
Abstract
This feature article for the thematic series on congestive heart failure (CHF) readmissions aims to outline important gaps in guidelines for patients with multiple comorbidities and the elderly. Congestive heart failure diagnosis manifests as a 3-phase journey between the hospital and community, during acute, chronic stable, and end-of-life (palliative) phases. This journey requires in variable intensities a combination of multidisciplinary care within tertiary hospital or ambulatory care from hospital outpatients or primary health services, within the general community. Management goals are uniform, ie, to achieve the lowest New York Heart Association class possible, with improvement in ejection fraction, by delivering gold standard therapies within a CHF program. Comorbidities are an important common denominator that influences outcomes. Comorbidities include diabetes mellitus, chronic obstructive airways disease, chronic renal impairment, hypertension, obesity, sleep apnea, and advancing age. Geriatric care includes the latter as well as syndromes such as frailty, falls, incontinence, and confusion. Many systems still fail to comprehensively achieve all aspects of such programs. This review explores these factors.
Introduction
Improvement in ejection fraction (RF) and congestive heart failure (CHF) class is the primary goal of management, and are associated with better prognosis. Doing so will also reduce readmissions.1,2 In the United States, prevalence of CHF is >5.7 million, with 670 000 new cases yearly. In Europe and globally, prevalence is >15 million and 37.7 million, respectively. 3 Congestive heart failure hospitalization rates are high, and it is the leading cause in patients >65 years of age, with more than 1 million primary presentations or 1% to 2% of all hospitalizations yearly. Annual Medicare expenditure in the United States exceeds US $17 billion.3–6 Following a CHF admission, 1 in 4 are readmitted within the first month and half within 6 months, where 80% of emergency room presentations are admitted.7–13 Matching funding to readmission strategies such as pay for performance or fee-for-service, which are either health system or client focused, has not generated the desired outcomes within traditional models of care. 13 In addition, presentations, readmissions, and costs for CHF are projected to increase by 50% by 2035.14–17
To achieve New York Heart Association (NYHA) functional class 1 with an improved EF, the early focus of pharmacologic therapies is now interwoven into a complex program with a range of services and therapies requiring multidisciplinary input. The OPTIMIZE-HF study showed that when such programs are used to deliver care, outcomes could be improved. 18 Studies also tell us that the gap between obtaining the highest class of evidence (Class 1A), the grade of recommendation, and the need to continually fine-tune evidence at the community level remains an understudied area. Thus, the future must in some fashion envision broader clarification in recommendations taking into account an aging population with multiple comorbidities.19,20 Could this be an important consideration when addressing readmissions?
More than half of CHF patients will suffer a concomitant comorbidity such as diabetes, chronic renal impairment (CRI), smoking-induced lung diseases, obesity, sleep apnea, hypertension, and atrial fibrillation (AF). 21 The elderly are also challenged by having greater comorbidities, psychological, and social vulnerability as well as geriatric syndromes such as falls, confusion, and frailty.22–24 It is not yet clear whether merely translating guidelines from a homogeneous randomized clinical trial to heterogonous population translates to improved outcomes and reduced hospital admissions. In this review, we explore CHF guidelines in the context of comorbid disease and advancing age focusing on opportunities to close the guideline gaps.
Understanding Registry and Trial Data in Translating Guidelines
Congestive heart failure still carriers a grave prognosis at all-time intervals, 30 days, 1, 5, and 10 years. 25 These differences can be greater across racial subgroups and global health systems. The etiology of CHF and associated risk factors also contributes to this. Although age-adjusted incidence, prevalence, and mortality are decreasing, the absolute number of patients are increasing as patients live longer. Postdischarge event rates remain high, whereas length of hospital stay is shorter for an increasingly complex patient cohort. Congestive heart failure is thus an epidemic, where rates are projected to increase, and uses resources on many fronts the most costly being hospitalizations.25,26 Table 1 summarizes the publications that have covered this in greater detail.
Summary of findings from key heart failure hospitalization registries.
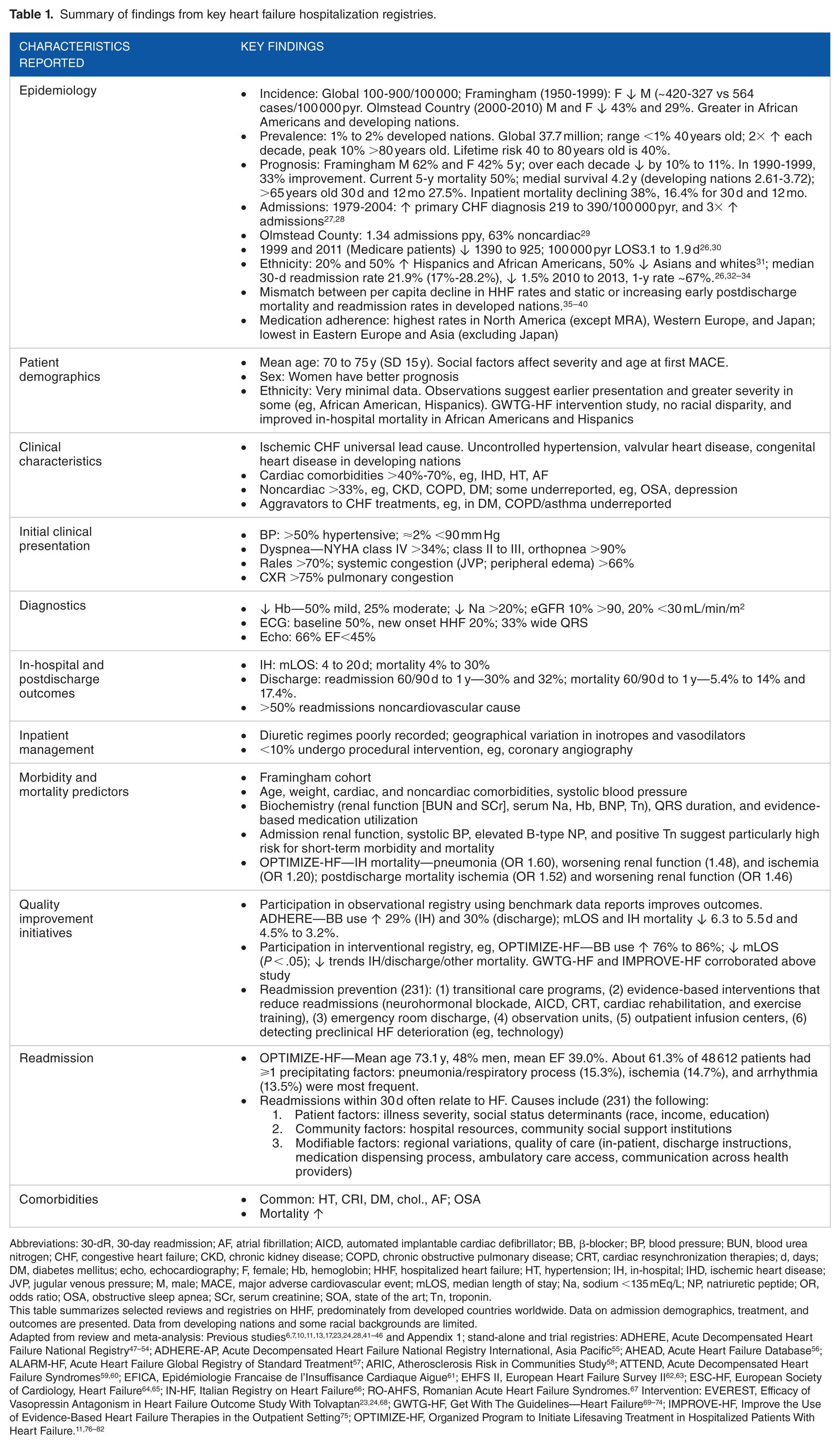
Abbreviations: 30-dR, 30-day readmission; AF, atrial fibrillation; AICD, automated implantable cardiac defibrillator; BB, β-blocker; BP, blood pressure; BUN, blood urea nitrogen; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CRT, cardiac resynchronization therapies; d, days; DM, diabetes mellitus; echo, echocardiography; F, female; Hb, hemoglobin; HHF, hospitalized heart failure; HT, hypertension; IH, in-hospital; IHD, ischemic heart disease; JVP, jugular venous pressure; M, male; MACE, major adverse cardiovascular event; mLOS, median length of stay; Na, sodium <135 mEq/L; NP, natriuretic peptide; OR, odds ratio; OSA, obstructive sleep apnea; SCr, serum creatinine; SOA, state of the art; Tn, troponin.
This table summarizes selected reviews and registries on HHF, predominately from developed countries worldwide. Data on admission demographics, treatment, and outcomes are presented. Data from developing nations and some racial backgrounds are limited.
Adapted from review and meta-analysis: Previous studies6,7,10,11,13,17,23,24,28,41–46 and Appendix 1; stand-alone and trial registries: ADHERE, Acute Decompensated Heart Failure National Registry47–54; ADHERE-AP, Acute Decompensated Heart Failure National Registry International, Asia Pacific 55 ; AHEAD, Acute Heart Failure Database 56 ; ALARM-HF, Acute Heart Failure Global Registry of Standard Treatment 57 ; ARIC, Atherosclerosis Risk in Communities Study 58 ; ATTEND, Acute Decompensated Heart Failure Syndromes59,60; EFICA, Epidémiologie Francaise de l’Insuffisance Cardiaque Aigue 61 ; EHFS II, European Heart Failure Survey II62,63; ESC-HF, European Society of Cardiology, Heart Failure64,65; IN-HF, Italian Registry on Heart Failure 66 ; RO-AHFS, Romanian Acute Heart Failure Syndromes. 67 Intervention: EVEREST, Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan23,24,68; GWTG-HF, Get With The Guidelines—Heart Failure69–74; IMPROVE-HF, Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting 75 ; OPTIMIZE-HF, Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure.11,76–82
Natural history of heart failure and the burden on health system
Progression of CHF or left ventricular (LV) recovery for any individual varies with the factors that influence the degree of ventricular remodeling and the causes.4,83 The greatest responders are seen with abnormalities in energetics, followed by toxins, and inflammatory cardiomyopathies. Readmissions are high when the remodeling process negatively affects systolic function.25,26,84,85 All cases will follow a 3-phase terrain of lifetime readmission risk with the highest risk “transition phase” and “palliative phase” and lowest in “plateau phase” (Figure 1). 86 The cost of HF care accumulates largely from repeated hospitalization, because ambulatory care for complex CHF, with comorbidities and for elderly patients are yet to find the most cost-efficient model.5,87

Natural history of heart failure (HF). Diagram demonstrates a 3-phase process once HF is diagnosed. The natural history of HF is chronological progression of left ventricular remodeling, manifesting with symptoms, physical morbidity, and early death. HF readmissions, presenting as acute decompensation, have greatest risks in the transition and palliative phases. The transition forward to more advanced phases is influenced by rate of recovery and normalization of LV function in correlation to the starting point of prior screening (black arrow), early treatment (blue arrow), and through its natural history (read arrow), and the type of cardiomyopathy, energetic defects > toxins > inflammatory causes. The slope of the arrows highlights the trajectory and prolongations toward death. Terminology: (1) Normalization of LV function, defined as an EF ⩾50%; (2) recovery of LV function, defined as an improvement in LF ejection fraction from 5% to 15 %; normalization occurs less frequently than recovery of LV function.
What have we learned from registries?
Most CHF cases are diagnosed in hospital and all patients will be admitted at some point. The past several decades have produced large, high-quality, multicenter registries, some with interventions that provided epidemiologic data as well as insight into the process of care (Table 1). The American Heart Association (AHA) has also published benchmarks for CHF taxonomy and clinical performance standards.88,89
Registries based on benchmarked data paired with interventions that optimize the delivery of proven strategies, alone, can deliver improvement in all performance measures such as readmissions and outcomes, largely through improved adherence to guidelines. Intervention tools include: evidence-based practice algorithms, standardized order sets, and discharge checklist; and access to specialist, with only 52% of Medicare patients receiving inpatient review when readmitted. Rewards-based system such as fee-for-service or award centers appear less significant. Gaps in authoritative data matching sociodemographics, comorbidities and older age support need for more heterogenous studies.13,90 Risk scoring tools are yet to deliver meaningful roles in clinical assessments.91–97
Heart Failure and Comorbidities
Early calls for recognizing multiple comorbidities 98 are increasingly factored in both American and European CHF management guidelines.99–102 Positions are also increasingly provided. There remain large gaps due to homogeneity of randomized clinical trials. Among Medicare beneficiaries, 68% have ⩾2 and 14% have ⩾6 chronic conditions,20,103–105 among beneficiaries with CHF specifically >40% to 55% have ⩾5 noncardiac comorbidities, which increase preventable and all hospitalizations proportionally.29,105–108 These points have consequences for management and guidelines. We focus on diabetes mellitus (DM), CRI, chronic obstructive pulmonary disease (COPD), sleep-disordered breathing (SDB), and obesity, where guidelines are yet to recommend (advocate) a specific as opposed to generic advice.
Significance of comorbidities, trial evidence, and impacts on readmissions
First, the Global Burden of Disease Study listed 17 primary causes, with two-thirds secondary to ischemic, hypertensive, rheumatic heart diseases, and COPD. Other causes include valvular, primary genetic/hereditary and acquired, secondary (systemic diseases) cardiomyopathies, congenital heart disease, and pericardial diseases. Causes are variably associated with greater comorbidities and association with socioeconomic status and developed nation status.5,90
Second, among 4 366 489 Medicare beneficiaries with CHF, the top ranked comorbidities are hypertension (85.6%), ischemic heart disease (72.1%), hyperlipidemia (62.6%), anemia (51.2%), DM (47.1%), arthritis (45.6%), CRI (44.8%), chronic airways disease (30.9%), and AF (28.8%). Many noncardiac conditions are excluded during the run in period of randomized controlled trials (RCTs).5,21,25,26
Third, in the clinical domain, a wider racial demography, female sex, and older population are managed, whereas data remain limited or or in some cases unreliable due to variations in case definition, sampling strategies, and enrollment. Observational evidence does support greater incidence in developing nations with greater comorbidities and disease burden, and socioeconomic disadvantage in some racial groups, eg, African Americans or even variations in disease patterns e.g women and East Asians.56,109
It is thus no surprise that patient and homogenous system delivery factors are both equally risk factors for readmission. How resources are allocated within the 8 categories and 34 subdomains of a disease management taxonomy could influence readmissions.11,89 A summary of some of these factors include: firstly there are varying complexities in CHF cohort including hospitalization, complexities of comorbidities or risk factors including male sex, advanced age, or disease (eg, low systolic blood pressure), cardiac comorbidity (myocardial ischemia, AF), noncardiac comorbidity burden (CRI, DM, anemia, COPD, hyponatremia), psychosocial well-being (depression, social support, literacy), noncardiac illnesses (respiratory tract infection, falls, and fractures), history and frequency of prior hospitalization, prescription of prognostic medications, patient-related/compliance factors (nonadherence, dietary indiscretion with salt and water with weight gain, and drug and alcohol abuse), iatrogenic factors (eg, use of nonsteroidal anti-inflammatory drugs), and system-related factors (insufficient access to follow-up care and rehabilitation, poor transitions of care);27,28,30,41–46,91,110–123 secondly poor correlation between existing readmission risk scores and translation in the clinical domain;92–97 thirdly, the finding that phenotypic variables other than EF, such as comorbidity or female sex, can determine outcomes, raising questions to broaden HF classification beyond left ventricular EF (LVEF).17,31,124
Diabetes mellitus
CHF contributes to DM morbidity and mortality through arterial diseases (especially coronary) and independently, ie, “diabetic cardiomyopathies,” an evolving term.32–34 Several points are however indisputable: (1) Epidemiology observations—greater chronology and severity of DM with all stages from prediabetes, metabolic syndromes, and established diabetes, risk of CHF ([hazard ratio 1.2 to 1.7] and [12.4 vs 30.9 per 1000 person-years]). 1 in 3 admitted patients shows new-onset impaired glucose tolerance and prevalence in registries range from 25% to 40%; (2) Prognosis—higher rates of mortality and hospitalizations; (3) Pathophysiology—alterations occur with structural changes in myocardium and vasculature, unfavorable imbalance in myocardial energetics, CRI, and other organ damage.34,125
Treatment guidelines highlight the need for excellent DM control but having glaring deficiencies beyond that. Optimal treatment options and dosing are based on limited evidence, often without accounting for potential interactions contributing to suboptimal regimes. Novel pharmacotherapies are also wanting, however, SGLT2 (sodium-glucose cotransporter-2) inhibitors, is one novel agent with potential revolutionary impact on CHF prevention in DM Strong public policy for education of cardiologists and general practitioners is required to help clinical translation. With existing drugs, vasodilator β-blockers, with distinct benefits, are not presently factored.35,36 Greater evidence is needed for benefits with metformin and sulfonylureas, safe insulin dosing, safety of thiazolidinediones, translation of DPP-4 inhibitors, and GLP-1 receptor antagonist (RAs).34,37,38 Finally, lifestyle modifications are addressed through cardiac rehabilitation or diabetic education and maintained through self-care are underutilized from poor funding; for example the Australian public health fund (Medicare) rebate is for limited duration and restricted to hospital specialist, disadvantaging community specialists and ambulatory patients. This lack of resourcing has not translated as a priority health policy issue. 35
Chronic renal impairment
The interaction between the failing heart and kidney is always bidirectional. This cardiorenal interaction now labeled “cardiorenal syndrome (CRS)” has been synthesized most comprehensively by Ronco et al. Short-term fluid and electrolyte imbalance, with long-term dysregulation of endocrine, sympathetic, immune (inflammatory) functions of the primary organ (heart or kidney), and secondarily every organ throughout the body contribute to a patient’s clinical presentation. 39 The Acute Decompensated Heart Failure National Registry (ADHERE) database of 175 000 admissions across the Unites States consolidated on the depth of a problem already suspected highlighted that, all grades of CRS contribute to pathology in the other. The risk increasing with baseline severity, where CRI is the single strongest predictor of CHF outcome even beyond LVEF. CRS is also under-detected, and prognostic CHF treatment is often suboptimally prescribed. 40
Guidelines have been cautious in taking strong positions on pharmacotherapies as advances in diagnostics have been slow. The estimated glomerular filtration rate (eGFR) is the most accurate estimate of CRI but lags by 2 to 7 days in predicting worsening CRI and cannot be used acutely to monitor renal function. Thus, using renin-aldosterone-angiotensin blockers when eGFR is between 20 and 45 mL/m becomes problematic. Novel renal function and injury biomarkers such as cystatin-C and neutrophil gelatinase–associated lipocalin have ongoing translational and cost-efficiency issues. 126 As optimizing conventional CHF therapies at lower eGFRs is difficult, a novel approach to prescribing may be required including agents with extracardiac benefits and targeting systemic factors such as autonomous sympathetic overactivity, nitric oxide deficiency, and endothelial dysfunction. 127 For acute heart failure, vasodilators (nesiritide; currently only selected patients), vasopressin antagonist (volume overload and resistant hyponatremia) 102 and novel agents (serelaxin and ularitide) offer alternative permutations for combination therapies in nephroprotection with CHF.47,128 We anticipate stonger positions in newer guidelines.
Chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease is present in a third of CHF cases, has an equal sex distribution despite a greater rate of smoking in men (suggesting greater susceptibility in women), and predicts mortality.32,48,49 Chronic obstructive pulmonary disease poses some unique challenges. First, it can be underdiagnosed due to underutilization of pulmonary function tests. Second, diagnostic challenges as the symptom of dyspnea is similar for both conditions. As pulmonary function tests are unreliable in acute settings, novel biomarkers such as B-type natriuretic peptide have been used, but more work is needed as up to 40% of respiratory distress are incorrectly admitted between cardiac and general medical units.50,51 Third, therapeutic issues such as underprescription of β-blockers in CHF while use of steroids and β-adrenergic agonist can enhance fluid retention and increase heart rates. The optimal cardioselective β-blockers is another area requiring attention. Finally, enrollment in cardiopulmonary, rehabilitation remains unclear.48,52–54
Obesity, Sleep-disordered breathing, and other comorbidities
Sleep-disordered breathing (SDB) which occurs in more than 1 in 3 HF patients, is part of a spectrum of metabolic-related conditions that are often overlooked. The common denominator is weight, where reduction targets are uniformly underachieved. Both forms of sleep apnoea are more prevalent in men and older age. Obstructive sleep apnea has greater correlations with weight and heart failure with preserved EF (HFpEF) and central sleep apnea with more severe CHF and AF. SDB is associated with greater readmissions and probably worse outcomes. The main treatment, continuous positive airway pressure effectively improves EF, physical function, and quality of life (QOL), but has issues with tolerability, and is yet to prove survival benefit.32,55,62–65,102
Obesity is a societal epidemic that is directly associated with CHF and indirectly through most CHF-associated comorbidity. It should be identified and treated with the same vigor as CHF and other comorbidities. However the resourcing involved prevents this, and so patients are at risk of accumulating additional comorbidities. Ideal body mass indices (BMIs) indexed for race are being defined. In one study, reference indices 26.5 to 30.9 kg/m2 had 27% improvement in mortality or hospitalization than those between <23.5 and >35 kg/m2. Cardiac cachexia, a contributor to mortality in lower weights, highlights the need for professional support in achieving weight reduction targets. With moderate degree of obesity (BMI <35 kg/m2), weight loss as a CHF treatment goal is not recommended. With greater obesity (BMI 35-45 kg/m2), tackling this issue with more advanced options such as bariatric surgery is showing benefits.61,66,67 Atrial, fibrillation, anemia, myopathy and deconditioning, depression, liver disease, frailty, and arthritis are other noncardiac comorbidities requiring considerations.32,48,102
Heart Failure in the Elderly
Defining elderly with a cutoff age of 70 to 80 years, registries have shown that >50% of acute HF admission (elderly - mean age 75 years or octogenarian ⩾80 years) range between 21% and 38%. Studies also demonstrate age differences in demography, clinical profiles and outcomes, comorbidities, and prognostic factors. Elderly presentations are >60% women, where 45% are new-acute HF, more likely associated with hypertension and AF, and less likely obese and diabetic. Respiratory distress is more common than peripheral edema, and atypical symptoms of sepsis, fever, confusion, fatigue, and loss of appetite are associated and added to the diagnostic difficulties (Table 2).13,22,23,56-60,68–82
Clinical characteristics of young versus elderly with acute heart failure (AHF).

Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blockers; BB, β-blocker; CS, cardiogenic shock; CV, cardiovascular; eGFR, estimated glomerular filtration rate; Hb, hemoglobin; JVP, jugular venous pressure; LA, left atrium; LV, left ventricle; MRA, mineralocorticoid receptor antagonists; NP, natriuretic peptide; NYHA, New York Heart Association; SBP, systolic blood pressure; SUN, serum urea nitrogen.
Table data from Brouwers et al. 22
Registries comparing prognostic medications with age such as IN-CHF (>70 years), OPTIMIZE-HF (>75 years), and EuroHeart Failure Survey II (EHFS II; >80 years) support significantly lower prescribing rates.13,23,68,73,74 Physiological differences with HFpEF, signs of organ impairment (lower eGFR), and perhaps uncertainty as to diagnosis and functional status influence practices. In EHFS II, and confirmed in other registries, various grades of frailty among the elderly were demonstrated by decline of independent function, self-care, and QOL with increased dependency for supported care. Data show >70% HF patients >80 years of age may be vulnerable, and this is assessable by “frailty scores.” As relatives and support services assume more care, communication pathways can become more complex even resulting in prescribing that is suboptimal or too complex.13,22,102 Gaps in organized clinical pathways undoubtedly contribute to high readmissions.
Cognitive decline could point to a range of pathologies. There is, however, no direct evidence that HF medication contributes to dementia. Mood disorder or depression is an important consideration for pseudodementia. Decompensated HF could manifest as acute delirium with prolonged hospital stay and higher mortality. Palliative and end-of-life care are usually provided after consultation with families, specialist, general practitioners, and allied health teams. In the Australian health system, providing this service with predictable intensity and duration in hospices are not a huge contributor to readmissions. In the absence of structured care, the need for regular communication and monitoring from patients or their supports, significantly contributes to high readmission rates within 3 to 6 months from discharge between 27% and 47%, where 50% relates to medication, disability, or an associated comorbid condition.22,70,71
Specific therapeutic considerations
Three major uncertainties are noted. First, the altered physiology with aging; altered pharmacodynamics, with increasing hepatic and renal impairment in the main excretory organs for drugs; and pharmacokinetics with reduced total body water content, body mass, and fat tissue. The resulting lower volume of distribution with either low or high plasma concentrations of lipophilic or hydrophilic drugs alters drug effects. Second, two thirds of elderly have >2 noncardiac comobidities and 25% have 6 or more noncardiac comorbidities. When associated with cognitive decline and polypharmacy (average of 10 medications) influences compliance and lowers safety for adverse events. Third, available social supports and ability to achieve high levels of self-efficacy can influence optimal prescribing. 70
Proven prognostic therapies include RAAS inhibitors and β-blockers. Digoxin and diuretics are mainstay for symptoms. All drug classes require close monitoring of weight, electrolytes, renal functionand cardiac haemodynamics. Serum digoxin levels >0.9 nmol/L have cognitive and mortality consequences. Angiotensin-converting enzyme inhibitor long-term benefits above 75 years decline, and angiotensin receptor blockers could be more beneficial.72,73 Eplerenone could have greater tolerability as 10% of men have gynecomastia as testosterone declines with age. β-blocker data are limited; however, tolerability appears lower than younger HF patients (84% vs 76%), In an older HF population, nebivolol improved readmissions and mortality for both systolic and diastolic HF.22,70,74 Finally, with devices, morbidity and mortality are higher in patients >80 years without clear outcome benefits. 68
Guideline gaps
The differences seen in the elderly excluded from RCT are co-morbidities and physiological changes of aging including an inherent increase by age alone. It thus remains unclear how much prognosis is genuinely extended or by a lead-time bias effect. Thus, factoring guidelines for octogenarians remains difficult. However, some principles must guide therapy:
Improved representation in trials, clinical trials, starting with post-marketing trials.
Delivering all proven therapies in conjunction with geriatric teams, achieving maximal tolerable or safe doses;
Regular monitoring of treatments with comparable use of diagnostics;
Minimizing polypharmacy in all other areas, by prioritizing prognostic and QOL improving agents;
Protocols when admitted to general medical units;
Protocols for early and appropriate palliative care referrals for severely deconditioned.
Closing the Gaps
The past 2 millennia have seen the fastest advancements in public health and innovations from assessment to therapies. Universal life expectancy has increased globally when compared with any historical baseline. The evidence generating process and implementation strategies have been the biggest contributors. However, as populations develop diseases later in life or survive for longer, the variables for each patient gradually exceed the boundaries or predefined internal validity parameters of trials. We are thus starting to see plateaus in the health of subgroups, such that health budgets escalate, but cost-efficiency (or return of investment) is not readily noticeable. There is a new phase of medical practice on the horizon, one that will incorporate a greater flexibility in prescribing and management and draw in technological advances. The failure to reproduce trial-level evidence at the population level is the greatest proponent for this argument. The concept of phase 4 or postmarketing studies is well defined but not translated into clinical practice. Moving forward, several avenues to consider are discussed (Figure 2).

Models for closing the gap. To address an outcome measure such as readmission requires arms of the health systems, which are often compartmentalized into silos, to overlap with common purpose. In answering, 5 key areas should be addressed: (1) defining the health jurisdiction from which most of the clients reside, (2) engagement of that community and its primary health infrastructure, (3) investing in technology to bring the gaps and address resource issues, (4) equipped for internal audits and aligning with partners to engage novel research, and (5) delivering these services at an acceptable cost.
Identification and classification of HF patients
As most of the proven evidence is derived from younger patients, health clusters must be able to develop systems that expands the efficacy of findings to all CHF patients. A surge of resources could be used at this point. While a similar prognostic target should not be denied, resources must be used to identify the support networks and readmission risks. Such scoring systems are not well developed (Table 1). 13
Databases—standardizing and prioritizing implementable key performance indicators
The ability to assess real-time performance of CHF programs is vital. The AHA has published the important domains and dimensions of care, systematically going through each of this and more importantly finding a way to determine the key performance indicators, where intervention policy should be delivered will make a great impact on the measured outcome. Such information will inform risk scoring or act as a feeder for a phase 4 trials with different variables from the evidenced RCT.
Evidence generation and outcome measures—RCT or other
Defining roles
Health practitioners are defined and remunerated for clinical services, researchers for productivity in generating new knowledge, and a percentage of clinical researchers manage to function in both camps. However, it has never been entirely clear what roles health practitioners have in auditing their clinical work particularly in relation to cost-efficiency. Larger tertiary hospitals and entire systems like the British National Health System have this as a prerequisite. The responsibility to determine whether public-funded therapeutics is delivering benefits must be part of more than less systems, preferentially over-sighted by accrediting bodies. This will ensure when auditing systems are not in place, collaborations with institutes can be facilitated.
Gaps in guidelines
Gaps in guidelines can only be addressed by generating translatable evidence. This requires resourcing, infrastructure, personnel, and wide support:
Investigator-sponsored noninferiority studies: Posttranslational (phase 4) research is underutilized. Clinicians in practice will notice that with comorbidities and elderly, the external validity of RCT findings is not clearly demonstrated in real-world practice. While the scientific community does not argue against the accepted physiological basis for therapeutic benefits, the properties of one individual drug may come into question when a variant clinical scenario presents itself. Some examples here are diuretics and some renin-angiotensin blockers (e.g lisinopril, losartan) and black race and HF-class and vasodilatory β-blockers. Health systems must also achieve consensus on what constitutes translatable evidence (i.e. allows local clinicians to vary practice) and what methods to use to allow for broader question and experiments (e.g prospective audits with nested interventions or quasi-experimental studies). A noninferiority outcome for the primary and comorbid condition could be acceptable.
Novel research and institutional partnership: Strength-ening existing institutes by partnering could allow for bidirectional benefits. Most research institutes will benefit from having access to patients, and most clinical centers will benefit from the research or trial effect. Research governance requires robust support and secure infrastructure. The added personnel also imparts a culture of learning and accountability.
Improving evidence translation and cost-efficiency
Rapid translation of novel therapies: Complex patients could benefit from regular structured complex case management meetings. Incorporating relevant primary care providers is crucial; remuneration is not presently factored. At these sessions, all available proven therapies relevant to all comorbidities are discussed. Several examples are SGLT-1 inhibitors, bariatric surgery, and atrial fibrillation ablations, all conditions that persist for the patient’s life. The ability to significantly change the trajectory of a comorbid condition that alters CHF prognosis and influences prognosis must always be discussed robustly.
Engaging community and policymakers: It has never been clear what role tertiary institutions plays in prevention, yet this is often the first front to be looked at when outcomes such as readmissions are questioned. Part of this process involves delineating the community and primary care services within its primary catchment and offers regular health updates and promotes regional evidence development. Patient days where specialist units are open to the public could be factored.Strengthening understanding with governmental bodies and research governance bodies that increase the weighting of locally generated evidence and prerequisites for auditing of costly new treatments into health clusters are also considerations.
Conclusions
Readmissions in CHF are a surrogate outcome for delivery of optimal care. Although inroads have been made in improving these statistics, the growing and aging population predicts an increase in resource utilization, economic costs, and wider discrepancies in outcomes with multiple comorbidities and in the elderly. Registries have identified markers of readmission and prognostic risk; however, such information is unlikely to translate to any meaningful bedside use in the foreseeable future. Comorbidities and the elderly often have less robust evidence, as they are excluded from studies in run-in-period or outright. They may require special considerations in diagnostics, choices of therapies including dosing, and other pharmacologic considerations. As the number of questions to be asked is vast, regular quality assurance audits with prospective databases are essential. In the real world, heterogeneity in demographics and lack of relevant models of services offer few choices for a diverse problem. Several process-of-care publications on chronic disease management programs and performance markers have provided a unique opportunity to standardize CHF programs. Although the randomized clinical trial would create an artificial lens to view outcomes for CHF in the real world, it provides a solid template to conduct posttranslational or phase 4 research. The completion of cost-efficiency exercise requires a further bridge for a gap in what is considered acceptable translation research that should be funded by local authorities. Service-based research to reduce readmissions should thus primarily be focused on cost-efficiency and generating translatable research within an agreed standardized framework, for more universal acceptance. Treatments that directly improve the disease trajectory should also be explored with broad stakeholders, where again translation is the priority. Clinical outcomes including improved readmissions are the likely beneficiaries.
Footnotes
Appendix 1
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: A.D. is supported by a Heart Foundation Future Leader fellowship 100472 from the National Heart Foundation of Australia. All co-authors have won independent and governmental research funding.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
PI conceived and designed the experiments, analyzed the data and wrote the first draft of the manuscript. PI, DL, CN, AD, THM, DLH contributed to the writing of the manuscript. PI, DL, CN, AD, THM, DLH agree with manuscript results and conclusions. PI, DL, CN, AD, THM, DLH jointly developed the structure and arguments for the paper. PI, DL, CN, AD, THM, DLH made critical revisions and approved final version. All authors reviewed and approved of the final manuscript.