
Abstract
Objective:
This study explores a suspected increasing incidence of Lyme arthritis in the Western New York pediatric population. In addition, we aim to describe a clinical picture of Lyme arthritis and the clinical features that distinguish it from other forms of arthritis.
Methods:
Patients diagnosed with Lyme arthritis between January 2014 and September 2018 were identified using International Classification of Diseases—10th Revision (ICD 10) codes for Lyme disease and Lyme arthritis. Patients were included in the study if they (1) exhibited arthritis, (2) tested positive for Lyme antibodies, and (3) exhibited a positive Western blot.
Results:
A total of 22 patients were included in the study. There was a general trend toward an increasing number of cases of Lyme arthritis over the 45-month observation period. We identified 1 case in each 2014 and 2015, 4 cases in 2016, 7 in 2017, and 9 in the first 9 months of 2018. In total, 17 patients had arthritis as their only symptom at the time of diagnosis and 10 patients had a rash or a history that prompted suspicion of Lyme disease. The knee was the most frequent joint (86.4% of patients), and patients typically had 2 or fewer joints affected (86.4% of patients).
Conclusions:
A significant increase (P = .02) in Lyme arthritis cases was observed at Oishei Children’s Hospital of Buffalo. Lyme arthritis may clinically present similarly to other forms of arthritis, such as oligoarticular juvenile idiopathic arthritis, so health care providers should be aware of distinguishing clinical features, which include rapid onset of swelling and patient age. Because the geographic area of endemic Lyme disease is expanding, all health care providers need to be aware of Lyme arthritis as a possible diagnosis.
Introduction
Lyme disease is an infection caused by Borrelia burgdorferi, which is primarily transmitted by 2 ticks: Ixodes scapularis and Ixodes pacificus. 1 Transmission results from a tick bite with a tick attachment for 24 to 48 hours. 1 The clinical manifestations of Lyme disease depend on the stage of the illness. Early localized disease occurs within the first 2 to 3 weeks of infection and typically presents with erythema migrans, sometimes accompanied by systemic findings, such as fever, fatigue, headache, neck pain, arthralgia, or myalgia.2,3 Early disseminated disease usually occurs weeks to several months after the tick bite. The clinical manifestations include multiple erythema migrans, cranial nerve palsy, meningitis, and carditis. Systemic signs and symptoms, such as fever, fatigue, headache, and arthralgia, are common in this stage.1,4 Late Lyme disease occurs weeks to months after the initial infection if the initial infection is not treated effectively, with arthritis being the most common manifestation. 5
Lyme arthritis, the presenting symptom in approximately 60% of untreated Lyme disease cases, often presents as asymmetric pain and swelling of one or more larger joints. 2 Most commonly, the affected joint typically shows warmth and swelling, and may show decreased range of motion and pain with motion or weight bearing. 6 The swelling can resolve spontaneously and will often reappear, affecting the same joint or another joint.
A 2-tiered test is recommended to confirm a diagnosis of Lyme arthritis. First, an enzyme-linked immunosorbent assay (ELISA) test for Lyme antibodies is completed, followed by a confirmatory Western blot (WB) test for recognition of 10 B burgdorferi proteins by immunoglobulin G (IgG) antibodies and 3 immunoglobulin M (IgM) proteins.7,8 Although untreated Lyme arthritis does not typically cause permanent damage, symptoms will persist or recur until the infection is treated with antibiotics. 7 The current Centers for Disease Control and Prevention 9 (CDC) recommendations for antibiotic treatment of Lyme arthritis are doxycycline, amoxicillin, and/or cefuroxime axetil.
In 1991, Lyme disease became a nationally notifiable condition in the United States. Data from the CDC show not only that the number of cases of Lyme disease in high-incidence areas has risen since 1991, but also that the geographic area where Lyme disease has been diagnosed is expanding.10 -12 Although the overall number of Lyme disease cases has remained relatively constant over the past 10 years, specific areas, mostly in the Northeast, have seen an increase in the number of Lyme disease cases (Figure 1). Erie County, the county in which Buffalo, New York resides, has seen an increase from 14 cases in 2011 to 53 cases in 2016. Erie County saw an even more drastic increase of cases from 2016 to 2017, reporting an increase of 53 to 89 cases in that year alone. 13
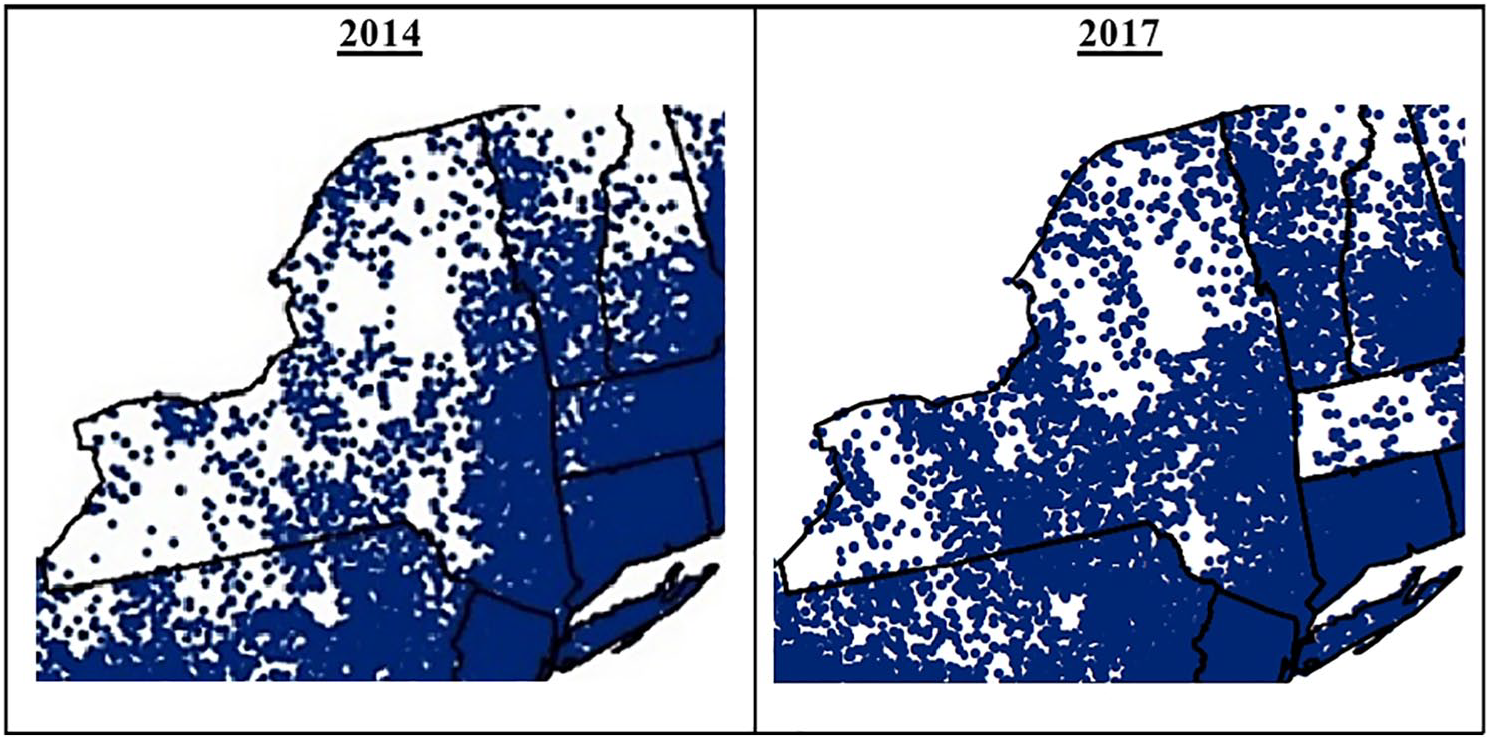
Incidence of cases of Lyme disease reported to the CDC between 2014 and 2017. Each dot represents a reported case of Lyme disease. An increase in the density of dots in certain areas indicates an increase in the incidence of Lyme arthritis in those areas. 12 CDC indicates Centers for Disease Control and Prevention.
The Pediatric Rheumatology Clinic at John R. Oishei Children’s Hospital, located in Buffalo, New York, observed an increase in Lyme arthritis diagnoses in 2017. By examining Lyme arthritis cases retrospectively, this study aims to (1) highlight the increasing incidence of Lyme arthritis as it correlates to the overall increase in Lyme disease incidence in the Western New York area, (2) describe the clinical manifestations and laboratory results in Lyme arthritis, and (3) increase awareness among health care professionals of arthritis as a first presentation of Lyme disease. This is especially important as other arthritic diseases, such as oligoarticular juvenile idiopathic arthritis (oligo JIA), often present similarly to Lyme arthritis.
Materials and Methods
This study retrospectively analyzed the medical records of children diagnosed with Lyme arthritis at John R. Oishei Children’s Hospital of Buffalo, in Western New York, between January 2014 and September 2018. Patients were identified using the International Classification of Diseases—10th Revision (ICD 10) code for Lyme disease (ICD 10 code A69.20) and Lyme arthritis (ICD 10 code A69.23). Patients were included in the study only if they exhibited (1) arthritis clinically, (2) positive testing for Lyme antibodies by enzyme immunoassay (EIA) or indirect immunofluorescence assay (IFA), and (3) a positive WB of recognition of at least 5/10 B burgdorferi proteins by IgG antibodies or 2/3 B burgdorferi proteins by IgM antibodies. This criterion is in alignment with CDC recommendations. 14 Patients also had to be 17 years or younger at the time of diagnosis to be included in the study. A total of 22 patients met these criteria and were thus included in the study. No patients who met these criteria were excluded from the study.
For each patient included in the study, the following data were recorded: demographics (age, sex, race, and county of residence), clinical presentation and physical exam findings at the time of the initial health care visit, laboratory findings (white blood cell [WBC] count, hemoglobin (Hgb), platelet count, erythrocyte sedimentation rate [ESR], C-reactive protein (CRP) level, and Lyme ELISA and WB results). In addition, the results of the synovial fluid analysis of 8 patients were also recorded and analyzed for the number of RBCs, nucleated cells, as well as gram stain and culture results. Polymerase chain reaction (PCR) for B burgdorferi DNA was performed in 3 patients and reported.
Analytic plan
Demographics, number of affected joints, and laboratory findings (WBC count, ESR, CRP), and synovial fluid findings were reported as means, standard deviations, and ranges. Geographic and clinical presentation characteristics of Lyme disease were described in frequencies and percentages. Pearson chi-square test of homogeneity was used to test whether Lyme disease cases changed over the annual periods from 2014 through 2018. All statistical tests were conducted assuming an alpha of 0.05 and with SYSTAT 13 (Systat Software, 2004).
Results
Demographics and incidence
In total, 22 patients were included in this study. Of these, 13 patients identified as male and 9 identified as female. The mean age of all patients was 8.59 years (range: 2-16). As shown in Figure 2, most of the patients resided in Erie County (65.6%). Overall, 1 (4.5%) patient was diagnosed in 2014, 1 (4.5%) in 2015, 4 (18.2%) in 2016, 7 (31.8%) in 2017, and 9 (40.9%) in the first 9 months of 2018 (Figure 3). This resulted in a statistically significant (P = .02) increase in the cases of Lyme arthritis diagnosed at Oishei Children’s Hospital between January 2014 and September 2017 using Pearson chi-square test of homogeneity.

The number of Lyme disease cases organized by the county wherein each patient resided. Only counties in Western New York (WNY) were included, but it should be mentioned that 2 patients resided outside of WNY, including 1 patient resided in McKean County in Pennsylvania and 1 patient resided in North Carolina.

(A) Number of Lyme arthritis (LA) cases seen at Oishei Children’s Hospital each year between 2014 and September 2018. (B) Number of Lyme disease (LD) cases reported by Erie County, NY Department of Health each year between 2014 and 2017 plotted with the number of LA cases seen at Oishei Children’s Hospital each year between January 2014 and September 2018.
Clinical presentation of affected patients
Every patient required a clinical diagnosis of arthritis to be included in this study. Most patients (86.4%) presented with 1 or 2 joints affected, with the number of joints affected at presentation ranging from 1 to 13 joints (Table 1). The knee joint was the most common joint affected with 19 patients (86.4%) exhibiting arthritis in at least 1 knee, and in 13 patients (59.1%) the knee joint was the only joint affected. The second most common locations were the ankle joint (18.2%) and the wrist joint (18.2%). In an unusual presentation for Lyme arthritis, 2 patients presented with arthritis in the interphalangeal joints bilaterally.
Demographic and disease characteristics of 22 patients with Lyme arthritis.

Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; RBC, red blood cell; WBC, white blood cell.
In 17 patients (77.3%), arthritis was the only clinical sign at the time of diagnosis. Furthermore, in 13 (59.1%) patients, there was no documentation or recollection of any symptoms of early Lyme disease, so it is possible that arthritis was the presenting symptom in these patients. Three patients (13.6%) also presented with neurologic symptoms in addition to arthritis, including 1 patient presented with a seventh nerve palsy, 1 patient presented with numbness in his legs, and 1 patient presented with headaches. Three patients (13.6%) presented with a rash. It should be noted that another 3 patients (13.6%) had a self-reported history of a rash or bug bite that had since resolved and 4 patients (18.2%) had a history of camping or residing in a wooded area. Therefore, 10 patients (45.5%) had a rash or a history that would cause a clinician to consider a Lyme arthritis diagnosis.
Laboratory evaluation of affected patients
The main methods of laboratory evaluation consisted of ESR, CRP, ELISA test for Lyme antibodies, and WB confirmation of ELISA results. The mean ESR for the 21 patients who had values reported was 46.76 mm/h and the average CRP for the 20 patients who had values reported was 32.85 mg/L (Table 1). An ELISA test for Lyme antibodies was performed for all patients and the average was 4.65 (range: 1.14-13.11). A WB was performed for all 22 patients, but the number of IgG and IgM antibodies present was reported for only 20 patients. There was 1 patient with Lyme antibodies 5.1 and WB from the available medical record reports positive IgG and negative IgM without giving the number of positive IgG proteins. There was another patient with positive Lyme antibodies 5.62 and WB from the available medical record reports positive IgG and negative IgM without giving the number of positive IgG proteins. Of those 20 patients, 14 (70.0%) were recorded as having IgG antibodies recognizing all 10 B burgdorferi proteins on the WB analysis and 7 (35.0%) were recorded as having IgM antibodies recognizing all 3 IgM proteins. The 7 patients who had positive IgM also had 6 or more positive IgG proteins.
For 8 patients, synovial fluid was also analyzed and the reported nucleated cell count, RBC count, gram stain, bacterial culture, PCR for B burgdorferi DNA if it was done, fluid appearance, and source of fluid were recorded for each analysis. For the 8 analyses that were performed, there was a nucleated cell count average of 36 664 cells/µL with the range of 7530 to 81 000 cells/µL (Table 1). One synovial fluid sample appeared to contain blood from an extraction error and was described to have bloody, red appearance. The average RBC count for the remaining 7 non-bloody synovial fluid analyses was 5325 cells/µL which ranged from 333 to 13 200 cells/µL. A PCR of synovial fluid for B burgdorferi DNA was also performed for 3 patients. All 3 patients had a positive PCR for B burgdorferi double-stranded DNA. All 8 samples had negative gram stain and negative culture.
Discussion
The results of this study indicate that there was a statistically significant (P = .02) increase in Lyme arthritis cases diagnosed at Oishei Children’s Hospital between January 2014 and September 2018 (Figure 3). If it can be assumed that the travel in and out of the Western New York region and the geographic area that Oishei Children’s Hospital serves has not changed significantly between 2014 and 2018, it is likely that this increase in the number of cases seen at Oishei Children’s Hospital represents an increase in the incidence of Lyme arthritis in Erie County and the greater Western New York region. Furthermore, there was a 75% increase in Lyme arthritis cases at Oishei Children’s Hospital between 2016 (n = 4) and 2017 (n = 7), which appears to be similar to the reported 67.9% increase in Lyme disease cases in Erie County between 2016 (n = 53) and 2017 (n = 89) (Figure 3B).
It should be noted that the study has several limitations. The data were limited to patients in the Oishei Children’s Hospital network, and it is therefore possible that more cases of Lyme arthritis could have been seen in other health care facilities over the period covered here. In addition, Lyme arthritis diagnoses are typically delayed and Lyme arthritis can present anywhere from months to years after a tick bite. 5 Our patients displayed a variable time course from the onset of symptoms to diagnosis that ranged from 1 to 365 days. In addition, the observed increase in Lyme disease and Lyme arthritis could have been due, at least in part, to local practitioners becoming more aware of the diagnosis and increasing their likelihood of testing for Lyme throughout the years observed in the study. Finally, it should be noted that John. R. Oishei Children’s Hospital moved locations in the Fall of 2017. This should not influence the recorded number of cases because the hospital moved only a distance of 1.1 miles and both locations are accessible by public transport, but it is a limitation of the study because no analysis was done to confirm that both locations were equally accessible.
Having a well-defined clinical picture of Lyme arthritis becomes increasingly important as the geographic area of Lyme disease expands. The clinical picture constructed by the results of the study is as follows: arthritis of 1 or 2 large joints, most commonly the knee that comes on suddenly and without any other symptoms in a child around the age of 8 years. History may reveal a previous rash or history of being in a forested area, but more often than not the history will give no indication to a previous Lyme disease infection or tick bite. 7 In our patients, we have 3 patients who have rash at the time of presentation and that is atypical as rash is usually early presentation in Lyme disease and arthritis is usually a late presentation. Laboratory tests will usually show an elevated ESR and CRP, whereas WBC count and Hgb will remain approximately normal. Synovial fluid analysis, if done, will show a variable, but an elevated number of WBCs present in the fluid. Finally, treatment with amoxicillin or doxycycline is usually sufficient. 9 In our patients, 77.3% required only 1 round of treatment.
The clinical picture derived from our data is reflective of the literature on Lyme arthritis. Studies that used child cohorts reported average patient ages of 8.1 to 9.5 years, with a higher male-to-female ratio.6,15,16 It should be noted that there is no proven physiological difference in sex that makes men more susceptible. Arthritis is frequently a presenting symptom, seen in approximately 60% of untreated Lyme disease cases.4,6,7 For 59.1% of our patients, arthritis was the first and only presentation of a Lyme disease infection. Although this is not an exact parallel, every case in our study is a patient that had untreated Lyme disease until it progressed to Lyme arthritis. When arthritis is the presenting feature, the literature reports an average number of 2 joints affected,3,15,16 with the knee being the most common. Our study found an average of 2.41 joints, but this result is skewed due to 1 patient that presented with 13 joints affected. This patient has confirmed Lyme testing with positive Lyme antibodies 13.11 and 10 IgG proteins by WB and should increase awareness about Lyme arthritis presentation with multiple joint involvement including small joints though it is not the typical presentation. In addition, Lyme arthritis typically has a sudden onset of swelling in the affected joint that may occur with or without pain. This swelling has been shown to resolve and remit periodically.7,15
Our data revealed that inflammatory markers, ESR and CRP, were nearly always elevated, but existed within a wide range. The literature shows that elevated ESR and CRP are highly likely in Lyme arthritis cases, that is, average ESR of 39 to 44.6 mm/h and CRP of 2.7 to 38.5 mg/L, but normal values should not exclude a diagnosis.6,15,17 In addition, ranges in synovial WBC counts are reported from hundreds to hundred thousands.6,15,17 Our study found an elevated average synovial WBC count (36 664) with a large SD (Table 1). Although many of the numbers from the study were not statistically significant due to a small sample size, the average laboratory and clinical values that were calculated do appear to be in line with the existing literature on Lyme arthritis.
The significant increase in Lyme arthritis cases observed at Oishei Children’s Hospital of Buffalo in the past 5 years indicates that the incidence of Lyme arthritis cases can be more than double in a few short years. As Lyme disease, and therefore Lyme arthritis, continues to spread quickly over a larger geographic area, it is important for all health care providers to be aware of the clinical features of Lyme arthritis, not just the providers in currently endemic areas. Diseases like oligo JIA that also cause swelling and arthritis in 4 or fewer joints and commonly affect the knee joint have a very similar presentation to Lyme arthritis and could easily lead to cases of Lyme arthritis being misdiagnosed.18 -20 It is very important for physicians to understand that testing is essential to make a diagnosis of oligo JIA over Lyme arthritis and to remember to test explicitly for Lyme arthritis. Better awareness of the increase in the incidence of Lyme disease and Lyme arthritis in previously low-incidence areas will lead to earlier and better patient diagnosis and management.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Oscar Gomez, MD in manuscript editing and review.
Author Contributions
All authors were involved with the drafting and/or revising of the manuscript and all authors approved the final draft for submission.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through the Rheumatology Research Foundation Medical and Graduate Student Preceptorship Grant.
Availability of Data
As per the study’s institutional review board, the data will be available until January 2020. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The University at Buffalo Institutional Review Board (UBIRB) issued a waiver due to the data being collected via chart review.