
Abstract
Background:
Adult-onset Still’s disease (AOSD) is a rare auto-inflammatory disorder with unknown etiology by which an infectious trigger is usually responsible for the onset of the disease. It is diagnosed by exclusion when certain clinical, biochemical, and radiological criteria are met after excluding all other potential causes. Besides, SARS‑CoV‑2 infection is increasingly being reported to have autoimmune complications. In the literature, 3 AOSD cases have been reported to be triggered by SARS‑CoV‑2 infection and here we report the fourth.
Case presentation:
A 24-year-old female doctor suffered from fever, sore throat, and mild cough a few days after a shift in the COVID-19 ward. A week later, she developed polyarthritis, salmon-colored rash, and high-grade fever, and the laboratory findings were indicating an inflammatory syndrome. COVID-19 IgM antibodies were positive indicating recent infection. After running a battery of tests, infectious, neoplastic, and rheumatic causes of these symptoms that persisted for about 50 days were excluded which led to a diagnosis of AOSD after fulfilling its criteria with subsequent treatment with methylprednisolone. Drastic improvement was achieved with no recurrence until the date of reporting.
Conclusion:
This case presents a new consequence of COVID-19 and adds to the emerging cumulative experiences with this disease. We encourage health care professionals to report such cases to further understand the nature of this infection and its possible outcomes.
Background
Adult-onset Still’s disease (AOSD) is an auto-inflammatory disorder characterized by a set of clinical and laboratory findings for which there are various groups of diagnostic criteria such as Yamaguchi, Cush, and Fautrel criteria, and it is diagnosed by exclusion. It is believed that this disease could result from a trigger event/agent that leads to pathological inflammation in a genetically predisposed individual. Potential triggers of this disease include viral or bacterial infections and malignancies. 1
SARS-CoV-2 virus, on the other hand, is a relatively novel virus that is still not fully understood, and a lot of its consequences remain of unknown mechanism. It may trigger a variety of clinical syndromes related to various organ systems. As such, COVID-19 is reported as a trigger for multiple autoimmune diseases such as vasculitis and arthritis. 2 In the medical literature, there are only 3 published cases of COVID-19 as a trigger for the first episode of Still’s disease, with this report presenting the fourth.
Case Presentation
A 24-year-old female doctor with no medical history complained of a sore throat, nasal congestion, fever ranging between 38°C and 38.5°C, chills, non-producing cough, and headache. She reported having a 1-night shift in the COVID-19 ward 5 days earlier with direct prolonged contact with a COVID-19-positive patient without wearing proper personal protective equipment. These symptoms persisted for about a week, after which she suffered from episodes of arthralgia, redness, pain, and swelling of phalangeal joints with pain in both knees, wrists, and shoulders. These were accompanied by an erythematous nonpruritic rash on the abdomen, hands, forearms, and thighs. She also suffered from a daily persistent fever that spiked up to 41°C at midday and had a good response to acetaminophen for a while only to peak up again to 40°C at night (Figure 1).

Oral temperature measurements for the patient. This occurred daily for almost the whole course of the disease.
A measured high-grade fever (41°C), tachycardia (110 beats per minute), normal blood pressure, and a high respiratory rate were revealed on physical examination. In addition, the proximal interphalangeal joints (PIP) of the first and third fingers of the right hand, all metacarpophalangeal joints, the first and fifth PIPs in the left hand, and both wrists were swollen and tender (Figure 2). Tenderness in both knees and shoulders was also noticed. No other important findings in other organ systems were found.

A photographic image showing the rash (black arrows) and joints swelling (red arrows): (A) on presentation; (B) later in the course of the disease.
Laboratory tests done to the patient throughout the course of the disease are presented in Table 1.
Laboratory findings of the patient (normal values are within parenthesis).
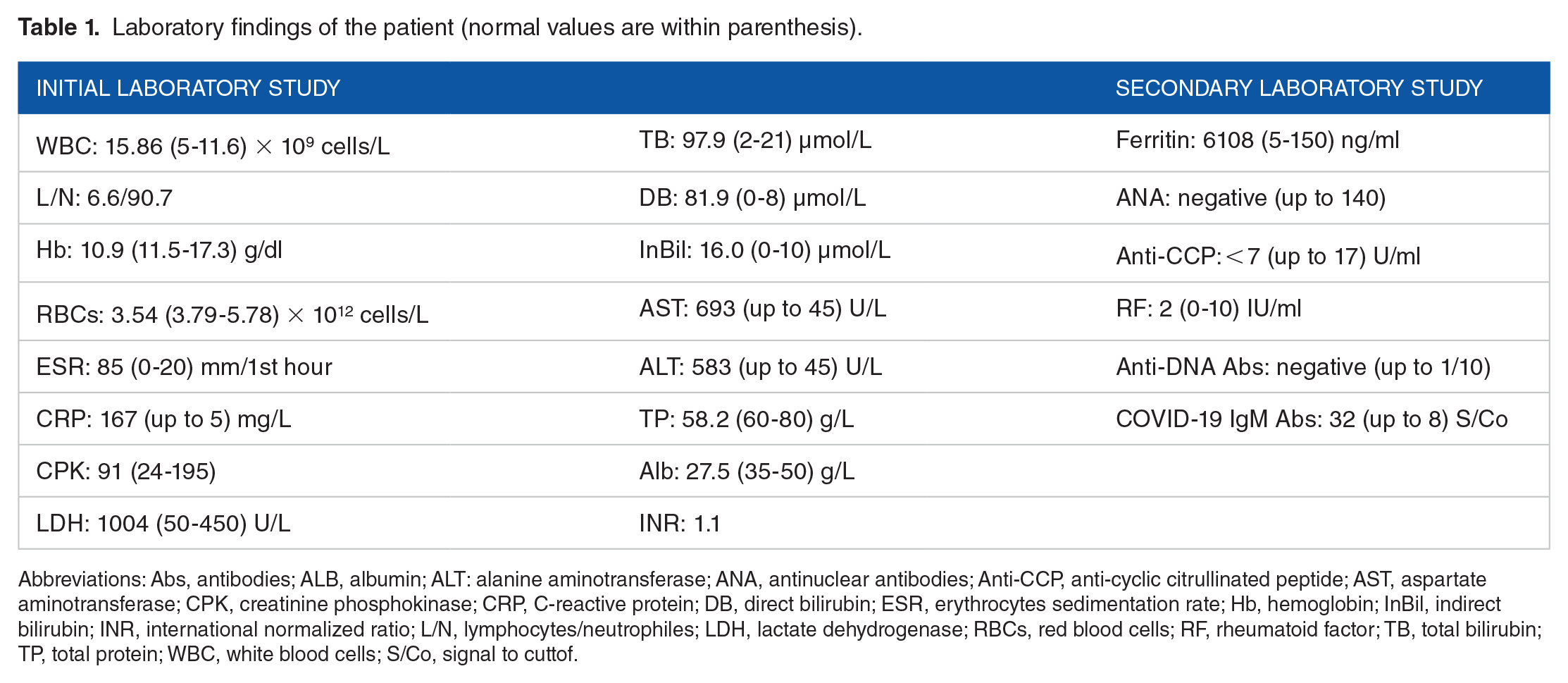
Abbreviations: Abs, antibodies; ALB, albumin; ALT: alanine aminotransferase; ANA, antinuclear antibodies; Anti-CCP, anti-cyclic citrullinated peptide; AST, aspartate aminotransferase; CPK, creatinine phosphokinase; CRP, C-reactive protein; DB, direct bilirubin; ESR, erythrocytes sedimentation rate; Hb, hemoglobin; InBil, indirect bilirubin; INR, international normalized ratio; L/N, lymphocytes/neutrophiles; LDH, lactate dehydrogenase; RBCs, red blood cells; RF, rheumatoid factor; TB, total bilirubin; TP, total protein; WBC, white blood cells; S/Co, signal to cuttof.
The symptoms were managed so far with acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs); Naproxine 500 mg b.i.d, and indomethacin 25 mg t.i.d daily for about a month with unsatisfactory results. As such, it was considered an inflammatory state with joints involvement induced by a prior respiratory infection justifying an opinion to start empirical treatment with steroids. Parenteral dexamethasone 8 mg per day was administered for 10 days with a drastic improvement of all of the symptoms, but pausing the treatment resulted in the recurrence of the symptoms within 2 days, and resuming it produced re-improvement.
To reach a conclusive diagnosis and to exclude other infectious, neoplastic and autoimmune etiologies, she was admitted to the hospital and a battery of tests was performed. These included urine analysis, echocardiography, blood cultures, Widal and Wright tests, and scanning computed tomography (CT) imaging, which came out all negative. Abdominal echography revealed mild splenomegaly (the spleen measurement was 15.5 cm on its largest diameter), which was confirmed with the CT imaging. Lupus erythematosus and rheumatoid arthritis were excluded because of the negative antinuclear antibodies (ANA), the normal anti-cyclic citrullinated peptide IgG antibodies (Anti-CCP) level, the normal rheumatoid factor (RF) level, and the negative anti-DNA antibodies (Table 1). A high ferritin level > 3000 ng/ml brought to the mind AOSD. At this point, a month and a half after the first symptoms occurred, COVID-19 IgM antibodies were measured with positive results (32 S/Co index, normal range up to 8 S/Co), which retrospectively confirmed a recent infection with the virus.
With the aforementioned symptoms that persisted for about 60 days (Figure 3) and after excluding all other potential causes, a diagnosis of AOSD was achieved according to Yamaguchi criteria, and subsequent treatment with prednisolone 50 mg daily was started. Two days later, a significant improvement in all the symptoms was observed. This dose was administered for 2 weeks and then tapered gradually over 3 months with no recurrence of symptoms. Following the patient up to 1 year of that incidence, no recurrent symptoms were observed.

Timeframe of the events in the case.
Discussion
Adult-onset Still’s disease is an auto-inflammatory systemic disorder with a prevalence ranging between 1 and 34 cases/1 million people. 1 Multiple sets of criteria are proposed to diagnose AOSD, including Yamaguchi criteria which have a sensitivity of 96.2% and specificity of 92.1%. 3 It includes major criteria (intermittent fever greater than 39 lasting for a week or more, arthralgia for more than 2 weeks, a nonpruritic salmon-colored rash appearing on the trunk or limbs accompanying fever, and a white blood cells count of greater than 10000/microliter with 80% or more neutrophils), and minor criteria (sore throat, splenomegaly and/or lymphadenopathy, abnormal liver enzymes titers, and a negative ANA/RF). To be diagnosed with AOSD, the patient should have 5 criteria with at least 2 major ones and all other causes must also be excluded, such as infectious, malignant, or rheumatic disease. 3
It is believed that genetic predisposition combined with a triggering factor results in a pathological inflammatory process that leads to the disease manifestations. A wide variety of possible triggers are suggested including viral or bacterial infections and malignancies. 1
SARS-CoV-2 is a novel pathogen that has caused a global pandemic of respiratory infections with multiple inflammation-mediated consequences, and its pathogenesis is still not completely understood. 4 A major innate immune system pathway involved in the immune response to SARS-CoV-2 infection is the endosomal Toll-Like Receptor 7 pathway expressed in the dendritic cells. 5 Excitingly, this receptor pathway is reported to be overexpressed in AOSD patients which could explain how SARS-CoV-2 infection could act as a trigger for AOSD. 6 In addition, AOSD and COVID-19 share high levels of IL-6 as a part of their pathophysiology, especially in the cytokine storm syndrome of COVID-19. This leads to similar clinical inflammatory symptoms and delays even thinking of the disease as a differential.7,8
In our patient, the respiratory symptoms disappeared, after which the inflammatory syndrome, high-grade fever, sore throat, arthritis, rash, and arthralgia persisted for a long period indicating another cause of that syndrome rather than the infection itself. At first, reactive arthritis was considered and treated with NSAIDs without significant improvement. Then, Clinical and laboratory assessments were compatible with a possible cytokine storm caused by the viral infection. Therefore, the treatment with dexamethasone was started, however, when it is discontinued, the constitutional symptoms, spiking excessive fever, and arthritis resurfaced. As a differential diagnosis, AOSD was proposed since our patient had 4 major and 4 minor criteria of Yamaguchi’s criteria, but all different diagnoses needed to be excluded to confirm AOSD.
Hence, a computed tomography scan, a blood culture, echocardiography, and Widal and Right tests were done to exclude malignancies, endocarditis, brucellosis, and typhoid respectively. In addition, RF, anti-CCP, and ANA were analyzed to exclude rheumatoid arthritis and systemic lupus respectively. After excluding all the other causes, AOSD was diagnosed. Subsequently, Prednisolone therapy was started and a significant clinical improvement was observed.
In the medical literature, there are only 3 published cases of COVID-19 as a trigger for the first episode of Still’s disease with our case being the fourth. The cases are summarized in (Table 2).
A summary and comparison between this case and other published cases.
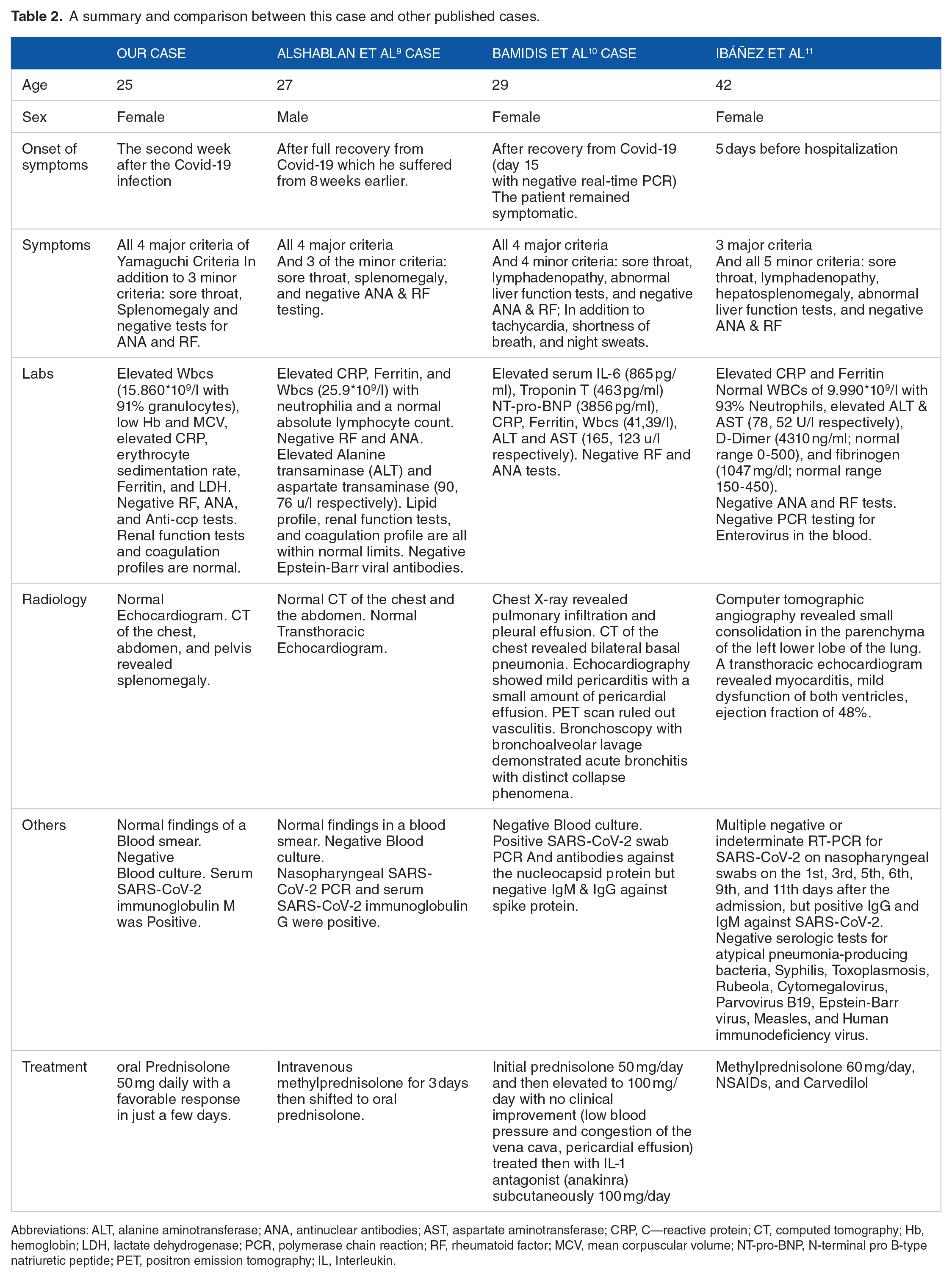
Abbreviations: ALT, alanine aminotransferase; ANA, antinuclear antibodies; AST, aspartate aminotransferase; CRP, C—reactive protein; CT, computed tomography; Hb, hemoglobin; LDH, lactate dehydrogenase; PCR, polymerase chain reaction; RF, rheumatoid factor; MCV, mean corpuscular volume; NT-pro-BNP, N-terminal pro B-type natriuretic peptide; PET, positron emission tomography; IL, Interleukin.
Finally, we have to mention that the definite diagnosis of a SARS-CoV-2 infection is usually achieved by doing a PCR on a nasal swab which was not done in our case, however, a very likely diagnosis could also be achieved considering the contact history and the symptoms of low-grade fever, runny nose, and cough combined with a positive SARS-CoV-2IgM antibodies testing which indicates a recent infection.
Conclusion
In this article, we shed the light on a new unforeseen consequence of SARS-CoV-2 infection as it was a trigger for AOSD. Also, it is worth mentioning that during the COVID-19 era, other medical conditions are having less attention and clinical suspicion when thinking about patient’s symptoms, which may delay a proper diagnosis. We encourage health care professionals to report such cases to further understand the nature of this infection and its possible outcomes, and to increase our understanding of AOSD.
Footnotes
Acknowledgements
We would like to thank the sworn translator Mr. Saleh Alali for his great efforts in proofreading our manuscript.