
Abstract
Bohler angle and the crucial angle of Gissane are used on the evaluation of calcaneus fractures. However, few authors have described the variation of the angles when the calcaneus is growing. In this study, Bohler angle and the crucial angle of Gissane in paediatric population were measured using lateral foot radiographs of 429 patients, from 0 to 16 years of age. The control group was composed of 70 adult patients. The sample had a mean Bohler angle of 35.4° ± 5.9° and a mean crucial angle of Gissane of 110.5° ± 7.4°. The greater mean difference was identified for Bohler angle (8°) in the age group of 5 to 8 years (39.6° ± 5.7°) and for the crucial angle of Gissane (5°-6°) in the age group of 0 to 4 years (115.8° ± 7.3) (P < .05). The influence of the ossification centres on the geometry of the calcaneus across age groups makes Bohler angle and the crucial angle of Gissane higher in young children. The increase in Bohler angle points out the relative development of the posterior facet in young children and the importance of the reconstruction of the posterior facet height in the intra-articular calcaneus fractures.
Introduction
The calcaneus fractures in children are the most frequent in tarsal bones. The fracture incidence ranges between 0.05% and 0.15% and has a peak between 8 and 12 years of age. 1 The aetiology is similar to that of adults.
The extra-articular fractures have an increased incidence in children and the intra-articular fractures in adolescents. 2 The orthopaedic principles behind the treatment procedures of intra-articular fractures are the same as in adults.3,4,5 The subtalar joint congruence is achieved after the reconstruction of calcaneus angles-Bohler angle and the crucial angle of Gissane. Specially for bilateral fractures, it is important to recognize its normal range,6,7,8 to determine the degree of deformity, 9 to provide a perfect reduction, and to evaluate the clinical outcome 10 of displaced, intra-articular calcaneus fractures.
The prenatal and postnatal growth of the calcaneus has been studied in the past.11-18 The calcaneus is the only tarsal bone that presents two primary and a secondary ossification centres. The process of growth creates geometric variations in the calcaneus. A few studies have described the normal range of calcaneus angles in children and the variation across age groups.19-21
The purpose of this study was to characterize the normal range and the variation of Bohler angle and the crucial angle of Gissane according to the postnatal growth of the calcaneus.
Methods
The study was approved by the appropriate ethics committee in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Specific national laws were observed.
An observational and retrospective study was performed through Picture Archiving and Communication System (PACS) consultation at a health centre which is composed of two hospitals in the North of Portugal serving a population of more than 200 000 inhabitants. The local population is predominantly white.
Between 2014 and 2015, 429 patients, from 0 to 16 years of age, were submitted to lateral foot radiographs in outpatient consultation. We defined calcaneal fracture, previous local surgery, and inadequate imaging as exclusion criteria. A total of 70 adult patients, fulfilling the same criteria, were used as a control group.
Measurement
The patients’ age, sex, and laterality were recorded. Bohler angle and the crucial angle of Gissane were measured using an on-screen angle tool on PACS system. Bohler angle is defined by the intersection of two semi-lines at the highest point of the posterior facet, one starting at the highest point of the tuberosity and another at the highest point of the anterior process (Figure 1B). The crucial angle of Gissane is specified by the intersection of two semi-lines on calcaneus sulcus, one along the posterior facet and another starting on the anterior process (Figure 1A). All images were evaluated and the angles were measured twice by one junior orthopaedic surgeon. The mean of these two measurements was recorded. All measurements were within a 2° range, indicating acceptable intra-observer measure reliability.

Measurement technique for Bohler angle and the crucial angle of Gissane: (A) Bohler angle and (B) Crucial angle of Gissane.
Statistical analysis
The IBM SPSS Statistics for Windows Version 24.0 (IBM Corp., Armonk, NY) programme was used for statistical analysis. We defined an error margin of 0.05.
Patients were divided into four groups according to their age (Group A: 0-4 years, Group B: 5-8 years, Group C: 9-12 years, and Group D: 13-16 years). The sample and the control group were defined as Group S and Group E, respectively.
The normality of variables was assessed by graphic analysis and Shapiro-Wilk test. 22 Chi-square test was used to evaluate sex and laterality differences between age groups. The independent samples t-test was applied to compare Bohler angle and the crucial angle of Gissane between the sample and the control group.
The distribution of angles across age was estimated using curve-fitting regression analysis. For Bohler angle, a cubic function defined by y = c0 + a1(t) + a2(t2) + a3(t3) was identified. In this model, y represents the Bohler angle in degrees and t is the age in years. For the crucial angle of Gissane, no model was adequate.
A one-way between-groups analysis of variance was used to compare the angle difference between each group. T-testing with Tukey adjustments quantified the mean difference and percentage of variation between groups. With a large sample, even very small differences between groups can become statistically significant. This does not mean that these differences have any practical or theoretical significance. To evaluate this, the strength of relationship between the angles and the age groups was assessed by eta-squared (η2) which represents the proportion of variance of the angle that is explained by the age groups. Values of η2 can range from 0 to 1. Strength of η2 values was defined as small, moderate, and large.23,24
Results
Bohler angle and the crucial angle of Gissane were measured in 429 children. The sample was mainly composed of two groups: 9 to 12 years of age (39%) and 13 to 16 years of age (31%). In the sample group, the mean Bohler angle was 35.4° ± 5.9° (95% confidence interval [CI]: 23.6°-47.2°) and the mean crucial angle of Gissane was 110.5° ± 7.4° (95% CI: 95.7°-125.3°). The difference in the control group regarding Bohler angle (4°, 10%, P < .001) and the crucial angle of Gissane (2°, 2%, P = .016) was statistically significant. The distribution of sex (P = .716) and laterality (P = .211) by age groups was similar (Table 1).
Mean Bohler angle and the crucial angle of Gissane across different age groups.

Mean (SD).
There was a statistically significant difference in Bohler angle (F(3, 425) = 29.3, P < .001) and in the crucial angle of Gissane (F(3, 425) = 6.8, P < .001) for the four age groups (Graphs 1 and 2). The effect size was large (η2 = 0.17) for Bohler angle and small (η2 = 0.05) for the crucial angle of Gissane.

Distribution of Bohler angle (mean) across different age groups.

Distribution of crucial angle of Gissane (mean) across different age groups.
The distribution of Bohler angle across age follows a cubic function of y = 20.43 + 7.11t − 0.93t2 + 0.033t3 (F(3, 425) = 39.59, R2 = 0.21, P < .001) (Graph 3). Post hoc comparisons using the Tukey honestly significant difference (HSD) test indicated that the mean Bohler angle of Group B (39.7° ± 5.7°) was significantly different from those of Group A (33.6° ± 5.5°), Group C (35.1° ± 5.5°), Group D (33.0° ± 5.0°), and control group (31.7° ± 5.2°). Group C was significantly different from Group D and from the control group.

Regression analysis of distribution of Bohler angle across age.
Regarding the crucial angle of Gissane, Group A (115.8° ± 7.3°) was significantly different from Group B (111.1° ± 7.5°), Group C (109.8° ± 7.2°), and Group D (109.8° ± 7.1°). Only Group C and Group D were significantly different from the control group. There was no difference between the other age groups (Table 2).
Results of Tukey post hoc tests to analyse the differences between age groups.

Group A: ⩽4 years of age; Group B: 5-8 years of age; Group C: 9-12 years of age; Group D: 13-16 years of age; Group E: ⩾18 years of age; Group S: 0-16 years of age; % ([I – J]/I): percentage of variation between Group 1 (I) and Group 2 (J).
Independent samples t-test.
P ⩽ .05.
Discussion
Our study showed that the mean Bohler angle is higher and the crucial angle of Gissane is lower in paediatric age than in adults. The Bohler angle is more dependent of the age than the crucial angle of Gissane (17%) particularly in transition through 5 to 8 years of age.
Traditionally, calcaneal fractures in children were treated conservatively, but recent publications have drawn attention to the operative treatment of intra-articular fractures.3,4 Bohler angle and the crucial angle of Gissane have been used as a method of evaluation of intra-articular fractures of the calcaneus.25,26
In the study of Boyle et al, 19 the mean of the crucial angle of Gissane in paediatric age was 111° (90°-147°). There was a little angle variation with the exception from 0 to 2 years of age that showed a statistically significant increase in this value compared with other groups. The measurement is unreliable in young children 20 not providing usefulness of this evaluation.
Three studies had measured Bohler angle in paediatric age.19-21 The measurement had reliability. 20 The angle rounded 35° (14°-58°). They showed several statistically significant differences between smaller age groups, with interesting age-related variation through 6 to 8 years of age. The variation was justified by the postnatal growth of the foot.
In the first months of life, the primary ossification centre of the calcaneus is oval,16,18 making the subtalar joint flatter (Figure 2A). By 1 to 2 years of age, the primary ossification centre elongates and develops the proximal third and the subtalar joint. 16 The primary ossification centre is 62% ossified at 3 months after birth but continues until 7 years of age. 16
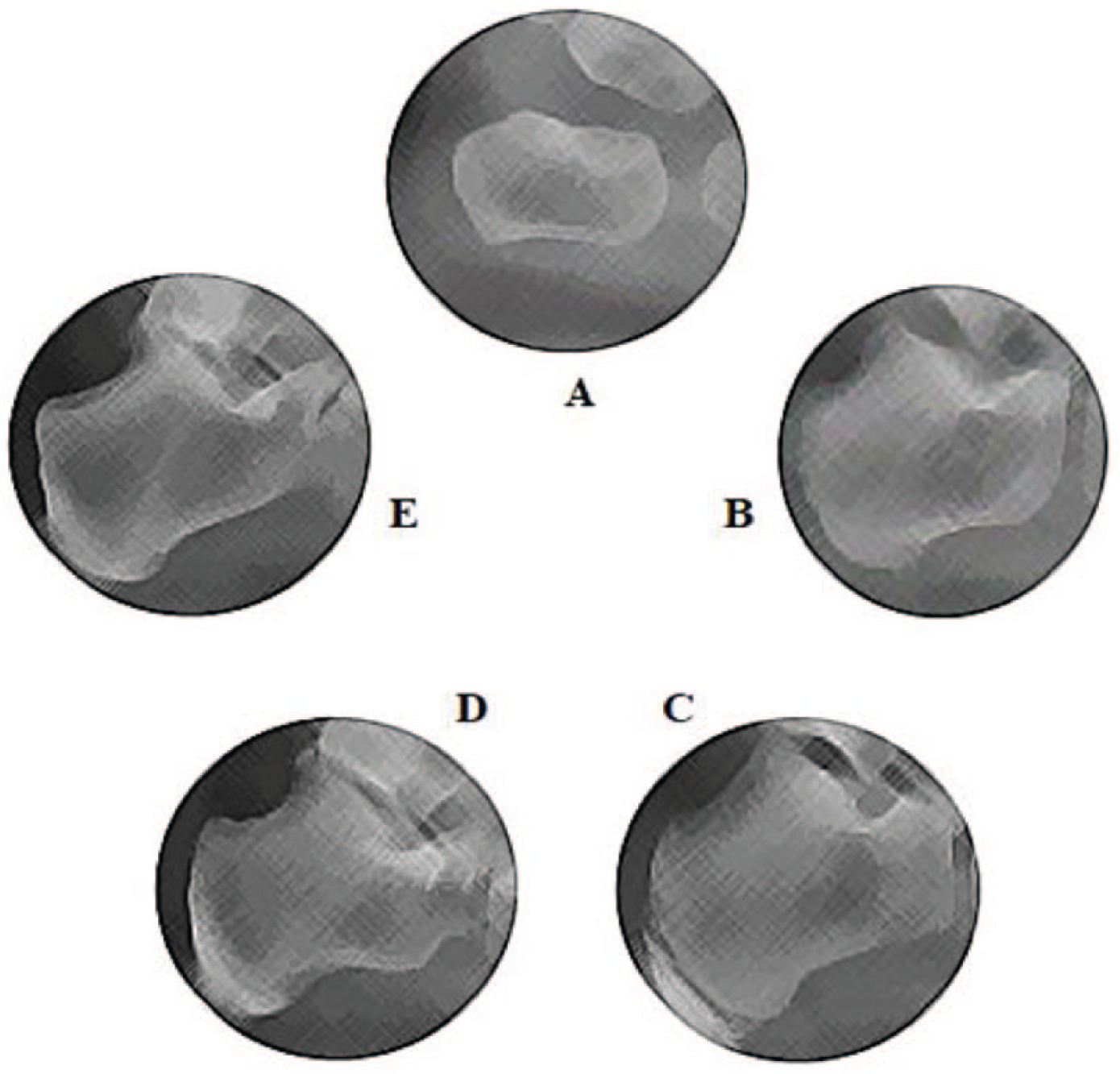
Growth of calcaneus across age groups: (A) ⩽4 years, (B) 5-8 years, (C) 9-12 years, (D) 13-16 years, and (E) ⩾18 years.
Between 5 and 7 years of age, one or more secondary ossification centres appear and initiate the development of the calcaneus apophysis.16,18 They are initially located at the lower third of the calcaneus (Figure 2B). Then they coalesce and elongate proximally and distally, forming a cap-like structure that surrounds the posterior margin of the primary ossification centre (Figure 2C). The ossification process of the posterior apophysis initiates in the middle of the ossification centre and ends on the superior and inferior extremities by the age of 14 to 18 years16,18 (Figure 2D and E).
In this study, the initial negative age-related variation of the crucial angle of Gissane in younger children is similar to other descriptions. 19 As we can see in Figure 2A and B, the development of subtalar joint makes the angle to decrease in measure. This is particularly notable in the first 8 years of age. After this period, the calcaneus apophysis develops, which has little impact on the subtalar joint and consequently on the angle.
The cubic distribution of Bohler angle is here described for the first time. We hypothesize that the initial increase, observed in Graph 3, is justified by the asymmetric development of the posterior facet (Figure 2B). When we compare Group B and the control group, the mean difference reaches a value of 8° (20%) suggesting that in children with displaced, intra-articular calcaneus fractures, between 5 and 8 years of age, the surgeon should be alert of its upper relative position to reconstruct the posterior facet. Also, particular care should be taken to put the least possible number of screws in the tuberosity, until 7 years of age, to preserve the primary ossification centre that is incompletely ossified 16 and the secondary ossification centres that appear. 18
Our study had some limitations. First, the retrospective analysis of a sample mainly composed by white people may not represent the population of all children and can decrease the external validity of the conclusions. Second, the measurement by only one rater could bias the study. However, as the reliability of Bohler angle was accomplished in other studies, 20 the impact on the conclusions is residual. In addition, the wide CI for Bohler angle can create challenges in clinical prediction. It is conceivable that a large sample or the development of a multiple regression model may increase the strength of the conclusions.
Conclusions
The higher relative position of the posterior facet of the calcaneus makes Bohler angle higher in children from 5 to 8 years of age and should make the surgeon take particular care in the reconstruction of the congruence of the subtalar joint.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Conception or design of the work, acquisition, analysis, and statistical interpretation of data: BP and ACF; Revision of the work for important intellectual content: LC.