
Abstract
This study confirms the association of risk factors for coronary artery disease (CAD) and the apoE polymorphisms, specifically related to the APOE*4 allele, with coronary disease in postmenopausal women. Significantly altered values of the lipid profile were found in patients when compared with controls, independent of the presence of the APOE*4 allele. However, the controls showed higher high-density lipoprotein cholesterol (HDL-C) levels and reduced triglyceride (TG) levels, differing significantly from patients. In this case, the study of subgroups, considering the APOE*3/3 and APOE*3/4 genotypes, suggests that the APOE*4 allele is not implicated in the variations of the lipid profile of patients and determined an increase in the production levels of HDL-C and a reduction in TG highly benefiting the control group compared with APOE*3/3 genotype. The metabolic kinetics of TG, although with the same pattern between groups, and the presence of the APOE*4 allele are suggested to be associated with accelerated clearance compared with APOE*3 allele in non-CAD group.
Introduction
Coronary artery disease (CAD), 1 the main cause of death in Western countries,2,3 is 3 to 4 times more common in men than in women with up to 55 years of age. Nevertheless, the risk increases as women at this age start menopause leading to nearly 250 000 deaths annually in the United States. 4 During menopause, the lipid profile of women undergo changes resulting in risks of CAD similar to men. In this phase, rises in the total cholesterol (TC), 5 triglycerides (TG), 6 and low-density lipoprotein cholesterol (LDL-C) fraction levels are observed, whereas the levels of the high-density lipoprotein cholesterol (HDL-C) fraction remain relatively constant. Estrogen deficiency also negatively affects coagulation, vascular reactivity, and endothelial function. 4 Furthermore, lipoprotein(a) 7 levels have also been found to rise in postmenopausal women; this is an independent risk factor for atherosclerotic disease linked to thrombogenic phenomena,8–12 in particular due to higher concentrations of factor VII, fibrinogen, and plasminogen activator inhibitor-1 (PAI-1).12,13
Family history also contributes to the development of CAD; the estimated inheritability for men is 20% to 80% and for women it is 30% to 60% on the basis of first-degree relatives. 14 It is estimated that 60% of the variability of serum lipid levels is genetically determined with many of these variations being polygenic. The association between apolipoprotein E (apoE) polymorphisms and atherosclerosis was initially established by Utermann et al 15 in studies of patients with type III hyperlipoproteinemia, the APOE*2/2 genotype and early-onset CAD. The APOE*3/4 genotype has been associated with acute myocardial infarction at an earlier age when compared with the APOE*2/3 and APOE*3/3 genotypes.16,17 A study of the possible genetic markers in Brazilian women showed an association of CAD with the apoE polymorphisms, as well as with apolipoprotein B polymorphisms and the LDL receptor gene. 18 There are also reports that patients with the APOE*4 allele are more common in clinics that specialize in the treatment of dyslipidemia than those with APOE*3. 6 The hypothesis that APOE*4 favors the development of atherosclerosis and that APOE*2 prevents it has been supported by the results of clinical studies on survivors of myocardial infarction, 19 patients with angiographically documented CAD, 20 and octogenarian patients. 21 However, the effects of the APOE alleles on plasma lipid levels are still unclear.22,23
The lipid metabolism comprises complex processes with significant individual changes occurring after a lipid-rich meal. Several studies on patients with CAD and individuals without the disease have shown changes, largely of the TG plasma level, in the postprandial period after a lipid-rich diet with high values being obtained 3 to 9 hours after ingestion.24,25 However, the participation of apoE in specific situations, including in postmenopausal patients with CAD, remains controversial, 26 and data on its relationship with the lipid profile and changes in TG plasma levels in the postprandial period are scarce or inexistent in Brazilian samples.
Thus, this study aimed at analyzing the prevalence of alleles and genotypes of apoE and their influence on the lipid profile and TG metabolic kinetics after a lipid-rich diet, considering their association with apoE in postmenopausal women with or without CAD.
Patients and Methods
A total of 180 postmenopausal women treated in the outpatients’ service of Hospital de Base Medical School in São José do Rio Preto (FAMERP), SP, Brazil, were allocated to 2 groups according to the presence or absence of CAD. The group of women with angiographically confirmed CAD and clinical manifestations before the age of 65 years was constituted of 90 patients aged from 47 to 73 years. The control group composed of 90 women aged from 50 to 71 years without angiographic signs or symptoms of CAD. Only women, who were not taking medications that might interfere in the lipid profile, at the time of diagnosis, including hormone replacement therapy, participated in the study. Patients with hypothyroidism, kidney or liver diseases confirmed by biochemical and hormone tests were excluded. The study project was approved by the Ethics Research Committee of the institution. All the participants received an explanation about the study and gave their written consent.
The clinical, epidemiologic, and biochemical characteristics are presented in Table 1. Women were considered diabetic when they were under treatment for diabetes or had a fasting blood sugar level equal to or greater than 126 mg/dL as stated in the criteria of the Primary Prevention of Cardiovascular Diseases in People with Diabetes Mellitus: a Scientific Statement from the American Heart Association and the American Diabetes Association.27,28 Patients were considered obese when they had a body mass index equal to or greater than 30 kg/m2 as defined by the World Health Organization. Systemic arterial hypertension was defined according to the criteria of the Seventh Report of the Joint National Committe on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure of United States of America (VII JNC-USA) (systolic and diastolic arterial pressures above 140 and 90 mm Hg, respectively) or when the patient was under treatment for hypertension. 29 The values considered normal for biochemical parameters were as follows: alanine transferase ≤ 20 IU/L, aspartate transferase ≤ 25 IU/L, creatinine from 0.2 to 1.4 mg/dL, thyroid-stimulating hormone from 0.1 to 5.0 μU/mL, and free T4 < 0.9 ng/dL.
Clinical, epidemiologic, and biochemical characteristics in postmenopausal women with coronary artery disease (CAD group) and controls (non-CAD group).

Abbreviations: ALT, alanine transferase; AST, aspartate transferase; BMI, body mass index; T4, tyrosine; TSH, thyroid-stimulating hormone.
Serum levels of TC, LDL-C, HDL-C, very-low-density lipoprotein cholesterol (VLDL-C) fraction, and TG were measured after 12 hours of fasting. In addition, TG levels were measured at 3 and 6 hours after the ingestion of a single high-lipid meal. The values of the variables of the lipid profile were analyzed considering the IV Guidelines on dyslipidemia of the Brazilian Cardiology Society. 30
ApoE Polymorphisms
The genomic DNA was extracted from the leukocytes of peripheral blood. 31 The segment of the apoE gene carrying the studied polymorphic regions was amplified using the polymerase chain reaction technique. The primers P1: 5′-ACAGAATTCGCCCGGCCTGGTACAC-3′ (sense) and P2: 5′-TAAGCTTGGCACGGCTGTCCAAGCA-3′ (nonsense) complementary to the regions near to the polymorphic codons 112 and 158 located in exon 4 of the apoE gene were used in the reactions. The restriction fragment length polymorphism technique was employed after digestion of the amplification product using the HhaI restriction enzyme.
The fragments of DNA referring to the APOE*2, APOE*3, and APOE*4 alleles were separated by nondenatured 6% polyacrylamide gel electrophoresis. The control was a standard DNA sample (pBR322; Gibco, Waltham, Massachusetts, USA) digested using the MspI restriction enzyme, which generates fragments of 110, 90, 76, and 67 base pairs. After electrophoresis in polyacrylamide gel, the fragments of DNA were identified as APOE*2/2, APOE*2/3, APOE*2/4, APOE*3/3, APOE*3/4, and APOE*4/4 genotypes.
Statistical Analysis
The comparative study of allele and genotype frequencies for apoE and other variables was achieved using the Fisher exact test and variance analysis for repeated samples. Exploratory analysis of the lipid profile included calculations of the mean values and standard deviations, with the differences between groups being compared using the Student t test, applying Welch correction for standard deviations or the Mann-Whitney test when the distribution was non-Gaussian. These tests were also applied to evaluate the association between the lipid profile and apoE polymorphisms with respect to the APOE*3/3 genotype compared with genotypes with at least one APOE*4 allele (_/APOE*4); the analyses compared the groups in isolation and values between groups. For the kinetic analysis of the TG metabolism in the postprandial phase, analysis of variance was employed to compare paired samples identified as fasting and 3 and 6 hours after a single dose of the lipid-rich diet, and the χ2 test was applied in the comparative analysis of the area under the curve. An α error of 5% was considered acceptable giving a significance level for P < .05.
Results
ApoE polymorphisms
The distributions of the APOE alleles and genotypes in patients and controls are presented in Table 2. A significantly higher frequency of the APOE*3 allele was observed in the non-CAD group when compared with patients with CAD (0.91 against 0.81, respectively; P = .009), and APOE*4 was significantly more common in the CAD group than in the non-CAD group (0.15 against 0.07, respectively; P = .028). The APOE*2 allele was rare, and no statistically significant difference was identified between the groups. APOE*3/3 was the most common genotype in both CAD and non-CAD groups, with a statistically significant difference between groups (69% versus 83.3%, respectively; P = .035). The _/APOE*4 genotypes, although more frequent in patients with CAD (25.5%) than in the non-CAD group (13.3%), did not give a statistical difference between groups (P = .059).
Distribution of the allelic and genotypic frequencies for apolipoprotein E in the evaluation of the genetic polymorphism by HhaI enzyme restriction in postmenopausal women with coronary artery disease (CAD group) and controls (non-CAD group).
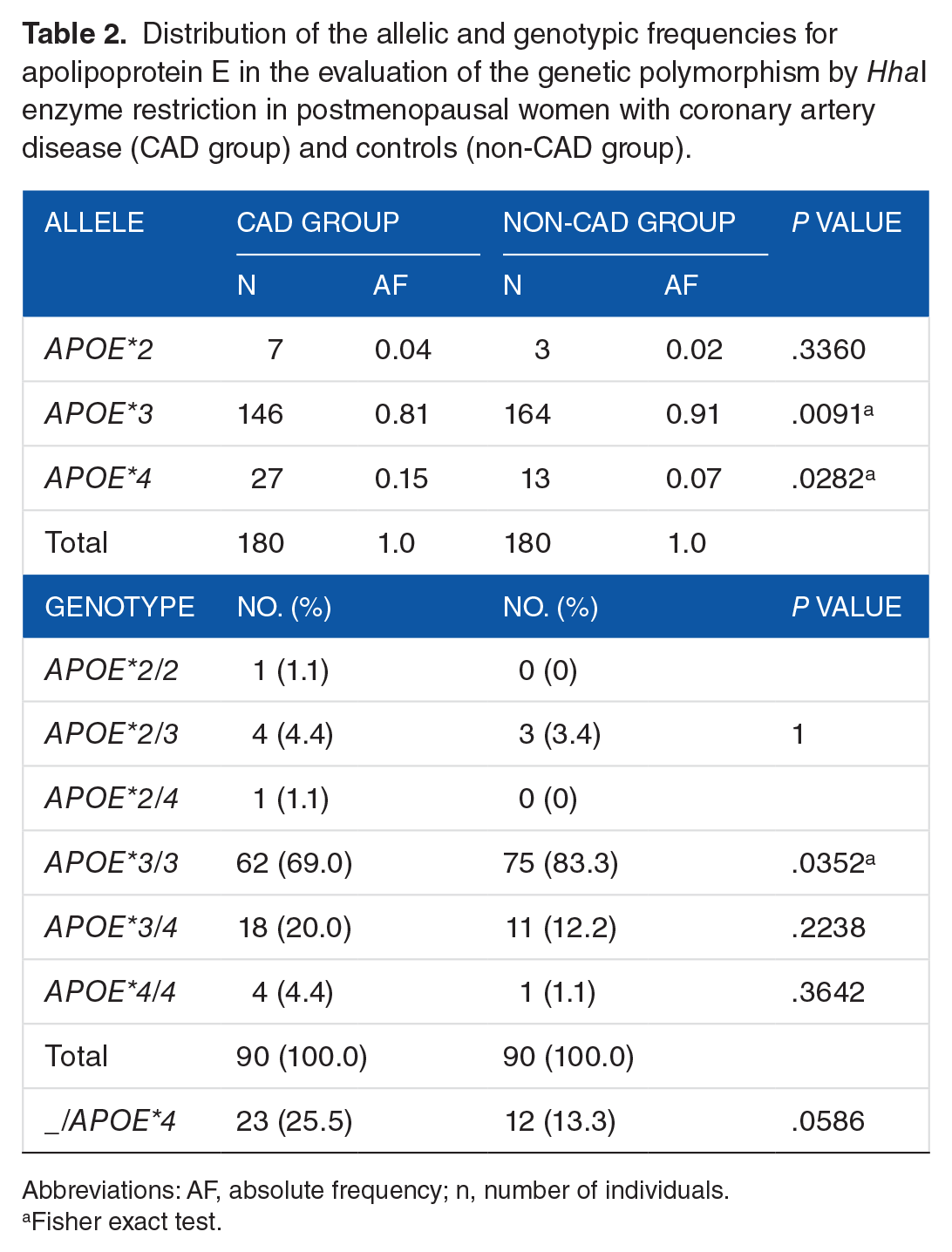
Abbreviations: AF, absolute frequency; n, number of individuals.
Fisher exact test.
Lipids and apoE polymorphisms
The mean values for the lipid profiles of CAD and non-CAD groups are presented in Table 3; both groups had increased levels of TC, LDL-C, VLDL-C, and TG; this was particularly true for patients with CAD who had significantly higher values when compared with non-CAD subjects (P < .01). Although the mean HDL-C concentration remained within the acceptable reference range, it was significantly lower in patients with CAD (50.2 ± 12.0 mg/dL) when compared with the non-CAD group (56.6 ± 16.7 mg/dL; P = .004).
Lipid profile in postmenopausal women with coronary artery disease (CAD group) and controls (non-CAD group).
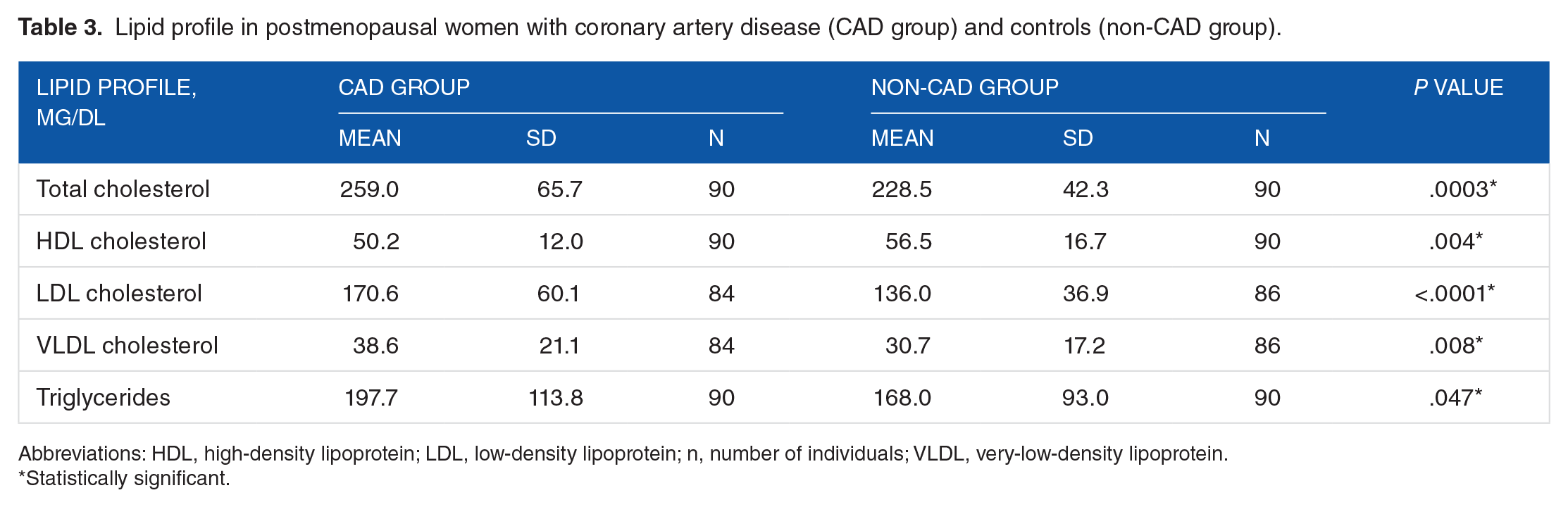
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein; n, number of individuals; VLDL, very-low-density lipoprotein.
Statistically significant.
Table 4 presents the mean values and standard deviations of the lipid profile in relation to the APOE*3/3 and _/APOE*4 genotypes. In the CAD group, there were increased values for all profiles except for HDL-C which was within the acceptable range for both genotypes. In the non-CAD group, the mean value of HDL-C was significantly higher in individuals with the _/APOE*4 genotypes than those with the APOE*3/3 genotype (70.8 ± 20.6, 56.5 ± 20.1 mg/dL, respectively; P = .02). Table 4 also presents a comparative analysis between groups for the apoE polymorphisms and lipid profile. The patients with the APOE*3/3 genotype had higher TC and LDL-C and lower HDL-C levels than controls (P < .05). For the _/APO*E4 genotype subgroup, lower HDL-C levels and higher TG levels were seen in patients compared with controls (P = .0005 and .023, respectively). On comparing both genotypes, there was no significant difference for the TC/HDL-C and LDL-C/HDL-C ratios between the CAD and non-CAD groups or individually within each group.
Lipid profile in postmenopausal women with coronary artery disease (CAD group) and controls (non-CAD group) in relation to APOE*3/3 and _/APOE*4 genotypes in postmenopausal women with coronary artery disease (CAD group) and controls (non-CAD group).

Abbreviation: n, number of individuals.
Statistically significant.
TG metabolic kinetics and apoE polymorphisms
For both groups, the TG levels were increased from 0 to 3 and 6 hours after the lipid-rich diet. However, at 3 hours the mean TG level had increased in the patients with CAD and non-CAD group (P = .444), and at 6 hours, it remained significantly higher in the CAD group compared with the non-CAD group (P < .05). Figure 1A shows that the areas under the curve were significantly higher in patients with CAD (1606) compared with non-CAD subjects (1447; P < .001).

Significantly greater areas under the curve in the patients with CAD (1606) compared with non-CAD group (1447; P < .001).
Individuals in the non-CAD group with _/APOE*4 genotypes showed significantly lower TG levels 6 hours after the ingestion of a lipid-rich diet (194.2 ± 111.7 mg/dL) compared with 3 hours after (251.5 ± 91.8 mg/dL; P < .01). However, non-CAD subjects with the APOE*3/3 genotype and patients with CAD independent of the genotype showed no signifcant differences in the TG levels 3 and 6 hours after the lipid-rich meal.
Figure 2 shows the areas under the curve in relation to the APOE*3/3 and _/APOE*4 genotypes in postmenopausal women. The area under the curve was significantly higher in the patients with CAD with _/APOE*4 genotypes compared with the controls (area = 1720 versus 1243; P < .001), whereas no difference was found between the groups for the APOE*3/3 genotype (area = 1518 versus 1487, respectively; P > .05).

Areas under the curve in relation to the APOE*3/3 and _/APOE*4 genotypes in postmenopausal women. Thus, the area under the curve is significantly higher in patients with CAD compared with controls both with _/APOE*4 genotypes (area = 1720 versus 1243; P < .001), whereas there was no difference between the groups in respect to the APOE*3/3 genotype (area = 1.518 versus 1.487, respectively; P > .05).
Discussion
This study confirms the association of risk factors for CAD and the apoE polymorphisms in postmenopausal women, specifically in relation to the APOE*4 allele. The lipid profile, although altered in both groups except for HDL-C, distinguishes the CAD and non-CAD groups. The APOE*4 allele, although associated with CAD, did not influence the lipid profile in either group, except for the fasting HDL-C level, which was higher in the non-CAD group. Even though the postprandial levels of TG are similar in both groups, the presence of the APOE*4 allele seems to be associated with accelerated clearance compared with the APOE*3 allele in the non-CAD group.
The postmenopausal women with CAD had high levels of TC, LDL-C, VLDL-C, and TG. After menopause, the TC levels and the small, dense particles of LDL increase, accompanied by an increase in TG and lipoprotein(a) and a reduction in HDL-C. The increase in the TG levels is particularly important because it is considered to be a better predictor of CAD in women than in men. 4 Studies of primary prevention in women, although few, revealed the same benefits as in men, as was demonstrated by the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS) 32 of 997 menopaused women under treatment using a lipid-lowering drug. The Scandinavian Simvastatin Survival Study, 33 a study of secondary prevention, also showed a significant reduction in the mortality risk (34%) of 827 women with levels of LDL-C between 213 and 310 mg/dL treated with lipid-lowering agents.
In this study, however, the levels of HDL-C, although lower in patients (50.2 ± 12.0 mg/dL) compared with controls (56.5 ± 16.7 mg/dL), were within the normal range. Elevated levels of HDL-C may have provided protection for the non-CAD group, as HDL is involved in the reverse transportation of cholesterol and maintenance of endothelial function and has important roles as an antioxidant and as protection against thrombosis. 4 The Framingham Heart Study demonstrated that low HDL-C levels constitute an independent risk factor for CAD. 34 The National Heart, Lung, and Blood Institute report, with data on 86 000 women from several cohort studies, demonstrated that in under 65-year-old women, reduced HDL-C levels and elevated LDL-C levels were associated with a higher risk of CAD. 35
Evidence accumulated from recent studies suggests that elevated levels of TG also constitute an important independent risk factor for CAD in women aged from 59 to 69 years. 36 In this study, both groups had elevated levels of TG but specifically the CAD group (P = .0468). In this case, there is reference of a 37% increased risk of mortality due to CAD after adjustments for other risk factors. 4 This reflects the atherogenicity of particles rich in TG, which can transport 5 times more esterified cholesterol than LDL. Furthermore, hypertriglyceridemia is associated with low levels of HDL-C and higher levels of highly atherogenic small, dense LDL particles. 35 Its effect is associated with blood hypercoagulability, platelet hyperaggregability, and alterations in fibrinolysis due to elevations of plasminogen activator inhibitor.
The association of genetic markers and cardiovascular disease has been reported in several studies, including with respect to the APOE*4 allele.37–39 Apolipoprotein E is also mentioned in the development of premature atherosclerotic disease along with apolipoprotein(a). 40 The high frequency of the APOE*4 allele in the Finnish population (23%) is associated with an increased risk of CAD17,41 and death due to the disease. 42 Cumming and Robertson 16 reported a prevalence of 0.233 for the APOE*4 allele in CAD, but only in women, with a value significantly higher than controls (0.147). Thus, this study, even though the prevalence of the APOE*4 allele (0.15) was low in postmenopausal women with CAD compared with other studies, is in agreement with the literature, with a significantly lower distribution in controls (0.07). In particular, this investigation corroborates the study by Salazar et al 18 of a sample of postmenopausal Brazilian women (48 ± 9 years) with angiographically diagnosed CAD, in which the APOE*3/4 genotype was more common in patients (40%) than in controls (14%). However, other studies sustain the absence of an association between apoE polymorphisms and CAD, including in survivors of myocardium infarction, 43 and different studies involving Chinese, 22 Brazilian, 18 and Greek populations. 44
The apoE polymorphisms have been associated with the diversity of the lipid profile, and the APOE*4 allele is considered to be a risk factor.45–47 Several authors agree on the influence of the apoE polymorphisms in the lipid metabolism.48,49 However, this study does not show any association between apoE polymorphisms and increased levels of TC and LDL-C or reduced levels of HDL-C, even with the significantly higher frequency of the APOE*4 allele in patients. Nevertheless, the Framingham Offspring Study, with a lower prevalence of the APOE*4 allele in postmenopausal women in relation to those in premenopause, showed an association between higher LDL-C levels and an increase in the mortality risk for patients with CAD. 50 Elevated levels of LDL-C and TC with the APOE*3/4 genotype were evident in individuals who survived myocardium infarction, as well as in a healthy Irish population. 37 However, in this study, although the TC and LDL-C levels were higher in individuals with the _/APOE*4 genotypes, especially in the patients, there was no significant difference between these values and the APOE*3/3 or _/APOE*4 genotypes in both groups.
A prospective study of 14 916 healthy men did not identify the APOE*4 allele as an independent risk factor for CAD but, as expected, an association between lower levels of HDL-C and elevated LDL-C and TG levels was found. 38 Guerra et al, 39 studying risk factors in obese children, did not find any association between insulin resistance and the apoE polymorphisms. Nevertheless, the CT/HDL-C and LDL-C/HDL-C ratios were higher in individuals with the APOE*4 allele than in those with APOE*3. In this study, the CT/HDL-C and LDL-C/HDL-C ratios were not associated with the genotypes.
Exogenous and endogenous pathways in the lipid metabolism show an influence on apoE polymorphisms in the lipid profile. Studies suggest that apoE2 determines a lower degree of absorption of intestinal cholesterol, whereas there is higher absorption with the apoE4 compared with the apoE3. According to Weintraub et al, 47 the faster removal of fat from the lipid-rich diet in individuals with apoE4 may be a possible mechanism to explain the higher level of LDL, as the greater capture of remnant particles would lead to a saturation of hepatic receptors and a consequent increase in these particles in the plasma. Furthermore, a higher concentration of remnant VLDL-C converted to LDL-C results in an increase in the concentration of LDL-C. This justifies, in part, the higher frequency of the APOE*4 allele among hypercholesterolemic patients, whereas the APOE*2 allele is more prevalent in hypertriglyceridemic patients when compared with the general population.43,45 The apoE2 possesses a low affinity for LDL and apoE receptors and thus binds weakly to them. This results in downregulation of the receptor and a subsequent decrease in LDL-C. Thus, apoE2 acts as a protector by reducing the participation of one of the factors involved in the development of atherosclerosis. In this study, due to the low frequency of the APOE*2 allele in patients (0.04) and controls (0.02), it was not possible to evaluate its association with the lipid profile.
The relationship between the apoE polymorphisms and CAD is not always associated with changes in the lipid profile as was observed in this study, even when only lipid and lipoprotein levels above the reference levels in individuals with the APOE*4 allele are taken into account. Although slight, the alteration in the lipid profile detected in APOE*4 individuals can represent a less favorable clinical evolution compared with patients with lower levels of cholesterol and without the APOE*4 allele, a subject for further research. Epidemiologic studies in secondary prevention have warned about the benefits of a reduction in the plasma cholesterol level. 33
In this study, significantly altered values of the lipid profile were found in patients with CAD when compared with non-CAD individuals independent of the presence of the APOE*4 allele. However, the non-CAD group showed higher HDL-C levels and reduced TG levels, differing significantly from patients with CAD. In this case, the study of subgroups with the APOE*3/3 and APOE*3/4 genotypes suggests that the APOE*4 allele is not implicated in the variations of the TC and LDL cholesterol in both groups and determined an increase in the HDL-C levels (70.8 ± 20.6 mg/dL) and a reduction in TG (131.2 ± 49.9 mg/dL), highly benefiting subjects in the non-CAD group compared with those with the APOE*3/3 genotype (56.5 ± 20.1; 174.6 ± 98.6 mg/dL, respectively).
In this study, it is possible that, in the non-CAD group, the reduction in some risk factors, including hypertension and familial history, contributed to the maintenance of desirable levels of HDL-C and TG, even in individuals with the APOE*4 allele. However, structural differences of the apoE isoforms can influence the metabolism and the synthesis of lipoprotein, altering its ability to interact with lipoprotein lipase during the conversion of VLDL to LDL. 51 This results in intense hydrolysis of the TG present in VLDL thereby reducing the TG levels. This profile was only observed in subjects in the non-CAD group with the _/APOE*4 genotypes when compared with those with the APOE*3/3 genotype. This results in an increase in LDL synthesis, 51 a condition that is also observed in the non-CAD group of this study with slightly altered mean levels of TC and LDL-C in the presence of _/APOE*4 (247.8 ± 41.7, 150.8 ± 40.2 mg/dL, respectively) compared with the APOE*3/3 genotypes (225.1 ± 42.3, 135.0 ± 35.2 mg/dL, respectively). This pattern was not observed in patients with CAD.
Alterations in plasma lipids mediated by apoE determine slight variations in the TG level. 45 Thus, it is possible that the transference of particles, including TG, phospholipids, proteins, and cholesterol esters, that occurs in the metabolism process and lipoprotein synthesis mediated by enzymes, may be accelerated in the presence of apoE4, thereby contributing to an increase in the HDL-C levels. Significant alterations have been reported in the cholesterol concentrations and in the TG metabolism rate after a lipid-rich meal.24,52 Higher variations in the TG plasma level have been described after a lipid-rich meal was consumed by healthy individuals, with the levels remaining high for a period of 3 to 9 hours.53,54 The patients with CAD presented with a significant increase in TG within the first 3 postprandial hours compared with fasting levels; levels remained high for between 3 and 6 hours, showing the slow removal of these particles. 54 These data were confirmed in the CAD group in this study. However, the non-CAD group, although presenting with a similar increase in TG within the first 3 hours, had a significant reduction in the mean level of TG at 6 hours.
Currently, there is much evidence showing the important role that postprandial lipemia plays in the atherogenic process. Hence, both chylomicrons, derived from the intestine, and VLDL, synthesized in the liver, contribute to triglyceridemia after the ingestion of fat. The postprandial increase in the number of TG-rich particles mainly occurs due to an increase in the level of large VLDL particles. 55 These particles accumulate after fat ingestion because of preferential lipolysis of chylomicrons by lipoproteic lipases. Consequently, VLDL particles represent 90% of the accumulated cholesterol present in TG-rich lipoproteins observed after fat ingestion and chylomicrons, and their remnants do not exceed 10% of the number of VLDL particles. The TG-rich particles correspond to 80% of the increase in cholesterol plasma concentration in the postprandial state. 56 Therefore, in this study, the increase in the levels of postprandial TG and its permanence in the circulation for up to 6 hours suggest a large increase in VLDL particles.
Structural differences of apoE isoforms determine their affinity to specific lipoprotein particles and may characterize their ability to interact with hepatic and lipoproteic lipases during hydrolysis of TG-rich particles, such as VLDL and chylomicrons, or interfere in the synthesis and removal of TG resulting in a delay of lipolysis and/or clearance of plasma TG. 57 Abnormalities in the postprandial metabolism have been associated with the cause of atherosclerotic disease. Many studies have shown disorders in the postprandial response of both diabetic and healthy individuals characterized by an accumulation of remnant particles and changes in their composition.58,59
In this study, individuals of the non-CAD group with _/APOE*4 genotypes presented with accelerated TG clearance when compared with those with the APOE*3 genotypes, resulting in significantly lower TG levels at 6 hours compared with 3 hours. This did not occur in the CAD group after the lipid-rich diet, with TG levels remaining high for at least 6 hours. In addition, in the controls, the APOE*4 allele was associated with higher levels of HDL-C, which may confer protection against cardiovascular disease in this group as HDL is involved in the reverse transportation of cholesterol.
By the way, the EARS II (European Atherosclerosis Research Study II) 59 analyzed whether a defect in the postprandial metabolism may constitute a genetically inherited risk factor. The results show a delay in TG-rich lipoprotein removal in patients with CAD when compared with control individuals, although the increased production of VLDL particles was not prevented. Thus, as in this study there was no difference with respect to the apoE phenotypes, even though the high TG levels were not tested after 6 hours, which is possibly too short a time to demonstrate any difference in the TG metabolism. It is believed that atherogenic TG particles are rich in cholesterol, and so, our results do not exclude the possibility that changes in the metabolism of TG remnants associated with certain apoE polymorphisms are connected to a higher risk of CAD in patients with a family history of the disease. 59
Hence, high levels of plasma TG and delay in the removal of TG-rich lipoproteins may identify a state of intolerance to fat associated with a high risk of CAD related to genetic control, a condition that cannot be detected in fasting TG measurements. Moreover, it is probable that the redistribution of cholesterol resulting from repeated increases in dietary fat would unfavorably modify plasma lipoproteins in such a way that the production of small, dense LDL particles and atherogenic TG would increase. 60
Several authors have agreed about the influence of apoE polymorphisms on the metabolism of lipids.48,49 The different isoforms of apoE interfere in the lipoproteic lipase activity during the conversion of VLDL to LDL. 51 Kinetic studies have shown a faster catabolization of apoE4 compared with apoE2, which is slower than apoE3.7,61 The apoE4 was associated with a faster removal of TG only in non-CAD individuals, and so, the difference may be attributed to lower TG fasting levels in this group as moderate increases in fasting TG constitute an impaired postprandial response.
Changes in plasma lipids mediated by apoE determine small alterations in the TG levels. 45 In the non-CAD individuals of this study, the _/APOE*4 genotypes were associated with higher levels of HDL-C and lower TG levels when compared with the APOE*3/3 genotype. This is contrary to other studies such as one on Australian Aborigines, where the high frequency of APOE*4 was associated with higher TG levels and reduced HDL-C levels, suggesting its contribution as one of the factors for high cardiovascular mortality. 62
However, more ample studies are necessary to clarify these aspects of lipid metabolism. It is evident that the predisposition for a complex disease such as CAD is determined by multiple genetic and environmental factors. Thus, the synergic effect among genetic polymorphisms, associated with environmental factors, could explain the variations in lipid profile.
Conclusions
In conclusion, the APOE*4 allele, although more common in postmenopausal patients with CAD than in the non-CAD group, does not influence the lipid profile. However, the APOE*4 allele seems to confer a protective effect when associated with elevated levels of HDL-C in healthy postmenopausal women. This effect may be enhanced as the APOE*4 allele is associated with quicker TG clearance compared with the APOE*3 in the non-CAD group.
Footnotes
Acknowledgements
The authors would like to thank the patients and the staff who participated in this project. They thank the reviewer, Mr David Hewitt, for correcting both the English spelling and grammar.
Peer Review:
Two peer reviewers contributed to the peer review report. Reviewers’ reports totaled 414 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
DRSS and LHBT conceived and designed the experiments and wrote the first draft of the manuscript. JCY-T analyzed the data. JCY-T, LNY, and MAdSP contributed to the writing of the manuscript. DRSS, JCY-T, and LHBT agree with manuscript results and conclusions. LHBT, DRSS, and LNY jointly developed the structure and arguments for the paper. LHBT, DRSS, LNY, MAdSP, and JCY-T made critical revisions and approved final version.
Disclosures and Ethics
As a requirement of publication, the authors provide to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy, and confidentiality. The authors have also confirmed that this article is unique and not under consideration or published in any other publication.