
Abstract
BACKGROUND
With the emergence of the WHO Framework Convention on Tobacco Control, globally the use of tobacco has decreased notably, although, it still requires efforts at individual, organizational, community level to decrease the rate further. Dental professionals are at an excellent position to provide tobacco cessation counselling and interventions, however, it is not practiced much due to lack of training and lack of knowledge. Therefore, this systematic review was conducted to assess the global status of knowledge, attitude and practice on tobacco cessation interventions among dental professionals.
MATERIALS AND METHOD
A systematic search of 6 databases with no language restriction since 2000 was undertaken. Studies were included if they assessed knowledge, attitude and practice on tobacco cessation interventions among dental professionals using a validated or prevalidated tool. The data obtained for assessment of knowledge, attitude, practice, curriculum and barriers were represented through heatmaps. Quality assessment of the studies was done using Newcastle Ottawa scale.
RESULTS
Fifty six studies were included in this systematic review. Majority of the studies were found to be of moderate quality. Knowledge regarding the tobacco cessation interventions was more theoretical than practical. All the studies showed a favorable attitude among dental professionals towards tobacco cessation intervention.
CONCLUSION
The included studies lack homogeneity in assessing knowledge, attitude and practice on tobacco cessation interventions. The development and validation of a standardized questionnaire to assess knowledge, attitude and practice on tobacco cessation interventions could be a potentially effective way to uniformly gather data on the subject.
Keywords
Introduction
The history of tobacco counseling dates back to the 1970s when the recommendations to dentists to help patients to quit smoking were initiated by the air force dental clinic at Lackland, USA. 1 Tobacco cessation counseling is a practice used by health professionals to train patients on how to quit tobacco use in any form. According to the World Health Organization, tobacco cessation should be a part of dental practice where dental and non dental professionals should be actively involved in helping patients to quit tobacco.2,3
Dental care professionals are in a better position and therefore play a potential role to identify tobacco users, as during a routine check up intraoral signs such as halitosis, tobacco stains and oral hygiene problems can be examined. 4 Combating the tobacco epidemic should be done through regular tobacco cessation intervention in their everyday clinical practice. However, globally studies have reported that the proportion of tobacco users who receive guidance and counseling from a dental professional is not sufficient.5,6
A comprehensive and integrated tobacco control programme must incorporate both the promotion of quitting smoking as well as the treatment of tobacco dependency. The healthcare professionals can support the smokers in their efforts to stop using tobacco and helping them to overcome their addiction may strengthen other tobacco control strategies as well, which is in fact in line with the WHO FCTC article 14. 7
Even though the consumption of tobacco has decreased globally by 22.3%, further efforts at tobacco control are required by the community, healthcare professionals and through changes in policy in order to see more decline in the trend of tobacco consumption. 8
Healthcare professionals must be informed of behavioral as well as pharmacotherapy related measures for tobacco cessation. 9 Previous systematic reviews have been conducted which have assessed either attitude 10 or practice11,12 among different healthcare workforce such as nurses, 11 dental professionals, 10 medical professionals, 13 healthcare workers. 12
Methodology
The systematic review was conducted according to the PRISMA guidelines. The protocol was registered with Prospero (Trial Number: CRD42021250962).
Search sources
The search was conducted electronically on PubMed, LILACS, Web of Science, Cochrane, CINAHL and Scopus databases from 15th May 2021 to 3rd September 2021 without any restriction of languages and from the year 2000 up till 2021. A search of the grey literature was performed in Google Scholar and Open-Grey. Two authors (NT and HP) performed the literature search independently according to a predefined strategy, and the duplicates were removed using EndNote software.
Search strategy
The 3 reviewers (HP, BMP and NT) identified the possible domains and subdomains using the PICO strategy to recognise the existing related literature on knowledge, attitude and practice on tobacco cessation intervention.
P : Dental Professionals; I : Tool for assessment of knowledge, attitude, practice of the tobacco cessation methods; Comparison: Not applicable; Outcome: Knowledge score, attitude score ,practice score, inclusion of tobacco cessation interventions in curriculum, barriers of the dental professionals regarding tobacco cessation interventions and responses of participating dental professionals in percentage.
The search was implemented using the keywords : Tobacco Cessation, Tobacco Counseling, Quitting Tobacco, Smoking and Smokeless Tobacco, Dental Professionals. Partial search was done using the boolean operators (AND, OR) with the keywords. The search strategy was carried out using the keywords and MeSH terms provided in Supplementary Table 1.
Study selection and eligibility criteria
All types of published studies (Cross-sectional, case control, cohort) assessing the knowledge, attitude and practice regarding tobacco cessation counseling among dental professionals were included. Similar studies assessing barriers to tobacco cessation counseling and inclusion of tobacco cessation in the dental curriculum was also included in this review. Randomized clinical Trials and studies with inadequate information regarding methods of development and validation was excluded. Letter to the Editor, Perspective and commentaries were also excluded.
Assessment of risk of bias
The included studies were evaluated for their methodological quality using the Newcastle-Ottawa Quality Assessment Scale 14 : Critical appraisal checklist for analytic cross sectional studies by BMP, USB, DA and MDB independently. In case of any disagreement between the reviewers, a fifth reviewer was consulted. Based on their methodological quality, the studies were divided into high, moderate and low risk of bias.
Results
The search strategy yielded a total of 3726 articles from the databases of PubMed, LILACS, Web of Science, Cochrane, CINAHL, and Scopus (Figure 1). Following removal of articles for duplication, 104 articles were found to be eligible for assessment. A total of 48 studies were further excluded as full text was not available, the survey instrument was not validated, study designs consisted of narrative review, systematic review, intervention studies, knowledge, attitude and practice component was not assessed in many studies and 1 study was conducted among school students. PRISMA flowchart.
Study Characteristics of the included studies in the systematic review.

*GHPSS = Global Health Professions Student Survey
Based on the inclusion criteria, all the studies had included a validated tool, 3 studies15,36,54 have used the Global Health Professions Student Survey (GHPSS) tool, whereas 2 studies17,21 have used a modified version of the same.
Since the questions used to assess knowledge, attitude, and practise regarding tobacco cessation counseling varied a lot, the data was visualized using heatmaps (Figures 2 to 4), where the width of the columns represents the number of studies that included the question and the color represents the level of awareness, positive attitude, and practice as 25%, 25-50%, 50-75%, and >75%. The heatmap includes the questions which were a part of the questionnaire in at least 3 or more studies. The similar questionnaires were clubbed together. Heatmap of questions on knowledge towards tobacco cessation interventions. Heatmap of questions on attitude towards tobacco cessation interventions. Heatmap of questions on practice towards tobacco cessation interventions.


A total of seventeen18,20,22,23,32,36,38,41,42,44,46,49,50,54,55,67,70 studies had questions related to knowledge about tobacco cessation counseling (Figure 2), among which eleven18,20,22,32,36,44,49,50,54,55,67 studies assessed the awareness on 5As and 5R where the knowledge score was found to be in the range of 75% and above in only 5 studies.36,44,50,54,67 Awareness on various forms of tobacco was reported in only 3 studies18,20,46 and in all 3 studies, the knowledge score was high. Knowledge on NRT/pharmacotherapy was also reported in studies conducted by Yahya NA et al, 50 Resende M et al, 49 Studts JL et al 41 and Saddichha S et al 54 and in majority it was found to be between 50-75%.
Figure 3 depicts thirty seven studies15-18,23-26,28-33,36, 37,39-42,44-46, 48-50,52,55-57,61,64,65,68,70,71 which assessed the attitude of dental professionals towards tobacco cessation counseling. A positive attitude was observed among the dental professionals in the majority of the studies18,23-25,28-33,37, 39-42,46,48,49,55-57,61,64,65,68,70 regarding advising patients to quit tobacco. Responses to negative impact of tobacco cessation counseling were also included and studies16,18,24,30,32,33, 40-42,45,50,52,56,70,65,71 were found to be less negative towards tobacco cessation counseling as a part of clinical practice.
Among the thirty four studies18,19,22,26,28-30,33-35,37,41,43-51, 54-56,58,59,61,67,70,68 which assessed the practice among dental professionals on tobacco cessation counseling (Figure 4), this review found that dental professionals were in the practice of conducting tobacco cessation counseling.18,19,30,33-35,43,46,47,49,50,54,56,66 The practice of 5As was followed more as compared to 5Rs, as evident from Figure 4. It was also observed that brief counseling was more prevalent as compared to prescribing NRT,22,29,35,37,43,49,51,59,68,66 drugs.22,41,44,49,68,66
All twelve studies15,21,30,35,36,44,46,49,57,58,68,66 reported that study participants had a formal training in tobacco cessation (Figure 5) and among thirty one16, 18,19,22,26,28-33,35,37,39, 41,42,44,48,50,52,53,55,56,58,59,61,67,70,66,68,71 studies which assessed barriers related to tobacco cessation interventions (Figure 6), time and training were cited to be the most common barriers. Heatmap of questions on curriculum on tobacco cessation interventions. Heatmap of questions on barrier towards tobacco cessation interventions.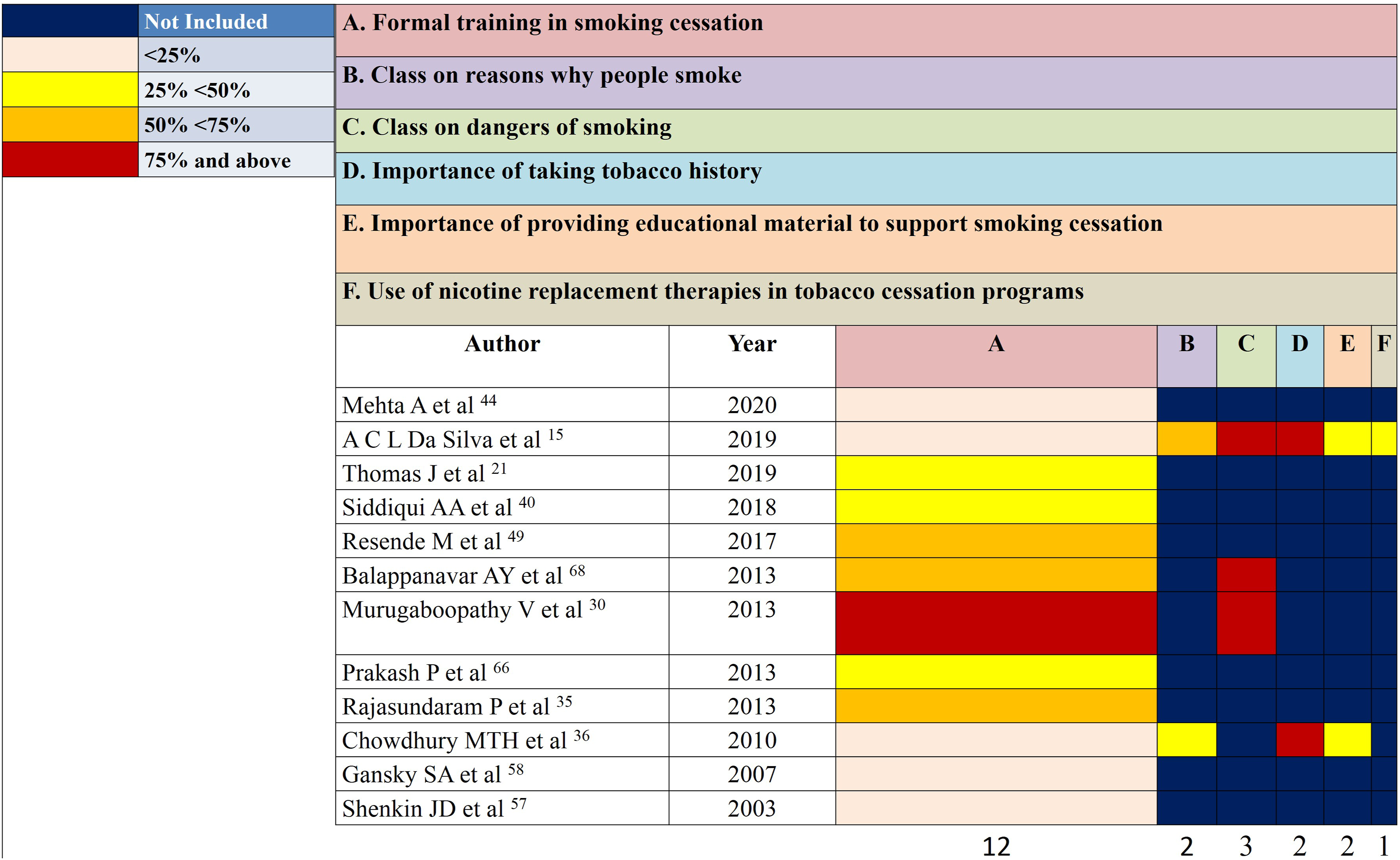

Risk of bias assessment of included studies in the systematic review.

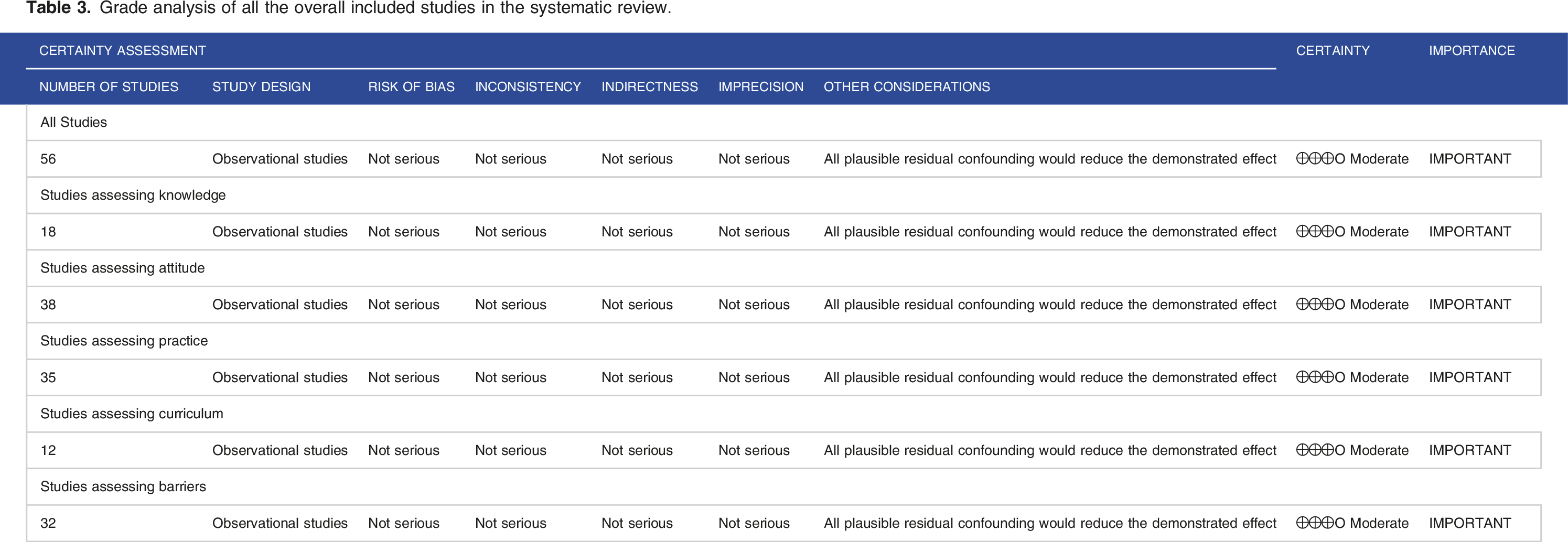
Grade analysis of all the overall included studies in the systematic review.
Discussion
The habit of tobacco consumption is one of the biggest public health threats the world is facing where about 8 million people a year around the world are affected. 72 Tobacco cessation interventions must be advocated strongly to result in benefits over manifolds for the tobacco users. 73 For healthcare professionals, providing tobacco cessation counseling should be one of the key roles. Especially for dental professionals, it is implied that it is an obligation which is required to restrict the consumption of tobacco. 74 Despite this, there is a lack in evidence generated data on the knowledge, attitude or perception and practice of dental professionals on tobacco cessation interventions.
Studies included in this systematic review have assessed the knowledge, attitude and practice regarding tobacco cessation interventions among healthcare professionals, however, no study has collated the data therefore, this current study was conceptualized to quantitatively assess those various studies in order to identify useful information which may be used for future development of a standardized questionnaire or methodology for tobacco cessation interventions.
Studies from developed nations are lesser in comparison, the reason for which could be an already existing system of tobacco cessation interventions among those nations.75,76 Since, the prevalence of tobacco is higher in the developing countries, 75 there should be provisions for generating awareness regarding tobacco cessation counseling among the healthcare professionals. Regarding the knowledge component, eleven studies18,20,22,32,36,44,49,50,54,55,67 assessed the awareness on 5As and 5Rs of tobacco cessation and among those, 5 studies36,44,50,54,67 showed awareness to be above 80%, however in certain studies18,58,59 the practice of 5As was found to be as low as 11%, 18 therefore there is a further need to incorporate 5As as a major intervention for tobacco cessation, as it is an established method of brief tobacco counseling which is not time consuming.
Four studies41,49,50,54 enquired on the knowledge of Nicotine Replacement Therapy/Pharmacotherapy among the healthcare professionals and it was below 75% among all studies. Attitude of the healthcare professionals is another crucial component while providing tobacco cessation counseling. Most of the studies had included questions evaluating the same. More than 75% of the healthcare professionals in about eighteen studies18,24,25,28,29,31,33,37,39-42,46,48,49,57,64,62 showed a positive attitude towards advising patients to quit tobacco. Similar findings were reported by Goel D, 77 where favorable attitudes were observed in spite of poor practice regarding tobacco counseling. In 7 studies18,26,32,33,41,45,70 25-50% of the healthcare professionals believe enquiring on tobacco habits leads to a negative influence on clinical practice.
This attitude among healthcare providers must be altered through training and thus create a positive impact for the patients. Various studies have remarked on the effectiveness of tobacco cessation counseling training for healthcare providers.78-80. Training programs are also shown to change the attitude of the healthcare professionals in tackling the barriers towards tobacco cessation counseling. 81 The training programs must be comprehensive, tailor made to target different sectors of population and must be reinforced at regular intervals, based on the current dynamic policies 82 and program developments on tobacco control.
Out of twenty three studies, fourteen studies19,26,29,30,34,35,37,43,45,55,61,67,70,71 reported that the healthcare professionals ask the patients about their tobacco consumption and it was found to be around more than 75%, as depicted in the heatmap. It is evident from the findings that compared to practice of 5Rs, more dental professionals practice 5As. This finding is partly consistent with a systematic review of doctor’s smoking status and their practice towards tobacco cessation interventions. 13
Only ten studies22,29,35,37,43,49,51,59,68,66 reported the dental professionals were in the practice of prescribing NRT, which is very low and efforts must be undertaken to educate the dental professionals on NRT and pharmacotherapy as well. The most common barriers in providing tobacco cessation counseling as enlisted by the studies were time,16, 22,26,29,32,33,37,39,41,42,44,48,50,52,53,58,59,61,67,70,66,68,71followed by training,18,22,28-32,35,37,39,44,48,52,53,59,66,68,71 and this similar finding was reported in a study conducted among African healthcare workers as well 12
The findings from this systematic review suggests that there is a need to develop and validate a standardized questionnaire to assess the knowledge, attitude and practice of tobacco cessation counseling among healthcare professionals.
There is lack of homogeneity among the included studies with regard to the questionnaires used, study population, therefore meta-analysis could not be done for the current study. There is a difference in the outcome measures of the studies as many studies have assessed either knowledge, attitude or practice rather than the entire KAP component, therefore it is difficult to compare and draw conclusions regarding the same. None of the studies have deducted any knowledge, attitude and practice score from their findings, hence it was not possible to quantify the knowledge, attitude and practice level.
Future implications and recommendation
The results imply that there is an urgent requirement to modify the current dental education curriculum to improve dental student’s involvement in tobacco control, as before entering the workforce, students should have tobacco cessation intervention training during their academic years.
Conclusion
The current findings of this systematic review shows that knowledge regarding aspects of tobacco cessation among dental professionals was lacking in developing countries. In spite of a favorable attitude towards tobacco cessation intervention, practice of conducting tobacco cessation counseling was not prevalent. A well designed structured questionnaire should be developed and validated for international comparisons to assess the knowledge, attitude and practice among healthcare professionals. The above stated recommendations could be incorporated in future studies assessing knowledge, attitude and practice among healthcare providers.
Supplemental Material
Supplemental Material - Global Status of Knowledge, Attitude and Practice on Tobacco Cessation Interventions Among Dental Professionals: A Systematic Review
Supplemental Material for Global Status of Knowledge, Attitude and Practice on Tobacco Cessation Interventions Among Dental Professionals: A Systematic Review by Harsh Priya, Manali Deb Barma, Bharathi M Purohit, Deepali Agarwal, Upendra Singh Bhadauria, Nitesh Tewari, Shalini Gupta, Deepika Mishra, Rahul Morankar, Vijay Prakash Mathur and Ritu Duggal in Tobacco Use Insights
Supplemental Material
Supplemental Material - Global Status of Knowledge, Attitude and Practice on Tobacco Cessation Interventions Among Dental Professionals: A Systematic Review
Supplemental Material for Global Status of Knowledge, Attitude and Practice on Tobacco Cessation Interventions Among Dental Professionals: A Systematic Review by Harsh Priya, Manali Deb Barma, Bharathi M Purohit, Deepali Agarwal, Upendra Singh Bhadauria, Nitesh Tewari, Shalini Gupta, Deepika Mishra, Rahul Morankar, Vijay Prakash Mathur and Ritu Duggal in Tobacco Use Insights
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s note:
Travel Grant by Burrow Foundation for registration and presentation at the Online European Association of Dental Public Health Congress 2021, Abstract number 55 under Education and Oral Epidemiology.
Supplemental Material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.