
Abstract
Cardiovascular toxicity in the form of cardiac dysfunction continues to be an obstacle for patients with cancer. Survival and quality of life of cancer survivors are frequently affected by increased incidence of cardiovascular disease. The involvement of the cardiovascular system by primary or secondary malignancies, as well as its dysfunction secondary to the administration of antineoplastics, has led to the development of a new discipline called Cardio-Oncology, an exciting cardiology subspecialty with more questions than answers and as a result an enormous opportunity for research in the field. Multidisciplinary efforts have been focused on the prevention, diagnosis, and treatment of cancer therapeutics–related cardiovascular dysfunction (CTRCD). This review article will focus on the early diagnosis of left ventricular dysfunction associated with chemotherapy. Currently, the identification of cardiac toxicity associated with cancer treatment is the cornerstone for critical decisions regarding anticancer therapy and cardioprotective strategies. Its early detection, especially in subclinical phases, allows immediate intervention to prevent further impairment of the myocardium and other cardiovascular structures. The most significant published studies were selected for this revision, providing an updated document for the health professionals involved in the care of patients with cancer. We examined the current evidence and recommendations for biochemical and noninvasive diagnostic techniques, including their specific role for identification of CTRCD. Traditional and advanced imaging modalities, used alone or in combination with cardiovascular biomarkers, are essential for the recognition of cardiotoxicity during cancer therapy. Evolving basic and clinical research are focused on the development of more sensitive and specific diagnostic tools and for the recognition of cardiac toxicity.
Introduction
Recent advancements in chemotherapy have improved outcomes of both solid and hematologic malignancies improving survival and allowing patients to have hopes for cure and better quality of life. However, cancer therapeutics–related cardiac dysfunction (CTRCD) is emerging as one of the major causes of morbidity and mortality among cancer survivors.1,2 The most common manifestations of cardiotoxicity secondary to chemotherapy include subclinical decline of left ventricular ejection fraction (LVEF), new-onset heart failure, conduction disorders, hypertension, thrombotic events, and cardiovascular ischemia. 3
Although a number of chemotherapeutic drugs such as cyclophosphamide, 5-fluorouracil, and vincristine in high doses are associated with CTRCD, the 2 most best characterized drugs associated with CTRCD are anthracycline and trastuzumab (Table 1). 2 Although the mechanisms by which these drugs cause cardiotoxicity are not fully understood, it is believed they work in different ways. Anthracycline increases oxidative stress leading to loss of myofibrils and vacuolization of the myocytes 4 ; it also blocks topoisomerase II enzymes by intercalating with double-stranded DNA, leading to breaks in DNA that cause apoptosis of cardiomyocytes. These effects are cumulative and dose dependent and are generally viewed as irreversible. 5 The estimated percentage of cardiomyopathy is 3% to 5% at a cumulative dose of 400 mg/m2, 7% to 26% at 550 mg/m2, and 18% to 48% at 70 mg/m2. 6 Trastuzumab blocks ErB2 signaling and affects cardiomyocytes in a non–dose-dependent manner but increases incidence of heart failure when used in conjunction with other agents. Incidence of heart failure of trastuzumab alone can reach 7% when used as monotherapy and increases to 27% when used with anthracyclines or other agents such as paclitaxel and cyclophosphamide. However, unlike anthracycline, the effects are usually reversible and cardiac function typically improves to baseline after discontinuation of the drug.3,7
Differences between classic patterns of cancer therapeutics–related cardiac dysfunction—type 1 (anthracyclines) and type 2 (trastuzumab) cardiotoxicity.

Abbreviation: dsDNA, double-stranded DNA.
Methods for early detection of subclinical cardiac injury are useful for selecting individuals who might benefit from therapeutic interventions to prevent further deterioration in left ventricular (LV) function with progression to subsequent cardiovascular events.8,9 Figure 1 highlights the progression of cardiovascular impairment after exposure to cancer therapy. The cornerstone for evaluating CTRCD is the use of noninvasive imaging techniques to assess the LV systolic function displacing cardiac biopsy as the preferred method. According to the last expert consensus for multimodality imaging evaluation of patients with cancer from the American Society for Echocardiography and the European Association of Cardiovascular Imaging, as well as the European Task Force, CTRCD is defined as a decrease in LVEF >10% to a value of <53% (or the lower limit of normality) with a repeat performed 2 to 3 weeks after the initial decrease is observed.9,10 However, despite significant advancements in imaging techniques and medical technology, there are several limitations conducting this assessment. There is considerable heterogeneity in technique and interpretation of the images, cumbersome to use on a regular basis, limited availability, and multiple contraindications to some of the imaging modalities. 11 Most notably, traditional noninvasive tests frequently used for evaluation of the LV function (ie, echocardiography and multigated blood pool imaging [multiple-gated acquisition (MUGA) scan]) may not detect significant CTRCD until there has been profound and likely irreversible myocardial damage.12,13
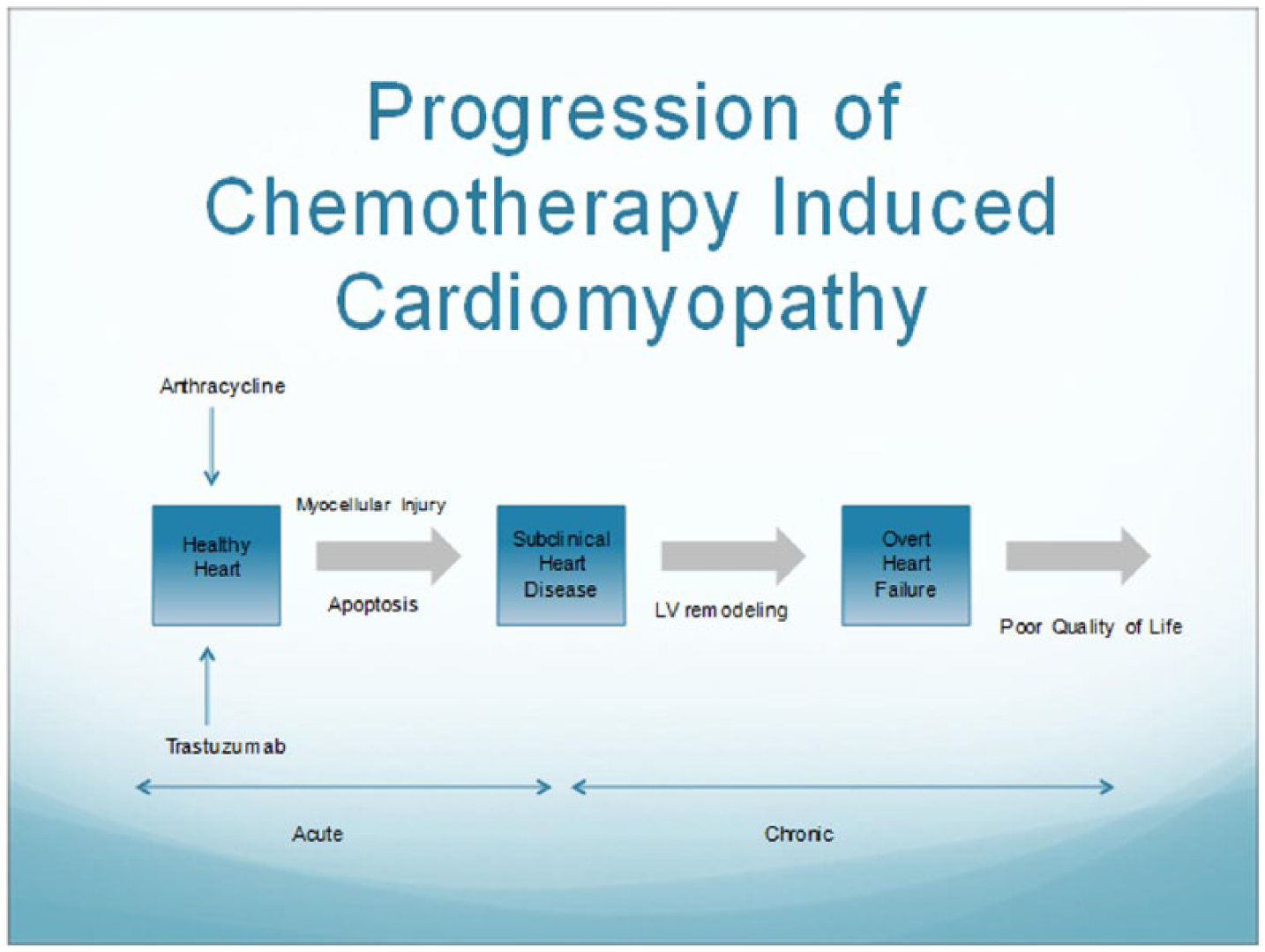
Progression of cancer therapeutics–related cardiac dysfunction. LV indicates left ventricular.
A potential alternative in detection of CTRCD is the measurement of cardiac biomarkers and the implementation of novel quantitative techniques such as strain imaging (Figure 2). This diagnostic approach may allow for early detection of cardiac toxicity and can offer an opportunity to provide interventions to reduce the risk of permanent cardiac dysfunction or subsequent cardiovascular events. 9 Some potential benefits of using biomarkers as a screening tool are that this strategy is easier to perform, noninvasive, cheaper, and reliable. The biomarkers that have been studied include cardiac troponin, B-type natriuretic peptide (BNP), C-reactive protein, and myeloperoxidase (MPO).

Stages of CTRCD and its diagnosis. 2D indicates 2 dimensional; CMR, cardiac magnetic resonance; LV, left ventricular; MUGA, multiple-gated acquisition.
Biomarkers
Troponin
Cardiac troponin is the gold standard biomarker in the assessment for myocyte damage, with both high diagnostic and prognostic value. It plays an important role in the diagnosis of acute coronary syndrome and myocardial injury 14 as it is released into the bloodstream during processes of myocardial cell disruption. It is located on the actin filament of myocytes and is essential for calcium-mediated cardiac muscle contraction. Recent advancements in troponin assays have increased the sensitivity of the biomarker to reflect cardiomyocyte injury with high sensitivity and specificity.
Elevation of troponins in patients receiving doxorubicin chemotherapy was first described by Lipshultz et al in children who were receiving treatment for acute lymphoblastic leukemia. 15 Since then, several studies have documented the role of this biomarker in patients undergoing cancer therapy. A follow-up prospective study by the same group found significant cardiac abnormalities in children who had at least 1 elevated troponin during treatment. 16 Another group investigated the utility of using early troponin measurements for predicting future cardiotoxicity.17–20 They documented a clear association between the pattern of troponin elevation and cardiovascular outcomes and prognosis. Patients undergoing high-dose chemotherapy for a variety of malignancies and who had negative troponins had no significant reduction in LVEF, demonstrating a high negative predictive value. Conversely, patients with early elevations in troponin had a decline of LV function and/or cardiac events of 37%, and those with both early and late positive biomarkers had an incidence of cardiac events of 84%. 19
However, studies investigating troponin in the setting of trastuzumab use are less well described and their results are less consistent with each other. In a study, Cardinale et al measured troponins in 251 women being treated for HER2+ breast cancer with trastuzumab. They reported that CTRCD occurred more frequently in patients with either baseline elevated troponin or elevations during treatment. Also, it was the only independent predictor of CTRCD and lack of LVEF recovery. In total, 60% of the women who developed LVEF dysfunction fully recovered after withdrawal of trastuzumab. 21 Conversely, other studies have shown no increase in troponin level after 12 months of follow-up in patients treated with trastuzumab for breast cancer 22 ; similarly, other investigators found that significant troponin elevation in the setting of trastuzumab therapy mainly occurred in patients who had been treated previously with anthracyclines or when trastuzumab is given in combination with other cardiotoxic agents. 23 In addition, a small study showed upregulation of myocardial HER2 (ErbB2) expression shortly after therapy with anthracycline, likely as compensatory mechanism due to cardiac exposure to oxidative stress. 24 Inhibition of HER2-neuregulin system in the heart (a pathway involved in the endogenous modulation of oxidative stress) by monoclonal antibodies shortly after cardiotoxic therapy may explain the elevated incidence of cardiotoxicity that has been found with the concomitant or sequential use of anthracyclines and trastuzumab.
Further research regarding cardiac troponin and its significance in CTRCD is needed. An important factor that needs to be characterized is the optimal diagnostic window for obtaining troponin level. The patterns in troponin elevation in acute myocardial infarction and catecholamine-induced cardiomyopathy are quite different, and it is therefore unwise to adopt either model for CTRCD.19,25,26 Adamcova et al 27 investigated the relation between anthracycline infusion, the pattern of troponin level elevation, echocardiographic parameters of LV function, and their correlation with CTRCD. Cardiotoxicity was induced by infusing daunorubicin weekly in an animal model. Multiple blood samples were drawn prior to and for several hours after the administration of anthracyclines (7 samples in total before and up to 1 week after the first, fifth, and eighth cycles). The group documented early troponin release during the first 24 hours after chemotherapy infusion with peak at 4 to 6 hours. However, they found persistent elevated troponin levels especially after the fifth cycle, describing a progressive elevation of the troponin values along with the cumulative dosage of the drug. It was shown that late and persistent troponin release in the setting of daunorubicin had a strong correlation with LV systolic dysfunction. The investigators suggested that measurement of troponin levels prior to forthcoming cycles of anthracyclines has a better predictive value and correlation with CTRCD than an early troponin release. Several other studies that may provide answers to this question are still in progress (Crohn’s Allogeneic Transplant Study [CATS] trial: NCT00858039, Detection of Cardiac Dysfunction in Patients Treated With Trastuzumab for HER-2 Positive Breast Cancer (CADY study): NCT00968682, A Multicenter Study in Patients Undergoing AnthRacycline-Based Chemotherapy to Assess the Effectiveness of Using Biomarkers to Detect and Identify Cardiotoxicity and Describe Treatment (PREDICT study): NCT01032278).
B-type natriuretic peptide
B-type natriuretic peptide is primarily produced in response to increased wall stretch and plays an important role in diagnosing heart failure with reduced and preserved ejection fraction (EF). N-terminal pro-BNP is an inactive protein of the BNP molecule that is cleaved from pro-BNP to release BNP. The results of BNP and its predictive value for CTRCD are mixed. It is possibly explained by virtue of the fact that many of the studies have small sample sizes, the heterogeneity of the population involved in the studies, and the diversity of clinical entities related to malignant disease and cardiovascular pathologies that are potentially associated with elevated BNP levels in the circulation.
A study involving 12 anthracycline-treated breast cancer patients with a cumulative dosage of >220 mg/m2 and with BNP >100 mg/mL was predictive of the development of heart failure. 28 Two other studies showed that persistently elevated levels of NT-proBNP for more than 72 hours were also predictive of LV impairment at 12-month follow-up with mean LVEF decreasing from 62.8% to 45.6%.29,30 In a larger study with 333 patients treated with anthracyclines, BNP was found to be an independent predictor of development of congestive heart failure and overall mortality. 31 Despite this evidence, the utility of BNP as a biomarker for CTRCD remains in question due to conflicting information, with several other studies showing no relationship and little prognostic value.22,32
There are several challenges in using BNP as a biomarker. First, natriuretic peptide levels serve as reasonable surrogates for both LV dysfunction and the cumulative dose of anthracyclines.33,34 Therefore, it is questionable whether BNP is just a marker for exposure to anthracyclines rather than true cardiotoxicity. Also, natriuretic peptides can be an unreliable biomarker as they tend to be influenced by age, gender, and other factors, including renal dysfunction, change in hemodynamic status, and obesity.
Other biomarkers
There are several other biomarkers under investigation that may show promise in predicting CTRCD. Myeloperoxidase is an enzyme that is involved in lipid peroxidation and is typically released in periods of inflammatory oxidative stress by neutrophils. Myeloperoxidase is being considered as a biomarker as it is believed that oxidative stress is one of the mechanisms of doxorubicin and trastuzumab cardiotoxicity. It was found in a study of 78 patients that a greater risk of cardiotoxicity (46.5%) was associated with patients with the greatest change in both troponin >0.121 ng/mL and MPO >422.6 pmol/L. This suggests that MPO can be an adjunct biomarker to troponin, although further studies are needed to confirm these findings. 35
Other biomarkers receiving attention are growth differentiation factor 15 (GDF-15), phosphatidylinositol-glycan biosynthesis class F protein (PIGF), soluble fms-like tyrosine kinase receptor-1 (sFlt-1), and galectin 3. GDF-15 is a member of the transforming growth factor β (TGF-β) cytokine superfamily with increased expression during events of ischemia, mechanical stretch, and oxidative stress. PIGF is a member of the vascular endothelial growth factor family and is under investigation as it may reflect the direct action of anthracycline and trastuzumab on angiogenesis. Galectin-3 levels are increased in patients with acute heart failure. None of these biomarkers were associated with increased risk of CTRCD, although these results may be due to small sample sizes.35,36
In summary, different biomarkers have been evaluated for the early diagnosis and prediction of CTRCD. Current studies have found a significant relation between late and persistent elevation of troponin level and the development of cardiac toxicity after cancer therapy. However, there are still unanswered questions regarding appropriate timing of the level measurements and its role in the surveillance during treatment using target therapies. However, the available evidence for other biomarkers is conflicting or has been derived from small studies requiring additional investigation. Further clinical research is currently underway to assess the role and timing of troponin and BNP testing in patients receiving anthracycline-based chemotherapy (PREDICT trial: NCT 01032278).
Cardiac Imaging Evaluation
Over the past decades, the LV function has been monitored throughout cancer therapy using serial 2-dimensional echocardiogram (2DE) or radionuclide ventriculography. 37 Furthermore, other methods are currently available for LV function quantification, including 3-dimensional echocardiogram (3DE), cardiovascular magnetic resonance (CMR), and strain speckle-tracking echocardiogram; however, they require sophisticated technology and advance medical and technical training compared with 2DE.
Multiple-gated acquisition scan
Historically, MUGA (also named equilibrium radionuclide angiography, multiple-gated acquisition scan, or equilibrium blood pool imaging) has been one of the preferred methods for serial assessment of LVEF while on cancer therapy. It was even considered the gold standard in the past for some groups due to its high reproducibility, lower inter- and intraobserver variability compared with 2DE, 38 and extensive validation literature. It is a noninvasive technique using 99mTc-labeled erythrocytes, which measures the cardiac blood pool through a γ-camera with electrocardiogram-triggered gated acquisition. It has been given class IA indication in the guidelines for cardiac monitoring while on chemotherapy.9,37,39 The guidelines recommended that cardiotoxic chemotherapy should not be given if baseline LVEF was 30% or less, and it should be discontinued if there is more than a 10% decrease in LVEF which results in LVEF values of less than 50%. 40 As a result of implementation of these recommendations, the incidence of heart failure due to chemotherapy decreased by 4 times. 41 Given the fact that LVEF determined by MUGA scan is more accurate and has more correlation with other 3-dimensional (3D) imaging modality (such as CMR) than echocardiography, it was considered that indirectly MUGA scan was responsible for that decrease. 42
The greatest limitation of MUGA scan has been the exposure to radiation, which will cumulate when performing the serial scans during the course of chemotherapy. In an adult patient, during each MUGA scan, radiation-absorbed doses to the critical organs (adrenals, heart, kidneys, liver, and spleen) are 8, 18, 14, 10, and 11 mGy. 43 In addition, pregnancy being a relative contraindication to undergo this test, other techniques, such as echocardiography or magnetic resonance imaging, are the preferred imaging modalities in this condition. Similarly, breastfeeding must be interrupted for 12 to 24 hours post study when using in vivo–labeled red blood cells because of the presence of free 99mTc-pertechnetate. 43 Another limitation of this technique is that the MUGA scan cannot be used for the accurate evaluation of right ventricular (RV) function due to the overlap between RV and right atrium. In addition, although highly reproducible, there are many potential sources of error that can lead to inaccurate assessment, such as inadequate labeling of erythrocytes with a reduced target-to-background ratio, inaccurate definition of the LV region of interest, and incorrect gating due to variability in heart rate, especially in the setting of conduction disorders, eg, frequent premature ventricular contractions and atrial fibrillation.
Multiple-gated acquisition scan has been tested by time to be an excellent noninvasive modality in serial measurement; however, a large retrospective study has shown that it is not accurate in heart failure prediction. 6 Similar to echocardiography, by the time LVEF is depressed, there is already enough myocardial damage that has happened. Detection of myocardial injury before irreversible LV dysfunction should be the goal to prevent it before even happening.
Two-dimensional echocardiography
Structural and functional evaluation of the heart prior to antineoplastic therapy with known cardiotoxic effects is strongly recommended.8,9 Due to its widespread availability, low cost, and great safety profile, echocardiography is currently the preferred imaging modality used in most of the centers for initial evaluation and surveillance of cardiac toxicity. It not only allows a complete evaluation of the myocardial function but also provides complementary information about great vessels, pericardial structure, heart valves, diastolic parameters, and hemodynamic conditions.
Historically, LVEF has been considered one of the most important echocardiographic predictors of adverse cardiovascular outcomes 44 and the parameter most frequently used for longitudinal monitoring of cardiac toxicity. In daily clinical practice, LVEF is most frequently derived from volumetric calculation obtained from 2DE or 3D echocardiography. 45 The current guidelines for cardiac chamber quantification recommend the biplane method of disks (modified Simpson’s rule) as the preferred 2DE method to assess LV volumes from the apical 4- and 2-chamber views. 45 Moreover, although 2-dimensional (2D) echocardiography technique has several advantages as previously discussed, it depends on imaging quality. Its accuracy is affected by apical foreshortening, endocardial dropout, poor echocardiographic windows, and geometrical assumptions of the LV shape. Also, echocardiographic parameters are influenced by changes in contractility, hemodynamics, and loading conditions. In addition, it is well documented that 2DE has a low sensitivity for detection of early impairment of myocardial function and subclinical cardiotoxicity. 13 In a recent study, adult survivors of childhood cancer with history of exposure to cardiotoxic therapy were screened for asymptomatic/subclinical cardiomyopathy. The investigators reported a low sensitivity and high false-negative rate by 2DE, 25% and 75%, respectively, for detection of EF lower than 50% compared with other imaging modalities (3DE and CMR). 13 In addition, it is documented that the decline of LVEF in patients with a prior exposure to cardiotoxic chemotherapeutic regimen represents an advanced stage of myocardial dysfunction, 46 and it is a marker for severe cardiovascular damage and/or reduced response to cardioprotective measurements.19,47 For those reasons, the LVEF is considered an insensitive tool for detecting cardiotoxicity at its early stage.9,48
In view of the limited factors discussed above, different echocardiographic techniques are available at this time for clinical evaluation and risk stratification of the cancer population, as well as for surveillance of cardiotoxicity. Contrast echocardiography, Doppler tissue imaging (DTI), 3DE, and speckle-tracking echocardiography (STE) are echocardiographic modalities that have been recently developed, which provide additional information to improve the accuracy of the cardiovascular evaluation.
Endocardial border dropout is a frequent limiting factor for 2DE reducing its accuracy for volumetric measurement. The current guidelines for chamber quantification recommend the use of contrast if 2 or more contiguous LV endocardial segments are not adequately visualized in apical views.45,49 It should be considered if improvement of endocardial definition is required as part of the echocardiographic evaluation of the cancer population, especially in patients with breast cancer who frequently require surgical procedures, reconstructive techniques, and/or radiation therapy. In the same way, complete evaluation of the diastolic function is recommended in all patients who are undergoing echocardiographic screening. 8 Early and late changes in diastolic parameters obtained using pulsed Doppler and Doppler tissue imaging (DTI) have been reported in the setting of cancer therapy. 50 However, their dependency on loading conditions—an important and highly variable factor in cancer therapy—the characteristic limitation of DTI by the acquisition angle and sample location, and its low capacity for differentiating the tethering effect of adjacent segments are well-recognized factors that limit their role as a predictive tool for CTRCD. 8
Finally, stress echocardiogram has a defined role during the evaluation of patients with malignant disease prior to anticancer therapy. It is frequently used for risk stratification of patients with elevated risk of coronary artery disease (CAD) prior to cancer treatment, especially if the chemotherapeutic agents have been associated with myocardial ischemia. 3 In those situations, it is recommended that current guidelines for screening and prognostication of stable CAD in general population be implemented. 51
3D echocardiography
Over the past years, 3DE has been gaining an important role in the assessment of cardiac structures, chamber volumes, and myocardial function, offering the accessibility of 2DE and the multidimensional evaluation of CMR (Figure 3). 52 Its better correlation with CMR compared with the traditional 2DE in the measurement of LV volumes and LVEF was documented in a recent meta-analysis. 53 This report was derived from 23 studies that included 1174 patients in whom 2DE and 3DE performance was analyzed compared with CMR. It was documented that both echocardiographic techniques underestimate LV volumes, but not EF, compared with the reference standard (CMR). However, 3DE demonstrates a superior accuracy for volumetric measurement and precision for EF estimation, as well as lower intra- and interobserver variability than 2DE. In another study using CMR for CTRCD screening on cancer survivors, Armstrong et al 13 demonstrated a higher sensitivity and lower false-negative rate for detection of low EF (<50%) by 3DE compared with 2DE. In the same way, other studies have reported similar findings regarding 3DE performance in monitoring oncologic patients. Thavendiranathan et al 54 followed the myocardial function of 56 patients who underwent chemotherapy with or without radiotherapy for breast cancer. They found stable global longitudinal strain (GLS) in all patients for 12 months, a sign of no cardiac toxicity. It was correlated with 2DE and 3DE, considering any variation in LVEF as temporal variability of the imaging technique rather than a secondary effect from the cancer therapy. Three-dimensional echocardiogram, using an automated or semiautomated endocardial contouring method, proved to be the echocardiographic modality with the lowest temporal variation during longitudinal monitoring and the lowest intra- and interobserver variability.
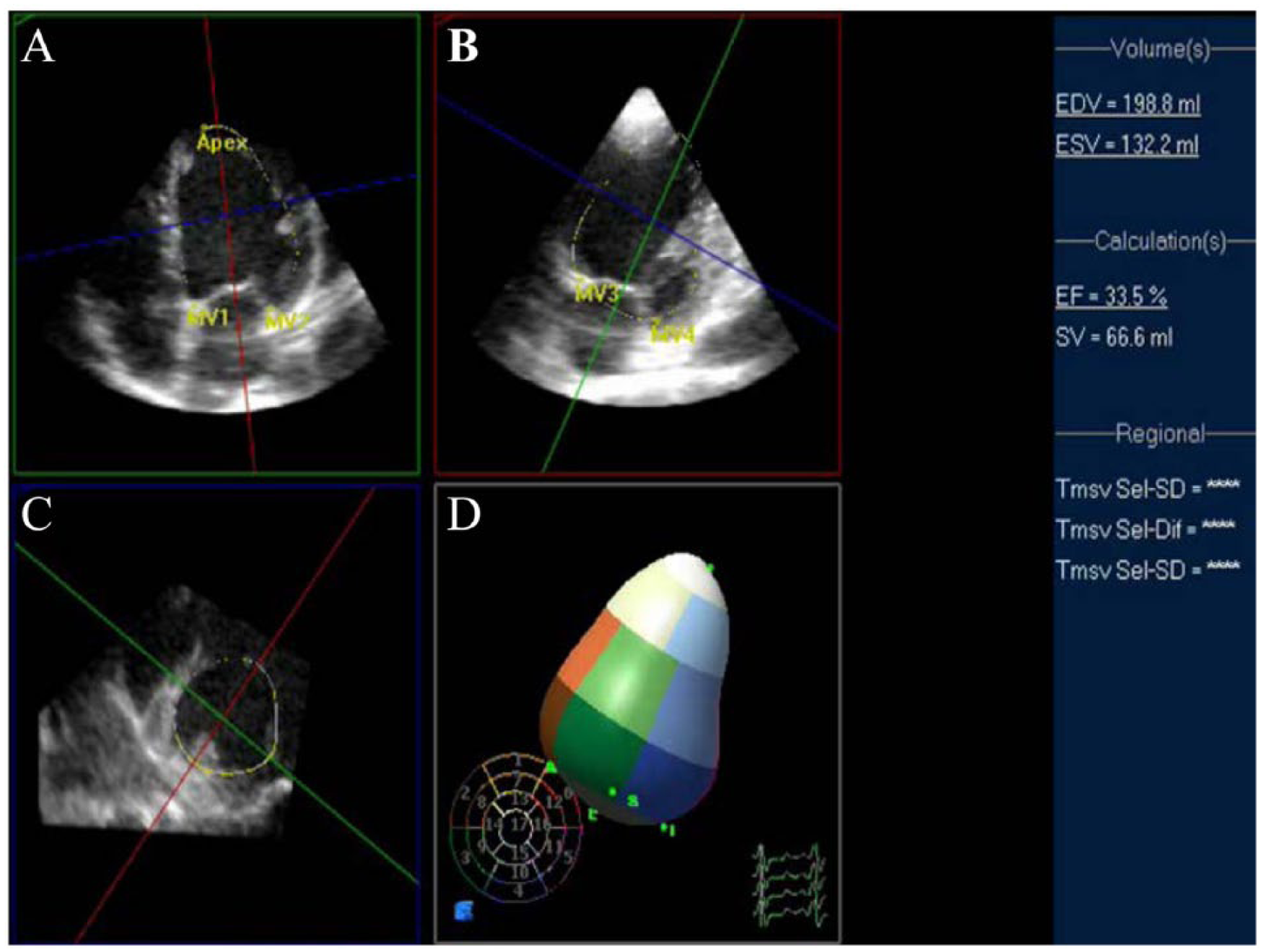
Real-time 3-dimensional echocardiogram (3DE). Left ventricular volume measurements and ejection fraction calculation using semiautomated endocardial delineation. (A) Apical 4-chamber view, (B) apical 2-chamber view, (C) short axes view, and (D) 3-Dimensional reconstruction of the left ventricle for volumetricmeasurements. EDV indicates end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; SV, stroke volume. (Courtesy D. Spevack, MD)
The improvement in performance characteristics of 3DE and its better correlation with the current criterion standard (CMR) compared with 2DE have been associated with the fact that volumetric measurements do not rely on geometrical assumption, and they are not affected by foreshortening of the LV apex. 53 Due to its accuracy, highly reproducibility, and low intra- and interobserver variability, 3DE has been recommended as the preferred method for serial monitoring of cardiac toxicity, if available and feasible at the echocardiographic laboratory.8,45 Finally, despite its demonstrated role in cardiovascular surveillance after cardiotoxic therapies, 3DE technique is not widely available in clinical practice. Its accuracy depends on imaging quality, and as mentioned above, its implementation requires expensive technology and expertise by sonographers and interpreters.
Speckle-tracking echocardiography
In the recent years, there have been significant advances in the field of echocardiography, especially strain imaging using speckle tracking, also known as deformation imaging. Strain is calculated as the fractional change in the length of a myocardial segment and is expressed as a percentage. In addition, strain rate is the temporal change of strain and measures the velocity at which myocardial deformation occurs. Strain and strain rate can be measured in 3 dimensions—longitudinal, radial, and circumferential—each of which can be measured for a predefined region or globally for the entire ventricle. Average peak systolic GLS is calculated using the average of longitudinal strain measurements from 3 long-axis views of the heart (Figure 4). Until now, of the 3 dimensions, only GLS has reliably and consistently shown to be of significance in predicting progression to CTRCD. 55 During the chemotherapy, more than 15% change in GLS from baseline is considered as abnormal and a likely predictor of CTRCD. 8 However, this cutoff of 15% is based on limited data, and large studies are needed to confirm this threshold.

Global longitudinal strain assessed by speckle-tracking echocardiography. Measurements are obtained from the 3 apical views and averaged.
In a meta-analysis of 16 articles with 5721 patients with varied causes of underlying cardiac dysfunctions, such as heart failure, acute myocardial infarction, and valvular heart disease, GLS was proven to be superior compared with LVEF for predicting overall mortality and major cardiac events. 12 The advantages of STE for evaluation and cardiotoxicity monitoring have been well documented. In a large cohort of cancer survivors, almost one-third of patients with a normal 3D LVEF have abnormal GLS. Also, early changes in GLS predicted reduction in LVEF and subsequent clinical heart failure at 15 months of follow-up. 56 In the same way, it has been shown that in patients treated with trastuzumab, change in GLS was able to predict its detrimental effects on LV systolic function, well before any decrease in LVEF occurred.57,58 In an observational study, GLS reduction was significantly higher in the group receiving both anthracyclines and trastuzumab than that in the group receiving trastuzumab only. Of the 52 patients with a significant change of GLS in this study, only 14 had a decrement of EF that would have justified a diagnosis of CTRCD based on current criteria. Notably, treatment with β-blockers significantly improved the LVEF and GLS. 59 Thus, GLS might be helpful in identifying patients with early evidence of subclinical LV dysfunction who will benefit from the initiation of cardioprotective therapy which could prevent subsequent progression to heart failure (Figure 5). Observational nature of this study precludes its generalization; nevertheless, it gives a signal of future trial design.

Bull’s-eye plot of a 60-year-old patient with breast cancer who received anthracycline-based chemotherapy followed by trastuzumab.
Loading condition dependency, no clear reference values, intervendor variability, and lack of universal standardization are the main problems with this advanced echocardiographic technique. Given that the absolute values of strain in the same patient vary by different vendor and software used for image acquisition and processing, relative change in strain values over time using the same vendor should be used for monitoring rather than a single point value at only one time. A recent publication showed that the combined subendocardial GLS and subepicardial LV twist has better predictive value compared with GLS alone in the development of CTRCD. 60 Strain by 3D speckle tracking has emerged as a further advancement to provide even greater insight. More data is needed before recommending either method for routine clinical use.
Finally, a multinational, multicenter, randomized controlled clinical trial (SUCCOUR [Strain Surveillance during Chemotherapy for improving Cardiovascular Outcomes, ACTRN12614000341628]) 61 is already on its way. It was designed to determine whether serial strain imaging in patients receiving cardiotoxic chemotherapy will reduce the incidence of overt heart failure compared with current recommendations of standard LVEF. This ongoing investigation will provide new evidence-based data regarding the clinical utility and advantages of STE for monitoring of cardiotoxic therapies.
In summary, despite the advantages of traditional noninvasive imaging modalities for the CTRCD surveillance, 2DE and MUGA scan have important limitations as previously discussed. However, the implementation of novel echocardiographic techniques, including 3DE and STE, has improved the sensitivity for early identification of myocardial damage secondary to chemotherapeutic toxicity. Ongoing prospective clinical studies will support their clinical implementation for monitoring of cardiac toxicity during cancer therapy. Finally, evolving echocardiographic techniques, eg, strain by 3DE speckle tracking and myocardial torsion, will allow a better understanding of early abnormalities in myocardial mechanics derived from cancer therapies, providing new tools for the development of more sensitive and specific diagnostic tests.
CMR imaging
Because of its 3D evaluation of the cardiac structures and its accurate volumetric estimation, CMR imaging has become the reference standard for assessing LV systolic function and volumes.9,62 In patients with heart failure or LV hypertrophy, CMR has been validated to be more accurate and reproducible compared with routine MUGA scan, 2D and 3D echocardiography.63,64 It is not just the accurate volumes and EF but the ability of CMR to perform tissue characterization, identifying fibrosis 65 and edema, that makes the use of this technique attractive in Cardio-Oncology.
In an animal model with doxorubicin exposure, CMR has shown to accurately identify precursors of LV dysfunction, which was also proven on biopsy. 66 This has been reproduced in 65 humans with breast cancer or hematologic malignancy with and without prior exposure to chemotherapy. An increase in signal intensity within the LV myocardium on contrast-enhanced T1-weighted images is associated with a reduction in LVEF. 67 Similarly, a small retrospective study showed delayed enhancement of the subepicardial lateral wall of the LV in patients with breast cancer is highly indicative of trastuzumab-induced myocarditis. 68 However, further investigation is required to confirm these findings. Conversely, other investigators reported that myocardial late gadolinium enhancement on CMR was infrequent in patients with anthracycline cardiomyopathy with a reduced LVEF. Nevertheless, in this study, a decrease in LV mass index by CMR imaging was a predictor of CTRCD. 69
Finally, CMR should be considered if the echocardiographic assessment is inadequate. Its high cost, longer image acquisition time, and low availability have hindered the widespread use of CMR for serial cardiac function monitoring in patients with cancer. Table 2 highlights the characteristics of different noninvasive imaging techniques recommended for evaluation and surveillance of CTRCD.
Characteristics of noninvasive imaging techniques recommended for evaluation and monitoring of patients undergoing chemotherapy with known cardiotoxic effects.

Abbreviations: 2D, 2-dimensional; 2DE, 2-dimensional echocardiogram; CMR, cardiovascular magnetic resonance; CTRCD, cancer therapeutics–related cardiovascular dysfunction; ECHO, echocardiography; LV, left ventricle; LVEF, left ventricular ejection fraction; MUGA, multiple-gated acquisition; RWMA, regional wall motion abnormalities.
Future directions
Stronger evidence supporting the role of early cardiotoxicity detection and its long-term impact on cardiovascular outcomes must be attained through further investigation. New knowledge derived from large multicenter randomized clinical trials is needed, especially if the studies include different populations affected by diverse malignancies, allowing a broader applicability of the evidence. In addition, standardization of protocols of advanced imaging techniques, definition of clear reference values, and resolution of intervendor variability are necessary for their universal implementation. Finally, close evaluation of the reliability of the implementation of the new noninvasive imaging techniques in the community is needed.
Limitations
Prior studies suffer from the paucity of recent data, especially in the field of new technologies such as strain echocardiography, 3DE, and CMR. Our review is the state of the art in this field and in sync with the recently published guidelines on a similar topic. A significant part of the current knowledge in this evolving area has been derived from small prospective clinical trials or retrospective and observational studies. Multicenter larger clinical trials are desired to strengthen the growing evidence-based clinical knowledge in this field. Other identified factors that could limit the applicability of the current evidence to all patients with cancer are the homogeneity of the population involved in the studies (predominantly white population) and the different technical protocols used in the studies for implementation of diagnostic techniques.
Conclusions
Early identification and treatment of subclinical LV dysfunction associated with cancer therapy is essential for improvement of cardiovascular outcomes. Vertiginous advances on the cardiovascular field have led to scientific and technological progress in laboratory test and imaging techniques, improving the availability of diagnostic tools in research and clinical practice. Current expert consensus recommends a comprehensive evaluation of the patient at risk of CTRCD; it includes the use of traditional and novel noninvasive imaging techniques as the preferred diagnostic method, as well as an integrated approach combining biomarkers and imaging modalities for risk stratification and surveillance of cardiotoxicity in selected patients (see Figures 6 and 7). Volumetric measurements, calculation of LVEF, and evaluation of LV function should be conducted with the most accurate method available in the institution. Finally, because all the available imaging techniques have their own advantages and limitations, it is recommended to follow the patient with the same imaging modality chosen during the initial assessment. Future prospective randomized controlled trials are required to determine the optimal diagnostic approaches using traditional and new biomarkers, as well as novel noninvasive imaging techniques. These strategies should be individualized taking into account the patient’s cardiovascular risk and the potential cardiotoxic effect of the therapy planned.

Evaluation and follow-up of patients receiving anthracyclines. 2DE indicates 2-dimensional echocardiography; 3DE, 3-dimensional echocardiography; CMR, cardiac magnetic resonance; CV, cardiovascular; ECG, electrocardiogram; GLS, global longitudinal strain; LVEF, left ventricular ejection fraction; LLN, Lower Limit of Normal.

Evaluation and follow-up of patients receiving trastuzumab. 2DE indicates 2-dimensional echocardiography; 3DE, 3-dimensional echocardiography; CMR, cardiac magnetic resonance; CV, cardiovascular; ECG, electrocardiogram; GLS, global longitudinal strain; LVEF, left ventricular ejection fraction; LLN, Lower Limit of Normal.
Footnotes
Peer review:
Six peer reviewers contributed to the peer review report. Reviewers’ reports totaled 571 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors participated in the preparation of the manuscript, and all of them have read and approved the content of the paper.