STEMI cases and in 67.8% of NSTE-ACS cases. Right coronary artery (RCA) was the second most commonly involved vessel, being involved in 202 (40.2%) of the patients. Left circumflex artery (LCX) was involved in 161 (32%) of the patients. As in the case of LAD involvement, there was no significant difference between STEMI and NSTE-ACS in terms of RCA or LCX involvement.
Angiographic profile of the study population.

Abbreviations: ACS, acute coronary syndrome; CAD, coronary artery disease; CAG, coronary angiography; DVD, double-vessel disease; LAD, left anterior descending artery; LM, left main coronary artery; LCX, left circumflex artery; NSTE-ACS, Non-ST elevation acute coronary syndrome; STEMI, ST elevation myocardial infarction; SVD, single-vessel disease; TVD, triple-vessel disease; RCA, right coronary artery.
Values are expressed as number (percentage).
In-hospital management strategies
Mean hospital stay in our study was 3.89 days (3.95 days in STEMI patients vs 3.83 days in NSTE-ACS patients, P = .138).
In-hospital management strategies in the study population.

Abbreviations: ACS, acute coronary syndrome; ACE-Is/ARBs, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers; CABG, coronary artery bypass grafting; NSTE-ACS, Non-ST elevation acute coronary syndrome; PCI, percutaneous coronary intervention; STEMI, ST elevation myocardial infarction; UFH/LMWH, unfractionated heparin/low molecular weight heparin.
Values are expressed as number (percentage).
Reperfusion therapy was administered to 71.5% (275 out of 385) of STEMI patients. Predominant form of reperfusion was thrombolysis (mostly with streptokinase) being administered to 207 (53.8%) of STEMI patients, whereas primary PCI was performed in 68 (17.7%) of STEMI patients. Most common reason for nonperfusion was late presentation.
Aspirin was administered to 609 (98.1%) patients with no difference between the subgroups. Clopidogrel was the second antiplatelet drug in most patients, being administered to 605 (97.4%) of the patients. Statin use was also high, being administered to 610 (98.2%) of the patient population. As with aspirin, there was no significant difference in clopidogrel and statin use between STEMI and NSTE-ACS subgroups. Angiotensin converting enzyme inhibitors/angiotensin receptor blockers (ACE-Is/ARBs) were used in 451 (72.6%) of the patients, being more commonly used in STEMI subgroup (76.4% vs 66.5%, P = .007). β adrenergic blockers were used in 502 (80.8%) of the patients, their use being more common in NSTE-ACS subgroup (87.7% vs 76.6%, P = .000). Similarly, nitrate use was more common in NSTE-ACS population (71.2% vs 62.3%, P = .024). Heparin (either unfractionated or low molecular weight) was used in 570 (91.8%) of the patients with no significant difference between STEMI and NSTE-ACS subgroups.
PCI was performed in 367 (59.1%) of the overall ACS patients, 239 being STEMI patients and 128 being NSTE-ACS patients. There was no significant difference between STEMI and NSTE-ACS subgroups. Nearly all PCI patients received second-generation drug-eluting stents (DES). CABG was performed in 40 (6.4%) of the patients, 19 being STEMI patients and 21 being NSTE-ACS patients. There was no significant difference between STEMI and NSTE-ACS subgroups regarding CABG.
In-hospital MACE
Composite MACE occurred in 119 (19.2%) patients being significantly higher in STEMI subgroup (23.9% vs 11.4%, P = .000). Cardiac arrest was seen in 16 (2.6%) of the patients, being more common in STEMI than in NSTE-ACS (3.6% vs 0.8%, P = .014). Heart failure was noted in 50 (8.1%) patients with no significant difference between STEMI and NSTE-ACS subgroups. Shock was seen in 14 (2.3%) of the patients being significantly more common in STEMI subgroup (3.1% vs 0.8%, P = .031). Reinfarction during hospital stay was seen in 8 (1.3%) patients with no difference in STEMI and NSTE-ACS subgroups. Major bleeding was seen in 6 (1%) patients with no difference between STEMI and NSTE-ACS subgroups. Stroke occurred in 5 (0.8%) patients, 3 being STEMI and 2 being NSTE-ACS patients. Overall, 20 (3.2%) patients died during the course of hospitalization. There were significant more deaths in STEMI subgroup as compared with NSTE-ACS (4.2% vs 1.7%, P = .046).
Discussion
Clinical characteristics, risk factors, and electrocardiographic profile
This study provides a unique insight into the clinical presentation, in-hospital management, and outcomes of ACS in a low socioeconomic status cohort from urban India. In our study, the mean age at presentation was 56.06 ± 11.29 years. This is comparable with other studies in developing world like Gulf RACE registry 16 (56.4 ± 13 years), SPACE registry 17 (58 years), and with many studies from India such as CREATE registry 18 (56 ± 13 years), Jose and Gupta 19 study (57 ± 13 years), Sharma et al 20 (54.70 ± 19.90 years), but less than Kerala ACS registry (60.4 ± 12.1 years). 21 Mean age in our study was significantly lower than in Western studies such as European Heart Surveys (European Heart Surveys ) I 22 and II 23 (65.2 and 64.7 years, respectively), studies by Hochman et al 24 (69 years), and studies by Chang et al 25 (73 years).
In our study, mean age at presentation in female patients was significant more than male patients (60.97 ± 11.23 years vs 54.5 ± 10.87 years), similar to that observed in DEMAT registry. 26 In our study, men constituted 75.8% of the cases, whereas women constituted 24.2% of the cases. This skewed distribution which was more pronounced in STEMI subgroup can be attributed to gender bias and atypical presentations similar to that seen in CREATE registry, 18 Kerala ACS registry, 21 INTERHEART study and its South Asian cohort, 27 and ACCESS registry. 28
Our study had a higher proportion of STEMI cases among the ACS cohort, as observed in CREATE registry, 18 Kerala ACS registry, 21 and DEMAT registry. 26 This is in contrast to Western studies including The Second Euro Heart Survey, 23 GRACE registry, 29 and studies from Middle-East including GULF RACE 16 and SPACE registries. 17
Median time from symptom onset to hospital admission was nearly 5 h in our study, which is comparable with that in ACCESS registry from developing countries, but unlike ACCESS registry, there was no significant difference between STEMI and NSTE-ACS subgroups. Median time in our study was less as compared with that in CREATE registry 18 (about 6 h), but was considerably more than in Western studies (140-170 min) like GRACE registry, 29 and EHS I and II.22,23 The delay could be related to poor educational status leading to less awareness of the symptoms, traffic congestions, consultations with local practitioners, and delay in referral from local dispensaries.
Our study population had high prevalence of hypertension (39%), diabetes (37.2%), and dyslipidemia (34.6%) like many contemporary Indian studies such as Sharma et al 20 and Kerala ACS registry. 21 This is in sharp contrast to CREATE registry 18 where prevalence of hypertension and diabetes in poor cohort was 14.1% and 18.7%, respectively. This can be attributed to a reversal of social gradient (higher prevalence of risk factors in the low SES group) for CVD risk factors, which has already occurred in the urban areas of India, especially in industrialized metropolitan cities like Bangalore—the site of this study. 30
In this study, as compared with STEMI subgroup, NSTE-ACS patients were older, with larger proportion of women, and were more likely to have hypertension, diabetes, and previous IHD, but were less likely to be smokers. This is similar to observations made from global (GRACE registry, 29 European Heart Survey I and II)22,23 and national (CREATE) 18 registries.
In STEMI subgroup, anterior wall MI was more common than inferior MI similar to the study by Jose and Gupta. 19 These results, however, differed from study by Singh et al 31 where anterior and inferior MIs had similar frequency. Incidence of RBBB in ACS patients in our study was 1.4%, which is much less than 4% to 10% reported in Western studies.32-34 However, it is comparable with 2.5% reported in a small Indian study by Sahni et al. 35 Lower incidence could be related to late presentation time in our study as compared with Western studies and patients with STEMI and RBBB, who are generally more sick as compared with others, succumbing to complications of STEMI before reaching the hospital. The incidence of complete AV block in our study was 2.3% in overall population and 3.6% in STEMI population. This is slightly higher than in Western studies by Aguiar et al 36 (1.9% in ACS population) and Harikrishnan et al 37 (2.1%-2.3% in STEMI).
In-hospital management and outcomes
Reperfusion therapy was given to 71.5% of STEMI patients (53.8% thrombolysis, 17.7% primary PCI), which is better than reported in CREATE registry 18 (66.5%) and Kerala ACS registry 21 (53.4%), but inferior than in Gulf RACE registry 16 (91%) and GRACE registry (78%). 29 Rate of primary PCI is better than CREATE registry (8%) and Kerala ACS registry (12.9%), but is much less than Western studies like GRACE registry (40%), EHS-I (40%) and EHS-II (58%). These lower rates can be explained by lack of 24 × 7 primary PCI services at our center due to administrative issues and hence pharmaco-invasive strategy being adopted in many STEMI patients (which has been given class I recommendation in recent European Society of Cardiology [ESC] Guidelines for STEMI). 38
The use of guideline-recommended pharmacotherapy was quite high in our study including dual antiplatelet therapy (DAPT) that was administered to nearly all the patients. This usage is much higher than in many Indian studies and comparable with studies from the Western world. Coronary angiography rates in our study were much higher than CREATE registry, 18 Kerala ACS registry, 21 SPACE registry, 17 and equal to that in GRACE registry. 29
On coronary angiography SVD was the most common pattern in our study with LAD being the most commonly involved vessel. The preponderance of SVD was less marked in NSTE-ACS subgroup. These results are similar to many Indian studies like Deora et al 39 and Sharma et al. 20 One interesting finding in our study was the higher incidence of TVD (29.4%) than DVD (16.7%) in NSTE-ACS subgroup in contrast to other studies. PCI rates in our study were much higher than in older registries such as CREATE registry, 18 Kerala ACS registry, 21 GRACE registry, 29 and EHS-I, II22,23 and is comparable with data from contemporary Chinese NSTE-ACS registry. 40
Overall, MACE rates in our study was comparable with contemporary registries from Saudi Arabia (SPACE registry), 17 which used similar definition of MACE. But our MACE rates were higher than Kerala ACS registry, 21 largely due to lower rates of heart failure/cardiogenic shock in Kerala ACS registry. These differences could be due to difference in definition of heart failure and its clinical detection as heart failure is largely a clinical diagnosis. MACE rates in our study were higher in STEMI than NSTE-ACS, consistent with most of the registries. Overall mortality rate was low in our study (3.2%), slightly lower than that reported in Kerala ACS registry 21 (3.9%), Gulf RACE registry 16 (3.7%). Our mortality rates were much lower than mortality rates for poor population subgroup of CREATE registry 18 (8.2%). These differences are driven by higher use of PCI (59.1% vs 15.3%) and guidelines recommended medical therapy such as beta blockers (80.4% vs 58.8%), ACE-I/ARBs (72.6% vs 63.2%), and statins (98.2% vs 61.2%) in our study due to provision of cashless facility under the ESIC insurance scheme, whereas in CREATE registry, nearly 75% of patients paid from their own pockets for medications and hospital procedures.
Limitations
Noninclusion of certain risk factors like obesity, family history of premature CAD, and stress levels constituted an important limitation. Out-of-hospital events were not recorded in our study that could have led to underestimation of mortality rates. Being a single-center study involving low SES population, our results cannot be generalized. Another important limitation is the lack of assessment of the long term outcomes after discharge from the hospital.
Conclusions
In our study of ACS in a cohort of low SES urban Indian population, patients were younger at the time of index event as compared with the Western population. There is high prevalence of hypertension, diabetes, and dyslipidemia in low SES populations. There is large delay in this population in seeking medical care. The SVD is the most common pattern of coronary artery involvement. Use of evidence-based pharmacotherapy and invasive interventions was high in our study, which is associated with low in-hospital mortality, comparable with studies from developed countries.
Our study demonstrates that with better access to specialized cardiac care and provision of cashless insurance schemes for treatment, mortality and morbidity from acute coronary syndromes can be reduced in poor sections of the society. However, there is still scope of improvement by imparting health education to less-privileged population including prevention and control of CVD risk factors, recognition of signs and symptoms of ACS, and seeking early medical care.
In-hospital major adverse cardiovascular events (MACE) seen in the study population.

Abbreviations: ACS, acute coronary syndrome; MACE, major adverse cardiovascular events; NSTE-ACS, Non-ST elevation acute coronary syndrome; STEMI, ST elevation myocardial infarction.
Values are expressed as number (percentage).
Footnotes
Author Contributions
All authors made major contributions for this manuscript: protocol design NSS, SKKR, DR, KV, CNM, data acquisition NSS, SKKR, DR, data analysis and statistics NSS, SKKR, DR, KV, CNM, preparation and writing of the final version NSS, SKKR, DR, KV, CNM, and accept of final version NSS, SKKR, DR, KV, CNM.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.