
Abstract
Background:
Hypertensive heart failure (HHF) is the commonest form of heart failure in Nigeria. There is paucity of data in Nigeria on 24-hour Holter electrocardiography (24-HHECG) and important predictors of arrhythmias among HHF patients.
Objectives:
To determine the 24-HHECG characteristics among HHF patients. To determine the clinical and echocardiographic predictors of arrhythmias detected using 24-HHECG among HHF patients.
Methods:
A total of 100 HHF patients as well as 50 age-matched and sex-matched apparently healthy controls were prospectively recruited over a period of 1 year. They all had baseline laboratory tests, echocardiography, and 24-HHECG.
Results:
Hypertensive heart failure patients had significantly higher counts of premature ventricular contractions (PVCs) than the controls (P ≤ .001). Ventricular tachycardia (VT) was recorded in 29% of HHF patients as compared with controls who had no VT on 24-HHECG. The standard deviation of all normal to normal sinus RR intervals over 24 hours (SDNN) was abnormally reduced among HHF patients when compared with controls (P = .046). There was positive correlation between atrial fibrillation (AF) and the following parameters: PVCs (r = .229, P = .015), New York Heart Association (NYHA) (r = .196, P = .033), and VT (r = .223, P = .018). Following multiple linear regression, left ventricular ejection fraction (LVEF) (P ≤ .001) and serum urea (P = .037) were predictors of PVCs among HHF patients. Serum creatinine (P ≤ .001), elevated systolic blood pressure (SBP) (P = .005), and PVCs (P ≤ .001) were important predictors of VT among HHF patients.
Conclusions:
Renal dysfunction and reduced LVEF were important predictors of ventricular arrhythmias. High counts of PVCs and elevated SBP were predictive of the occurrence of VT among HHF patients. The NYHA class and ventricular arrhythmias have a significant positive correlation with AF. The SDNN is reduced in HHF patients.
Keywords
Introduction
Hypertensive heart failure (HHF) is the commonest form of heart failure (HF) in Nigeria and accounts for about 44% to 79% of cases of HF in Nigeria.1-4 Hypertensive heart failure, just like other causes of HF, is associated with a poor prognosis with arrhythmias being one of the potent factors conferring increased risk of a poor outcome.5,6 Other notable risk factors for a poor outcome among HF patients include long duration of high blood pressure (HBP), magnitude of HBP, lack of awareness of HBP, high cardiothoracic ratio on chest X-ray, long duration of HF, and lack of previous therapy for HBP.7,8 Some other poor prognostic indices of HF include systolic dysfunction, hyponatremia, renal dysfunction, New York Heart Association (NYHA) class (III and IV), prolonged corrected QT interval (QTc), advanced age, third heart sound (S3) on auscultation, as well as increased brain natriuretic peptide.9-11
Arrhythmias are recognized as poor prognostic factors among HF patients, but resting 12-lead electrocardiography (ECG) may not to be very useful in assessing their significance. 12 However, 24-hour Holter ECG (24-HHECG) may be better at assessing the presence and significance of arrhythmias when compared with 12-lead ECG as the recordings in the former span a longer period of time. The 24-HHECG also provides more prognostic information apart from detection of arrhythmias such as heart rate variability (HRV). Therefore, the autonomic nervous system function can be assessed when the various time domains of HRV are measured.
There might be some interplay between echocardiographic findings and 24-HHECG parameters among HHF patients. Therefore, important echocardiographic findings as well as other clinical parameters may serve as surrogate markers for important ECG findings detected on 24-hour Holter monitoring if strong associations are found. This potential finding may be useful in resource-poor settings where 24-HHECG is not readily accessible due to cost considerations and logistics difficulties.
To the best of our knowledge, studies on assessment of 24-HHECG among HHF patients are scarce. We therefore aim to assess the 24-HHECG characteristics among HHF patients and attempt to find useful echocardiographic and clinical correlations. We also aim to identify important predictors of arrhythmias, as arrhythmias have been implicated as a major cause of sudden cardiac death among patients with HF.5,6
Methods
This study was conducted at Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC), Nigeria. Informed written consent was obtained from each of the study participants, and approval of the Ethics and Research Committee of OAUTHC was obtained before the commencement of the study.
A total of 100 HHF patients and 50 age-matched and sex-matched apparently healthy controls were consecutively recruited to participate in the study over a period of 1 year.
Heart failure was defined based on the recommendations of the European Society of Cardiology for the diagnosis of HF or the Framingham criteria.13,14 High blood pressure was defined as average of 3 blood pressure (BP) measurements ≥140/90 mm Hg or if the subject was already on antihypertensive therapy. 15 Subjects admitted with suspected HF who did not meet the diagnostic clinical criteria for the diagnosis of HF or HBP were excluded from the study. Subjects with HF from any other cause other than HBP were also excluded.
A clinical proforma was completed by all the study participants. The BP was measured supine and standing with an Accoson mercury sphygmomanometer. Korotkoff phases 1 and 5 were used for systolic and diastolic BPs, respectively. Three consecutive measurements were taken at 5-minute intervals and the average values were recorded.
Baseline laboratory investigations were also performed on all the subjects. The packed cell volume, electrolytes, serum urea, and creatinine were recorded for all the study participants.
The Vivid 7 Dimension ultrasound imaging system made by the General Electric (GE) Medical Systems was used to perform echocardiographic assessment for all the study participants. All the study participants had 2-dimensional (2D), 2D-derived M-mode, Doppler (pulsed-wave, continuous-wave, color flow) and tissue Doppler transthoracic echocardiography with simultaneous ECG recordings in accordance with the recommendations of the American Society of Echocardiography. 16
The left ventricular ejection fraction (LVEF) was calculated from the Teichholz formula 17 based on volumes computed from the echocardiographic machine. The average of 3 consecutive readings was documented as the LVEF.
The early (e′) and late (a′) septal diastolic mitral annular velocities were obtained via pulsed-wave Doppler from the septal side of the mitral annulus in the apical 4-chamber view with the septal annulus movement aligned with the sample volume. The ratio of early transmitral inflow velocity (E) to the early septal diastolic mitral annular velocity (e′) was then calculated.
In turn, the pulmonary capillary wedge pressure (PCWPcal) was calculated using the formula developed by Nagueh et al 18 :

Doppler evaluation was used to confirm and quantify the degree of diastolic dysfunction (DDF). The early (E) and late (A) transmitral inflow velocities were obtained by pulsed-wave Doppler echocardiography with the sample volume placed at the tip of the mitral valves in the apical 4-chamber view. Normal diastolic function was defined as the presence of the following: E/A ratio between 1 and 2, early septal diastolic mitral annular velocity (e′) >10 cm/s and e′/a′ >1.
Grade 1 DDF (impaired relaxation) was considered if the E/A ratio was <1, e′ velocity <10 cm/s and e′/a′ <1. Grade 2 DDF was defined as E/A ratio of between 1 and 2, e′ <8 cm/s and e′/a′ <1. Grade 3 DDF was considered if the E/A ratio was >2 and e′/a′ <1. 18
The Tei index (combined systolic and diastolic function) was determined by pulsed-wave Doppler with sample volume first placed at the tips of the mitral valve in the apical 4-chamber view to measure the time interval (a′) between the closure of the mitral valve for one cardiac cycle and its opening for the next cycle. The left ventricular ejection time (LVET) (b) was then derived by placing a sample volume below the aortic valve in the apical 5-chamber view to display the left ventricular ejection jet profile.19-21
The Tei index was then calculated as follows:

where “a − b” is the sum of both the isovolumic relaxation time (interval between aortic valve closure and mitral valve opening) and the isovolumic contraction time (interval between mitral valve closure and aortic valve opening), whereas “b” is the LVET (interval from opening to closure of aortic valve).
The reference value is <0.4 in normal individuals and increased in patients with HF. 20
All the study participants also had 24-HHECG recordings. This was recorded using the Schiller type (MT-101) with a bipolar V1-V5 lead system. Each HHF patient had the recorder strapped around the chest and allowed to go back to the hospital bed. The controls also had the recorder strapped to the chest and were allowed to go home with the device. During the recording, subjects were instructed to record timing of any symptoms such as palpitations, dizziness, and chest pain. After completion of the recording over a 24-hour period, the recorder was retrieved and analyzed with Schiller’s cardiovit CS-200 digital ECG computer.
The following data were recorded from all participants: Total heart rate, HRV, ST depression, premature ventricular contractions (PVCs), couplets, ventricular tachycardia (VT), supraventricular tachycardia (SVT), premature atrial contractions (PACs), and atrial fibrillation (AF).
The HRV was analyzed in 4 time domains in accordance with standards.22,23 The time domains of HRV are as follows:
SDNN—Standard deviation of all normal to normal sinus RR intervals over 24 hours.
SDANN—Standard deviation of the averaged normal to normal sinus RR intervals for all 5-minute segments.
RMSSD—root-mean-square of the successive normal sinus RR interval difference.
PNN50—percentage of successive normal sinus RR intervals >50 ms.
Reference values for these time domains that have been shown to be predictive of poor prognosis in HF are stated below 23 :

Significant PVCs were defined as presence of PVCs greater than 10% of the total QRS complexes.
The Lown grading of PVCs among patients with PVCs was applied as follows 24 :
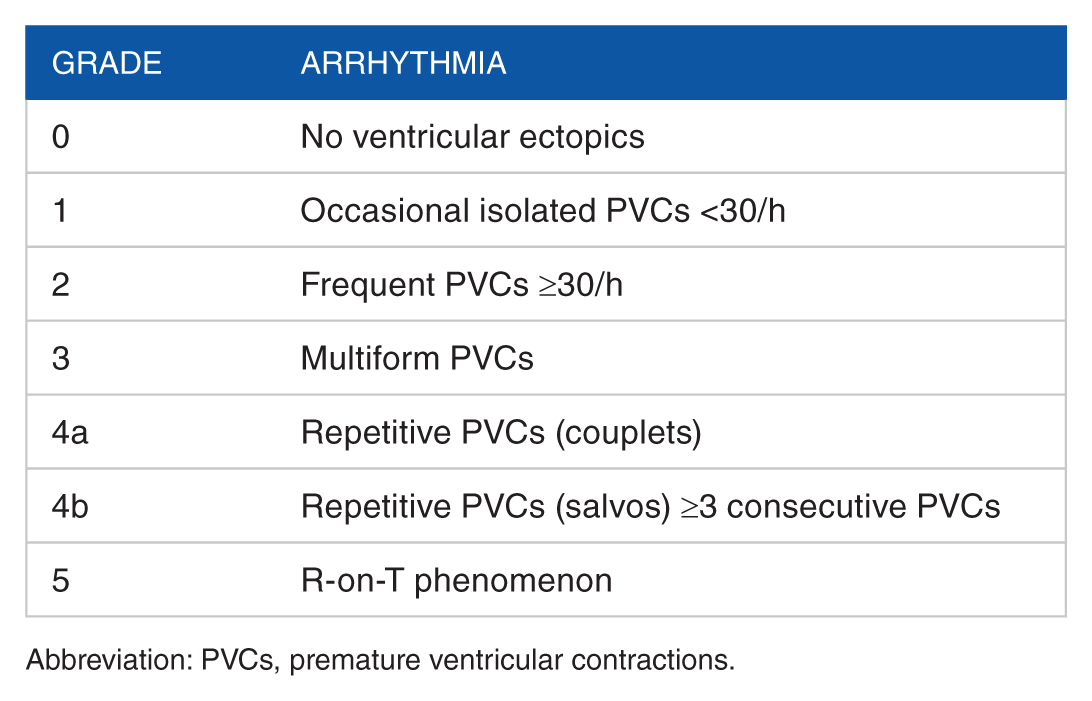
Abbreviation: PVCs, premature ventricular contractions.
Statistics
The data analysis was performed using IBM SPSS software version 20.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics was computed for continuous variables, whereas frequency tables were generated for categorical variables. The continuous variables were expressed as mean ± standard deviation, whereas categorical data were expressed as percentages. Differences between 2 continuous variables were determined with the independent Student t test. The differences between categorical data were done by the χ 2 test. The Pearson coefficient test was used to test correlation between relevant variables. Multiple regression analysis was also performed to predict the occurrence of some dependent variables from several independent variables. The level of significance was P of ≤.05 and confidence interval of 95%.
Results
A total of 100 HHF patients and 50 apparently healthy individuals, who served as controls, were recruited into this study. The HHF patients comprised 62 (62%) men and 38 (38%) women, whereas the controls comprised 30 (60%) men and 20 (40%) women. As shown in Table 1, there was no significant difference in the mean age of HHF patients and controls (64.43 ± 12.92 vs 60.26 ± 11.65 years; P = .057). The age range of the HHF patients was 37 to 90 years. About 50% of the HHF patients were in NYHA class III/1V.
Demographic, clinical, and laboratory characteristics of the study participants.

Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; HHF, hypertensive heart failure; PCV, packed cell volume; SBP, systolic blood pressure.
P ≤ .05 for HHF vs control.
There was also no significant difference in the serum sodium between HHF and controls (131.62 ± 10.22 mmol/L vs 132.76 ± 1.32 mmol/L; P = .43). The HHF patients, however, had significantly lower packed cell volumes (P ≤ .001) than the controls. The HHF patients also had significantly higher serum urea (P ≤ .001) and serum creatinine (P ≤ .001) than the controls as shown in Table 1.
As shown in Table 2, HHF patients had significantly lower LVEF (39.68% ± 14.86% vs 68.24% ± 5.50%; P ≤ .001) and fractional shortening (20.24% ± 9.19% vs 38.20% ± 4.47%; P ≤ .001) than controls. The HHF patients also had markedly elevated end systolic volume (114.52 ± 67.92 mL vs 30.88 ± 12.75 mL; P ≤ .001) as compared with the controls.
Echocardiographic parameters of the study participants.

Abbreviations: E/e′, ratio of early transmitral inflow velocity (E) to the early septal diastolic mitral annular velocity (e′); ESV, end systolic volume; IVSTd, interventricular septal thickness in diastole; LADi, left atrial diameter index; LVEDD, left ventricular end diastolic diameter; LVEF, left ventricular ejection fraction; LVESD, left ventricular end systolic diameter; LVFS, left ventricular fractional shortening; LVPWTd, left ventricular posterior wall thickness in diastole; PCWPcal, calculated pulmonary capillary wedge pressure; TEI, Tei index.
P ≤ .05 for HHF vs control.
Table 2 also shows that the Tei index was significantly higher in HHF patients as compared with controls who had normal mean Tei index values below the cutoff of 0.4 (0.52 ± 0.19 vs 0.27 ± 0.07; P ≤ .001).
Among the HHF patients, there were moderate to severe valvular regurgitations of the following valves detected on echocardiography: mitral (62%), tricuspid (42%), pulmonary (44%), and aortic (30%). None of the controls had moderate to severe regurgitations across any of the valves.
The prevalence of DDF among HHF patients was 88% compared with 10% in the controls. The patients in the controls with DDF all had grade 1 DDF. The distribution of diastolic function among the HHF patients is as follows: normal diastolic function (12%), impaired relaxation or grade 1 DDF (32%), grade 2 DDF (18%), and restrictive pattern or grade 3 DDF (38%).
Heart failure with preserved ejection fraction (HFpEF) defined as EF greater than 50% was seen in 28% of HHF patients. Heart failure with reduced EF (HFrEF) defined as EF less than 40% was seen in 51% of HHF patients, whereas 21% of the HHF fell in the borderline group as they had EF between 40% and 49%.
As shown in Table 3, the HHF patients had significantly higher counts of PVCs than the controls (3578 ± 655.8 per 24 hours vs 19.78 ± 26.71 per 24 hours; P ≤ .001). Even though HHF patients had higher heart rates than the controls, the difference was not statistically significant (P = .135).
The 24-hour Holter ECG parameters of the study participants.
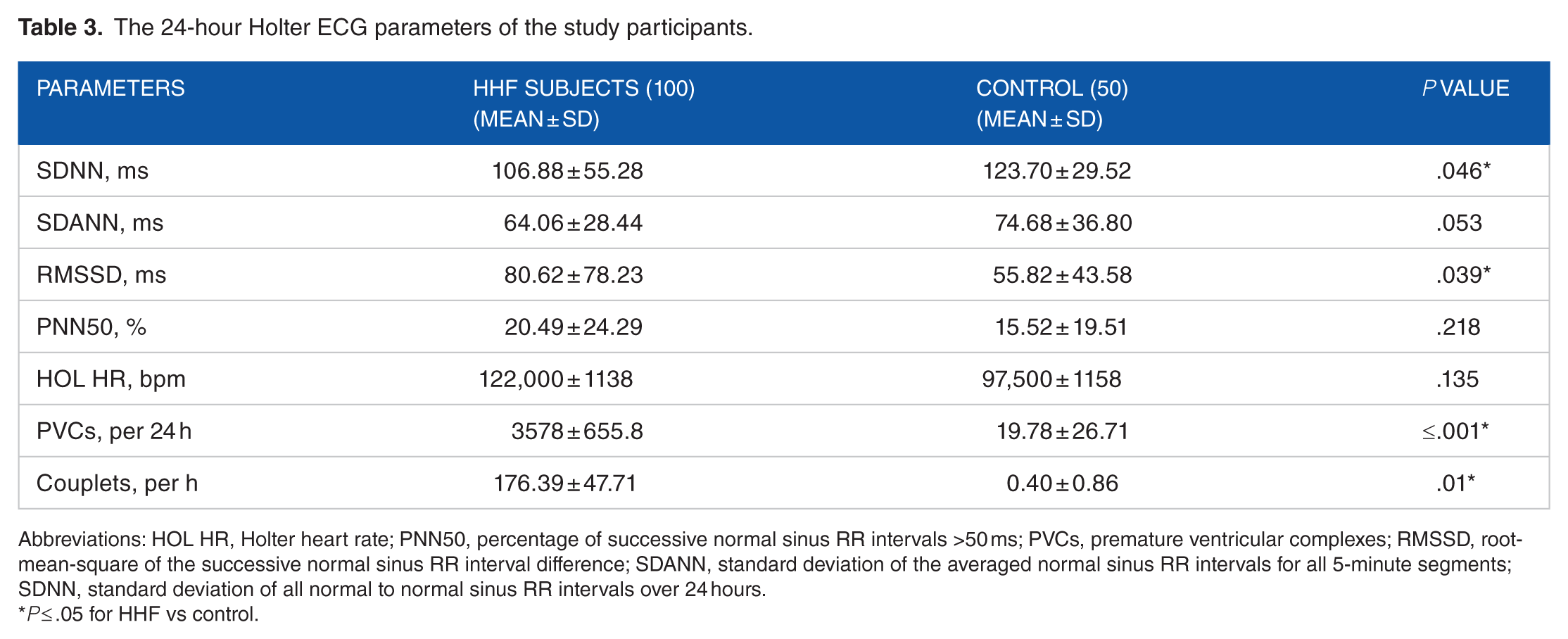
Abbreviations: HOL HR, Holter heart rate; PNN50, percentage of successive normal sinus RR intervals >50 ms; PVCs, premature ventricular complexes; RMSSD, root-mean-square of the successive normal sinus RR interval difference; SDANN, standard deviation of the averaged normal sinus RR intervals for all 5-minute segments; SDNN, standard deviation of all normal to normal sinus RR intervals over 24 hours.
P ≤ .05 for HHF vs control.
The standard deviation of all normal to normal sinus RR intervals over 24 hours (SDNN) was abnormally reduced among HHF patients as compared with controls (P = .046).
Significant PVCs defined as PVC count greater than 10% of the QRS complexes seen on 24-hour Holter monitoring was seen in 18% of HHF patients. The remaining 82% of HHF patients had nonsignificant PVCs on 24-hour Holter monitoring. On the whole, 25% and 42% of the HHF patients belonged to Lown grades 4 and 2, respectively. However, 34 (78%) of the controls had nonsignificant PVCs on 24-hour Holter monitoring and all belonged to Lown grade 1 of PVCs.
About 21% of HHF patients had significant PACs defined as PACs greater than 10% of the electrical complexes on 24-hour Holter monitoring. The rest of the HHF patients (79%) also had PACs on 24-hour Holter monitoring but were not significant based on the above definition. Only 6 (12%) of the controls had nonsignificant PACs on 24-hour Holter monitoring. Supraventricular tachycardia and VT were recorded in 38% (38) and 29% (29) of HHF patients, respectively, following 24-hour Holter monitoring. All but 1 of the 29 HHF patients with VT recorded on Holter ECG had nonsustained VT. Only 1 patient with HHF had sustained VT. None of the controls had SVT or VT on 24-HHECG monitoring.
ST depression and AF were seen in 32% and 25% of the HHF patients on 24-HHECG monitor, respectively. There was positive correlation between AF and the following parameters: PVCs (r = .229, P = .015), NYHA (r = .196, P = .033), VT (r = .223, P = .018). Overall, 52% of HHF patients were deemed to have abnormal 24-hour Holter recordings, whereas all the controls had normal recordings.
As shown in Table 4, LVEF and serum urea were predictors of PVCs among HHF patients. Serum creatinine, systolic blood pressure (SBP), and PVCs were important predictors of VT as seen in Table 5.
Multiple regression analysis for predictors of premature ventricular contractions.

Abbreviations: β, standardized coefficients; B, unstandardized coefficients; LVEF, left ventricular ejection fraction; SBP, systolic blood pressure.
P ≤ .05.
Multiple regression analysis for predictors of ventricular tachycardia.
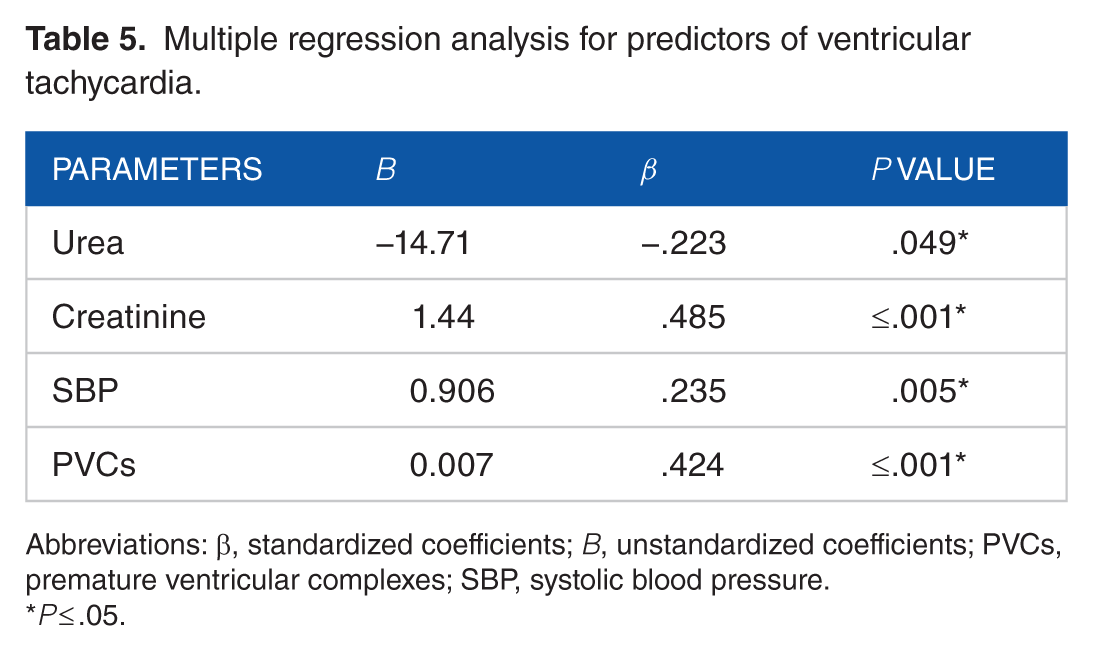
Abbreviations: β, standardized coefficients; B, unstandardized coefficients; PVCs, premature ventricular complexes; SBP, systolic blood pressure.
P ≤ .05.
As shown in Figure 1, there is a negative correlation between LVEF and the occurrence of PVCs on 24-HHECG (r = −.312, P = .002). The graphical representation of the relationship between serum creatinine and VT is displayed in Figure 2 (r = .446, P ≤ .001). There is a positive correlation between PVCs and VT (r = .462, P ≤ .001) and this is clearly displayed in Figure 3.

Scatterplot depicting the correlation between premature ventricular contractions and left ventricular ejection fraction.
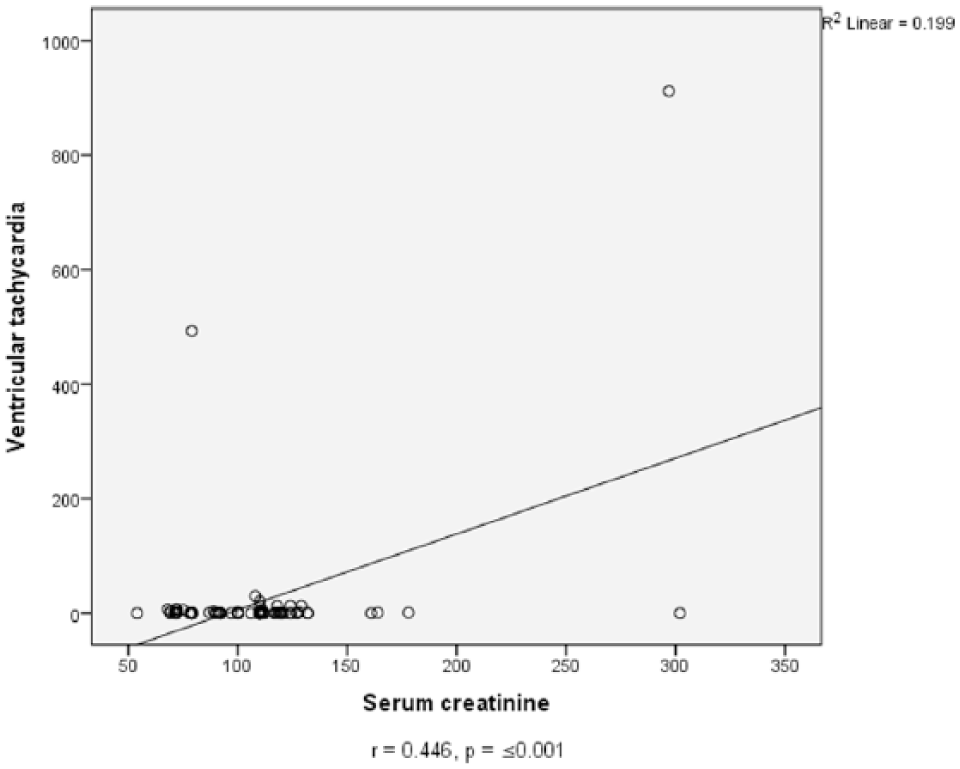
Scatterplot depicting the correlation between ventricular tachycardia and serum creatinine.

Scatterplot depicting the correlation between ventricular tachycardia and premature ventricular contractions.
Discussion
In this study, HHF patients had significantly higher BPs (P ≤ .001), serum urea (P ≤ .001), and serum creatinine (P ≤ .001) than the controls. They, however, had significantly lower packed cell volume (P ≤ .001)) than controls. Renal dysfunction and anemia are associated with HF which may account for the significant difference in these parameters between HHF patients and controls. 8
The HHF patients also had lower LVEF (P ≤ .001) than the controls. The HHF patients also had higher Tei index values than controls indicating lower global myocardial performance among the HHF cohort as compared with the controls. A low LVEF is characteristic of patients with HFrEF 25 and may account for lower values in HHF patients as compared with controls. Heart failure with preserved ejection fraction patients still have a poor prognosis similar to that of patients with HFrEF.26-28 This may imply that several other factors may interplay with LVEF as an indicator of prognosis among HF patients.
The HHF patients were also seen to have higher counts of PVCs, VT, as well as AF on 24-HHECG monitoring. These have been shown to be accompaniments of HF 29 and may account for the higher prevalence of these arrhythmias among the HHF population in this study. Heart rate variability was also significantly lower in the HHF cohort as compared with controls indicating autonomic perturbations that may be predicative of a poor outcome.
Arrhythmias are prevalent among HF patients and constitute a huge burden among this group of patients. 29 It carries a very poor prognosis and as a result, we attempted to determine the predictors and important associations of these arrhythmias. 30 Following multiple regression, LVEF was a significant predictor of the occurrence of PVCs among HHF patients. From our results, lower LVEF is predictive of higher counts of PVCs (Figure 1 and Table 4). This finding is in consonance with those of other researchers.31-35 Left ventricular ejection fraction less than 35% has been stated to be the cutoff for high risk of sudden cardiac death among HF patients. However, patients with moderately reduced LVEF may still be at risk of sudden cardiac death based on the findings of Zhao et al. 31 Conversely, Zorzi et al 34 suggest that the incidence of Holter ECG–detected ventricular arrhythmias was more among HF patients with LVEF <35% and not much of ventricular arrhythmias were detected in patients with LVEF >35%. Zorzi et al 34 also suggested that early detection of ventricular arrhythmias may confer some mortality benefit as therapy may be instituted early. Occurrence of these arrhythmias later on in the course of the disease, however, carried a very high fatality rate. 34
Another important predictor of PVCs among HHF patients in this study is elevated serum urea. Elevated serum creatinine was also an important predictor of VT among HHF patients (Figure 2 and Table 5). Sadly, the combination of a low LVEF and renal dysfunction may confer a high risk of mortality among HF patients even in the presence of state-of-the-art therapeutic measures. 36 Kreuz et al 36 found that HF patients with a low LVEF and renal dysfunction could have about a 300-fold increase in mortality as compared with those with better LVEF and renal function even when these patients had implantable cardioverter defibrillator (ICD). They opined that the risk of death may be so high that implanting an ICD in this group of patients may not be worthwhile. McCullough et al 37 demonstrated a graded increase in the risk for atrial and ventricular arrhythmias with increasing renal dysfunction. Lin et al 38 also demonstrated that PVCs on Holter ECG monitoring served as an independent risk factor for all-cause mortality, cardiovascular hospitalization, all-cause hospitalization, and new-onset HF.
High counts of PVCs on 24-HHECG monitoring served as an important predictor for the occurrence of VT (Figure 3 and Table 5). Although PVCs and less likely nonsustained VT may be commonly seen in the population, a high frequency of these among HF patients may be deleterious.39,40 Premature ventricular contractions may be an important harbinger for dangerous VT as demonstrated in this study and the report of Sheldon et al.39,41
Following multiple linear regression, SBP was found to be a significant predictor of VT (P = .005). There have been divergent views of the impact of SBP among patients with HF. Isezuo et al7,8 opined that the severity of elevated BP, duration, and unawareness of elevated BP is associated with increased mortality risk among HHF patients. It is not known if this increased mortality risk is related to the association of VT with elevated BP or some other associations. However, in the report of the organized program to initiate lifesaving treatment in hospitalized patients with HF (OPTIMIZE-HF [Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure]) trial, increased SBP at admission up to a threshold of 160 mm Hg was associated with a lower risk of in-hospital mortality. They stated that each 10-mm Hg increase in SBP up to 160 mm Hg was associated with a 17% reduction in in-hospital deaths. 42 Therefore, mortality was highest in HF patients with low SBP and high serum creatinine subgroup. 42 The disparity in the findings of the OPTIME-HF study and that of Isezuo et al on the effect of BP on mortality in HF may be due to the fact that SBP was assessed in conjunction with serum creatinine as a subgroup in the former.
In this study, there was significant positive correlation between AF and ventricular arrhythmias (PVCs: r = .229, P = .015 and VT: r = .223, P = .018). There are few studies to the best of our knowledge that has attempted to find a correlation between AF and ventricular arrhythmias. Tan et al, 43 however, stated that changes in ventricular repolarization occur during AF which in turn results in QTc prolongation and increased risk of ventricular arrhythmias if class 1A/III anti-arrhythmic agents are used to terminate AF.
There was also a significant positive correlation between AF and NYHA class (r = .196, P = .033). As a result, HHF patients with a higher NYHA class tend to have a higher tendency of having AF. This is in consonance with recent studies.44,45 Kotecha et al 44 found that a higher NYHA class was associated with AF among patients with HFrEF as compared with those with HFpEF. This is in agreement with our findings as 51% of the HHF patients had HFrEF as opposed to 28% of patients with HFpEF. A larger proportion of our HHF patients may have had reduced EF possibly because of late presentation and advanced disease at the time of presentation. Khand et al 46 reported that dual therapy with carvedilol and digoxin among patients with AF and chronic HF resulted in improved NYHA class and median ventricular rate among other factors as compared with use of digoxin alone. This may imply that a more aggressive approach toward treating AF among HF patients may bring about reduction in ventricular rate, improvement in NYHA class, and possibly a better outcome among HF patients. Such targeted therapy can only be initiated if arrhythmias are detected which underscores the pivotal role of 24-hour Holter monitoring among HHF patients.
In this study, HRV as measured by SDNN was significantly lower among HHF patients than controls (P = .046). This is in agreement with the findings of other researchers.47,48 The thinking is that a higher variability in the heart rate in response to various hemodynamic changes is indicative of a healthy autonomic nervous system. 48 However, a reduced HRV is suggestive of autonomic disequilibrium and increased vulnerability to life-threatening arrhythmias among patients with HF.49,50 As a result, a decreased HRV may be associated with a poor outcome among HF patients.49-51 Therefore, therapies which are aimed toward altering the HRV may be useful in improving outcomes among HF patients. This theory was tested by Kurtoglu et al 48 where an 8-week therapy with ivabradine resulted in increased HRV among patients with chronic HF from nonischemic cardiomyopathy. They suggested more studies and a larger sample size to further evaluate the usefulness of this line of therapy.
Conclusions
The HHF patients had higher prevalence of arrhythmias as compared with normal controls. Heart rate variability was low as measured by SDNN among HHF patients. Renal dysfunction and reduced LVEF were important predictors of ventricular arrhythmias. High counts of PVCs, elevated serum creatinine, and SBP were predictive of the occurrence of VT among HHF patients. New York Heart Association class and ventricular arrhythmias have a significant positive correlation with AF.
Limitations of this study
A useful parameter such as heart rate turbulence could not be assessed among our study population because of the limitation of our Holter ECG software.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceived and designed the experiments: TOM, MOB, AOA, RAA. Analyzed the data: TOM, MOB, AOA, RAA. Wrote the first draft of the manuscript: TOM. Contributed to the writing of the manuscript: TOM, MOB, AOA, RAA, OEA, VNA, OAO, ANI, BM, OJB. Agreed with manuscript results and conclusions: TOM, MOB, AOA, RAA, OEA, VNA, OAO, ANI, BM, OJB. Jointly developed the structure and arguments for the paper: TOM, MOB, AOA, RAA, OEA, VNA, OAO, ANI. Made critical revisions and approved the final version: TOM, MOB, AOA, RAA, OEA, VNA, OAO, ANI, BM, OJB. All the authors reviewed and approved the final manuscript.