
Abstract
Introduction:
Adult-Onset Still’s Disease (AOSD) is a rare inflammatory disease. It usually causes high fevers, joint pain, a fleeting rash, and very high ferritin levels. The symptoms can mimic infections, autoimmune disorders, or cancers, so it can be hard to diagnose. Liver involvement is common but usually mild. Severe hepatitis is rare.
Case Presentation:
We report a 24-year-old woman who had 3 weeks of daily high fevers, a temporary salmon-pink rash, sore throat, muscle pain, and joint pain. Her blood tests showed high white blood cells with mostly neutrophils, persistent monocytosis, severely elevated liver enzymes, and very high ferritin. Tests ruled out infections, autoimmune diseases, and cancers. She met criteria for AOSD, and her glycosylated ferritin was low. The patient responded rapidly to intravenous methylprednisolone, but relapsed with polyarthritis upon tapering, which resolved completely within 48 hours of initiating anakinra.
Discussion:
This case highlights the diagnostic challenges of AOSD presenting predominantly with hepatic involvement and atypical laboratory features such as persistent monocytosis. Recognition of extreme hyperferritinemia as a diagnostic clue can prevent delays in diagnosis. The dramatic response to IL-1 blockade underscores cytokine dysregulation as a central pathogenic mechanism.
Conclusion:
Clinicians should consider AOSD in patients with febrile hepatitis and extreme hyperferritinemia. Early initiation of biologic therapy targeting IL-1 can achieve rapid remission, improve quality of life, and prevent complication.
Introduction
Still disease is the term used to describe systemic juvenile idiopathic arthritis, and was first identified in children by Still. 1 While Adult-onset Still’s disease (AOSD) designates the condition that manifests after age 16 and was only described in the early 1970s. 2
AOSD is a rare disorder with a variable spectrum of signs and symptoms at onset that can mimic other inflammatory or infectious conditions. Its annual incidence is estimated to be between .16 and .62 per 100 000 individuals worldwide, regardless of ethnicity. There’s a slight inclination for females over males and a bimodal pattern to the age distribution, with the first peak taking place between the ages of 15 and 25 and the second peak between the ages of 36 and 46. The origin of AOSD has been attributed to a number of causes, including infections (from bacterial and viral pathogens), a dysregulated immune system, and genetics (association with human leukocyte antigen [HLA] DRB1 * 1201 and 1501, B35, DR2, and DR5). It has also been proposed that stressful life events including family, career, and health might be a trigger for AOSD.3 -5
Herein, we report a rare case of AOSD presenting with atypical hepatitis and persistent monocytosis, an uncommon laboratory feature not typically emphasized in classic descriptions of the disease.
Case Presentation
A 24-year-old previously healthy female presented with a 3-week history of daily, spiking fevers up to 40°C, typically occurring in the late afternoon or evening and resolving by morning. She reported a transient, non-pruritic salmon-pink rash on her trunk and proximal extremities that coincided with the fevers, along with severe sore throat, myalgia, and arthralgia involving her wrists and knees.
Her medical history was unremarkable, with no prior arthralgia, arthritis, Raynaud’s phenomenon, chronic illnesses, or hospitalizations. She took no regular medications and had no known drug allergies. Family history was notable for a maternal grandmother with rheumatoid arthritis. She denied recent travel, sick contacts, high-risk behaviors, and was a non-smoker.
On examination during a febrile episode, she appeared ill. Vital signs showed a temperature of 39.8°C, heart rate of 110 bpm, and normal blood pressure. Physical findings included a blanching, macular salmon-pink rash on the chest and back, bilateral conjunctival injection, and mild pharyngeal erythema without exudates. There was no lymphadenopathy or hepatosplenomegaly. Joints were tender but without synovitis initially.
Laboratory investigations revealed marked leukocytosis with predominant neutrophilia, persistent absolute monocytosis, and markedly elevated inflammatory markers (CRP, ESR). She had severe transaminitis, with ALT and AST over 15 times the upper limit of normal, and an extremely elevated ferritin of 18 500 ng/mL (Table 1).
Serial Laboratory Parameters from Presentation to Remission.
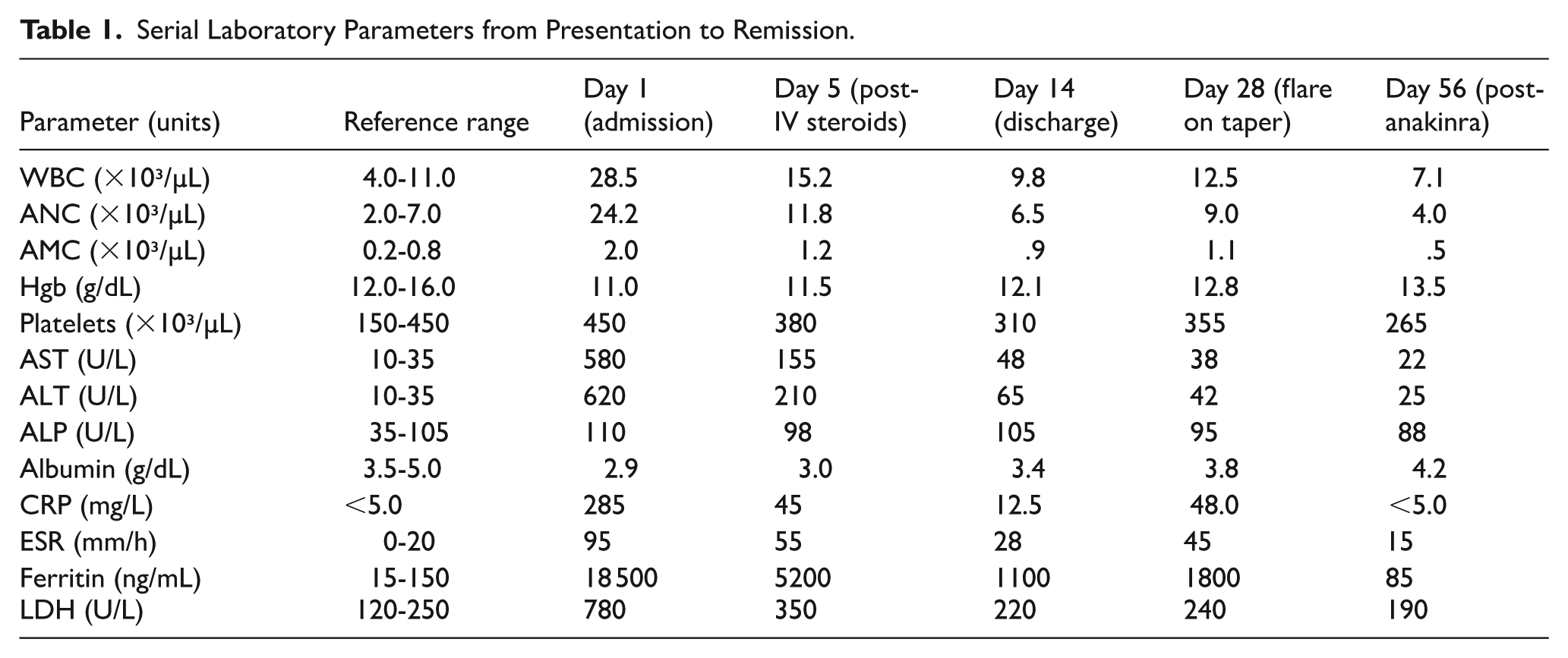
A comprehensive fever-of-unknown-origin workup was negative: viral serologies (Hepatitis A, B, C, EBV, CMV, HIV), multiple blood cultures, and autoimmune panels (ANA, RF, ANCA) were all unremarkable (Table 2). Abdominal ultrasound showed normal liver echotexture without biliary obstruction.
Key Investigations in the Diagnostic Workup for Fever of Unknown Origin.

After exclusion of infection, malignancy, and other autoimmune disorders, AOSD was diagnosed using the Yamaguchi criteria (Major: fever >39°C, arthralgia, typical rash, leukocytosis; Minor: sore throat, lymphadenopathy, hepatic dysfunction, negative ANA/RF). A serum glycosylated ferritin level <15% further supported the diagnosis.
The patient was started on intravenous methylprednisolone 1 mg/kg/day, resulting in resolution of fever within 24 hours and significant improvement of rash and sore throat. Transaminitis and inflammatory markers began to decline, and she was discharged on a tapering dose of oral prednisone.
During tapering to 20 mg/day, she developed new-onset polyarthritis in the wrists, knees, and MCP joints, accompanied by rising inflammatory markers. Given this steroid-dependent course, she was started on subcutaneous anakinra 100 mg daily. The response was dramatic, with complete resolution of arthritis within 48 hours. Laboratory parameters normalized over the next month, prednisone was discontinued, and at 6-month follow-up, she remained in clinical and biochemical remission on anakinra monotherapy.
A timeline summarizing the patient’s symptoms, laboratory findings, and treatment interventions throughout her illness is shown in Figure 1.
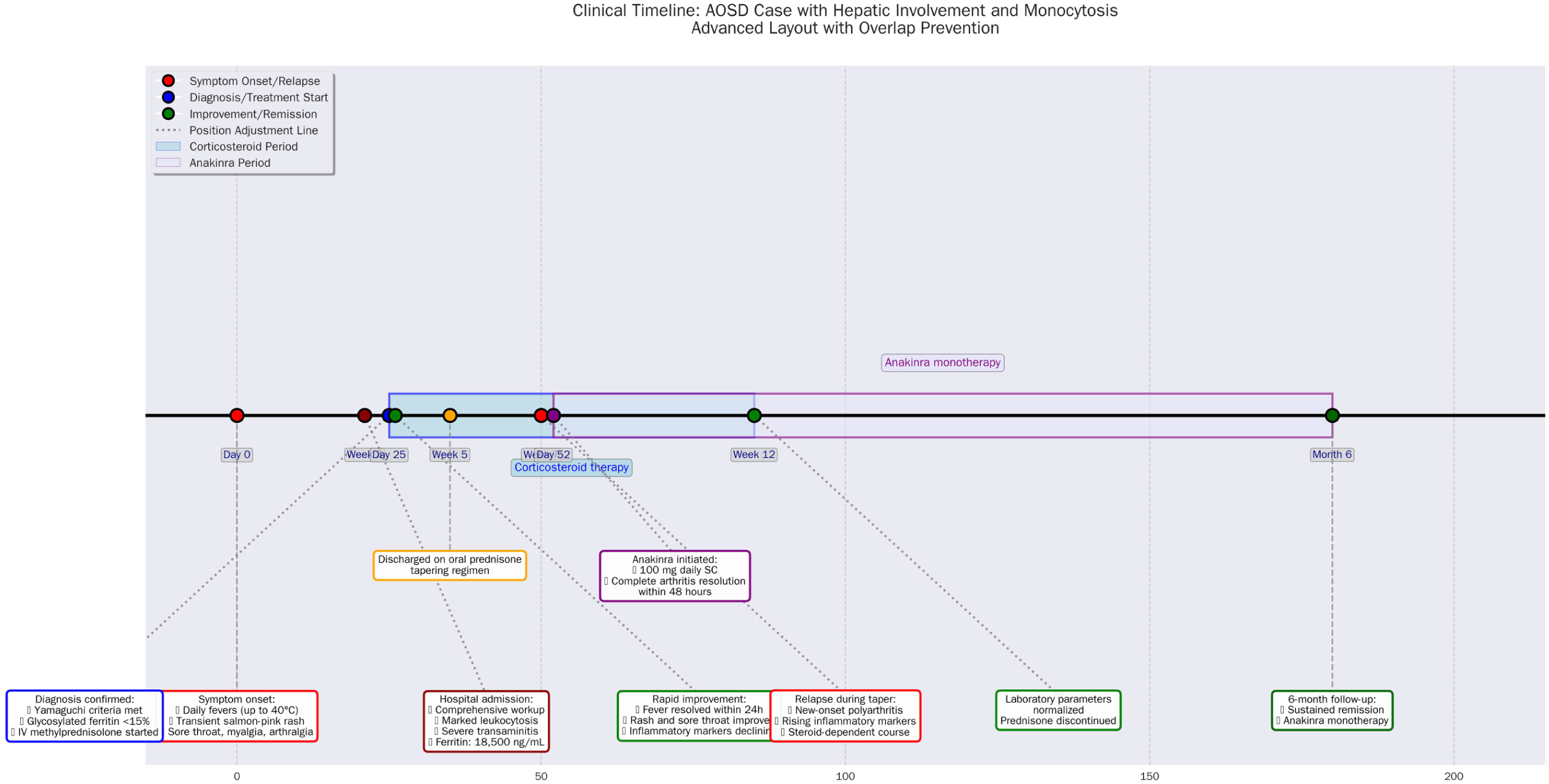
Clinical timeline illustrates the sequence of clinical events, diagnostic milestones, and therapeutic interventions from symptom onset through 6-month follow-up.
The patient experienced significant distress from prolonged fevers, pain, and diagnostic uncertainty. Rapid improvement with corticosteroids and complete resolution with anakinra restored her confidence and highlighted the importance of timely diagnosis and effective treatment.
Discussion
The diagnosis of AOSD is primarily clinical, as no definitive biomarker currently exists, and relies on established classification systems, with the Yamaguchi criteria being the most sensitive and widely used. 6 According to these criteria, a diagnosis of AOSD can be made when at least 5 criteria are fulfilled, including 2 or more major criteria. The major criteria include a fever of at least 39°C persisting for 1 week or longer, arthralgia or arthritis lasting 2 weeks or longer, a typical evanescent salmon-pink rash, and leukocytosis ⩾10 000/μL with at least 80% neutrophils. The minor criteria include sore throat, lymphadenopathy or splenomegaly, liver dysfunction, and negative antinuclear antibody (ANA) and rheumatoid factor (RF) tests. Importantly, these criteria are applied after excluding infectious, neoplastic, and autoimmune conditions that may present with similar features. Before a correct diagnosis and a successful treatment plan can be made, patients usually experience a journey of perplexing symptoms, delayed or incorrect diagnoses, and a number of unsuccessful therapies. All of these can accelerate the onset of the uncommon and sometimes lethal complications associated with AOSD, as well as result in longer hospital stays and increased expenses. 3
The hematological features of AOSD typically include normocytic normochromic anemia, thrombocytosis, and marked leukocytosis, often exceeding 15 000/μL with neutrophil predominance, which can mimic hematologic malignancies. 4 Our patient met all major criteria and several minor criteria. She also had persistent absolute monocytosis, initially raising concern for hematologic malignancy, such as chronic myelomonocytic leukemia, which was subsequently excluded. Macrophage activation syndrome (MAS) was also considered but ruled out, as the patient lacked pancytopenia, coagulopathy, hepatopathy, or hemophagocytosis.5,7,8 To strengthen the diagnosis, we applied the Fautrel criteria, which incorporate glycosylated ferritin ⩽20% as a diagnostic marker; our patient’s level was <15%, allowing a rapid and definitive diagnosis.
Another noteworthy finding in our case is severe hepatitis, as indicated by the incredible ferritin levels of 18 000 ng/dL and transaminitis of more than 15 times the upper limit. Many clinical disorders including infections, chronic liver and kidney illnesses, storage diseases, cancers, and iron overload, can have elevated ferritin levels. But serum ferritin levels under these circumstances hardly ever surpass 3000 ng/mL. On the other hand, Ferritin titers over 10 000 ng/mL are highly suggestive of AOSD and have only been reported following several blood transfusions, in hemophagocytic syndrome (HPS), and in AOSD patients with significant liver damage.9,10
Despite the fact that hepatic involvement is very common in AOSD, with a frequency of 50% to 75%, Yamaguchi’s criteria do not need liver injury in order to diagnose AOSD. 11
Notably, a retrospective study on 77 Chinese AOSD patients revealed that only about 10% of them had ALT and AST levels above 500 IU/L, 12 and another systematic review on AOSD found that most cases of transaminitis are mild and transient, indicating that liver involvement is usually mild to moderate. 5 Severe hepatitis can be seen when AOSD is accompanied by concurrent viral infections such as EBV, CMV, and parvovirus. Medications such as sulfasalazine, iron replacement, and biological therapies have also been linked to serious liver damage in AOSD patients.
Lymphomas, particularly primary hepatic lymphoma, can also mimic AOSD with liver damage. 9 After excluding the previous possibilities, the severe hepatitis and transaminitis in our patient was attributed to AOSD itself.
The mainstay of AOSD treatment includes corticosteroids and NSAIDs, while DMARDs such as methotrexate, azathioprine, and leflunomide are reserved for refractory cases. Biologic agents targeting IL-1 or IL-6, including anakinra, canakinumab, rilonacept, and tocilizumab, are indicated for severe or steroid-dependent disease, and combination therapy with high-dose IL-1 blockade and IV corticosteroids is recommended for patients at risk of MAS.9,13 Given that over 80% of patients fail to achieve remission with NSAIDs and nearly 20% experience adverse effects, we initiated systemic corticosteroids immediately. The patient’s systemic symptoms responded promptly to IV methylprednisolone, but she later developed polyarthritis and rising inflammatory markers, indicating a chronic articular course. We chose anakinra instead of DMARDs due to her persistent monocytosis, markedly elevated inflammatory markers, and the risk of MAS. Methotrexate, while commonly used, achieves disease control in only 40% to 70% of steroid-dependent patients and requires careful liver monitoring. 5 Remarkably, her symptoms resolved within 48 hours of anakinra, confirming the diagnosis and highlighting the central role of IL-1—mediated inflammation. This case underscores the efficacy of biologic therapy over DMARDs, particularly in patients with persistent monocytosis.
Conclusion
This case underscores the diagnostic challenges of Adult-Onset Still’s Disease, particularly when hepatic involvement and persistent monocytosis dominate the presentation. Recognizing AOSD as a potential cause of febrile hepatitis with extreme hyperferritinemia is crucial to avoid delays in management. The rapid and complete response to anakinra further supports the pivotal role of IL-1—mediated inflammation in AOSD and highlights the efficacy of early biologic therapy in achieving remission and preventing complications.
Supplemental Material
sj-docx-1-icr-10.1177_11795476251401288 – Supplemental material for Atypical Presentation of Adult-Onset Still’s Disease with Predominant Hepatic Involvement and Monocytosis: A Case Report
Supplemental material, sj-docx-1-icr-10.1177_11795476251401288 for Atypical Presentation of Adult-Onset Still’s Disease with Predominant Hepatic Involvement and Monocytosis: A Case Report by Ziad W. Elmezayen, Zeina Zakarya Marzouk and Mohammad Adi in Clinical Medicine Insights: Case Reports
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethical approval was not required for this case report, as it involves a single patient and does not meet the criteria for research requiring institutional review board (IRB) oversight. The use of authorized medications was consistent with clinical practice guidelines, and the management of this individual patient did not require IRB approval. This case report adheres to the CARE (CAse REport) Guidelines for accurate and transparent reporting of clinical cases.
Consent to Participate
Written informed consent was obtained from the patient prior to publication of this case report and any accompanying images. This consent includes permission for the use of unauthorized, off-label medications as part of the treatment plan. The completed consent form is available to the Editor upon request and will be treated confidentially.
Authors Contribution
Ziad W. Elmezayen: Conceptualization, Supervision, Study Design, Writing – Review & Editing. Zeina Zakarya Marzouk: Methodology, Data Interpretation, Approval of Final Manuscript, Supervision. Mohammad Adi: Data Curation, Formal Analysis, Writing, Writing – Original Draft, Review and Editing, Contributions to Discussion.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data pertinent to this case report have been included in this article. Further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.