
Abstract
Background:
Musculoskeletal symptoms are a presenting manifestation in a number of lymphoproliferative disorders including leukemia, especially in children. Among these primary symptoms, midfoot arthritis seems to be an important alarm for malignancy in children. The aim of this study is evaluation association of midfoot arthritis with malignancy in children.
Method:
In this cross-sectional study, all medical records of patients with arthritis were identified and reviewed. All clinical and laboratory data were recorded in the information form and data were analyzed by SPSS 25 software.
Results:
A total of 557 cases of arthritis were evaluated, of which 18 (3.2%) cases have primary symptoms of midfoot arthritis. Four of 18 patients (22.2%) had B-cell precursor acute lymphoblastic leukemia, that midfoot arthritis was their first manifestation. Also, their laboratory findings confirmed that platelet, lactic acid dehydrogenesis, and uric acid values were significantly higher in these children. Based on statistical evaluation, there was no significant difference between age and sex in these patients.
Conclusion:
According to the findings of the present study, it can be concluded that “midfoot arthritis” may be the first manifestation of leukemia in children even with a near-normal hematologic values.
Background
Children with a variety of malignancies, especially leukemia, may be diagnosed with various symptoms. Malignancies often involve the musculoskeletal system. 1 Skeletal symptoms are often characterized as centralized or diffuse bone pain, and in some patients arthritis is associated with these conditions. Leukemia is one of the most common childhood malignancies.2,3
Bone and joint pain has been reported in 20% to 59% of children with acute lymphoblastic leukemia (ALL). This pain has been reported in the bone and articular region, which is usually acute, localized, severe, and sudden onset, but may also be intermittent. 4 Osteoarthritis due to malignancy appears to be due to bone, periosteal, or bone capsule injuries and less synovial involvement.5,6
However, leukemic infiltration has been shown in some patients, and in others, elevated serum uric acid has an important role. Immune complexes in patients with various malignancies have shown that acute leukemia may present with symptoms similar to childhood rheumatic diseases and may delay the diagnosis. 7 Schwaler studied 10 children with rheumatologic and leukemia-related diseases who were involved in knees, ankles, and elbows at the same time. 8 Beukelman et al 9 studied 6 children with arthritis associated with acute leukemia, who mentioned that positive laboratory evidence of rheumatologic disease was the definitive diagnosis in most patients with leukemic arthropathy. “Midfoot” portion of the foot is analogous to the articulation, or joint formation. Various studies have reported a link between types of malignancy and bone disease however; midfoot arthritis seems to be a red flag.8,9 According to abovementioned studies, ALL presenting with osteoarticular manifestations may initially be misdiagnosed, leading to a significant delay in diagnosis and management. The present study was designed to determine the association of midfoot arthritis as the first manifestation of ALL in children.
Patients and Methods
Study setting
This study was a cross-sectional (descriptive-analytical) study that was performed in a pediatric hospital.
Study population
The statistical population included all children with arthritis and primary symptom of midfoot arthritis referred to Pediatric Hospital. Sample size included all children with arthritis and juvenile idiopathic arthritis (JIA) with primary symptom of midfoot arthritis referred to Mofid Children Hospital during 2009 to 2018.
Measurements
The study was performed on children with arthritis who referred to the pediatric hospital with primary symptoms of midfoot arthritis during 2009 to 2018. Midfoot arthritis was diagnosed by physical examination and using ultrasound. After obtaining the necessary licenses, all medical records of patients with arthritis were reviewed. In the presence of midfoot arthritis in children, demographic data; clinical and paraclinical findings; and clinical symptoms including fever, weight loss, morning stiffness, laboratory results of white blood cell (WBC), hemoglobin (Hb), platelet (PLT), erythrocyte sedimentation rate (ESR), lactic acid dehydrogenesis (LDH), C-reactive protein (CRP), uric acid, calcium, anti nuclear antibody (ANA), and rheumatic factor (RF) were recorded in a questioner for all patients. Then bone marrow aspiration and biopsy findings and bone marrow flow cytometry were evaluated to determine the presence of malignancy. If proven malignant, its association with midfoot arthritis was determined. Data were analyzed using SPSS 25 software.
Ethical considerations
Ethical issues completely observed by authors. The study group adheres to the principles of medical ethics introduced by the Health Ministry and the Declaration of Helsinki and legislation in medical ethics committee of Shahid Beheshti University of Medical Sciences and approved the method of study with ethical code as IR.SBMU.MSP.REC.1398.007.
Statistical analysis
Data were analyzed by SPSS software version 25. Normal quantitative variables are represented as mean and standard deviation. One-Sample Test was used to evaluate the normality of the distribution of quantitative variables. Data were analyzed using chi-square, Fisher exact, t test, Mann–Whitney test, and Pearson correlation coefficient. Significance level in all tests considered as P < .05.
Study tools
The data collection tool was an information form that was completed by the researchers with observation technique.
Results
This study was performed on all patients with arthritis referring to Mofid Children Hospital during 2009 to 2018. A total of 557 cases of arthritis were studied, of which 18 (3.2%) cases were diagnosed as having primary symptom of midfoot arthritis and referred to pediatric hospital.
The mean age of children with primary symptom of midfoot arthritis was 7.6 ± 5.4 years, ranging from 1 month to 14 years. Of the 18 children with midfoot arthritis, 6 (33.3%) cases were female and 12 (66.7%) cases were male, with a male to female ratio of 2 to 1. Also the mean duration of illness in children with primary symptom of midfoot arthritis was 9.1 ± 3.9 months with a range of 1 month to 4 years. Regarding the initial diagnosis, the most common primary diagnosis was B-cell precursor acute lymphoblastic leukemia (BCP-ALL) in 4 cases (22%), unclassified arthritis in 4 cases (22.2%), and enthesitis-related arthritis (ERA) in 3 cases (16.7%) (Figure 1). Overall, midfoot arthritis was bilateral in 4 patients (22.2%) and unilateral in 14 patients (77.8%). A total of 6 children (33.3%) had clinical symptoms, with arthralgia (67%) and fever (22.2%) being the most common clinical symptom in children with primary symptom of midfoot arthritis (Figure 2). Involvement of joints other than midfoot joints was observed in 14 patients (22.2%), knee (8 patients, 44.4%) and ankles (6 patients, 33.3%) being the most common joints (see Figure 3). The mean and standard deviation of patients’ laboratory parameters were often at normal levels which are fully stated in Table 1. On the other hand, laboratory data showed that platelet, LDH, and uric acid values were significantly higher in children with malignancy (P < .05) (Table 2). Just 1 of the patients had positive ANA, but none of them had a positive RF. There was no significant difference between age and sex of patients and fever between patients with arthritis and BCP-ALL (P > .05) (Table 3).

Frequency distribution of final diagnosis in children with midfoot arthritis. ALL indicates acute lymphoblastic leukemia; ERA, enthesitis related arthritis; JIA, juvenile idiopathic arthritis; PSRA, post streptococcal reactive arthritis.

Frequency distribution of clinical symptoms in children with midfoot arthritis.

Distribution of frequency of other painful joints in children with midfoot arthritis.
Distribution of laboratory values in children with midfoot arthritis.
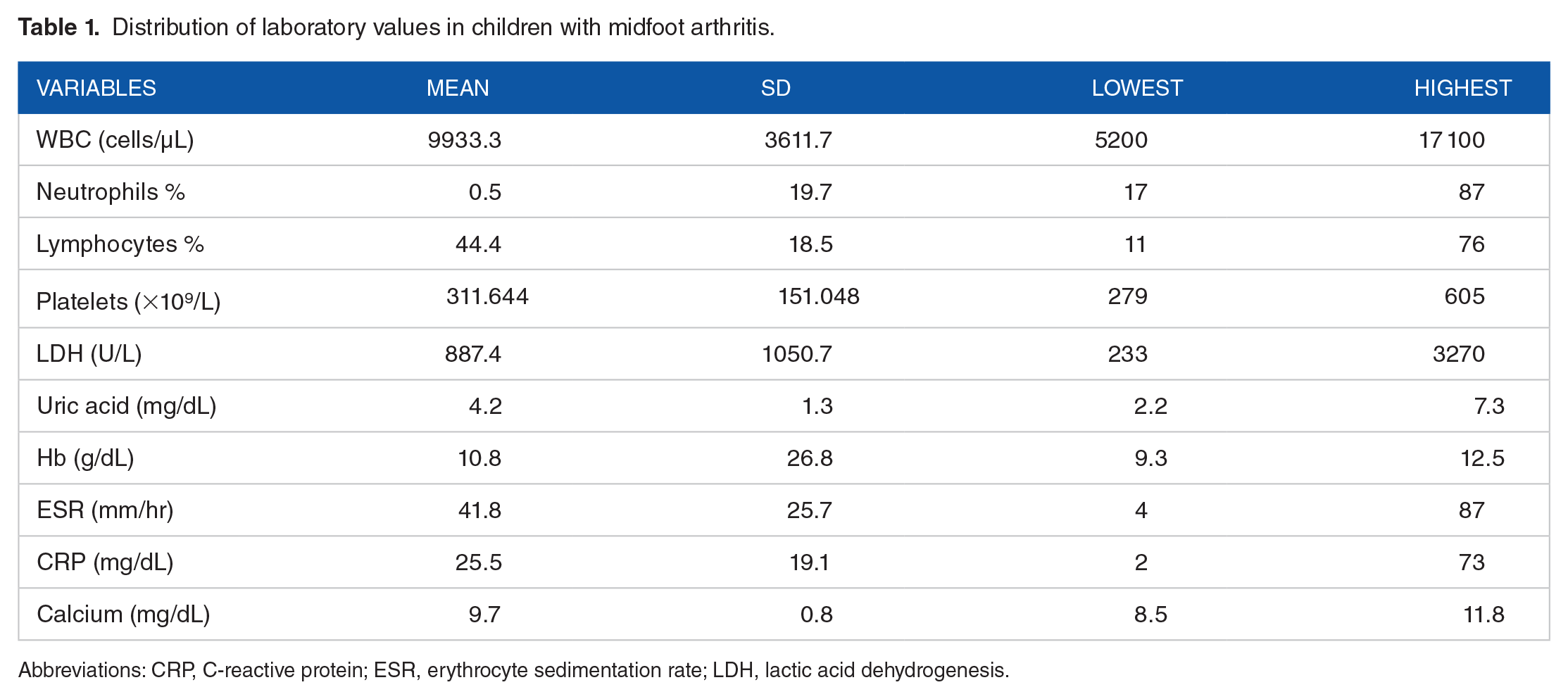
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; LDH, lactic acid dehydrogenesis.
Comparison frequency of abnormal laboratory findings by final diagnosis in children with midfoot arthritis.
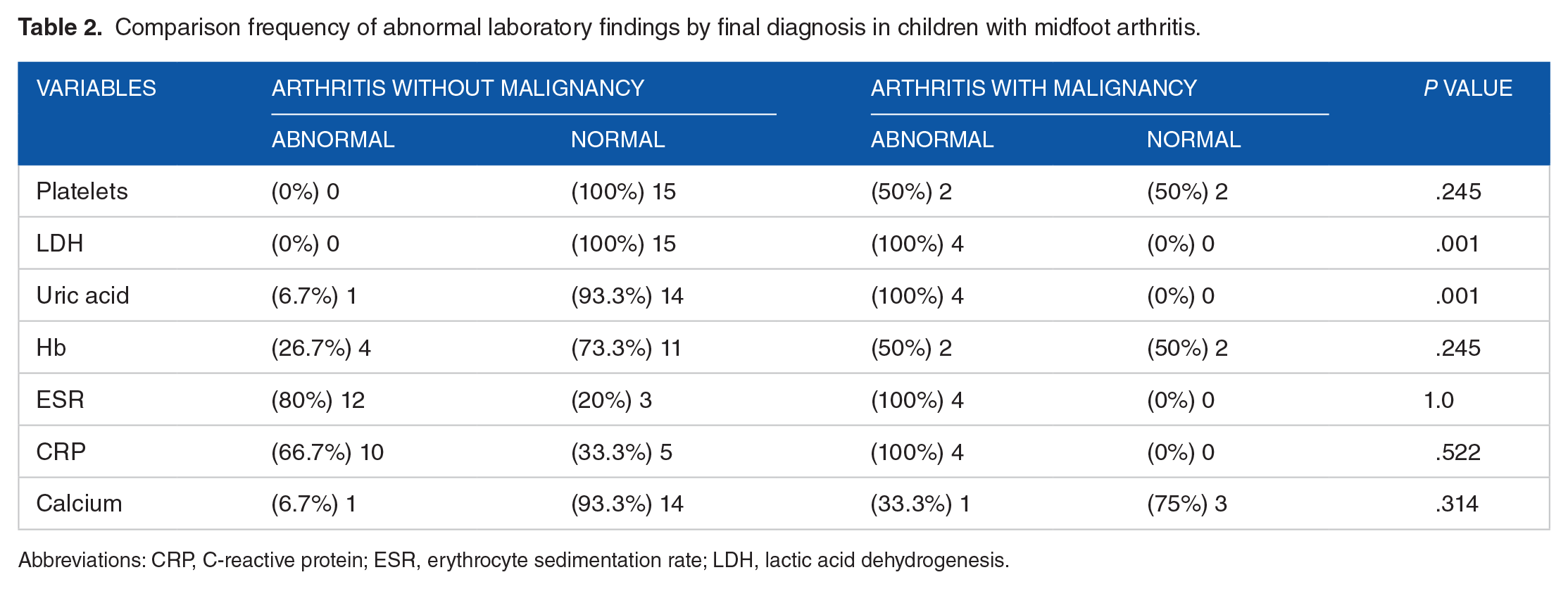
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; LDH, lactic acid dehydrogenesis.
Comparison frequency of risk factors in children with midfoot arthritis.
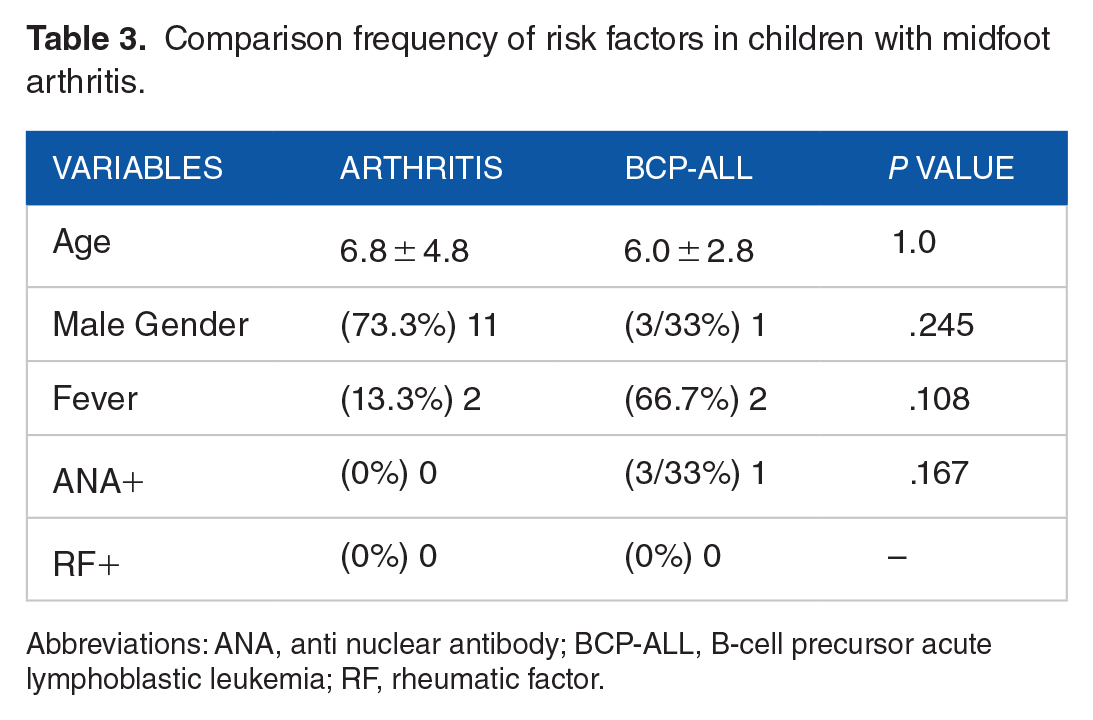
Abbreviations: ANA, anti nuclear antibody; BCP-ALL, B-cell precursor acute lymphoblastic leukemia; RF, rheumatic factor.
Discussion
Cancer as a chronic disease after accidents and unintentional deaths is the third cause of death among children aged 1 to 14 years. 10 However, childhood cancers are neglected in developing countries, even though approximately 84% of the cancer cases below 15 years old occur in the low-income and middle-income countries. 11 The prevalence of acute lymphoblastic leukemia in boys is higher than in girls and the prevalence increases with age. 12 In Iran, during the years 2003 to 2008, the percentage of annual changes in leukemia in men and women were estimated to be 18.7% and 19.9%, respectively. It has also been reported that bone and joint pain occurs in 21% to 29% of children with acute leukemia. The pain caused by bone leukemia usually begins with a sharp, localized, severe, and sudden onset that can also be intermittent. 13
Present study was performed on all patients with arthritis and JIA referring to Mofid Children Hospital during 2009 to 2018. The aim of this study was to determine the association of midfoot arthritis with malignancy. A total of 557 cases of arthritis and JIA were studied, of which 18 (3.2%) referred to pediatric hospital with primary symptom midfoot arthritis during 2009 to 2018. Using ultrasound showed that the joint between the midfoot and forefoot (tarsometatarsal) was most involved. Also based on flow cytometry and bone marrow biopsy findings, 4 patients (22.2%) had BCP-ALL who had delayed diagnosis of cancer due to referral to pediatric rheumatology clinic with early diagnoses of JIA and psoriatic arthritis. Laboratory findings confirmed that platelet, LDH, and uric acid values were significantly higher in these 4 children with malignancy. Overall, none of the patients had a positive rheumatoid factor. ANA positive was seen in 1 patient with malignancy. There was no significant difference between the age and sex of patients and the presence of fever between patients with arthritis and malignancy.
Midfoot arthritis is a challenging problem that causes chronic pain and affects daily activity. In the Phatak et al 14 study, 55 children with ERA were studied, with a prevalence of Midfoot involvement in 24 patients (43.6%); only 2 case studies were found in the literature review. In a study by Dewar et al, a 5-year-old boy was described who had suffered left ankle injury 2 weeks before admission. He had swelling and tenderness on the midfoot side. The patient was initially considered to be a soft tissue injury, but with increased leg pain; in this patient, radiography and tests were normal. Two weeks later, he was diagnosed with acute myeloid leukemia after bone marrow aspiration. 13 In the Simard et al study, 9027 children with JIA were studied, the relative risk of malignancy in these patients was 1.1% compared with the control group. Increased risk of cancer was significantly associated with longer duration of illness. 15
In the Nordstrom et al study, the incidence of malignancy was 0.67 per 100 000 cases in children with JIA and 23.2% in healthy individuals. Children with JIA are also about 3 times more likely to develop cancer than healthy ones. 16 Also in a study by Bernatsky et al, an invasive malignancy occurred in 1834 patients compared with the 7.9 Hodgkin’s lymphoma. The researchers concluded that in the first years after the diagnosis of JIA, the risk of invasive cancers did not increase significantly. But it is possible to increase the risk of hematologic malignancies. 17 In addition, Thomas et al studied 652 patients with rheumatic diseases in Scotland between 1978 and 1992. Among patients with rheumatoid arthritis, the potential risk of hematopoietic, lung and prostate cancer was increased. 18 In the study of Schaller et al, 13 children with acute lymphoblastic leukemia with joints with swelling, heat, and loss of movement were similar to rheumatoid arthritis, but severe articular pain and tenderness and multiple joint involvement were obvious. Symptoms were seen in more than 1 month in 1 joint in 60% of children. In 1 case, erosion of the sacroiliac joints was observed. 19
In the study of Heinrich et al, 107 children with acute lymphoblastic leukemia were studied. Fifty-seven percent of children had skeletal abnormalities in radiology at the time, and 75% of evaluated cases had bone metaphysis disorders. Fifty-two percent had osteoporosis or periosteal reaction and 46% had diffuse osteopenia, 15% of sclerotic changes, 13% of lytic lesions, 4% of mixed lithic and sclerotic pattern had bone changes. Seven percent of children with acute lymphoblastic leukemia had a pathological fracture that occurred in the spine. The follow-up period in these patients was 10 years. 20 In addition, in the Jonsson et al study, bone pain was the primary symptom of childhood with acute lymphoblastic leukemia. Of the 296 patients studied, 52 (18%) cases had bone pain that prevented other leukemia manifestations. In addition, patients with bone pain had lower serum uric acid and calcium levels than other children. 21 Therefore, most results that observed in these studies were coordinated with our finding.
Conclusion
Based on the findings of the present study, it can be concluded that midfoot arthritis itself is not common in children (3.2%). However, the chance of leukemia is high in children with the midfoot arthritis (22.2%) even with near-normal hematologic values. Therefore, we recommend bone marrow aspiration and flow cytometry for all children with midfoot arthritis especially when the serum levels of uric acid and/or LDH are higher than normal limits.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Authors make substantial contributions to conception and design, and/or acquisition of data, and/or analysis and interpretation of data: R.S., N.S., K.R., V.J.P., and S.S.
Authors participate in drafting the article or revising it critically for important intellectual content: R.S., N.S., M.H.Y., and S.S.
Authors give final approval of the version to be submitted and any revised version: R.S.