
Abstract
Introduction
Electronic cigarettes (e-cigarettes), also known as “vapes,” are battery-powered devices that heat a liquid to produce an aerosol, commonly referred to as “vapor.” E-cigarettes were first marketed in 2004 as a tool that deliver a noncombustible nicotine to help people who smoke cigarettes to quit, while minimizing the nicotine withdrawal symptoms 1 In recent years, e-cigarettes increased in popularity among youth,2,3 young adults 4 and adults4,5 including individuals who are pregnant. 6 This rising trend has been associated with perceptions of reduced harm compared to conventional cigarettes,6,7 convenience of use, and the appealing appearance and flavors.1,7
Currently, there is no conclusive evidence supporting the safety of e-cigarette use during pregnancy. Although some studies suggest e-cigarettes may be less harmful than cigarettes during pregnancy 6 or a potentially safe cessation aid, 8 a growing body of research indicates otherwise.9,10 At least, e-cigarettes contain nicotine, which is a substance recognized for its addictive properties and known to adversely affect fetal development. Evidence links prenatal e-cigarettes to negative neonatal outcomes such as low birthweight,11,12 small-for-gestational-age, and preterm birth. 11 Maternal health risks have also been documented, including inadequate prenatal care, reduced breastfeeding rates, 11 and an elevated likelihood of dual use of cigarettes and e-cigarettes among pregnant individuals.13,14 These findings pose significant concerns for individuals who are pregnant and for the developing fetus, underscoring the need for a precautionary approach to e-cigarette use in this population.
Romania has implemented several tobacco control measures, such as banning cigarette smoking in public places, placing health warnings on tobacco packaging, and restricting tobacco advertising. 15 However, tobacco use remains a significant public health issue, especially among people of reproductive age. 16 Based on national data, current tobacco use was reported by nearly 30% of individuals aged 15 and above, with the highest rates found among individuals aged 15-39 (peak reproductive age). 16 Although cigarette smoking is the most common form of tobacco use in Romania, recent evidence indicates an increasing trend in e-cigarette use among individuals of reproductive age. 16 Targeted public health interventions are needed to address all forms of tobacco use, including e-cigarettes among individuals who are pregnant, or planning to be pregnant.
Most of the research on e-cigarette use during pregnancy has been conducted in the United States.6,13,17-19 To our knowledge, no studies have examined the prevalence of e-cigarette use and its associated factors among pregnant individuals who currently or formerly smoked cigarettes in Romania. This study aimed to fill that gap by examining the prevalence of e-cigarette and its associated factors in a sample of pregnant individuals who currently or formerly smoked cigarettes in Romania. These findings provide important baseline information on e-cigarette use during pregnancy in Romania and highlight the urgent need for educational interventions to raise awareness about its potential harms.
Methods
Participants
This study reports on a secondary data analysis of the cross-sectional data collected from two convenience samples of pregnant individuals who currently or formerly smoked cigarettes in the quantitative formative research phase (n = 155; May 2016-Jan 2017) and baseline phase (n = 161, June 2017-May 2019) of a randomized controlled trial (RCT) implemented in Romania. 20 The planned sample size was driven by practical considerations, including research funds availability and participants’ flow. The total sample size (n = 316) though deemed reasonable to evaluate feasibility and effect size for a future larger and more adequately powered study.
Individuals were recruited by trained research assistants from the waiting areas of two State-owned obstetrics and gynecology clinics and by general practitioners (GP) from the waiting areas of two GP offices in Cluj-Napoca, Romania. Individuals were eligible to participate if they were eighteen or older, pregnant, currently or formerly smoking cigarettes, and if they reported having a stable life partner. Individuals were considered to have formerly smoked cigarettes if they reported quitting up to 6 months before becoming pregnant, in preparation for their pregnancy, or any time during pregnancy. Participation was voluntary, all participants provided written informed consent, and the Michigan State University Institutional Review Board approved the study (IRB# 14-910).
Data Collection
The data collection process is described elsewhere.20-22 Briefly, individuals either filled out a paper-and-pencil version of the study survey in the waiting rooms of the clinics and GP offices (quantitative formative research phase) or an online version of the same questionnaire through a dedicated project website (RCT baseline phase).
The questionnaire composed of 6 sections: socio-demographics, reproductive and medical history, cigarette smoking and alcohol consumption, relationship with the partner, and emotional health. The questionnaire items were developed based on literature and expert input and the instrument itself was not previously validated. For this study, we used data from the first 4 sections only including the information about ever and current use of e-cigarettes and the perception of harm associated with their use.
Measures
The main outcomes of the study were ever and current use of e-cigarettes. Ever use was assessed by asking whether the participant had ever used e-cigarettes, with responses being recorded as binary (yes/no). Current e-cigarette use was derived from the participants’ self-reported frequency of use that was assessed by asking “How often, if at all, do you use e-cigarettes since you found out about the pregnancy?” with original ordinal responses “none, daily, less than daily but weekly, or monthly”. Current use was then created by recoding those responses, where “none” indicates non-current use and was coded as “0” and the other responses indicate “current use” and were all coded as “1.” The original frequency categories were retained and reported in the descriptive analyses to provide more insight about current e-cigarette use patterns.
Independent variables were: (1) using e-cigarettes with an intention to quit cigarette smoking during pregnancy, measured as binary (Yes/No); (2) the perceived harm reduction of using e-cigarettes as opposed to conventional cigarettes, assessed using a 4-point Likert scale numbered from 1 to 4, with the highest being “totally disagree” and asking individuals to rate their level of agreement with the statement “Electronic cigarettes are less harmful than cigarettes”; (3) change in cigarette smoking behavior due to pregnancy, measured by asking the participant to report whether she is smoking cigarettes from time to time, less, the same, more, or quit since finding out about the pregnancy; (4) the partner’s cigarette smoking status measured as binary; (5) the number of previous quitting attempts measured by asking a “how many times have you tried to quit smoking?”, with responses being recoded as binary where “1” indicates reporting any quitting attempt and “0” indicates reporting never attempted to quit cigarette smoking; (6) level of tobacco dependence, measured using Heaviness of Smoking Index score 23 ; (7) anxiety and depression measured by Patient Health Questionnaire for Depression and Anxiety [PHQ_4] 24 and (8) presence of any chronic health conditions in individuals that was measured using 9 questions with binary responses (Yes = 1, 0 = No) about asthma, hypertension, anemia, obesity, thrombophilia, Lupus, epilepsy, cancer, or any other disease. A new binary variable was created namely “morbidity,” and the responses were coded as “1” if at least one morbid condition was reported and “0” if none.
Other factors included age (calculated by subtracting the date of birth from the date of the survey), socioeconomic indicators such as education, employment status, and income as multinomial. Participants were asked to select their total monthly household income from one of the following categories: 0-1500 RON; 1501-3000 RON; 3001-5000 RON; and >5000 RON. For context, Romania’s average net monthly wage (take-home pay) ranged from approximately 2114 RON in 2016 to 2957 RON in 2019. 25
Statistical Analysis
Summary measures were frequencies and proportions for categorical variables and mean and standard deviation for continuous variables. Only valid percentages were reported. Missing data for most variables ranged from 0 to 5%, except for moderate to severe anxiety and depression [PHQ-4] (18.0%), perception of e-cigarette harm (13.3%), and nicotine dependence (6.3%), and ever using e-cigarettes (6.3%). Of the 122 participants who ever used e-cigarettes, only 2 (1.6%) did not report their current e-cigarette use status (Appendix 1).
Dummy variables were created for multinomial variables as needed. Ever and current use of e-cigarettes were reported separately. Specifically, 122 (41.2%) participants reported ever using e-cigarettes, and 42 out of them reported current use. Due to the small number of individuals who reported current e-cigarettes use (n = 42), only bivariable analysis was used to examine the factors that are likely associated with current e-cigarette use during pregnancy. We have considered alternative methods such as Firth’s penalized logistic regression. 26 Which can reduce small-sample bias. However, given the exploratory aim of the study, the limited number of events, and the study’s focus on descriptive and bivariate associations, we did not pursue this approach.
Multivariable Logistic Regression was used to identify the factors that were associated with ever using e-cigarettes. Variables with a P-value ≤0.20 in the bivariable analyses were included in the multivariable model to avoid excluding potentially important variables (effect modifiers) that may become significant in the adjusted model. 27 Multicollinearity was assessed using Variance Inflation Factor (VIF) values calculated from a linear regression model using the same independent variables as in the logistic regression and age as a continuous dependent variable. VIF values were all below 2.5 (1.1-1.8), suggesting no evidence of problematic multicollinearity. 28 All analyses were conducted using Statistical Package for Social Sciences (SPSS) version 26.0. Significance was set to P < 0.05.
Results
Sociodemographic Findings
The sample included 316 pregnant individuals, 235 (74.4%) currently and 81 (25.6%) formerly smoked cigarettes. Their age ranged between 18 and 46 years old (Mean = 28.4, SD = 5.7), 59.1% had a level of education less than bachelor, 52.2% worked in or outside home, 63.3% had a monthly income less than 3001 RON (1 Romanian Leu [RON] =$0.22), and 96.1 % were married or currently living with their partners.
E-Cigarettes Use
A total of 122 (41.2%) participants have used e-cigarettes and 42 (13.3%) were currently using e-cigarettes, out of which 17 (40.5%) used them more than once a week and 9 (21.4%) used them daily. Attempt to quit cigarettes was reported by 249 (84.4%) individuals, of which 100 (40.2%) ever used e-cigarettes and 35 (14.1%) used e-cigarettes at their last cigarettes’ quitting attempt. Among pregnant individuals who reported current e-cigarette use, 23 (54.8%) reported using them with the intention of helping them to quit cigarettes during pregnancy. E-cigarettes were perceived as not less harmful than conventional cigarettes by 136 (49.6%) of the whole sample, by 54 (45.8%) of the individuals who ever used e-cigarettes and by 13 (31.0%) of those who were currently using them.
Description of the Study Sample by Potentially Associated Factors and the Reported History of Ever Using e-Cigarette

Note: Discrepancies between the overall total and the category-specific totals are due to missing data. Only valid column percentages were reported.
aReporting at least one of the following (Asthma, diabetes, hypertension, thrombophilia, obesity, anemia, lupus, epilepsy, cancer, or any health condition).
bPatient Health Questionnaire for Depression and Anxiety. 21
cCalculated using heaviness of smoking index score. 19
Unadjusted Analyses of Potential Factors of Ever Versus Never e-Cigarettes Use Among a Sample of Pregnant Individuals Who Currently or Formerly Smoked Cigarettes From Romania

aReporting at least one of the following (Asthma, diabetes, hypertension, thrombophilia, obesity, anemia, lupus, epilepsy, cancer, or any health condition).
bPatient Health Questionnaire for Depression and Anxiety. 21
cCalculated using heaviness of smoking index score. 19
Adjusted Factors Associated With Ever Using e-Cigarettes Among a Sample of Pregnant Individuals Who Currently or Formerly Smoked Cigarettes From Romania
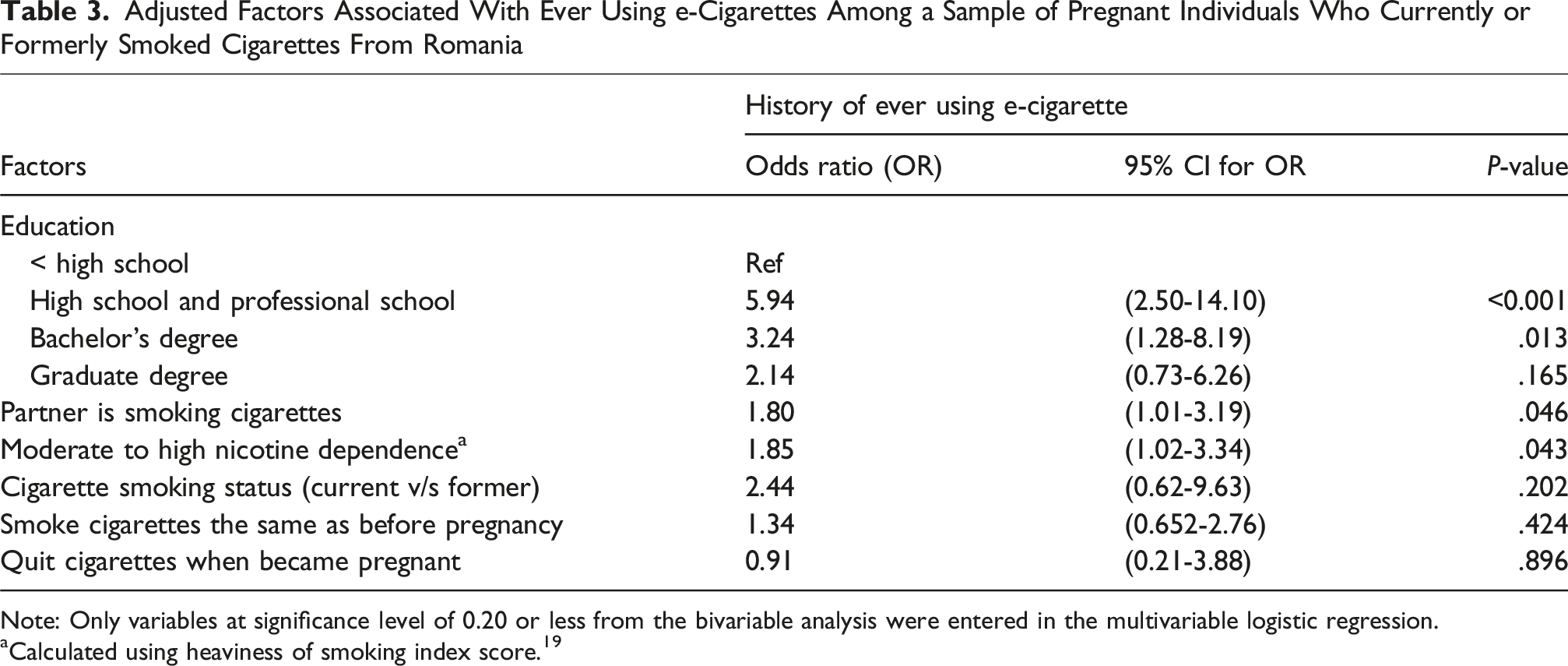
Note: Only variables at significance level of 0.20 or less from the bivariable analysis were entered in the multivariable logistic regression.
aCalculated using heaviness of smoking index score. 19
Nearly one third of the individuals who ever used e-cigarettes have reported currently using e-cigarettes. Bivariable analysis showed differences in the perceived reduced harm of the e-cigarettes compared to cigarettes between individuals who did and who did not report current e-cigarettes use. Compared to non-current users, a higher proportion of current users have totally or partially agreed that e-cigarettes are less harmful than cigarettes. In addition, a higher proportion of individuals who reported current e-cigarette use have used e-cigarettes in their last attempt to quit smoking than those who reported non-current use.
Unadjusted Difference Between Former and Current e-Cigarettes Users by Potential Factors in a Sample of Pregnant Individuals Who Ever Used e-Cigarettes From Romania (n = 122)

Note: Discrepancies between the overall total and the category-specific totals are due to missing data. Only Valid percentages were reported.
Significant difference in column proportions using z-test P < 0.05 and continuous measures difference using independent t-test (*P < 0.05, **P < 0.01).
aReporting at least one of the following (Asthma, diabetes, hypertension, thrombophilia, obesity, anemia, lupus, epilepsy, cancer, or any health condition).
bPatient Health Questionnaire for Depression and Anxiety 21 .
cCalculated using heaviness of smoking index score 19 .
Discussion
This study examined the prevalence and predictors of ever and current e-cigarette use among pregnant individuals from Romania who currently or formerly smoked cigarettes. Our results showed that 41.2% of the study participants had ever used e-cigarettes, and up to 13.3% were using them during pregnancy. The prevalence of moderate to high nicotine dependence was higher in pregnant individuals who ever experimented with e-cigarettes than those who never experimented with them. A higher percentage of individuals who had ever used e-cigarettes had completed intermediate education (High school to Bachelor) compared to non-users. Additionally, more than half of the individuals who had reported current e-cigarette use had used them in their most recent attempt to quit cigarettes. Our results also showed that e-cigarettes were perceived as less harmful than regular cigarettes among individuals who reported current e-cigarette use. Moreover, receiving tobacco quit advice was negatively associated with current e-cigarette use in the unadjusted model. Finally, individuals with a partner who smoked cigarettes had higher odds of reporting current e-cigarette use than those with a partner who did not smoke cigarettes.
The use of e-cigarettes has increased worldwide in the past years and evidence suggests that its use during pregnancy might also continue to increase, 6 especially that previous research suggests that some pregnant individuals turn to e-cigarettes with the intention to help them quit cigarette smoking. 29 In line with prior research, our findings showed that nearly half of the individuals who had reported current e-cigarette use had also reported using e-cigarettes in their most recent attempt to quit cigarette smoking, suggesting continued exposure to nicotine, which may also explain the higher prevalence of “moderate to high nicotine dependence” in pregnant individuals who ever used e-cigarettes than those who never used them. This difference can be interpreted by dual use of e-cigarettes and conventional cigarettes, 30 compensatory overuse of e-cigarettes to manage cravings, 31 or constantly holding the device throughout the day, which may increase the frequency of its use. 32
Given that e-cigarette use has the potential to increase nicotine exposure and dependence, there is a growing demand to raise the level of awareness regarding the safety of e-cigarettes use during pregnancy. 33 E-cigarettes might be at least as harmful as traditional cigarettes because they increase nicotine intake during pregnancy, 9 and nicotine exposure alone, regardless of delivery method, has been shown to be associated with serious fetal development consequences. 34 In this context, abstinence from nicotine during pregnancy is highly recommended.
Few countries, such as the United Kingdom, have recommended regulated electronic cigarettes only for pregnant individuals who find it difficult to quit cigarettes using other methods. 35 This position reflects a harm-reduction approach based on the belief that, for adult smokers who cannot quit, switching to e-cigarettes may be less harmful than continuing to smoke combustible cigarettes. 36 However, this remains a nuanced and evolving area of public health policy, and recommendations may differ depending on the interpretation of emerging evidence and regulatory perspectives.
One of the main findings of this study is the observed relationship between education and ever using e-cigarettes. The highest percentage of e-cigarette use was among pregnant individuals who had intermediate educational attainment (high school to bachelor’s degree). This is consistent with prior studies suggesting that individuals who use e-cigarettes are more likely to report more than a high school education. 37 While higher education is often associated with higher awareness, individuals with intermediate education levels may be susceptible to contradicted messages about e-cigarettes. This trend may interpret the growing popularity of e-cigarettes among older youth and young adults.8,38 Other studies suggest that perceptions of e-cigarette safety that are common among pregnant individuals18,30 may be more prevalent in those with intermediate education than in those with either lower or higher educational attainment. 21 This suggests that individuals may be more likely to experiment with e-cigarettes if they believe they are safer than conventional cigarettes. In addition, prior research has shown that perceptions of reduced harm are key drivers of e-cigarette uptake, particularly among dual users.6,12,13 Dual use during pregnancy is a public health concern because it increases nicotine exposure and the subsequent adverse maternal and neonatal outcomes.11,12
Within this context, provider influence becomes highly relevant. Healthcare professionals play a critical role in shaping tobacco-related behaviors during pregnancy.21,39-41 Among this sample of pregnant individuals, unadjusted bivariable analysis showed that receiving advice to quit smoking tobacco from a healthcare professional was not associated with ever using e-cigarettes but was negatively associated with current e-cigarette use. Continued e-cigarette use during pregnancy was less common among those who received cessation guidance related to tobacco from a healthcare provider. This finding suggests that provider guidance may be more effective in discouraging continued use rather than initial experimentation, potentially due to missed opportunities to counsel specifically on e-cigarette risks, 15 or due to a contradicting messaging around their use. For example, earlier studies indicated that some physicians recommended e-cigarettes as a smoking cessation aid.40,41 However, this guidance may not reflect current clinical practice given the accumulating evidence linking e-cigarette use with adverse maternal and neonatal outcomes. 11 We would like to note that this study did not include information on whether participants have received advice specifically related to e-cigarette use.
Another noteworthy finding of this study is that pregnant individuals with a partner who smokes cigarettes have higher odds of being current e-cigarettes users than those with a partner who doesn’t smoke cigarettes. Based on previous research, pregnant individuals who smoke cigarettes are less likely to quit cigarettes during pregnancy when their partners continue to smoke cigarettes. 42 This can be interpreted by the perceived partner’s support and understanding relationship that has shown to be associated with cigarette smoking cessation during pregnancy.42,43
One of the interesting findings in this study is the interaction that was observed between partner smoking, current cigarette smoking, and smoking cigarettes during the same as before pregnancy. These variables emerged as positive effect modifiers for the relationship between ever using e-cigarette and the intermediate educational attainment (high school to bachelor’s degree). After adding those variables, the odds of reporting a high school education increased from 3.68 in the unadjusted model (P = .001) to 5.94 in the multivariable model (P = <.001), and the odds of reporting a bachelor’s degree increased from 1.89 (P = .126) to 3.24 and became significant (P = .013) among individuals who ever used e-cigarettes compared to those who never used them. Our findings emphasize the need for consistent public health messaging and tailored perinatal educational interventions to raise awareness about the risks associated with cigarette and e-cigarette use during pregnancy. These interventions should target pregnant individuals and their partners, with a particular focus on reaching high school and college students.
Our study provides an important opportunity to fill in the gap in research on using e-cigarettes during pregnancy in Eastern European Countries. It is the first to report the predictors of using e-cigarettes in a sample of Eastern European (Romanian) pregnant individuals who currently or formerly smoked cigarettes. However, this study has several limitations. First, the study used a convenience sample, which limits the generalizability of the findings. This approach may also introduce sampling bias, as participants who attend prenatal visits at participating sites may differ systematically from those who do not. Second, the original study was a pilot randomized controlled trial, and sample size decisions were driven by feasibility, resource availability, and projected participant flow. Still, our sample size (n = 316) exceeded the estimated minimum required sample size (n = 195), which was calculated to allow for adequate precision in estimating the prevalence of smoking among pregnant individuals in Romania, assuming a national prevalence of 15%.44,45 While this study was not powered for hypothesis testing of intervention effects, the larger sample size strengthens descriptive and exploratory findings, enhances the precision of prevalence estimates and the reliability of the subgroup analyses. Third, although the baseline questionnaire items were based on prior literature and expert input, they were not previously validated in this population, which may limit the instrument’s construct validity and measurements’ reliability. Fourth, this study relied on self-reported data that is prone to recall bias and social desirability bias, which may lead to underreporting, particularly for sensitive behaviors such as tobacco use including e-cigarette.46-48 These factors should be considered when interpreting the findings. Fifth, we did not perform multivariable analysis for current e-cigarette use due to the small sample size in that subgroup. However, the bivariable analysis satisfies the exploratory purpose of this study. Finally, the cross-sectional design of the study limits our ability to draw causal conclusions regarding factors associated with e-cigarette use.
Conclusions
More than half of this sample of pregnant individuals who currently or formerly smoked cigarettes had ever used e-cigarettes, with a notable proportion reporting current use. A higher percentage of current users had used e-cigarettes in their recent attempts to quit cigarette smoking during pregnancy and became dual users. Individuals who ever used e-cigarettes had a higher nicotine dependence score than those who never used it. Ever use was more common among women with education beyond high school, and these women also reported higher nicotine dependence scores. Perceptions of reduced harm were more prevalent among current users. Finally, having a partner who smokes was associated with higher odds of current e-cigarette use. These findings highlight the need for targeted educational and clinical strategies to reduce e-cigarette use and nicotine exposure during pregnancy. Prenatal care providers should consistently screen for e-cigarette use, offer evidence-based cessation counseling, and correct misconceptions about the safety of e-cigarettes during pregnancy. Public health messaging should also address social influences, such as partner smoking, and address the risks of dual use. Incorporating these strategies into prenatal care processes could help alleviate nicotine-related harms to both pregnant individuals and their infants.
Supplemental Material
Supplemental Material - E-Cigarette Use and Its Associated Factors Among Pregnant Individuals Who Currently or Formerly Smoked Cigarettes From Romania
Supplemental Material for E-Cigarette Use and Its Associated Factors Among Pregnant Individuals Who Currently or Formerly Smoked Cigarettes From Romania by Rana Jaber, Oana M. Blaga, Marina D. Dascăl, Cristian I. Meghea in Tobacco Use Insights
Footnotes
Ethical Considerations
Michigan State University Institutional Review Board approved the study.
Consent to Participate
Participation was voluntary, all participants provided written informed consent
Author Contributions
R.J and C.M conceived and designed the study. R.J analyzed the data and produced the first draft of the manuscript. O.B and M.D collected the data and participated in writing the discussion section. C.M secured fund, planned methods, made general supervision and reviewed and edited the final version. All authors approve the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center of the National Institutes of Health under Award Numbers K01TW009654, R21HD103039, R33HD103039 to CI Meghea.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Clinical Trial Registration
NCT02512913
Contributorship
Rana Jaber: Conceptualizing, Formal analysis, Writing – review & editing. Cristian Meghea: Funding acquisition, Conceptualization, Supervision, Project administration, Methodology, Writing – review & editing. Oana Blaga: Writing – review & editing, and Methodology. Marina Dascal: Writing – review & editing, and Methodology
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available because it is institutional private data, but the deidentified data can be available from the corresponding author on a reasonable request
Supplemental Material
Supplemental material for this article is available online.
Appendix
Missing Data for the Key Variables (N = 316)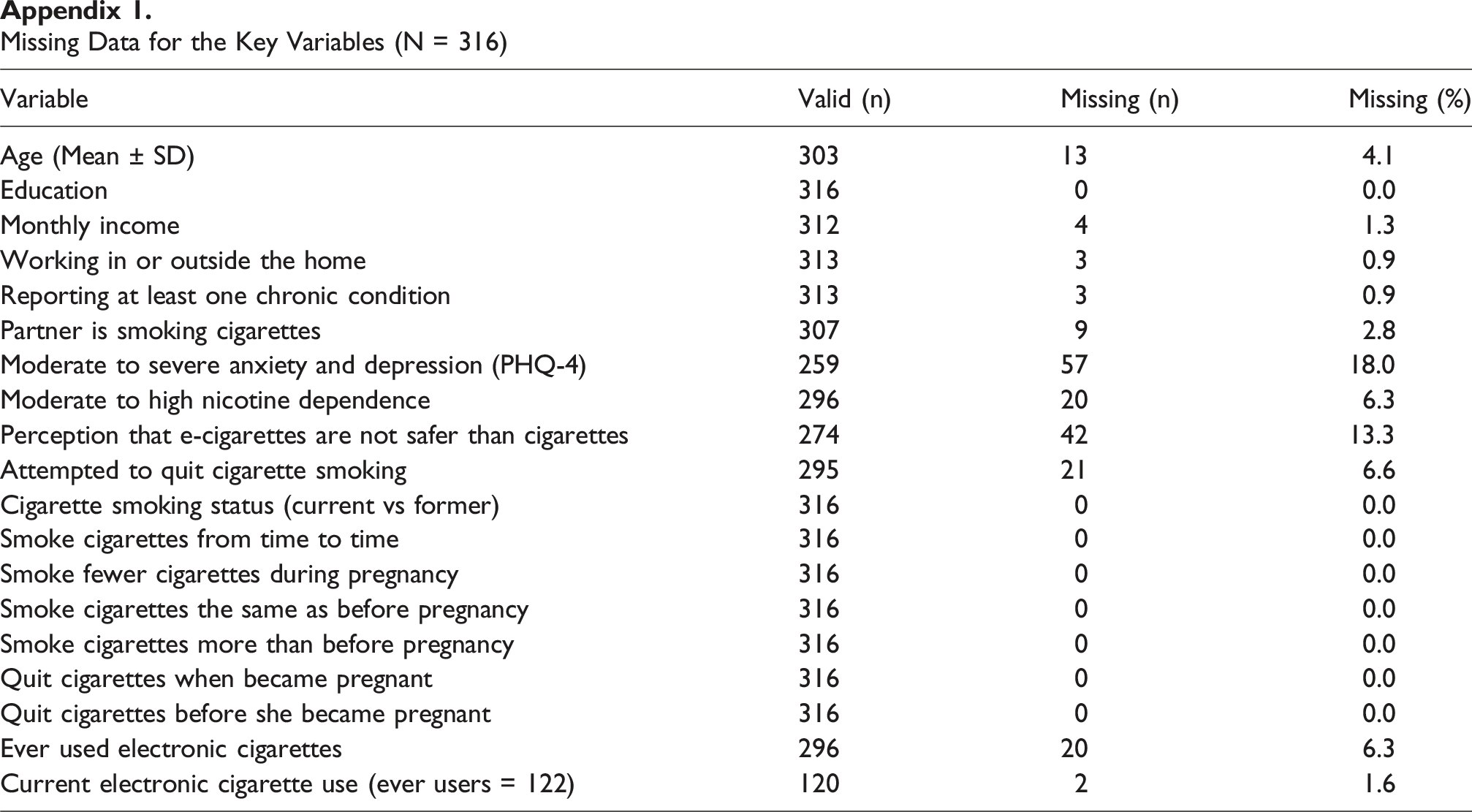
Variable
Valid (n)
Missing (n)
Missing (%)
Age (Mean ± SD)
303
13
4.1
Education
316
0
0.0
Monthly income
312
4
1.3
Working in or outside the home
313
3
0.9
Reporting at least one chronic condition
313
3
0.9
Partner is smoking cigarettes
307
9
2.8
Moderate to severe anxiety and depression (PHQ-4)
259
57
18.0
Moderate to high nicotine dependence
296
20
6.3
Perception that e-cigarettes are not safer than cigarettes
274
42
13.3
Attempted to quit cigarette smoking
295
21
6.6
Cigarette smoking status (current vs former)
316
0
0.0
Smoke cigarettes from time to time
316
0
0.0
Smoke fewer cigarettes during pregnancy
316
0
0.0
Smoke cigarettes the same as before pregnancy
316
0
0.0
Smoke cigarettes more than before pregnancy
316
0
0.0
Quit cigarettes when became pregnant
316
0
0.0
Quit cigarettes before she became pregnant
316
0
0.0
Ever used electronic cigarettes
296
20
6.3
Current electronic cigarette use (ever users = 122)
120
2
1.6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.