
Abstract
Introduction
E-cigarettes and heated tobacco products (HTPs) are gaining worldwide significance. The tobacco industry is promoting these products as healthier alternatives to conventional cigarettes.
Methods
In this four-arm crossover study, we examined the acute effects of cigarette smoking, vaping IQOS, or vaping e-cigarettes (with or without nicotine) on hemodynamics, arterial stiffness, and small airways. Twenty subjects (10 male, 10 female), all occasional smokers, completed each study arm. There was at least a 48 h washout period before each test day. Arterial stiffness and peripheral and central hemodynamics were assessed using Mobil-O-Graph™ (I.E.M., Germany), whereas tremoFlo® c-100 (Thoracic Medical Systems Inc) was used to evaluate the effects on the small airways and resistance.
Results
Cigarettes, IQOS, e-cigarettes containing nicotine, and nicotine-free e-cigarettes had similar effects on peripheral and central hemodynamics as well as on arterial stiffness. We observed a significant increase in all parameters. However, only nicotine-containing products lead to increased bronchial obstruction, higher reactance, and a higher tidal volume.
Conclusion
Therefore, we concluded that cigarettes, IQOS, and e-cigarettes have similar effects on hemodynamics. No differences were observed between the nicotine-containing and nicotine-free e-cigarettes. All nicotine-containing products also influence small airways. These findings suggest that e-cigarettes and HTPs are not healthier alternatives than conventional cigarettes.
Keywords
Introduction
Tobacco smoking continues to be very popular with about 1.3 billion tobacco users worldwide in 2020, and is still the most common cause of preventable diseases worldwide.1,2 In Germany, it causes every fifth tumor in men and every 12th in women. 3
The tobacco industry has introduced new forms of nicotine intake such as electronic cigarettes and the more recently launched heated tobacco products (HTPs), for instance “IQOS.” Compared to combustible cigarettes, new devices no longer burn tobacco for nicotine extraction and are therefore widely advertised by the tobacco industry as a less harmful method of nicotine consumption.4–7
While the prevalence of tobacco smoking has decreased continuously over the last decade, the use of alternative tobacco products has increased worldwide, with e-cigarettes and HTPs taking on greater significance.8–10 Interestingly, there has been an increase in the incidence of tobacco smoking in Germany since 2021. 11 The reasons for this development remain unclear. However, individual patients state that their smoking habits are due to the mental pressure caused by the war and the coronavirus pandemic.
The extent to which e-cigarettes and HTPs can provide a less harmful alternative to conventional cigarettes has been widely discussed in academic research and general media.
E-cigarettes produce aerosols by vaporizing a liquid consisting of a solvent and other variable substances such as nicotine or flavors. The composition of the aerosol and nicotine delivery is not only dependent on the constituents in the liquid, but is also influenced by the power of the device and individual user behavior, such as puff topography.12,13
HTPs heat a special tobacco composition, releasing nicotine into the inhalable steam. 14 Although the first studies on HTPs showed lower levels of carcinogenic and toxic substances than combustible cigarettes, IQOS aerosols contain significantly higher levels of other substances. The impact of these substances on the overall toxicity or potential harm of IQOS is yet to be determined. 15 Moreover, several early studies were funded by the tobacco industry. Newer findings also indicate that HTPs worsen arterial stiffness and have similar effects on blood pressure as combustible cigarettes. 16
Medical knowledge of adverse health effects originating from long-term usage of e-cigarettes and HTPs is limited because of the short period of time since its introduction to the global market. Tobacco smoking, on the other hand, has numerous effects on the development and progression of various diseases such as cancer, pulmonary diseases, and cardiovascular diseases.8,17
Smoking is a well-known risk factor of hypertension and increased arterial stiffness.18–20 Elevated arterial stiffness is associated with a higher cardiovascular risk and may also be an early sign of the development of hypertension. HTPs and e-cigarettes both lead to elevated arterial stiffness, which may indicate an increased cardiovascular risk.19–24
Smoking-associated long-term lung damage includes lung cancer and “chronic obstructive pulmonary disease” (COPD). Lung cancer has been identified as one of the most common forms of cancers and is considered the primary cause of malignancy-associated mortality worldwide 25 while COPD is the third highest contributor to global mortality. 26 Inflammatory processes in the small airways cause irreversible narrowing of the bronchi, leading to obstructive ventilation disorders and lung overinflation. Various studies have suggested that small-airway disease may be an early indicator of COPD.27,28 These changes can be evaluated by oscillometric measurements. 27
The primary aim of this study was to determine if e-cigarettes or HTPs can be considered a healthier option to conventional cigarettes. To achieve this aim, we analyzed the earliest changes in small airway function and immediate effects on hemodynamics after using e-cigarettes, HTPs and combustible cigarettes.
Methods
Study Design and Study Cohort
This single-center, four-arm intervention study in a crossover design included 20 healthy subjects (ten male and ten female), all at least occasional smokers. First, the subjects were screened for behavioral, health, and demographic exclusion criteria: (i) non-smoker, (ii) obesity, (iii) pregnancy, (iv) mental disorders, (v) cardiovascular disease, (vi) pulmonary disease, (vii) age <18 years, and (vii) abnormal physical examination. Participants were consecutively included in the study after they consented within the framework of informed consent. A comprehensive characterization of the cohort was carried out via clinical examination, anamnesis, non-invasive blood pressure measurements, and a questionnaire regarding nicotine consumption.
Before the first measurement, the study participants were randomly allocated to an individual test arm sequence by drawing four numbered pieces of paper, each representing one test arm.
To ensure test validity, a 48-hour washout period was required between the test days, during which subjects were not allowed to smoke or use any other device for nicotine consumption. Furthermore, every test day was scheduled to start simultaneously, minimizing deviations or errors due to circadian rhythm.
The four study arms were composed as follows: (a) cigarette (cig) (Malboro Gold 0.5 mg/cigarette), (b) e-cigarette with free-base nicotine (e-cig (+)) (DIPSE-eGo-cigarette, tank-based; 24 mg/mL, tobacco flavour) (c) IQOS 2.2 (Philip & Morris 0.5 mg/stick) (d) e-cigarette without nicotine (e-cig (-)) (DIPSE-eGo-cigarette, tank-based; zero mg/mL, tobacco flavour). Each participant completed all four study arms for inclusion in the final study.
All participants were instructed on how to use the different devices and how to follow a special smoking scheme for standardization. Regarding the cigarette or the “IQOS” HTP, participants were instructed to smoke the cigarette or the corresponding “IQOS” device until they were fully consumed. The e-cigarettes with and without nicotine had to be vaped ten times, each puff lasting three–five seconds with a resting time of 30 s between the puffs. In addition to the smoking device, all test days followed the same setup. Cardiovascular baseline measurements were conducted every 5 minutes using the Mobil-O-Graph™ (I.E.M., Stollberg, Germany), starting 30 min before the intervention.29,30 Small airway function was measured by oscillometry with the tremoFlo® c-100 (THORASYS Thoracic Medical Systems Inc)31,32 twice throughout the 30 minutes baseline period and 5, 15, 30, and 60 min after intervention.
The local ethics committee agreed to participate in the study and included it in DRKS (DRKS00020446).
All participants received a compensation of €60 for their efforts.
Measurement of Peripheral and Central Blood Pressure and Arterial Stiffness
All cardiovascular parameters, peripheral and central blood pressure, and arterial stiffness were measured with the validated Mobil-O-GraphTM (software version HMS CS 4.2, I.E.M. GmbH) using the oscillometric measuring technique.29,30,33 The measured brachial waveform was recorded at the diastolic blood pressure level and processed using the ARCSolver transfer function, resulting in the central systolic blood pressure. Pulse waveform analysis used the derived central waveforms to calculate the augmentation pressure and augmentation index 34 which was adjusted to a heart rate of 75 bpm. Baseline measurements were used to collect reference data for each participant for statistical analysis.
Measurement of Resistance and Reactance in Central and Small Airways
Central and peripheral lung function, including small airway function, was quantified using the TremoFlo ® c-100 (THORASYS Thoracic Medical Systems Inc), using airwave oscillometry (AO). This technique offers a higher sensitivity than spirometry in identifying bronchodilatory reactions and in patients with poor asthma control than spirometry. 35 In AO, oscillation frequencies ranging from 5 to 37 Hz are briefly superimposed on quiet breathing, allowing the calculation of resistance (R) and reactance (X). R represents the ratio between the pressure drop and flow rate along an airway section, offering a valid and sensitive method for detecting changes in the peripheral airway function. High readings reflect high airflow resistance.
X is used to assess the elasticity of the lungs, compliance, and force of inertia of the motile air column in conducting airways.
Moreover, the reactance area AX5, an indicator of obstruction in small airways, and the air volume between inspiration and expiration, defined as the tidal volume (VT), were calculated using the collected data.31,32
A single measurement was divided into 3 separate data collections of 20 seconds each, and the mean of each measurement was used for statistical analysis. For the measurement to be valid, the coefficient of variation (CV) was less than 15%. 32
Statistical Analysis
No statistical interim analyses were performed during the data collection. Statistical analyses were performed at the end of the study. SPSS statistical software (SPSS 23 Inc, Chicago, IL, USA) was used for statistical analysis. Graphic illustrations were created using Sigma Plot 8.0 (Systat Software Inc, San Jose, USA).
Baseline mean values were used as statistical references for blood pressure, arterial stiffness, resistance, and reactance of the central and small airways. Throughout the investigation period, blood pressure and arterial stiffness were automatically every 5 minutes. By calculating the mean of 3 consecutive values, the measurements were summarized at 15 min intervals for statistical analysis.
First, the values of blood pressure, arterial stiffness, resistance, and reactance of the central and small airways were tested for normal distribution using of Kolmogorov-Smirnov tests.
Based on the crossover design, a two-way repeated measures ANOVA was performed to estimate the interaction between the different devices used and time, followed by post-hoc tests (Bonferroni) performed with G-Power (3.1.9.7) if there was an interaction. In addition, the paired Students t test and Wilcoxon test were used to compare individual time points within the four different test settings. Using ANOVA, we separately analyzed the differences at various times between the four devices. Multivariate analysis of variance (MANOVA) was applied for age, mean arterial pressure (MAP), heart rate (HR), and sex. All data are expressed as mean ± standard error of the mean (SE), unless otherwise identified.
Results
Baseline Characteristics
We included 20 subjects into our study, 10 male and 10 female. They were on average 25.4 years old with an average weight of 67.5 kg. All our subjects were active smokers (mean: 3.3 cigarettes per day). No subjects had to be excluded at any point.

Nicotine Leads to Rise of Bronchial Obstruction, Reactance and Tidal Volume
The central obstruction (R5) increased after smoking cigarettes (P < 0.05), nicotine-containing e-cigarettes (minute 5, P < 0.01; minute 15, P < 0.05), or IQOS (minute 5: P < 0.01, minute 15: P < 0.05). In contrast, there was no change in central obstruction after the use of e-cigarettes without nicotine. After correcting for multiple testing, the increase remained statistically significant (P = 0.016).
Cigarette smoking (P < 0.01), nicotine-containing e-cigarettes (minute 5: P < 0.05; minute 15-30: P < 0.01), or IQOS (minute 5: P < 0.01; minute 15: P < 0.05) caused an increase in peripheral bronchial obstruction (R5-20). Similar to our findings for central obstruction, no change in peripheral bronchial obstruction was observed after smoking an e-cigarette without nicotine. These findings remained significant after correcting for multiple tests (P = 0.001).
Reactance increased significantly 5 min after the consumption of cigarettes, IQOS, and nicotine-containing e-cigarettes (P < 0.05). At minute 15, there was no significant difference in reactance. After vaping a nicotine-free e-cigarette, there was no significant change in the reactance. A significant P-value (P = 0.001) was observed after Bonferroni correction for treatment and time.
Smoking a cigarette or a nicotine-containing e-cigarette significantly increased the tidal volume (P < 0.01) at 5 min. The same effect was observed after consuming IQOS (P < 0.05). In addition, the tidal volume increased until 30 min. Vaping a nicotine-free e-cigarette had no significant effect on tidal volume. After correcting for multiple testing, the results remained statistically significant (P = 0.001).
Peripheral Blood Pressure, Pulse Pressure and Heart Rate Rise After Smoking or Vaping
All four study arms showed an increase in peripheral systolic blood pressure immediately after consumption (Figure 1A) with a P-value of <0.01 after 5 min. Smoking significantly elevated systolic blood pressure, which persisted at high levels for 45 min. After smoking a nicotine-containing e-cigarette, it persisted for only 20 minutes. Smoking of an e-cigarette without nicotine led to increased systolic blood pressure for 20 min. In comparison to these findings, systolic blood pressure remained elevated for 35 minutes after the consumption of IQOS. After correcting for multiple comparisons of treatment and time, a significant difference was observed (P = 0.034). (A) R5 rose significantly after smoking or vaping nicotine containing products. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (B) R5-20 rose significantly after smoking or vaping nicotine containing products. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (C) AX rose significantly after smoking or vaping a nicotine containing product. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (D) After smoking or vaping nicotine containing products the TV rose significantly. Values are presented as mean ± SE. ANOVA showed no difference between the groups. ANOVA, analysis of variance; AX, reactance; cig, cigarette; e-cig, e-cigarette; R5, central obstruction; R5-20, peripheral obstruction; SD, standard deviation; SE, standard error; TV, tidal volume.
In contrast, the significant increase in peripheral diastolic blood pressure was shorter. After smoking cigarettes, it remained elevated for 15 min. The consumption of nicotine-containing e-cigarettes led to an elevated diastolic blood pressure for 20 min (P < 0.01 until minute 10, P < 0.05, at minutes 15 and 20). Similar effects were observed after consuming an e-cigarette without nicotine (P < 0.01 until minute 20). In contrast to the other arms, elevation of diastolic blood pressure after vaping IQOS started at minute 5 (minutes 5-15, P < 0.01; minute 20, P < 0.05). At minutes 5 and 10, the four arms showed a significant difference from each other (ANOVA, P < 0.05 and P < 0.01), with the highest rise after vaping IQOS. However, after Bonferroni correction (treatment and time), no significant differences were observed (P = 0.617).
Peripheral pulse pressure increased immediately after smoking in all four groups. After smoking cigarettes, it remained elevated for 20 min (P < 0.01 until minute 10 and minute 20; minute 15: P < 0.05). In contrast, the peripheral pulse pressure remained elevated only for 10 minutes after the consumption of an e-cigarette containing nicotine (minute 1: P < 0.05; minute 5-10: P < 0.01) and for 35 minutes after the use of IQOS (minutes 1 and 20: P < 0.05; minute 5-15: P < 0.01). Vaping e-cigarettes without nicotine led to elevated peripheral pulse pressure for 25 min (minutes 1 and 20: P < 0.05; minute 5-15: P < 0.01). After correcting for multiple tests, a significant difference was observed (P = 0.032).
After the intervention, the heart rate increased significantly in the groups that smoked or vaped nicotine-containing products (P < 0.01, minute 1), whereas it took 5 minutes to significantly increase after vaping an e-cigarette without nicotine (P < 0.01). The heart rate remained significantly elevated for 20 min after the consumption of a cigarette, whereas it normalized 15 min after an e-cigarette. Similar effects were observed after IQOS (blood pressure normalized after 25 min). Smoking an e-cigarette without nicotine led to an increased heart rate from minutes 5 to 10, and at minute 30. A significant difference was observed between the groups at min 1 and 5 (ANOVA, P < 0.01). After smoking a cigarette or vaping IQOS, the heart rate increased more than that after vaping an e-cigarette. After correcting for multiple testing, there was still a significance (P = 0.001) Figures 2–4. (A) pSBP rose significantly after smoking or vaping. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (B) pDBP rose significantly after smoking or vaping, IQOS leading to the highest diastolic blood pressure followed by cig. Values are presented as mean ± SE. ANOVA showed a difference between the groups at minute 5 and 10. (C) pPP rose significantly after smoking or vaping. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (D) After smoking a cig or vaping IQOS the heart rate rose higher than after vaping an e-cig. Values are presented as mean ± SE. ANOVA showed a difference between the groups at minute 1 and 5. ANOVA, analysis of variance; cig, cigarette; e-cig, e-cigarette; pDBP, peripheral diastolic blood pressure; pPP, peripheral pulse pressure; pSBP, peripheral systolic blood pressure; SD, standard deviation; SE, standard error. (A) cSBP rose significantly after smoking or vaping. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (B) cDBP rose significantly after smoking or vaping, cig leading to the highest central diastolic blood pressure followed by IQOS. Values are presented as mean ± SE. ANOVA showed a difference between the groups at minute 5 and 10. (C) cPP rose significantly after smoking or vaping. Values are presented as mean ± SE. ANOVA showed no difference between the groups. ANOVA, analysis of variance; cig, cigarette; cDBP, central diastolic blood pressure; cPP, central pulse pressure; cSBP, central systolic blood pressure; SD, standard deviation; SE, standard error. (A) AIX-75 rose significantly after smoking or vaping. Values are presented as mean ± SE. ANOVA showed no difference between the groups. (B) TPR rose significantly after smoking or vaping. Values are presented as mean ± SE. ANOVA showed no difference between the groups. AIX-75, augmentation index adjusted at heart rate 75 bpm; ANOVA, analysis of variance; cig, cigarette; TPR, total peripheral resistance; SD, standard deviation; SE, standard error.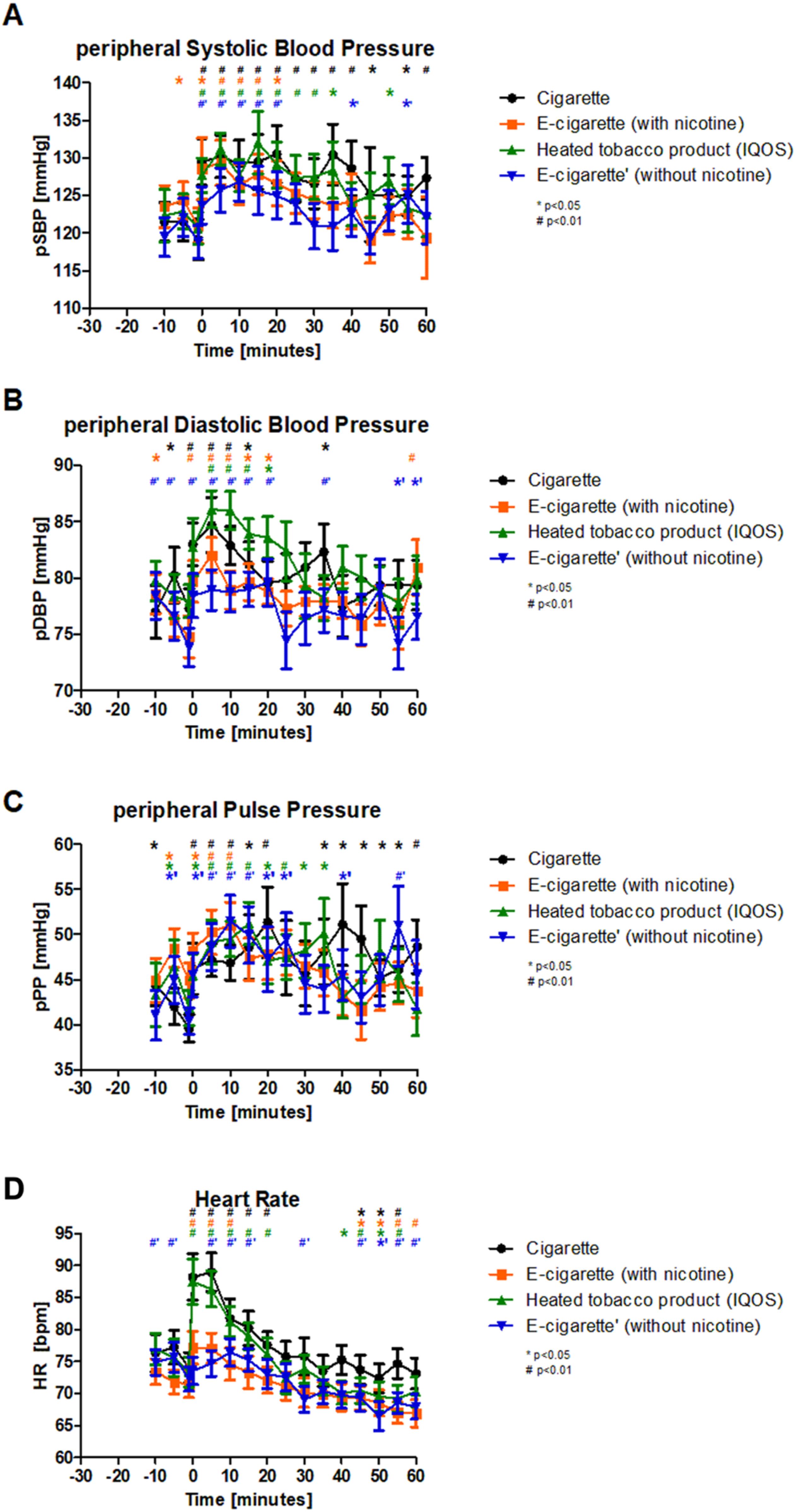


Central Blood Pressure and Central Pulse Pressure Rise After Smoking/Vaping
Central systolic blood pressure increased immediately after smoking a cigarette (P < 0.05), a nicotine-containing e-cigarette (P < 0.05), or an e-cigarette without nicotine (P < 0.01). After vaping IQOS, it took 5 min for elevated central systolic blood pressure to be observed. After smoking cigarettes, the central systolic blood pressure remained elevated for 40 minutes. For the first 20 minutes after the intervention, e-cigarettes containing nicotine and those without nicotine caused a significant increase in central systolic blood pressure. IQOS led to significantly elevated central systolic blood pressure for 30 min (minutes 5– 35). After Bonferroni correction for treatment and time, there was still a significant difference (P = 0.04); however, there was no difference among the four groups.
The central diastolic blood pressure increased immediately after all four interventions (cig, e-cig (+), IQOS: P < 0.01; e-cig (-): P < 0.05). The use of IQOS resulted in the longest increase in all interventions (25 minutes). A significant difference among the four study arms was observed at minutes 5 and 10. At minute 5, the highest increase was observed after smoking a cigarette, whereas at minute 10, the highest increase in diastolic blood pressure was observed after vaping IQOS. After correcting for multiple testing, no significant differences were observed (P = 0.132).
The central pulse pressure increased significantly in all four groups immediately after smoking (IQOS: P < 0.01; e-cig (+), e-cig (-): P < 0.05). After smoking cigarettes, IQOS, or e-cigarettes without nicotine, it remained elevated for 20 min. In comparison to these findings, the central pulse pressure increased for only 15 min after using an e-cigarette containing nicotine. After the Bonferroni correction, a significant difference was observed (P = 0.045).
Cigarette, IQOS, E-cigarette Containing Nicotine and E-Cigarette Without Nicotine Lead to Elevated Heart Rate-Adjusted Augmentation Index and Total Peripheral Resistance
The heart rate-adjusted augmentation index (adjusted at 75 bpm; AIX-75) increased in all four groups immediately after the intervention. After smoking a cigarette, IQOS, or e-cigarette without nicotine, it remained elevated for 20 min (cig: P < 0.01, from minute 15 to-20 P < 0.05, e-cig (-), IQOS: P < 0.01), whereas after using a nicotine-containing e-cigarette, it remained elevated only for 10 min (P < 0.05 at minute 1; minute 5 -10: P < 0.01). After correcting for multiple tests (time and treatment), a significant difference was observed (P = 0.039).
Total peripheral resistance/vascular resistance (TVR) increased significantly after smoking cigarettes (P < 0.05), IQOS (P < 0.05), or e-cigarettes containing nicotine (P < 0.01). The TVR remained elevated for 10 min after the consumption of a cigarette, whereas the elevation persisted for 25 min after consumption of a nicotine-containing e-cigarette. After using IQOS, a significantly elevated TVR was detected until the end of the examination. In contrast, after using e-cigarettes without nicotine, the TVR increased from minute 5 to minute 20 (P < 0.01). We observed a significant difference (P = 0.044) after Bonferroni correction.
Discussion and Conclusion
Nicotine is well known to increase blood pressure and heart rate when inhaled via cigarettes or e-cigarette.36–38 In our study, we observed an increase in systolic and diastolic blood pressure immediately after consuming a cigarette or e-cigarette, or after vaping IQOS. Interestingly, the blood pressure increased after smoking e-cigarettes without nicotine intake. We observed similar effects on the heart rate. Therefore, nicotine cannot be the only component that influences the heart rate and blood pressure. E-cigarettes contain multiple chemicals, such as propylene glycol, glycerol, and flavoring agents, and it is not possible to determine which is responsible for the increase in blood pressure or heart rate. 39
Compared to the other arms of our study, the increase in diastolic blood pressure was higher after vaping IQOS. HTPs negatively impact the cardiovascular system. 40 Ioakeimidis et al. reported an increase in systolic blood pressure after vaping of IQOS. In contrast to our data, there was no significant difference in blood pressure after smoking a cigarette or vaping. 41 Nevertheless, both studies showed that HTPs have similar effects on the cardiovascular system as cigarettes do. Moreover, nicotine intake after cigarette smoking and vaping IQOS was similar. 42 Whether the observed effect was due to nicotine or other components should be evaluated in future studies.
After smoking a cigarette or vaping IQOS, the heart rate increased more than that after vaping an e-cigarette with or without nicotine. St. Helen et al reported lower peak nicotine plasma levels after vaping an e-cigarette than after smoking a cigarette. 43 This might explain the observed difference in the heart rate increase. Consistent with our data, they also reported a lower increase in heart rate after vaping an e-cigarette than after smoking a cigarette. 43 Ioakeimidis et al. were unable to show a difference in the effect on heart rate between IQOS and cigarettes. 41 Therefore, the observed difference between e-cigarettes and cigarettes/IQOS may be due to the differences in inhalant use.
Corresponding to the findings of a previous study, we observed an increase in peripheral pulse pressure in all four study arms after smoking or vaping. 44 Elevated pulse pressure is an indicator of reduced arterial compliance and elevated arterial stiffness.45–47 Furthermore, the total peripheral resistance/vascular resistance (TVR) increased in all four study arms after smoking/vaping, which is also an indicator of elevated arterial stiffness. No significant differences were observed between the groups.
In a mouse model, El-Mahdy et al. observed that long-term exposure to e-cigarettes leads to vascular dysfunction, which causes an increase in vascular resistance. A smaller effect was observed when vaping nicotine-free liquids. 48 However, these effects were observed after long-term vaping, whereas the acute effects were analyzed. In another study, the same author showed that vascular endothelial dysfunction also occurred after vaping nicotine-free e-cigarettes. Loss of NO leads to reduced vasodilatation and loss of anti-inflammatory and anti-apoptotic functions, which cause vascular damage. These effects were intensified when a nicotine-containing liquid was inhaled. Even if these findings are observed after long-term use, further data suggest that acute use results in oxidative stress and elevated inflammatory markers, which could cause vascular damage. 49 These effects and our short-term observation setup might explain why we were unable to show a difference in the parameters associated with arterial stiffness.
Moreover, elevated pulse pressure is associated with cardiovascular diseases such as coronary heart disease or congestive heart failure.46,50 Consequently, our data indicated that smoking and vaping have a negative impact on the cardiovascular system. As we observed elevated pulse pressure in all our groups, the observed effect cannot only be attributed to the impact of nicotine.
Furthermore, peripheral pulse pressure was correlated with age. 51 In our cohort, the mean age was 25.4 years which is very young compared with the general population in Germany.52,53 Consequently, the observed changes in pulse pressure may have been even greater in the older cohort.
After smoking or vaping, the central systolic and diastolic blood pressures increased significantly in all four arms of our study. It is known, that cigarettes or nicotine containing e-cigarettes influence blood pressure and arterial stiffness. 16 Dimitrades et al suggested that vaping nicotine-containing e-cigarettes may activate the sympathetic nervous system. 37 In addition, we observed an increase in central blood pressure after vaporing nicotine-free e-cigarettes. Other components such as fine and ultrafine particulate matter are known to influence blood pressure. 54 Moreover, central blood pressure correlates more strongly with the incidence of cardiovascular diseases than peripheral blood pressure. 55 Therefore, smoking and vapor may increase the risk of cardiovascular events. Whether the impact of nicotine-free e-cigarettes is the same as that of nicotine-containing products and whether other components contained in liquids or HTPs influence blood pressure should be evaluated further in future trials.
At minutes 5 and 10, peripheral and central diastolic blood pressures differed significantly among the four study arms. However, this significance may be because diastolic blood pressure values are lower than systolic blood pressure values. Consequently, a small increase due to normal variations in blood pressure or slightly elevated diastolic blood pressure may result in significant data. This might explain why we did not observe a difference in systolic blood pressure between the groups.
Central pulse pressure can be an indicator of cardiovascular events and renal impairment. 56 Additionally, elevated central pulse pressure is associated with vascular remodeling.57,58 Smoking and vaping led to an increase in pulse pressure in all the groups. This finding also strengthens our hypothesis that smoking and vaping result in vascular remodeling and increase the risk of cardiovascular events.
Cigarette smoking leads to an increase in AIX-75, a parameter that represents arterial stiffness. Vaping an e-cigarette or IQOS had the same effect; however, the effect of a nicotine-containing e-cigarette lasted for only 10 min, whereas the others lasted longer. In contrast to our data, Antoniewicz et al found that only vaping a nicotine-containing e-cigarette led to an increase in AIX-75. 59 They did not observe any effect of the nicotine-free liquid on AIX-75. More trials are needed to evaluate the effects of e-cigarettes, IQOS, and their different liquids on arterial stiffness.
Central and peripheral bronchial obstruction increased after smoking or vaping nicotine-containing products. These findings are consistent with data showing that nicotine has an obstructive effect on bronchi. 60 Moreover, these findings show a similar impact of nicotine regardless of the mode of consumption. Consequently, our data suggests, that regarding the nicotine-related impact, e-cigarettes or HTPs are not a healthier alternative to cigarettes.
As some patients with COPD develop clinical symptoms before presenting with airflow obstruction, 61 it is important to find methods showing earlier evidence of COPD. Several studies have demonstrated that small airway disease precedes emphysema in COPD.27,62,63 Oscillometry was used to quantify these changes. 27 Our oscillometric measurements showed an increase in peripheral bronchial obstruction after smoking or vaping nicotine-containing products. Therefore, we were able to show that nicotine has an immediate effect on small airways, and that this effect can be measured using oscillometric techniques.
Gellatly and colleagues showed that nicotine-free e-cigarette vapor leads to an increased inflammatory reaction and increased mucin production in the small airways. 64 In our study, we did not observe inflammatory reactions, as we only evaluated acute effects. However, inflammation is an important component of small airway disease and should be evaluated further.
As there were no changes in obstruction after vaping nicotine-free liquids, other components contained in these liquids seemed to have less of an effect on bronchial obstruction. However, Chapman et al. showed that different liquids have different effects on allergic airways disease. 65 Consequently, different flavors may have different effects on bronchial obstruction. Only one flavor was used in our study. Therefore, more data are required to draw conclusions regarding the effects of nicotine-free liquids on bronchial obstruction.
After smoking or vaping nicotine-containing products, the tidal volume increased significantly. This effect may be caused by an elevated respiratory drive resulting from sympathetic activation due to the influence of nicotine. 37
This trial evaluated the effects of smoking a cigarette or vaping an e-cigarette/HTP on central and peripheral hemodynamics, arterial stiffness and lung function. They had similar effects on hemodynamics, and all nicotine-containing products also affected the small airways.
We observed that vaping a nicotine-free e-cigarette influenced arterial stiffness, as well as central and peripheral hemodynamics. Therefore, nicotine may also affect the cardiovascular system.
In contrast, the effects of IQOS on heart rate were stronger than those of smoking cigarettes or vaporing e-cigarettes.
Study Limitations
The limitations of this study primarily arise from the small number of subjects and their low mean age of 25.4 years. Having used DIPSE-eGo-cigarettes and IQOS with specific liquids, our results only apply for these particular devices and liquids. Based on our findings, we can only hypothesize generalizability for HTPs or e-cigarettes in general.
Furthermore, standardization of smoking and vaping remains difficult despite the following smoking scheme as all individuals differ in their depth of inspiration. Additionally, by instructing the subjects to continue breathing calmly to measure lung function, breathing changed unconsciously because of their intentness.
Owing to the limited observation time, this study can only show acute effects and does not allow long-term monitoring of effects. We did not monitor blood pressure directly by arterial catheterization and did not quantify catecholamines during our experiments. This may increase the inaccuracy of our measurements.
All participants were occasional smokers, which may have influenced their baseline values and measured effects. As we did not measure nicotine or cotinine serum levels, we were unable to objectify our participants’ smoking habits. Different smoking habits may have led to different baseline values, which may have influenced the results. Not having drawn blood at any timepoint, we were not able to analyze cotinine levels subsequently. Nevertheless, we are addressing this limitation in future studies implemented by our group.
From an academic point of view, it would have been interesting to include non-smokers in our study. However, this is ethically not justifiable. This is the reason why we chose a nicotine-free liquid as control. We did not quantify the liquid’s ingredients by gas chromatography.
Moreover, we did not analyze the influence of smoking or vaping on inflammatory parameters. Inflammation plays an important role in vascular remodeling and small airway disease and should therefore be addressed in further studies.
Conclusions
All nicotine-containing products influence small airways. Concerning hemodynamics, cigarettes, IQOS, and e-cigarettes have similar effects. No differences were observed between the nicotine-containing and nicotine-free e-cigarettes. Consequently, our data suggests that HTPs and e-cigarettes are not healthier alternatives to cigarettes.
Footnotes
Author Contributions
Conceptualization, L.J., I.B., A.H., M.W., D.D. and K.F.F.; methodology, L.J., I.B., A.H., M.L., T.J., and K.F.F.; software, K.F.F., L.J., I.B., M.L., and D.D.; validation, L.J., I.B., M.L., T.J., D.D. and K.F.F.; formal analysis, L.J., I.B., and K.F.F.; investigation, I.B., A.H.; resources, M.W., D.D. and K.F.F.; data curation, I.B., A.H. and K.F.F.; writing—original draft preparation, L.J., I.B., A.H., and K.F.F.; writing—review and editing, L.J., I.B., A.H., M.L., T.J., M.W., D.D., and K.F.F.; visualization, L.J., I.B., and K.F.F.; supervision, K.F.F.; project administration, K.F.F.; funding acquisition, M.W., D.D. and K.F.F. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by This study was financed by Medizinische Klinik III of University Hospital Schleswig-Holstein, Luebeck, Germany.