
Abstract
Vascular compromised fractures typically result in a high rate of healing complications, such as avascular necrosis, nonunion, delayed union, and arthritis, which severely affect a patient’s function and quality of life. The purpose of this review was to identify and describe the epidemiology and available treatment options for the most well-known vascular compromised closed fractures. The injuries discussed in detail in this review were scaphoid, lunate, femoral neck, and talar fractures. Current evidence suggests that optimal treatment for vascular compromised fractures is dependent on the degree of fracture displacement and comminution, and the patient’s post-injury functional demands, age, and bone quality. Conservative efforts generally include casting or splinting with a period of immobilization. Surgery is indicated for substantially displaced fractures, patients who require higher functional demands and an earlier return to activity, or if complications occur following nonoperative treatment; however, operative intervention is typically performed for femoral neck fractures regardless of the amount of displacement. Various surgical techniques exist, though internal fixation with screws is a common procedure among these injuries and can be used in combination with other implants, such as plating or Kirschner wires (k-wires), when needed. Severe fracture comminution, poor bone quality, or arthritis can contraindicate the use of screws and more invasive intervention will be required. Bone grafting is done in some cases to enhance vascularity. Salvage procedures exist for patients who develop severe complications, but these will permanently alter the anatomy of the injured area and should be considered a last resort.
Introduction
Vascular compromised fractures are injuries with a severely impaired healing process due to the limited blood flow to these areas.1–4 Because of this, fractures in these regions are associated with a high rate of necrosis and union complications, making the management of these injuries challenging.1,4–7 The purpose of this review was to identify and describe the epidemiology and treatment options for the most well-known vascular compromised closed fractures.
Background on scaphoid and lunate fractures
Fractures of the scaphoid represent about 50% to 90% of all carpal fractures in young, physically active individuals.1,8 Approximately 345 000 scaphoid injuries occur in the United States every year. 3 With these injuries, the patient will present with wrist pain on the radial side after a traumatic event. 9 There may also be tenderness in the anatomical snuffbox, pain on palpation of the scaphoid, pain with axial compression of the thumb, and pain in the thumb during range of motion (ROM). 9 These clinical signs are important to investigate, as the injury may be missed on plain radiographs. 9 Advanced imaging will help determine fracture stability and amount of displacement. 9 Because of the vascular insufficiency present in the scaphoid bone, nonunion is a common complication following injury to this area, with rates ranging from 5% to 15%.1,3 Other concerns include delayed union, arthritis, reduced wrist motion, and loss of strength. 3 The probability of a scaphoid nonunion will be reduced with early recognition, appropriate treatment, and immobilization. 10
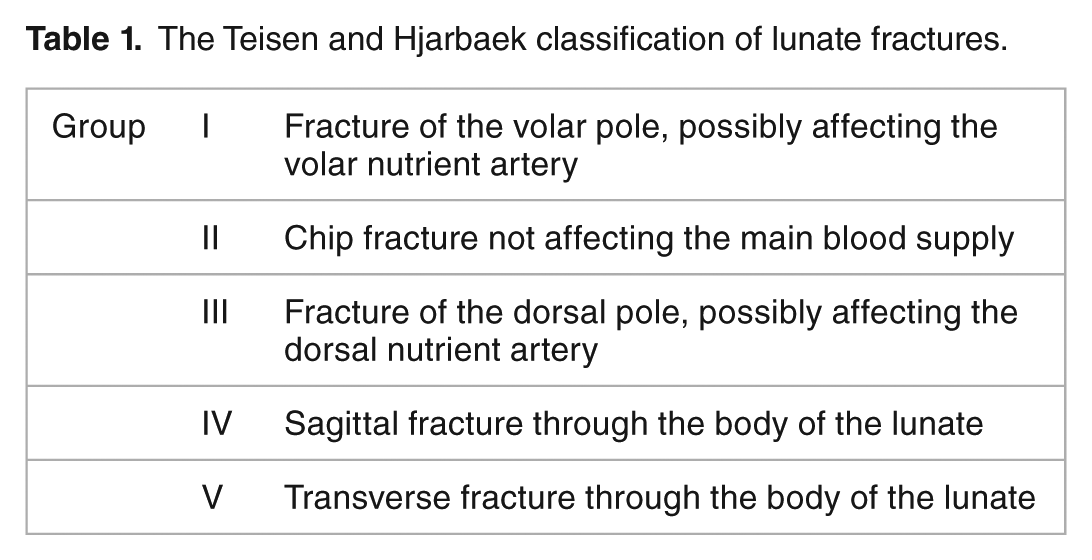
Isolated lunate fractures are rare as they are typically associated with other wrist injuries; however, there are concerns that the injury is being missed on diagnosis and computerized tomography (CT) or magnetic resonance imaging (MRI) may be needed for proper identification.11–13 They account for approximately 0.5% to 6.5% of carpal fractures.11–13 The most common mechanism of action is falling on an outstretched hand, but the injury may occur following hyperflexion or a direct blow. 13 Teisen and Hjarbaek categorized these fractures based on radiographs and vascularity, as described by Gelberman and Gross (Table 1).11,14,15
The Teisen and Hjarbaek classification of lunate fractures.
Treatment of scaphoid fractures
If the injury is deemed minimally displaced, cast or splint immobilization may be employed; however, fracture consolidation via this method ranges from 8 to 12 weeks, which may be too long for a younger, more active patient.8,9,16 Once union is achieved, hand therapy may begin. 9 Complications, including muscular atrophy, joint stiffness, and reduced grip strength, may occur and could delay the patient’s return to work and activities. 8
Different surgical fixation methods, screws, bone grafts, and approaches have been investigated in the literature.1,3,17 Bone grafting, typically from the radius, is done to enhance vascularity.1,10 Screw fixation provides structural support by compressing the 2 fragments and prevents bending at the fracture site; a single headless compression screw along the central longitudinal axis is the most common method of fixation.1,3,9,10 Designs have evolved since the original Herbert screw, claiming to improve load to failure, stiffness, and compression at the fracture site, though screw selection is currently based on the surgeon’s personal preference, as a better understanding of the different compressive forces and clinical effects generated by these various screw designs is still required.9,18 Kirschner wires (k-wires) are helpful for stabilizing the ligamentous forces acting on the area and involve minor soft tissue damage, but can lead to pin tract infection, stiffness, and the need for re-intervention.1,8 Volar plating may be indicated when there is a large degree of comminution or bone loss.9,10 Generally, internal fixation is associated with good union rates, ranging from 85% to 90%, while also providing earlier return to mobilization.8,18 Not only is vascular compromise an issue, but instability can also be the cause of complications, such as nonunion, post-injury; therefore, a combination of these different treatments may be needed to address all underlying issues in some of these patients. 1 In a biomechanical study, Guss et al 3 found that a 50% intact scaphoid with a headless compression screw provided similar load to failure and stiffness to a fully intact, uninjured scaphoid. There is inconsistent evidence on the use of k-wires alone, but in a case-control study of 25 patients with scaphoid nonunion, Allon et al 1 found that the addition of k-wires to headless screw fixation and bone grafting was safe and should be considered when suboptimal stability is present during surgery. When a nonunion occurs, salvage procedures include proximal row carpectomy, scaphoid excision with arthrodesis, or total wrist fusion; however, these operations can lead to permanent changes in wrist function. 10 For such cases, fixation with a headless compression screw, with or without bone grafting, is currently the standard when attempting to stabilize and unite the scaphoid.10,19 Metaphyseal decompression of the distal radius, along with the insertion of compression screws, is a more recently developed method that may increase vascularization of the radial column of the carpus for scaphoid nonunion. 17 The addition of a volar plate to screw fixation can provide more buttress support, if needed (Figure 1). 10

Overview and treatment of scaphoid and lunate fractures.
Treatment of lunate fractures
Conservative treatment includes prolonged immobilization with a plaster cast for at least 6 weeks, which may be reserved for undisplaced fractures.11,12,20
Displaced lunate injuries are treated via internal fixation with screws, and possibly k-wires, as it ensures good reduction and compression; however, this is not possible if the fracture is comminuted (Figure 1).11–13 This treatment method is also an alternative for patients who do not want to experience prolonged immobilization (ie, want a quicker return to work) when the injury is treated conservatively.11,12 If chronic instability or arthrosis develops, salvage procedures include proximal row carpectomy and wrist arthrodesis (Figure 1). 12
Background on femoral neck fractures
The number of hip fractures is rising due to the aging population, though such injuries can still occur in young adults.21–23 In a recent study conducted by Rosengren et al, 24 the authors reported that the number of people aged ⩾50 years rose from 1.6 to 2 million from 1980 to 2010 in Denmark and from 2.8 to 3.5 million from 1987 to 2011 in Sweden. During these same years, the number of annual hip fractures (per 10 000 person-years) generally increased in these countries, from ~7 in men and ~28 in women to ~14 and ~39, respectively, in Denmark and from ~23 to ~29 in Swedish men (incidence rates in Swedish women were similar between 1987 and 2010; ~75/10 000 person-years). 24
Femoral neck fractures, in particular, are challenging as they are at an increased risk of complications, such as fixation failure, malunion, nonunion, and avascular necrosis of the femoral head.23,25 They may occur due to either low- or high-energy trauma, or because of a sport injury, and can be classified using the Garden or Pauwels classification system (Tables 2 and 3).5,25–27 Femoral neck fractures are a leading cause of disability and morbidity in the elderly, and, in the United States, yearly incidence rates for this injury have ranged from 146 to 242 per 100 000 adults. 28 Displaced fractures, relative to nondisplaced, are associated with higher complication rates.5,29 For example, Campenfeldt et al 5 found rates of 23%, 15%, and 28% for nonunion, avascular necrosis, and reoperation, respectively, in patients with displaced fractures, whereas these rates for those with nondisplaced fractures were 0%, 12%, and 8%.
The Garden classification of femoral neck fractures.

The Pauwels classification of femoral neck fractures.

Treatment of femoral neck fractures
The aim of surgery is to reduce pain and allow for early mobilization. 21 It is believed that early fracture reduction and stabilization via surgery may improve femoral head blood flow, resulting in a greater likelihood of union and less complications; delayed treatment may also increase the risk of mortality.23,25,30–32 Although there is no definitive criteria as to what is considered an “unacceptable delay” for surgical intervention, guidelines suggest that surgery should be performed within 24 h of injury. 32 Surgical options for a femoral neck fracture include internal fixation or an arthroplasty procedure.5,21,22,28 A patient less than 70 years old should undergo internal fixation, regardless of the degree of displacement, which is hypothesized to preserve the hip joint while allowing the patient to function.5,21,23,25 Relative to nonoperative treatment, internal fixation lessens the risk of displacement and allows earlier weightbearing and rehabilitation. 33 Another reason internal fixation is recommended for patients <60 years is that they are at a higher risk of experiencing a revision with a total hip replacement due to their greater life expectancy. 5 The procedure can be done with screws, resulting in good functional outcomes for most patients.5,23,25 For example, 76% of patients in the study by Campenfeldt et al 5 achieved a “good” or “excellent” result on the Harris Hip Score 24 months post-surgery. There is variation in the size and number of screws, and their angle of insertion and placement, with no clear consensus on the best approach.23,25 Bone grafting may be done along with compression screw insertion to help improve vascularity in the region.23,33 Another method of internal fixation includes a sliding hip screw.25,33 After screw insertion, the sliding and compressing of fragments during loading are hypothesized to induce fracture healing while controlling the shear forces, but femoral neck shortening may occur. 25 The patient’s bone quality and the amount of fracture comminution are other factors to consider as they may contraindicate internal fixation.22,25,29 Arthroplasty is typically done for patients who are older (ie, ⩾60 years) and have displaced fractures, or when a patient experiences a failure with less invasive treatment.21,22,25,28 For older patients, arthroplasty promotes early mobilization and weightbearing, reducing the likelihood that the patient will remain bedridden and encounter subsequent comorbidities (Figure 2). 22

Overview and treatment of femoral neck fractures.
Background on talar fractures
Talar fractures account for about 0.1% to 0.3% of all fractures and 1% of foot and ankle fractures.4,7,34 The talus is the most superiorly located bone of the foot and is vital in maintaining ankle function and ROM. 6 Injuries are typically due to high-energy trauma, such as a motor vehicle collision or fall.7,34 Plain radiographs will be required for diagnosis, but a CT scan or MRI may be used to further characterize the fracture.7,35 Clinically, the patient will have pain and swelling at the ankle with the inability to bear weight. 7 Talar fractures may be missed on initial examination, being diagnosed as an ankle sprain. 36 Changes in gait will be observed and post-traumatic arthritis is another concern.7,34
The talus comprises a neck, head, body, lateral process, and posterior process; not all regions of the talus are vascularly compromised.6,7 Talar neck fractures are the most common type as this area is the weakest part of the bone, representing about half of these injuries.6,7 The severity of talar neck fractures can be classified using the methods described by Hawkins (Table 4). 37 Avascular necrosis, osteoarthritis, and worse clinical scores increase with fracture severity.6,7 Talar body fractures account for about 20% of all talar fractures. 7 The articular surfaces of the ankle and, occasionally, subtalar joints are generally involved, increasing the likelihood of developing osteoarthritis. 7
The Hawkins classification of talar neck fractures.

Treatment of talar fractures
A nondisplaced talar neck fracture with adequate alignment may be treated conservatively with immobilization in a lower leg cast for 6 weeks, allowing for partial weightbearing only.6,7,35,38 Rehabilitation may be started once the fracture is radiographically healed. 38
Type II to IV talar neck fractures require immediate internal fixation.6,7 Talar body fractures are almost always managed operatively; however, complications are still common as the blood supply becomes disrupted. 7 Screws may provide optimal compression except when there is extensive communition; in such cases, a plate may also be required or an excision may be performed, though the latter procedure can alter hindfoot stability and biomechanics.7,35 K-wires may help achieve closed reduction and temporary fixation prior to screw insertion. 39 If avascular necrosis develops, another procedure may be required, such as talectomy, pantalar arthrodesis, tibiotalar arthrodesis, or tibiocalcaneal arthrodesis (Figure 3). 7
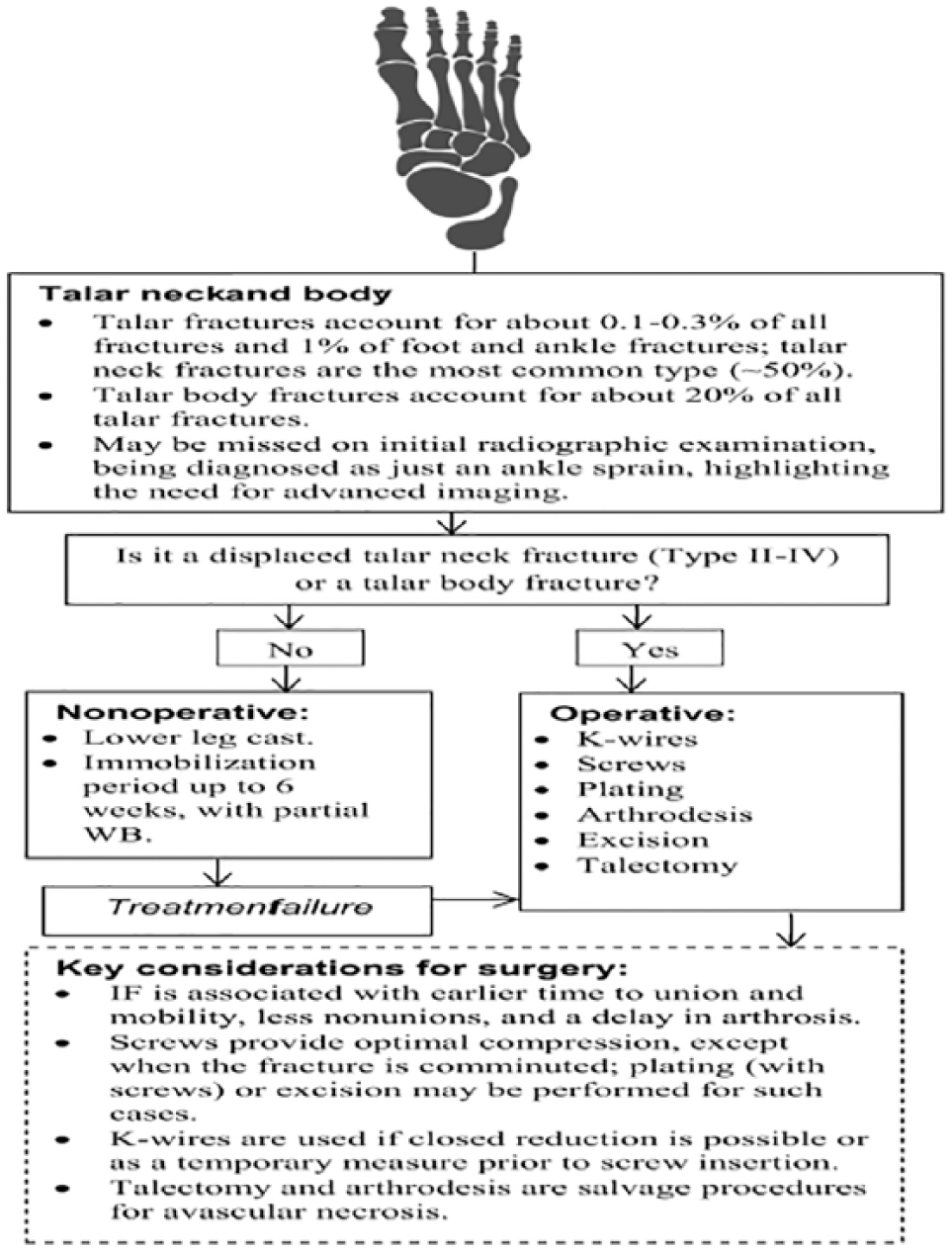
Overview and treatment of talar neck and body fractures.
Conclusions
Current evidence suggests that optimal treatment for vascular compromised fractures is dependent on the degree of fracture displacement and comminution, and the patient’s post-injury functional demands, age, and bone quality. Conservative efforts generally include casting or splinting with a period of immobilization. Surgery is indicated for substantially displaced fractures, patients who require higher functional demands and an earlier return to activity, or if complications occur following nonoperative treatment; however, operative intervention is typically performed for femoral neck fractures regardless of the amount of displacement. Internal fixation with screws is a common procedure among these injuries and can be used in combination with other implants, such as plating or k-wires, when needed. Severe fracture comminution, poor bone quality, or arthritis can contraindicate the use of screws and more invasive intervention will be required. Bone grafting is done in some cases to enhance vascularity. Salvage procedures exist for patients who develop severe complications, but these will permanently alter the anatomy of the injured area and should be considered a last resort.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: The preparation of the manuscript was funded, in part, by a research grant from Acumed. Christopher Vannabouathong is an employee of OrthoEvidence, Inc.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CV and MB contributed to the design of the study, and acquisition and interpretation of data. CV drafted the manuscript. MB, ES and BP reviewed and revised the manuscript prior to submission. All authors approved the final version of the manuscript.