
Abstract
Purpose:
The purpose of this study was to obtain information on safety and short-term efficiency of a single intra-articular injection of mannitol-modified cross-linked hyaluronic acid (HANOX-M-XL) in patients with painful first metatarsophalangeal joint osteoarthritis (1stMTPJ-OA).
Methods:
The study involved an observational, single-arm, prospective multicentre trial, with a 3-month follow-up. Inclusion criteria were patients with symptomatic 1st MTPJ-OA not relieved by analgesics and / or non-steroidal-anti-inflammatory drugs and / or foot orthotic. All patients received a single, imaging-guided intra-articular (IA) injection of 1 mL of HANOX-M-XL in the 1st MTPJ. The primary outcome was the change in pain between the date of injection and month 3. The secondary outcomes were the patient assessment of effectiveness, the decrease in painkiller use and the influence of the radiographic score on the clinical efficacy.
Results:
Sixty-five participants (72.3% women, mean age = 60) were included in the trial. Coughlin-Shurnas radiological grade was 1 in 28 patients, 2 in 29, and 3 in 6. At baseline and month 3, the average pain (0-10) was 6.5 ± 1.8 and 2.8 ± 2.3, respectively. The change in pain score was highly significant (−3.1 ± 2.9; P < .0001). At baseline there was no statistically difference in pain between the radiological stages (P = .69). At endpoint, the average pain score was 2.0 ± 1.9 in x-ray stage 1, 3.1 ± 2.3 in stage 2 and 3.3 ± 2.4 in stage 3 (P = .001). Mild to moderate adverse reactions were reported by 15 patients. All were a transient increase of the hallux pain that occurred immediately and up to 6 hours after injection and resolved in 1 to 7 days.
Conclusion:
This pilot study suggests that a single IA injection of HANOX-M-XL is safe and mainly benefits patients with mild moderate 1st MTPJ-OA. Further randomized controlled trials are necessary to confirm these preliminary encouraging results.
Keywords
Introduction
The term hallux rigidus refers to osteoarthritis (OA) of the metatarsophalangeal joint (MTPJ) of the first toe. This disease was first reported in 1887 by Davies-Colley. 1 Osteoarthritis of the 1st MTPJ is one of the most common disorders affecting the foot, after hallux valgus, 2 with a prevalence of about 7.8% in people aged over 50 years.
Hallux rigidus is characterized by joint pain and stiffness, progressive limitation in range of motion, and enlargement of the joint, mainly due to dorsal osteophytosis.
Treatment of the 1st MTPJ involves conservative measures 3 such as physical therapy, pharmacological treatment, foot orthoses, footwear modification or, at a late stage, surgical intervention, either conservative 4 or joint-destructive procedures. An alternative treatment termed ‘viscosupplementation’ – the intra-articular (IA) injection of high molecular weight hyaluronic acid (HA) into osteoarthritic joints with the aim of restoring the viscoelasticity of the synovial fluid – has been proposed and has attracted considerable attention in the medical literature as a treatment for OA. 5 The mechanisms of action of HA are complex and not yet fully understood. They include lubricant properties, anti-nociceptive and anti-inflammatory actions and disease-modifying effects, supporting that HA is not only just a simple device used for viscosupplementation but also a biologically active molecule that can affect the physiology of articular cartilage. 6
Very few studies have been designed to demonstrate the effectiveness of viscosupplementation in patients with 1st MTPJ OA. It is not possible to draw formal conclusions from these studies due to conflicting results and very different administration protocols.7 -9 HANOX-M-XL is a mannitol-modified HA cross-linked viscosupplement, developed for single-injection dose regimen. It has been shown to be effective and well tolerated in knee, 10 hip,11,12 ankle 13 and trapezio-metacarpal 14 OA.
The present pilot study was designed for collecting information on safety and efficacy of a single injection of HANOX-M-XL as a second-line adjunctive treatment in patients with symptomatic 1st MTPJ OA insufficiently relieved by standard care. Based on the observation that for most joints (knee, hip, etc) the effectiveness of HANOX-M-XL was better in the early radiological stages of OA,5,11,15 we hypothesized that this should be the same in the 1st MTPJ. Another objective of the research was therefore to investigate whether the radiological stage of 1st MTPJ OA may influence the effectiveness of viscosupplementation.
Patients and Methods
Regulatory
The study received the approval of the Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé (CCTIRS), and of the Commission Nationale de l’Informatique et des Libertés (CNIL). It has been registered by the French Agence Nationale de Sécurité du Médicament (ANSM) under the name REPAR trial (EudraCT N° 2015-AO1904-45). The study has been achieved in accordance with the Good Clinical Practice and the Declaration of Helsinki. Before enrolment, patients were required to give informed consent and were free to withdraw at any time for any reason. The patient informed consent form and the protocol, which complied with the requirements of the International Conference on Harmonisation (ICH), were reviewed and approved by the CCTIRS.
Study population
The present study was an observational, single-arm, prospective multicentre open-label clinical trial, with a 3-month follow-up. All the patients were recruited between September 2016 and September 2017 by experienced specialists in foot OA (rheumatologists or orthopaedic surgeons). Patients with symptomatic 1st TMJ OA, not sufficiently relieved by usual first line treatments, and who had undergone a radiography showing evidence of OA (joint space narrowing and/or osteophyte) were included in the study. Patients with other MTPJ involvement (ie, hallux valgus, microcrystalline or inflammatory arthritis of the 1st MTPJ), those who received viscosupplementation in the target joint within last 3 months, or corticosteroids during the last previous month, those having to undergo surgery during the 3 months of follow-up and the patients unable to give their informed consent themselves were not included in the trial.
Intervention
All patients received a single imaging-guided IA injection of 1 mL of HANOX-M-XL (Happymini, LABRHA Laboratory, Lyon, France) in the 1st MTPJ. The volume injected was in accordance with that of other studies.7 -9 HANOX-M-XL is a HA viscosupplement, specifically designed for small joints, constituted of a high HA concentration (16 mg/mL), a cross-linked structure and the addition of 35 mg/mL of mannitol, that delays the in situ degradation of HA. 16 These specificities allow HANOX-M-XL to be injected using a single-injection regimen. To ensure the accurate intra-articular administration of the device, all injections were performed under ultrasound or fluoroscopy guidance, 17 according to the investigator’s preference. Investigators were aware for not using local anaesthetic and for injecting a minimal amount of contrast product (<0.5 mL) since it has been demonstrated that both lidocain and iodine contrast products altered dramatically the HA rheological properties. 18
Evaluation
During the screening visit, the investigator handed a document providing key information about the study and obtained the patient’s informed consent for participating in the trial. Then they collected the demographic characteristics (age, sex, weight, height, body mass index) and disease features (symptoms duration, bilaterality, previous and current treatments for foot OA, concomitant therapies for co-morbidities). The patient self-assessment of pain on walking was obtained using a 11-point numerical rating scale (0-10 NRS). The investigator also had to assess the radiological stage (stage 0-3) according to the Coughlin-Shurnas radiological classification, 19 grade 1 meaning mild dorsal osteophyte with minimal joint space narrowing, grade 2 meaning periarticular osteophyte with flattened appearance to metatarsal head, mild-to-moderate joint space narrowing and sclerosis, and grade 3 meaning same as grade 2 with substantial narrowing and possibly periarticular cystic and sesamoid changes. At the end of the screening visit, the investigator had to plan the HANOX-M-XL injection within 15 days and to choose the imaging guidance technique.
At the last study visit, 3 months after injection, the investigator reported on the clinical report form (CRF) the patient self-assessment of walking pain on a 0-10 NRS (0 = no pain to 10 = extreme pain), the patient perception of treatment efficacy (0 = not effective to 3 = very effective), the change in analgesic intake (<25%, 26%-50%, 51%-75%, >75%) and the occurrence of any adverse event (AE).
The primary outcome for assessing the treatment efficacy was the change in pain between the injection date (D0) and month 3 (D90). The secondary outcome measures were the patient perception of treatment efficacy and the variation in analgesic/nonsteroidal anti-inflammatory drug (NSAID) use. The number and percentage of patients fulfilling the Patient Acceptable Symptom State 20 (PASS) at baseline and endpoint was also calculated. The PASS score, which is the threshold that defines the concept of symptomatic remission, is 4 on a 10-point NRS. 21 Differences in pain between radiographic grades were studied.
Safety was evaluated by recording all the adverse events occurring between injection and month 3 using the European Medicines Agency recommendations. Investigators had the responsibility to grade any adverse event as severe or not and as related to the viscosupplement/procedure or not.
Statistics
In this exploratory study, the number of participants could not be determined a priori. Taking into account the multiple factors to be analysed, the minimum number of patients to be included was set at 60 by a committee of experts specialized in the field, with an expected percentage of dropouts of 15%. Baseline and 6-month follow-up data are given as number, percentage, median and range or mean and standard deviation (SD). The statistical significance of the change in pain over time was studied with the paired Student t test. The relationship between pain (score and changes over time) and radiological score was studied from the intent-to-treat (ITT) population by processing missing data with the Last Observation Carried Forward (LOCF) method. A second similar analysis was achieved on the per protocol (PP) population. A multivariate analysis including sex, age, pain at baseline and body mass index (BMI) was also performed to overcome confounding factors. The regression coefficients of the multivariate models (analysis of covariance [ANCOVA] and mixed model) were considered significant if they were less than 5%. Data were analysed using Xlstats software 2017 (Addinsoft, Paris, France).
Results
Sixty-five participants were included. About 72.3% were women, mean age 60 (range = 28-85), with mean symptom duration of 34.2 ± 35.4 months and a mean BMI of 24.9 ± 3.1 kg/m2. Intra-articular injections were performed using fluoroscopy in 59% and ultrasound in 41% of the cases. Patients’ characteristics at baseline are summarized in Table 1. The Coughlin-Shurnas radiological grade was 1 in 32 patients, 2 in 29, and 3 in 6. At baseline, the average pain on walking (± SD) was 6.5 ± 1.8 (median = 7, range = 3-10). Only 9 patients (13.8%) met the PASS criteria.
Characteristics of patients at baseline.
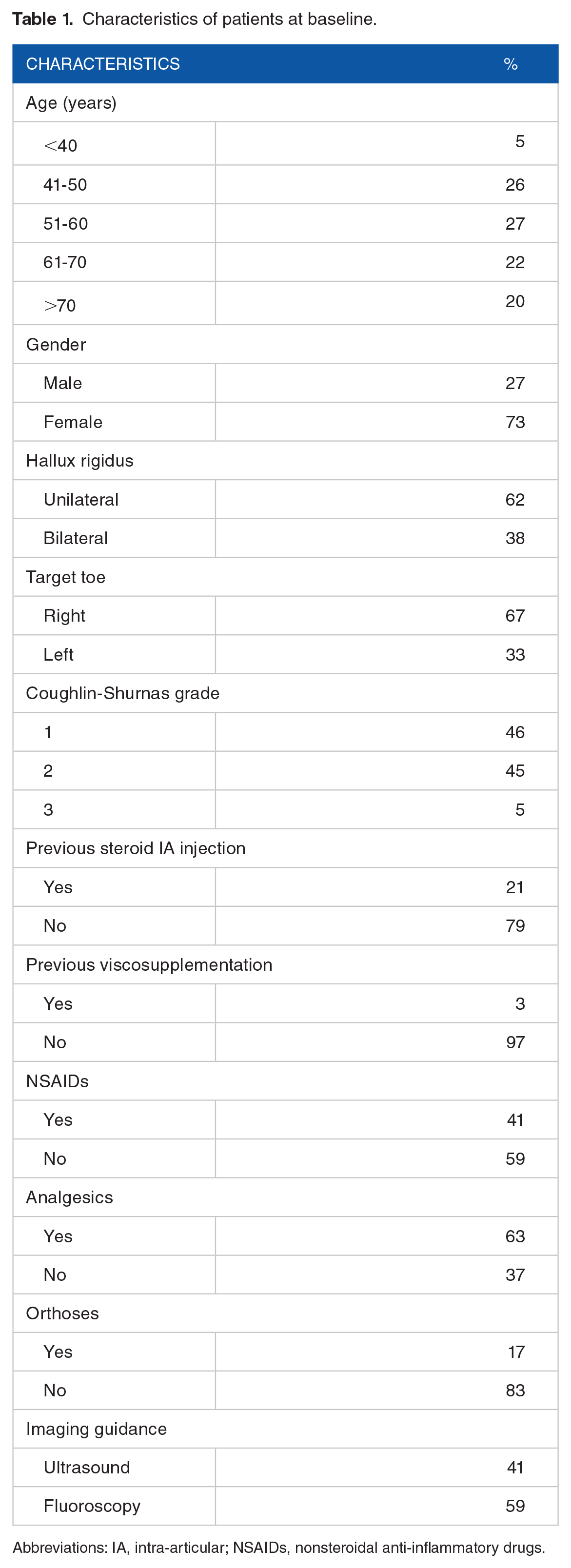
Abbreviations: IA, intra-articular; NSAIDs, nonsteroidal anti-inflammatory drugs.
Nine patients (13.5%) were lost to follow-up. At endpoint, the mean walking pain was 2.65 ± 2.2 (median = 2, range = 0-8). The pain score difference between baseline and month 3 was highly statistically significant (−4.2 ± 2.5 and −64.6%; P < .0001) (Figure 1). At the end of follow-up, 43 patients (76.8% of the completers, 66.1% of the ITT population) met the PASS criteria (Figure 2). Forty-five patients (80.3% of the completers, 69.2% of the ITT population) rated the treatment as very effective or effective. Seventy-two percent of patients, who were taking analgesics and/or NSAIDS, significantly decreased painkiller use, throughout the follow-up period. The average decrease in analgesics/NSAIDS exceeded 50% in 1 patient out of 2.
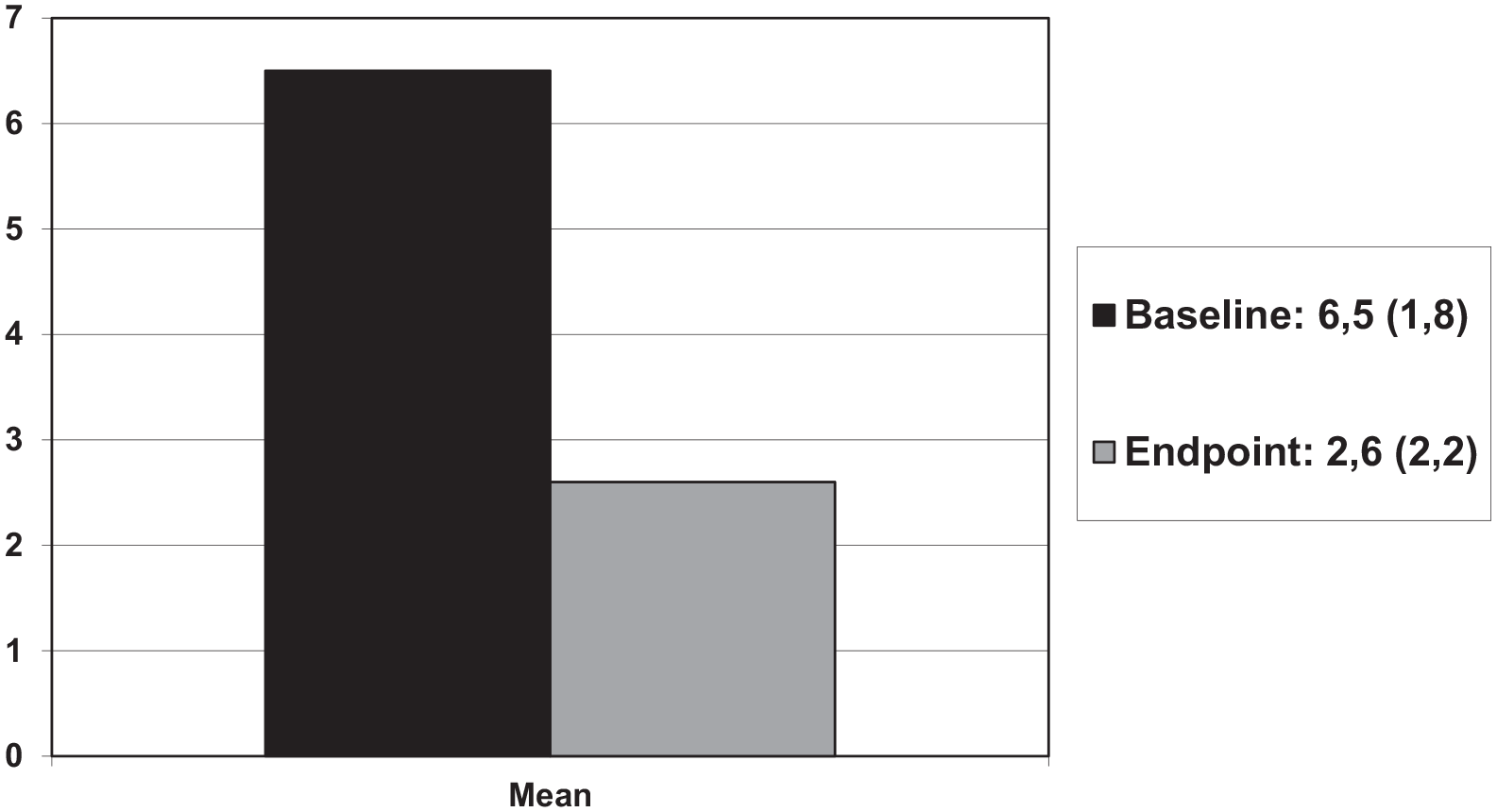
Mean walking pain score (0-10) (SD) variation between time of injection and month 3, in 65 patients with 1st metatarsophalangeal osteoarthritis (hallux rigidus) treated with a single intra-articular injection of HANOX-M-XL (P < .0001).

Number of patients according to pain score categories (numerical rating scale 0-10) at baseline (N = 65) and 3 months after viscosupplementation (N = 59). Patients with a pain score ⩽ 4 fulfilled the Patient Acceptable Symptom State (PASS) criterion.
Device and/or procedure-related adverse events (AEs) were reported by 15 patients (22.7%). All were described by patients as a transient increase of the big toe pain, which occurred the very next hours after injection (mean = 2 hours, range = 0.5-6 hours). All but 2 were rated as mild to moderate. Two patients reported severe pain during the 6 hours following injection. All AEs have been resolved in 3 to 7 days (mean = 4.4 days), spontaneously (9 cases) or with the help of analgesics (4 cases) or NSAIDs (1 case). The imaging guidance method was unrelated with the occurrence of side effects (P = .81). No severe or systemic AE was reported.
There was no statistically significant difference in pain between radiological stages at baseline (r = 0.25; P = .69). On the contrary, the average pain score at endpoint was significantly lower in patients with the Coughlin-Shurnas grade 1 (2.0 ± 1.9) than in those with grades 2 (3.1 ± 2.3) and 3 (3.3 ± 2.4) (P = 0.001) (Figure 3) despite a very significant decrease of pain versus baseline in both grades 2 and 3 patients. There was no difference between grades 2 and 3 (Figure 4). In multivariate analysis, the Coughlin-Shurnas grade was the only factor significantly related to the level of pain at month 3.

Percentage of patients with hallux rigidus, treated with 1 intra-articular injection of HANOX-M-XL (N = 59), rating the treatment as very effective/effective or slightly effective/uneffective.

Walking pain score (0-10) variation between time of injection and month 3 in 65 patients with hallux rigidus treated with 1 intra-articular injection of HANOX-M-XL (N = 65), according to the Coughlin-Shurnas radiological grade (all P < .0001).
Discussion
This prospective exploratory open-label pilot study is the second largest cohort ever published on viscosupplementation for hallux rigidus.7 -9 It suggests that a single IA injection of HANOX-M-XL is an effective and well-tolerated adjunctive treatment for patients with painful 1stMTPJ OA, not adequately relieved by standard care. Our results showed a very significant reduction in pain at day 90 compared with that reported at Day 0, a very positive patients’ perception of the efficacy and a relevant decrease in painkiller consumption. However, in the absence of a control group, the present pilot study does not allow to formally assert that HANOX-M-XL acts better than a placebo. Nevertheless, the magnitude of pain decrease, in both absolute value and percentage, greatly exceeded the threshold that defines the Minimal Clinically Important Improvement 21 (ie, −2 points and −20%), suggesting the clinical relevance of this improvement.
Two previously published open-label studies also suggested the effectiveness of HA injection(s) for relieving pain and improving function in patients with 1stMTP OA. Pons et al 8 evaluated, by repeat examinations up to 84 days, the effectiveness and safety of a single 1 mL IA injection of a linear sodium hyaluronate compared with 1 mL of triamcinolone acetonide in 37 patients with painful hallux rigidus. Pain at rest or with palpation and pain on passive mobilization decreased significantly in both treatment groups in comparison to baseline but not significantly in the between-group analysis. Petrella and Cogliano 9 studied the efficacy, safety, and patient satisfaction of repeat IA injections of a linear HA, in 47 patients suffering from golfer’s toe. All patients received 1 mL of HA in the 1st MTPJ, once a week, 8 consecutive weeks. At weeks 9 and 16, a significant improvement in pain at rest and after tiptoe walking and range of motion was observed. On the contrary, the only randomized double-blind, controlled trial, published by Munteanu et al 7 failed to demonstrate the superiority of viscosupplementation versus placebo. One-hundred fifty-one patients with symptomatic 1st MTPJ OA were randomly allocated to receive 1 mL IA injection of either Hylan G-F 20 or saline. The primary outcome measurement was the foot pain domain of the Foot Health Status Questionnaire (FHSQ) at 3 months. Secondary outcome measurements were foot function, 1st MTPJ pain, stiffness and range of motion, magnitude of pain and function changes, patient satisfaction and quality of life. The authors did not identify any statistically significant between-group difference in foot pain at 3 months, whereas they found few significant differences in the secondary outcome measures. They concluded that Hylan GF-20 injection was not superior to placebo in the treatment of hallux rigidus. The fact that HANOX-M-XL is 2 times more concentrated in HA than Hylan GF-20 (16 mg/mL versus 8 mg/mL), and that, thanks to the presence of mannitol, HA degradation is 3 times slower 22 might explain the differences in efficiency reported in our study and that of Munteanu.
Our study suffers from other limitation than the non-controlled design. The main weaknesses or the study is the duration of follow-up. A 3-month follow-up is appropriate to evaluate short-term clinical results but is probably short to extrapolate to long-term efficacy. However, in view of the strong improvement at month 3, the duration of pain relief is likely to last much beyond month 3. Another point to emphasize is we investigated only the pain dimensions (pain score, efficacy, satisfaction and painkiller use) but neither the function, nor composite scores such as FHSQ.
Unsurprisingly, our results showed that a greater improvement was observed in patients with early stage of 1st TMJ OA. However, contrary to what is found in knee and hip OA,11,23 the magnitude of pain decrease remained relevant even in the most advanced stages. Indeed, two third of the patients with radiological scores 2 and 3 rated the treatment as effective or very effective (versus 3 out of 4 of those with stage 1).
The main strength of this study is that it was conducted on the second largest cohort ever published in 1st MTPJ OA viscosupplementation. Furthermore, the study protocol required mandatory use of imaging guidance to ensure HA to be strictly administered intra-articularly. 17 Moreover, the recruitment of patients, that was made by both rheumatologists and foot specialist orthopaedic surgeons, as well as the absence of inclusion/exclusion criteria related to clinical or anatomical severity of the disease, allowed to have a study population as close as possible to that met in daily clinical practice.
Finally, this study provided interesting supplementary data concerning the tolerability of HANOX-M-XL. No patient experienced any serious, unexpected or systemic adverse event. Transient injected joint discomfort was observed in 22% of patients. Increasing 1st MTPJ pain occurred the very next hours after injection and lasted 3 to 7 days. None was considered as severe and all resolved spontaneously within less than a week. In patients with trapezometacarpial OA treated with a single injection of HANOX-M-XL, Dauvissat et al 14 reported a good tolerability of the device, similar to that reported in the literature with non-cross-linked and non-mannitol-modified HAs. Nevertheless, it seems important to carefully inform the patients on the possible increase of pain, and to prescribe a painkiller for the very next days following the injection.
In conclusion, this pilot study suggests that a single injection of 1 mL of HANOX-M-XL, performed under imaging guidance in 1st MTPJ, reduces significantly pain on walking, for at least 3 months, especially in patients with mild joint space narrowing. However, most patients with moderate OA were also significantly improved. Although the overall tolerability was good, it seems to us that providing careful information to the patient is necessary, regarding the risk of pain increase the few days following injection. Further controlled studies, with longer follow-ups, are needed to confirm these promising results.
Footnotes
Acknowledgements
We thank Dr Benoit Loze, Dr Jean Fulpin, Dr Jacques Despaux, Dr Karim Sebaa and Dr Henri Lellouche for their clinical contributions as investigators of the trial.
Author Contributions
All authors contibuted to patients selection and evaluation. Thierry Conrozier performed the statistcal analysis. Laurent Galois and Thierry Conrozier wrote the manuscript. All authors reviewed, commented and accepted the manuscript.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Laurent Galois did not receive remuneration for his contribution to the article. Jean-Yves Coillard did not receive remuneration for his contribution to the article. Jérôme Porterie did not receive remuneration for his contribution to the article. Sylvie Melac-Ducamp did not receive remuneration for her contribution to the article. Thierry Conrozier received fees from LABRHA for scientific, speaker and board member services.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research project was provided by LABRHA SAS.