
Abstract
We report a first case of hallux rigidus successfully treated in an elderly patient by intra-articular infiltration of cross-linked hyaluronic acid (HA) 21 mg/mL with mannitol (Desirial Plus) and review the previous literature on the different compositions of HA infiltrative treatment applied to hallux rigidus. A 77-year-old female patient with moderate unilateral pain of 6 months of evolution and stiffness of the movement of the first metatarsophalangeal joint of the left foot, corresponding to grade 2 of the classification proposed by Coughlin and Shurnas. The objective of the study was to perform a pilot test to (a) evaluate the correct technique of intra-articular infiltration as well as (b) the use of a commercial cross-linked HA 21 mg/mL with mannitol, to a voluntary patient diagnosed with hallux rigidus. A single cross-linked HA infiltration is applied to the first metatarsophalangeal joint with an administered amount of 1 mL. The loaded dorsiflexion, the unloaded dorsiflexion, and the unloaded plantarflexion angles of the first metatarsophalangeal joint improved from 15°, 20°, and 10°, respectively, before injection to 45°, 52°, and 22°, respectively, at 14 days after injection. Moreover, these improvements maintained until the final follow-up (400 days). The intensity of pain, according to the visual analog scale, improved from 7 of 10 before the injection, passing through 4 of 10 at 14 days after the injection, to 1 of 10 at 60 days after the injection. Cross-linked HA 21 mg/mL with mannitol improves symptomatology, joint mobility of the first metatarsophalangeal joint, and quality of life in the patient with stiff hallux submitted to the pilot test. These effects have been maintained for more than 14 months.
Introduction
Hallux rigidus (HR) is defined as a degenerative and progressive evolution of osteoarthritis of the metatarsophalangeal (MTP) joint of the first toe, the hallux.1-4 Clinically, it is characterized by pain, a sensation of joint stiffness, a progressive loss of the range of movement of the first MTP joint, mainly from extension to the sagittal plane, and the formation of dorsal or periarticular osteophytes. 1
The Coughlin and Shurnas classification (2003), the most cited and the most complete, assesses clinical and radiological parameters. It divides the HR into 5 grades (from 0 to 4) requiring the inclusion of subjective symptoms (pain in different areas of the range of motion) in the anamnesis, physical examination (range of motion, expressed in degrees), and a radiological evaluation.5,6 The diagnosis of HR is based on an anamnesis with physical examination, visual inspection, and complementary tests.
Regarding treatment, there are 2 possibilities: conservative and surgical treatment. Conservative treatment includes shoe modifications, 7 orthopedic insoles, drug treatment, hyaluronic acid (HA) infiltrations 8 or corticosteroids, and physical therapy.2,4,9-11 Surgical treatment is indicated when it is not possible to reduce pain or improve gait with conservative treatment, or to respond to the patient’s specific requirements (degree of deformity, complementary activities, daily work, etc). 4
In foot surgery, HA infiltrations constitute an alternative to conservative pharmacologic treatment or may be the first option to treat pain and reduce inflammation with fewer undesirable and more beneficial effects. 1 Currently, they are used in ankle joint infiltrations 12 as well as for Morton’s Neuroma, 13 MTP arthritis, 14 and even for the treatment of infected ulcers in patients with diabetes. 15
The results of 5 clinical trials carried out to date report the efficacy of HA injections to relieve pain and improve joint function.14,16-19 Four of these studies analyze the results of non-reticulated HA at different concentrations.14,16,18,19 Two non-comparative studies analyze only the use of non–cross-linked HA16,17; 1 study compares HA without cross-links with a placebo (saline solution) group 18 ; a third study compares the results between non–cross-linked HA and triamcinolone acetonide. 14 Finally, a single study analyzes the clinical efficacy of HA cross-linked with mannitol. 19
Cross-linked HA 21 mg/mL with mannitol helps to reconstitute moderately or severely hypertrophied tissues and causes a lasting increase in the volume and hydration status of the “labia minora” in postmenopausal women, as demonstrated by a study by Berreni et al 20 after the clinical trial conducted by Boucher. 21 In addition, the treatment decreases the inflammatory symptoms of patients. The treatment proposal of this study is based on recovering the intra-articular volume to improve joint mechanics which, added to the anti-inflammatory activity of the infiltrating product, will act in synergy to improve the signs and symptoms of the MTP joint.
In this case, with a volunteer patient with painful HR, treated at the Virginia Novel Podiatry Hospital of the University of Barcelona, we analyzed different parameters: the intensity and effective time of pain treatment and degrees of movement of the first MTP joint. The latter being the most important, as in the bibliography analyzed, none of the articles refers to the value in degrees of movement of plantar flexion and extension of the joint that increase or decrease with the treatments.
Case Presentation
A 77-year-old woman attended the Virginia Novel Podiatry Hospital of the University of Barcelona referring unilateral pain in the first MTP joint of the left foot of 6 months evolution previously diagnosed as HR grade 2 of the Coughlin and Shurnas classification.5,6 She reports a pain intensification both in the erect position and during bipedal gait. When assessed with the “visual analog scale” (VAS), the pain intensity value was 7 of 10.
The relevant medical history reveals arterial hypertension and hypercholesterolemia. The podiatry history includes personalized therapeutic insoles since October 2021 and an infiltration of corticosteroids in the plantar fascia of the left foot in 2019.
Physical examination
The patient presents an Egyptian foot, minus index, and normal skin surface temperature. The metatarsal head bunion is visible as a red and brilliant protrusion in the medial vision (Figure 1A). Neither alteration nor absence of hair growth is observed on the dorsum of the foot. She presents also a bilateral fourth finger hammer toe with no other evident skin or nail lesions (Figure 1B). On palpation, she manifested pain in the gastrocnemius muscle, medial and central fasciculus of the plantar fascia, along the course of the peroneus longus and the tibial anterior muscles of the left foot.

Inspection of a patient with HR: (A) dorsoplantar view in load position showing both feet and (B) profile image in charge where the dorsal bunion can be seen. DB indicates dorsal bunion.
A profile X-ray is taken in the loaded position to assess the eventual presence of osteophytes (Figure 2).

Profile X-ray of the left foot in loaded position. White arrows signal the osteophytes. D indicates dorsal; MH, metatarsal head; PPhB, proximal phalanx base.
From the neutral position of the first MTP joint, the practitioner assessed the extension and plantar flexion of the joint resistance is noted according to the method of Munteanu and Bassed 22 and Kappel-Bargas et al. 23
The results of the joint mobility assessment in unloaded position were as follows: 20° extension of the first MTP joint of the left foot, limitation of the extension movement of the tibiofibular-talar joint of the left ankle, and reduced internal rotation capacity in the lower extremity left. On the other extremity, the first MTP joint of the right foot showed 40° of extension. Plantar flexion and extension movement of the explored joints of the right foot were preserved.
The PodoScope (Figure 3A) for foot scanning and the computed study (Figure 3B) carried out in standing (load) position allows to determine the following parameters:
Jack test 24 : bilateral positive.
Test of resistance to supination 25 : bilateral negative.
Maximum pronation test 26 : bilateral positive.
Assessment of first MTP joint: HR of the left foot and FnHL of the right foot.
Bilateral hindfoot varus position (more accentuated in the right foot).
Increased pressure in the plantar zone of the central rays and absence of support of the belly of the bilateral hallux.
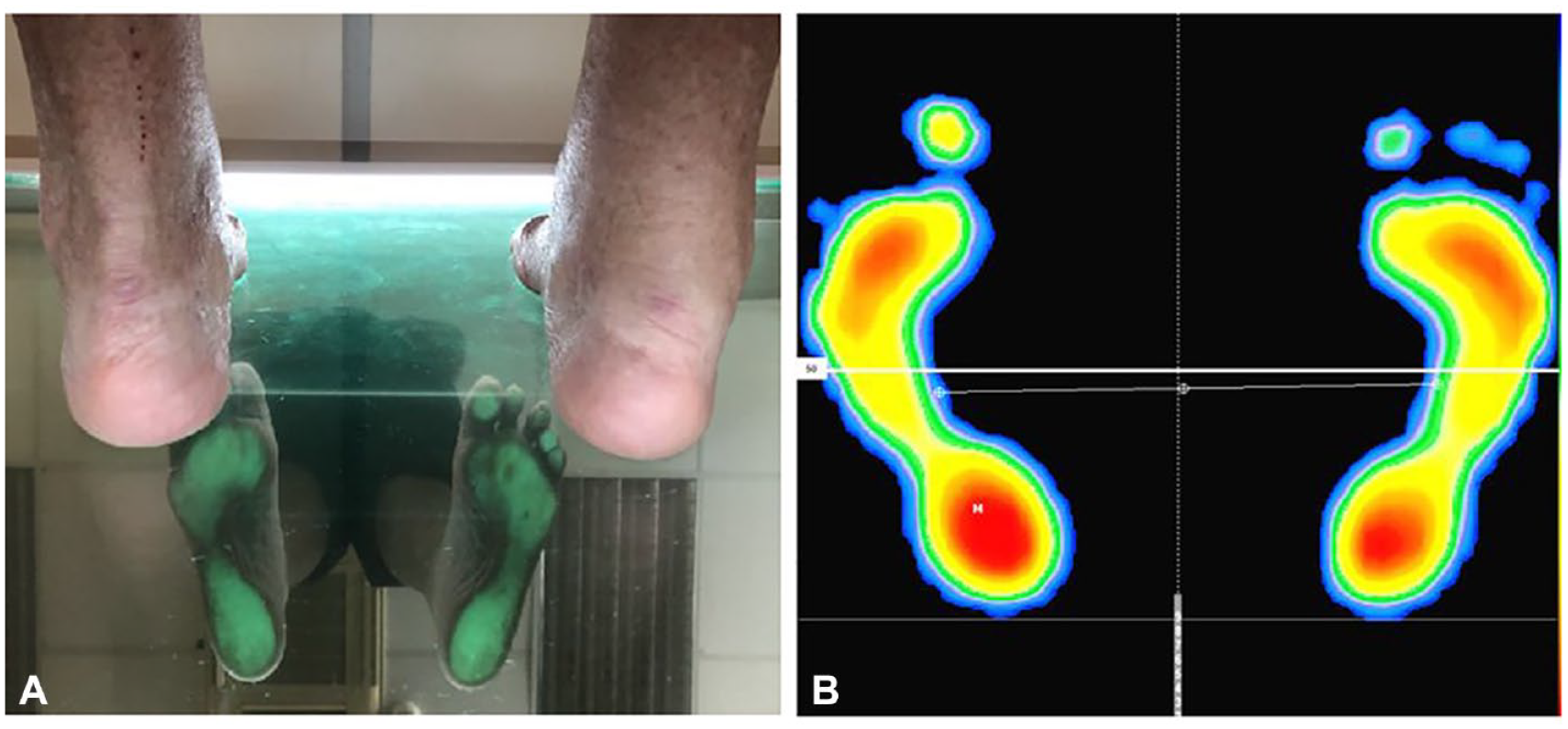
(A) Evaluation by the PodoScope with the patient in a static position, where the areas of maximum pressure are observed and hindfoot varus and (B) computed study: the areas of maximum pressure are observed in the patient’s static position.
The biomechanical study of the gait is carried out with the PodoPrint S4 platform. The following results were obtained:
Plantigrade gait with decreased Fick’s angle (<15°).
A shorter stride length.
During the full support phase, the subtalar joint presents an increase in joint pronation due to insufficiency of the first ray, causing a displacement of the plantar forces toward the bilateral smaller radius of foot, thus being able to initiate the take-off phase.
Preparation, puncture, and infiltration
Once the patient’s diagnosis was established, treatment with cross-linked HA 21 mg/mL with mannitol was proposed due to the absence of a beneficial effect of the personalized orthopedic insole. The patient signed the informed consent to perform the treatment. This study with human participants was conducted in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Bioethics Committee of the University of Barcelona (December 6, 2018).
To perform the procedure under rigorous aseptic conditions, surgical hand washing was performed with antiseptic liquid soap (4% Chlorhexidine Gluconate Solution) and sterile nitrile gloves were placed. The protocol requires that the procedure be performed in an operating room suitable for minor surgical procedures.
The patient is asked to lie on his back on a table with a sterile scrub under his feet. The material is prepared (2-mL pre-filled syringe of cross-linked HA 21 mg/mL with mannitol and a 27-G needle). The skin of the first MTF joint is disinfected with circular movements with 2% chlorhexidine in 70% alcohol gauze. To facilitate the location of the safe injection zone between 10 and 2 o’clock in both feet using the clock method described by Malagelada et al. 27
A movement of extension and plantar flexion of the hallux is performed to increase the safety of intra-articular puncture in the first MTP joint. Using the ultrasound-guided puncture, we administer the necessary volume of cross-linked HA (1 mL in this case), the needle is removed, massaged, and gently moved into the joint to ensure an even distribution of the HA. To minimize adverse effects, aspiration is recommended before, during, and after the injection, to avoid intravascular puncture 28 and to monitor the exact amount of infiltrated product. The infiltration area is covered with a sterile bandage.
Once the patient has recovered from the procedure, we proceed to recalculate the degrees of extension and plantar flexion of the first MTP joint both in unloading and then in load with a 2-branch goniometer.22,23
During the postoperative follow-up visits (14 days, 30 days, 60 days, and up to 400 days), the patient did not have any adverse effects of the procedure or the drug (no bleeding, no inflammation, no itching, no edema, no nodules, no pain, and no infection), which indicates the high safety of the procedure and the drug.
Outcome
Table 1 shows the pre- and post-infiltration results of the degrees of dorsiflexion, both in the loaded and unloaded position, as well as the degrees of flexion, measured in the unloaded position. The values obtained immediately after the intervention, during the operative procedure, constitute a 100% increase in all the initial values: both unloaded and loaded dorsiflexion and plantar flexion increase to twice the preoperative values. Measurements done during the first visit 2 weeks after the intervention showed a new increase of 100%. Thus, the values reached 14 days after the intervention tripled with respect to those obtained initially, both in dorsiflexion with load and in dorsiflexion without load and plantar flexion. These degrees of mobility have been maintained during successive control visits up to the time of this report, 400 postoperative days.
Degrees of dorsiflexion (in loaded and unloaded position) and plantar flexion (unloaded) of the first MTP joint.

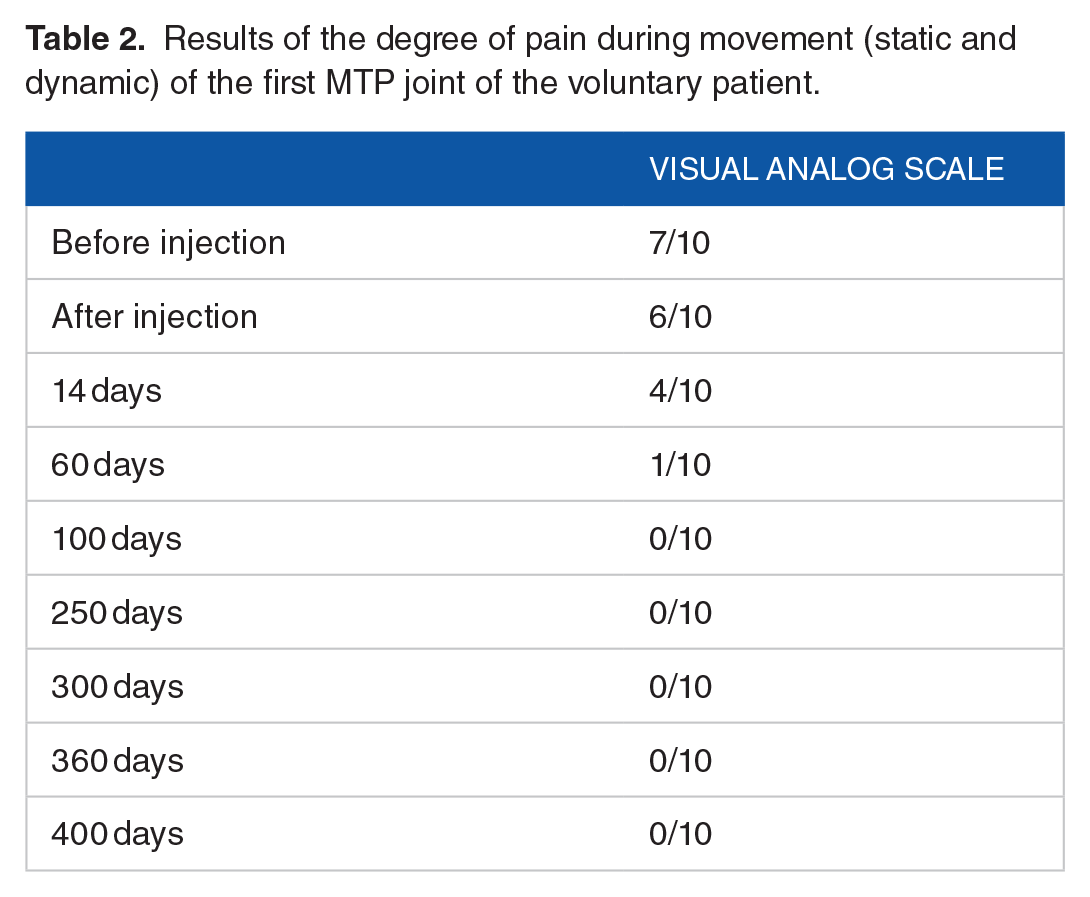
The evaluation of the patient’s symptoms over such a long period of time was performed using the VAS pain scale. Table 2 shows the results of the pain perceived by the patient. The difference in pain intensity before (7/10) and after injection (6/10) does not change at the same speed as movement. The substantial change in the patients’ perception of pain occurs between days 14 (4/10) and 60 (1/10). However, as occurs with movement, this improvement is maintained throughout the time evaluated. The patient reported an improvement in symptoms and a reduction in the fourth toe of the claw, which remains more than 14 months after infiltration.
Results of the degree of pain during movement (static and dynamic) of the first MTP joint of the voluntary patient.
Discussion
In this case, with a volunteer patient with painful HR, treated at the Virginia Novel Podiatry Hospital of the University of Barcelona, we analyzed different parameters: effective time of pain treatment and degrees of movement of the first MTP joint. The latter being the most important, as in the bibliography analyzed, none of the articles refers to the value in degrees of movement of plantar flexion and extension of the joint that increase or decrease with the treatments. In turn, the patient reported an improvement in the associated clinical symptoms of the minor radii (digital claw).
Immediate postoperative results show a doubling of the range of dorsiflexion in the loaded and unloaded positions. Surprisingly, these values triple after 14 days and maintain this range of motion value after 400 days. Plantar flexion range of motion also doubles in value at the immediate postoperative assessment, an improvement that remains stable after 400 days.
Patient results show that intra-articular infiltration of cross-linked HA 21 mg/mL with mannitol is a minimally invasive treatment that is effective in reducing pain and improving function of the first MTP joint. Consequently, by improving the joint mobility of the first MTP joint, a reduction in the clawed toe of the fourth toe is obtained, which remains more than 14 months after the infiltration.
The measurement instrument used to assess pain in the patient was the VAS. Our results show better values in the short and long term than the studies by Pons et al, 14 Petrella and Cogliano, 16 and Maher and Price 17 using the same pain assessment instrument.
To evaluate the functionality and joint range of motion of the first MTP joint of our patient, both in loading and unloading, the 2-branch goniometer was used, obtaining immediate results of increased and improvement in joint range of motion after intra-articular infiltration. These data cannot be compared with the studies by Pons et al, 14 Petrella and Cogliano, 16 Maher and Price, 17 Munteanu et al, 18 and Galois et al. 19
Regarding the amount administered in our study, it was 1 mL of HA, the same amount used in the studies by Pons et al, 14 Munteanu et al, 18 Maher and Price, 17 and Galois et al 19 in a single intervention. Instead, Petrella and Cogliano 16 administered 1 mL for 8 consecutive weeks, obtaining similar results to our study and other previous studies.
Regarding the molecular composition, we have used a 21 mg/mL cross-linked HA with mannitol. The molecule is more compact, providing volume and, therefore, increasing the intra-articular space and thus avoiding compression between the 2 joint facets and causing a decrease in symptoms in patients with HR. Galois et al 19 who used a crossover HA and obtained similar results to our study in symptoms.
The research follow-up time has exceeded 14 months, although the patient will continue to undergo monthly check-ups to analyze the degree of reversal of symptoms. The shortest follow-up time, 3 months, is that of the studies carried out by Galois et al 19 and Pons et al. 14 The study by Petrella and Cogliano 16 reports a 4-month follow-up, whereas the study by Munteanu et al 18 reports a 6-month follow-up. In addition, the longest follow-up study is the study by Maher and Price, 17 which is 18 months.
The treatment applied to the patient consists of a single intra-articular injection of 21 mg/mL cross-linked HA with mannitol that has been shown to be effective in relieving pain and improving the patient’s quality of life. As it is a pilot clinical trial, we have not been able to assess the general condition of the patient or her limitations in daily life, although we have verified that the treatment is effective in reversing her symptoms at 14 months. These conclusions agree with those advanced by Pons et al, 14 Maher and Price, 17 Munteanu et al, 18 and Galois et al. 19
The main limitation of this study is the very limited sample size (n = 1).
Conclusions
Cross-linked HA 21 mg/mL with mannitol improves symptomatology, joint mobility of the first MTP joint, and quality of life in the patient with stiff hallux submitted to the pilot test. These effects have been maintained for more than 14 months.
Footnotes
Acknowledgements
Not applicable.
Ethical approval and consent to participate
This study with human participants was conducted in accordance with the principles of the Declaration of Helsinki. The approval was granted by the Bioethics Committee of the University of Barcelona (December 6, 2018) with the name ID: IRB00003099. We also obtained informed consent from the voluntary patient, informed in writing and orally, to perform this study. We obtained written consent from the patient.
Consent for publication
The patient gave her consent, verbally, to publish her case in the journal.
Author contributions
Availability of data and materials
The data sets used and analyzed during this study are available from the corresponding author on reasonable request.
Competing interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.