
Abstract
Background
Evidence suggests that the prevalence of tobacco use has declined significantly in the general population but still remains high among people incarcerated in high-income countries. Tobacco use is the second leading risk factor of mortality and morbidity worldwide. The objective of this study is to synthesize evidence on the prevalence of smoking among people incarcerated in Western European countries.
Methods
We searched the PubMed database for articles published between June 2010 and June 2020, website of international organizations and hand-searching references. One author reviewed studies that met pre-defined inclusion criteria, and this was cross-validated by a second reviewer, following the MOOSE guidelines. The Meta prop command of Stata (V16) was used for pooling smoking prevalence estimates. Random effects modelling, heterogeneity with subgroup analysis and publication bias was assessed.
Results
Out the 236 identified articles, 25 with full texts were eligible, and 16 were finally included in this study. The overall pooled estimate of smoking prevalence was 72.3%, 95% CI (54.8–84.7), and high heterogeneity (I2 = 99.73%). Females had a pooled prevalence 44.1% (95% CI 9.4–82.6) while males 83.3% (95% CI 72.0–92.1). The total number of prisoners combined in this study was 16,435 (ranging from 31-21,451) with age ranging from 24-43 years.
Conclusion
A relatively high smoking rate was observed among incarcerated people - higher among the male population. The study findings are useful for informing policy-makers of the existing burden of smoking in special vulnerable populations across Western Europe-and the need for comprehensive tobacco control policies in different population settings.
Background
The Global Burden of Disease (GBD) Study in 2019 estimated more than 200 million tobacco-attributable deaths worldwide over the past 30 years, and tobacco use is the second leading risk factor for premature mortality and morbidity.1,2 Recently, smoking rates have decreased in high- income countries partly due to comprehensive changes to policy-making such as a high taxation on tobacco, mass media campaigns, restrictions on tobacco sponsorship, promotion, and advertisement, and smoke-free policies.3,4 However, this overall decline in smoking rates is not equally distributed, exposing vulnerable populations, such as the incarcerated people, at greater risk of nicotine addiction 4 . Tobacco remains the most frequently used psycho-active drug among the incarcerated people - ranging from 64-90%, with variations across and within countries. 5
The health of incarcerated people remains a public health challenge because people incarcerated are at a higher risk of substance use, and prone to overall physical and mental health problem as compared to the general population.6,7 Incarcerated people are also trapped in this vicious cycle of being in prison and out in the community, and again from community to a prison setting, 7 thus influencing the background risk of a specific community. 8 The financial burden of tobacco use-both on individuals and on the national economy is well-established. A recent WHO report estimated that smoking costs the governments and the households over US$1.4 trillion globally through healthcare expenditure and lost productivity.1,9 Importantly, evidence suggests that tobacco use is three to four times higher in the incarcerated population compared to the general population5,10-14 However, there has been no meta-analysis conducted to determine the pooled estimate of recent smoking prevalence in the incarcerated population in Western Europe.
Therefore, we set out to systematically synthesize evidence on the prevalence of smoking among the incarcerated population in Western European overall, and by gender distribution, to provide a pooled estimate of smoking prevalence, for evidence-informed policy decisions.
Methods
Search Strategy
Pre-defined eligibility criteria were formulated based in a PICO format (Appendix 1). We followed the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines (Appendix II). One author (DSA) searched PubMed database for relevant articles published between 4th June 2010 and 4th June 2020. The rationale for using only PubMed database is that PubMed is a comprehensive medical database and its most widely cited. We excluded pre-prints and non-peer reviewed journal articles, which lends support to using PubMed.
Details of the full search strategy are available in Appendix III & Appendix IV. In brief, key search terms coupled with MeSH terms, were employed. Examples include, (tobacco use OR tobacco prevalence OR smoking AND incarcerat*) using the OR and AND Boolean operator. We also searched through references of systematic review conducted on worldwide prevalence. 4 We searched publicly available international organizational websites, such as the WHO, for additional information on prevalence of tobacco in the general population for comparison. For studies conducted after 2015, the recent WHO report on trends in tobacco use 15 was used, and for studies conducted before 2015, the WHO tobacco report 2015 was used, both for extracting comparison data. 16 Baseline characteristics of the selected studies are shown in Table 3.
Eligibility Criteria
Inclusion and Exclusion Criteria.

Zotero 5.0.95 software was employed for data management. Only studies that met the eligibility criteria were included in this review. A second reviewer (ZK) reviewed the eligible studies. There were no duplicates because only one comprehensive database was used. The Western European countries included are Greece, Finland, Norway, Italy, France, Switzerland, Germany, Spain, and Netherlands based on the WHO classification. The PRISMA flow diagram
17
is shown in Figure 1 PRISMA flowchart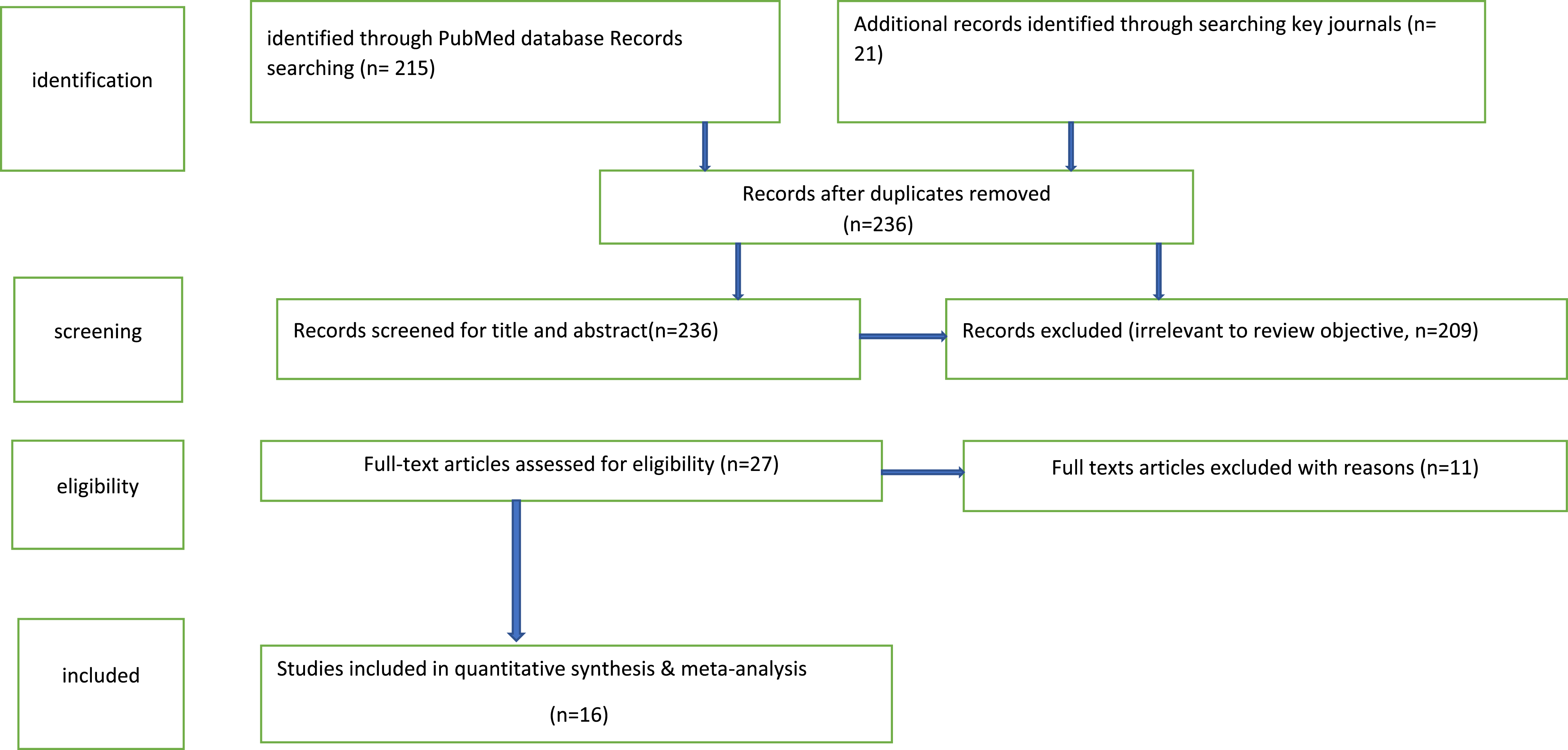
Data Abstraction
To extract data, the first reviewer (DSA) independently extracted data into a standardized data collection form. The 2nd reviewer (ZK) cross-checked this to minimize bias. However, any discrepancy was resolved through discussion. Information extracted include author’s name & year, study design, region of study, age, sex, purpose, sample size, smoking prevalence of incarcerated population, smoking prevalence of general population, fold increase, list of confounders and intervention type.
Bias and Quality Assessment
Quality assessment summary of all studies included in the review

Statistical Analysis and Meta-Analysis
Meta-analysis was undertaken for the pooled estimate on the prevalence of tobacco use among people in incarceration in Western Europe. Stata (version 16) was used for this pooled analysis, and the
Characteristics of Studies included on tobacc

AbbreviationCOPD- Chronic Obstructive Pulmonary Disorder
Smoking prevalence of prisoners- gotten from each study
General population prevalence- obtained from WHO tobacco report 2015(24) and WHO report in trend in tobacco use 2019 20
Fold Increase: obtained by dividing prevalence of prisoners by prevalence of general population
Results
Search Results
Our initial search yielded a total of 236 articles in PubMed and additional records (hand searching reference list, journal and WHO data). After screening the titles and abstracts, 211 studies were excluded, and 25 full-text studies were eligible. A total of 16 articles finally met the inclusion criteria.
Reasons for excluding full text eligible studies are shown in appendix VII. The NIH tool was applied to demonstrate that nine studies were rated as ‘good’, seven were rated as ‘fair’, and only one was rated being poor as outlined in Table 2. All the studies included for this review were cross sectional except for Hiscock et al., 36 which was a retrospective cohort study.
Result of the Meta-Analysis
Prevalence of Tobacco Use
The overall pooled prevalence of tobacco use among incarcerated people was 72.3% (95%CI 57.8-84.7) with a large heterogeneity (I2 99.73%, P=.00) (Figure 2). One study Vera-Remartínez (2014) (33) was included twice in the meta-analysis because the study reported the prevalence of tobacco use among male and female incarcerated persons, separately. The total number of participants who took part in the 16 studies were 16,435 but the overall population was 21,451 (Table 3). Out of the 9 countries included in our study, there was not any prevalence of tobacco use among people incarcerated lesser than the prevalence in the general population. The fold increase across these countries ranged from 1.36-4.76, suggesting the widening gap of tobacco use among the incarcerated population. Greece and Italy had the highest pooled prevalence of 100%, Norway 97.7%, Finland 90.9%, Spain (only male) 87.4%, France and Netherlands ranging 50.1–65.7 and three countries showed a pooled prevalence <50% which are Germany, Switzerland, Finland, and Spain (only female). Forest plot of pooled prevalence of tobacco use among prisoners in Western Europe included in the meta-analysis.
Subgroup-Analysis
Study quality: stu dies were grouped as “good, fair and poor” based on the NIH quality appraisal tool assessment. “Good” quality studies yielded a pooled smoking estimate of 89.0% (95% CI 75.0-97.8) with significant heterogeneity (I2 99.4%, P = .00); “fair” quality studies had a pooled smoking estimate of 52.2% (95% CI 25.3–78.5), with significant heterogeneity (I2 99.8%, P = .00). The pooled smoking estimate of “poor” quality studies (one study) was 25.8% (95% CI 18.8–34.3) with no heterogeneity. The forest plot is shown in Figure 3. Subgroup analysis by study quality on the prevalence of tobacco use among prisoners in western Europe.
Gender: gender was categorized into three: males, females, and both. In the meta-analysis, 7 studies included both genders, 4 studies reporting female rates, and 6 reporting male rates. The pooled smoking estimate for studies with no gender distinction was 76.9% (95% CI 51.8–94.6), with significant heterogeneity (I2 99.7%, P = .00); pooled smoking estimate for studies on females only was 44.1% (95% CI 9.4–82.6) with significant heterogeneity (I2 99.7%, P = .00); the pooled smoking estimate for studies on males only was 83.3% (95% CI 72.0–92.1), with significant heterogeneity (I2 99.0%, P = .00). The forest plot is shown in Figure 4. Subgroup analysis by gender on the prevalence of tobacco use among prisoners in western Europe.
Publication Bias
We assessed for publication bias, and the P-value after conducting Egger’s test was not significant suggesting no publication bias (Egger’s test P = .76). No study was imputed when the meta trim fill command was used. By visually looking at the funnel plot, the funnel plot was symmetrical, which shows that there is no evidence of small studies effect. This funnel plot is shown in Figure 5. Meta-regression was conducted by plotting a bubble plot to explore heterogeneity and to check if there was an association between the population prevalence (effect estimate) and sample size. The P-value was .53 suggesting no evidence of an association between population prevalence and sample size. Funnel plot on the prevalence of tobacco use among prisoners in western Europe.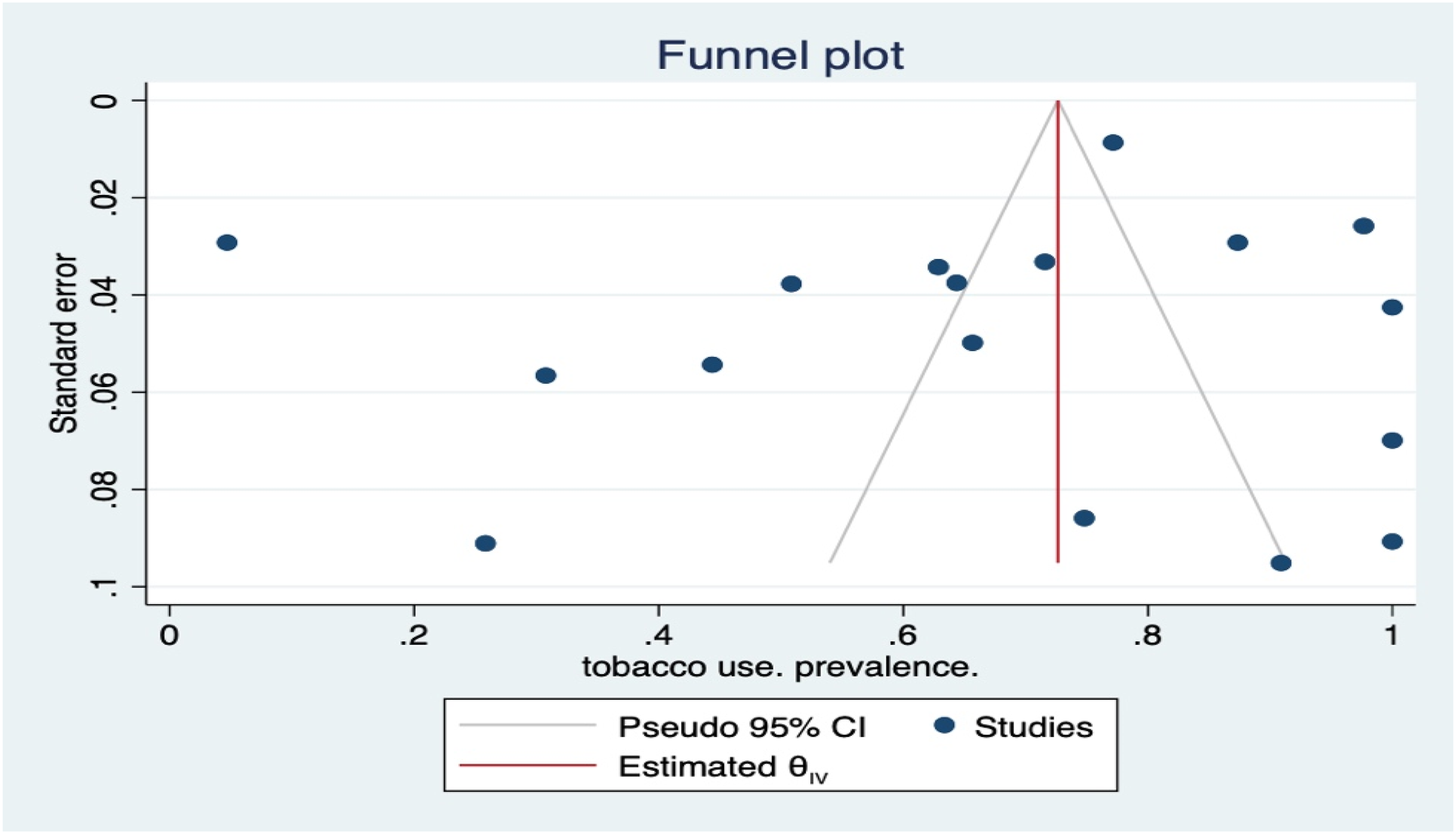
Discussion
The primary aim of this study was to synthesize evidence on the prevalence of tobacco use among incarcerated population in Western Europe. The pooled estimate of smoking prevalence was 72.3%; 95% CI (54.8–84.7). Male incarcerated population had two-fold increased prevalence of tobacco use compared to their female counterparts (44.1%). The fold increase ranged from 1.36–4.76 as there was no country which had a higher prevalence of tobacco use in the general population than in the prison population. To the best of our knowledge, this is the first study to estimate an overall pooled prevalence of tobacco use among people in incarceration, particularly in Western Europe. A recent systematic review reported on the prevalence of smoking in correctional facilities, but it was on a global scale-not limited to Western Europe and did not estimate a pooled smoking prevalence. 4 By using reports on tobacco trends from WHO data, we could make comparisons between tobacco use among general population and tobacco use among people incarcerated. Nine countries from Western Europe were included in this study with Greece and Italy reported the highest smoking prevalence of 100%. Norway 97.7%, Finland 90.9%, Spain, the Netherlands, and France reported a smoking prevalence ranging from 50.1%-87.4%. Switzerland, Germany, Finland, and Spain reported a prevalence of <50.
One major finding about this study is that the male had a two-fold increased prevalence of tobacco use (83.26%) compared to the females (44.06%). However, a study conducted among female incarcerated in Greece reported that female incarcerated are at higher risk of smoking, using drugs and alcohol, reproductive health, and mental health than male and even the general population.7,11 The large difference in gender prevalence could be because of the dearth of studies on female incarceration. Moreover, the population of the male incarcerated are 90% or more and generally, women make up approximately 7% of the incarceration rate worldwide. 11
Our findings are in agreement with published literature11,19,20 demonstrating that the prevalence of tobacco use is heightened among people incarcerated compared to the general population. Another recent systematic review looked at the prevalence of alcohol and substance use disorder among people in incarceration but tobacco use was exempted. 14 This worldwide study carried out a meta-analysis and the pooled prevalence for alcohol was 24% with male prevalence slightly higher than female, while for drug use male had overall prevalence of 30% and female 51%. 14 The prevalence of alcohol use higher in males than in females lend support to our findings whereby tobacco use is higher in males than in females but the prevalence of drug use was higher in female than in male. To put into perspective, comparing these three substances (alcohol, drug and tobacco), tobacco use in the incarcerated population is the most prevalent.
Strengths and Limitations
Our study has both strengths and limitations. A strength of our study is an overall pooled estimate on the prevalence of tobacco among Western Europe incarcerated population, which is novel to the best of our knowledge. We demonstrated no evidence of publication bias across the studies included. Another strength is that the meta-regression conducted for these studies showed that there was no association between prevalence and sample size, indicating validity of our study findings.
One of the major limitations is the use of a single database with date restrictions of 2010-2020. However, PubMed database is a comprehensive medical database and is widely cited. Also, some studies had small sample size and data was extracted from them, and even studies in which smoking was not the primary outcome were included in the study. Therefore, there should be cautiousness in interpretation because not all these incarcerated populations be generalizable to the whole incarcerated populations of a particular country. There was not much data on the female incarceration because of relatively fewer female incarcerated. Also, there was insufficient data on the average number of cigarettes smoked and the type of tobacco products. This study only focused on Western Europe, and even though a systematic review on this topic has been done worldwide, no pooled estimate of smoking was undertaken. 4 Despite these limitations, our study findings can help inform policy targeting people in incarceration, especially in Western Europe.
Conclusion
Our systematic review showed a very high prevalence of tobacco use among people incarcerated in Western Europe. The findings can inform policy makers and decision practitioners to consider gender-specific, comprehensive tobacco control policies across all Western European countries, targeting this vulnerable population. There is a need to shift focus on the incarcerated population for tobacco control interventions akin to improvements in smoking rates among the general population in Western Europe.
Footnotes
Appendix I. The pico.
Population
Prisoners
Exposure
Tobacco use–this can be in form of smoked tobacco, smokeless tobacco (dissolvable), waterpipe tobacco, cigars, cigarettes and electronic cigarette.
Comparison
General population–other population different from those in prison.
Outcome
Smoking prevalence(primary), effectiveness of tobacco control policies (secondary).
Appendix II. MOOSE Guidelines for Meta-Analyses and Systematic Reviews of Observational Studies*
*Modified from Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000;283:2008-12.
Topic
Page number
Title
Identify the study as a meta-analysis (or systematic review)
1
Abstract
Use the journal’s structured format
1
Introduction
Present:
1
The clinical problem
1
The hypothesis
1
A statement of objectives that includes the study population, the condition of interest, the exposure or intervention, and the outcome(s) considered
15
Sources
Describe:
Qualifications of searchers (e.g., librarians and investigators)
1
Search strategy, including time period included in the synthesis and keywords
1, 2
Effort to include all available studies, including contact with authors
3
Databases and registries searched
1
Search software used, name and version, including special features used (e.g. explosion)
1
Use of hand searching (e.g., reference lists of obtained articles)
2
List of citations located and those excluded, including justification
2, 22
Method of addressing articles published in languages other than English
n/a
Method of handling abstracts and unpublished studies
n/a
Description of any contact with authors
3
Study Selection
Describe
Types of study designs considered
2
Relevance or appropriateness of studies gathered for assessing the hypothesis to be tested
Rationale for the selection and coding of data (e.g., sound clinical principles or convenience)
n/a
Documentation of how data were classified and coded (eg, multiple raters, blinding, and inter-rater reliability)
n/a
Assessment of confounding (e.g. comparability of cases and controls in studies where appropriate)
n/a
Assessment of study quality, including blinding of quality assessors; stratification or regression on possible predictors of study results
n/a
Assessment of heterogeneity
3
Statistical methods (e.g., complete description of fixed or random effects models, justification of whether the chosen models account for predictors of study results, dose-response models, or cumulative meta-analysis) in sufficient detail to be replicated
3
Results
Present
A graph summarizing individual study estimates and the overall estimate
9
A table giving descriptive information for each included study
4-6
Results of sensitivity testing (e.g., subgroup analysis)
9, 10
Indication of statistical uncertainty of findings
—
Discussion
Discuss
Strengths and weaknesses
11
Potential biases in the review process (e.g., publication bias)
9
Assessment of quality of included studies
7
Consideration of alternative explanations for observed results
—
Generalization of the conclusions (i.e., appropriate for the data presented and within the domain of the literature review)
11
Guidelines for future research
—
Disclosure of funding source
1
Appendix III. Search Strategy-4th of June 2020 (sort by most recent,filter by abstract,free full text,in the last 10 years,humans,English)
Search number
Query
Results
Time
39
((((((((((tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter]) AND (2010:2020[pdat]))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco consumption AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco smoking prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar*smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar* smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((((((((((prisoner* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (smoke-free prison AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional setting AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional facilities AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (incarcerat* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (detainees AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (internee AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (socially disadvantaged AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (marginalized AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (vulnerable AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND (((((((((((tobacco policy AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (tobacco control AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco use cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco program* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking intervention AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking compliance AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation*, tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smokeless tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation, smokeless tobacco AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND (((Europe) OR (EU)) OR (Western Europe) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))
215
17:26:19
38
((Europe) OR (EU)) OR (Western Europe)
118,914
17:19:11
37
(((((((((tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter]) AND (2010:2020[pdat]))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco consumption AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco smoking prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar*smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar* smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((((((((((prisoner* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (smoke-free prison AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional setting AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional facilities AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (incarcerat* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (detainees AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (internee AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (socially disadvantaged AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (marginalized AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (vulnerable AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND (((((((((((tobacco policy AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (tobacco control AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco use cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco program* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking intervention AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking compliance AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation*, tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smokeless tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation, smokeless tobacco AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) (smoking cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation*, tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smokeless tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation, smokeless tobacco AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) (smoking cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation*, tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smokeless tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation, smokeless tobacco AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))
1223
17:17:08
36
((((((((((tobacco policy AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (tobacco control AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco use cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco program* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking intervention AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking compliance AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smoking cessation AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation*, tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (smokeless tobacco cessation* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cessation, smokeless tobacco AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))
38,618
17:16:27
35
((((((((tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter]) AND (2010:2020[pdat]))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco consumption AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco smoking prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar*smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar* smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((((((((((prisoner* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (smoke-free prison AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional setting AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional facilities AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (incarcerat* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (detainees AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (internee AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (socially disadvantaged AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (marginalized AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (vulnerable AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))
28,977
17:14:33
34
(((((((((prisoner* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter]))) OR (smoke-free prison AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional setting AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (correctional facilities AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (incarcerat* AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (detainees AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (internee AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (socially disadvantaged AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (marginalized AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (vulnerable AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))
28,977
17:13:03
33
(((((((tobacco use AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter]) AND (2010:2020[pdat]))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco chewing AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco consumption AND ((ffrft[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (tobacco smoking prevalence AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar*smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))) OR (cigar* smoking AND ((ffrft[Filter]) AND (fha[Filter]) AND (y_10[Filter]) AND (humans[Filter]) AND (english[Filter])))
1,842,706
17:03:42
32
cessation, smokeless tobacco
5297
17:01:35
31
smokeless tobacco cessation*
240
17:00:56
30
tobacco cessation*
5297
16:59:51
29
cessation*, tobacco use
5371
16:59:30
28
smoking cessation
8294
16:58:37
27
smoking compliance
1046
16:56:16
26
smoking intervention
33,675
16:56:04
25
tobacco program*
3170
16:55:47
24
tobacco use cessation
5297
16:55:31
23
tobacco control
6902
16:55:16
22
tobacco policy
3714
16:55:06
21
vulnerable
23,270
16:54:48
20
marginalized
1145
16:54:35
19
socially disadvantaged
3960
16:54:25
18
internee
7
16:53:56
17
detainees
102
16:53:42
16
incarcerat*
1726
16:53:17
15
correctional facilities
216
16:52:51
14
correctional setting
149
16:52:31
13
smoke-free prison
19
16:51:27
12
prisoner*
1920
16:50:55
11
cigar* smoking
11,154
16:50:30
10
cigar*smoking
9
tobacco smoking prevalence
7612
16:50:07
7
tobacco prevalence
9887
16:48:42
6
tobacco consumption
18,376
16:48:27
5
tobacco consumption
26,121
16:48:19
3
tobacco chewing
26,121
16:46:26
4
tobacco chewing
18,376
16:46:10
2
tobacco use
18,942
16:44:36
1
tobacco use
26,121
16:44:02
Appendix IV. Additional Studies Obtained
Because of our eligibility criteria which stated that already conducted review would not be included in this study, the references of an already conducted systematic review on the worldwide prevalence of tobacco use by Anne et al. in 2018 4 was searched, and we obtained an additional 9 articles of which two got excluded as they did not meet the criteria.
In addition to this, WHO report on trends in tobacco use 2019, the European region was also searched to get comparison data on tobacco prevalence among the general population for studies after 2015 (29) and WHO Tobacco Report 2015 was used for comparison data for studies before 2015.(24) Reported smoking prevalence was compared with the general population based on the country being looked at. The 2015 report had four indicators, and the years were divided by interval of five years 2000, 2005, 2010, 2015, 2020, 2025.(24) For any study conducted by the year 2015 and below, this report was used and the study year closest in a forward direction to any of the aforementioned years was used. The point estimate of current smoking trends of both sexes aged 15 and above was the indicator displayed in the table below during the extraction of data for this review. In contrast, for the 2019 report,(29) there were only two indicators used in this report which are current smoking and daily smoking because of the availability of data. However, for the purpose of this review, the author used data on current smoking by looking at the graph in the report showing the overall age-standardized estimate and giving a sense of precise estimate. It is also of importance to know that for mixed studies; meaning studies that had both sexes, the point estimate of both sexes calculated in the report already was used while for gender-specific studies, the point estimate of that particular sex was used.
Appendix V. NIH Quality Appraisal For Included Studies
Criteria: 1. Was the research question or objective in this paper clearly stated? 2. Was the study population clearly specified and defined? 3. Was the participation rate of eligible persons at least 50%? 4. Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? 5. Was a sample size justification, power description, or variance and effect estimates provided? 6. For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? 7. Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? 8. For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)? 9. Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? 10. Was the exposure(s) assessed more than once over time? 11. Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? 12. Were the outcome assessors blinded to the exposure status of participants? 13. Was loss to follow-up after baseline 20% or less? 14. Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?

STUDY AUTHORS
1
2
3
4
5
6
7
8
9
10
11
12
13
14
a. Bania et al. 2016
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
b. Vainnionpaa et al. 2019
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
c. Geiotona and Miloni 2016
Yes
Yes
Yes
Yes
No
No
No
Yes
No
No
No
Other
Other
No
d. Muller et al. 2018
Yes
Yes
Yes
Yes
No
No
No
Yes
Other
No
No
Other
Other
Yes
e. Lind et al. 2015
Yes
Yes
No
Yes
No
No
No
Yes
Yes
No
Yes
Yes
Other
No
f. Nobile et al. 2011
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
g. Hiscock et al. 2013
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
No
Yes
Yes
No
Yes
h. Makris et al. 2012
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
i. Etter et al. 2012
Yes
Yes
No
No
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
j. Jayes et al. 2019
Yes
Yes
Other
Other
Other
Other
Yes
Yes
Yes
Yes
Yes
No
Other
No
k. Semple et al. 2020
Yes
Yes
Other
Other
Other
Other
Yes
Yes
Yes
Yes
Yes
Other
Other
No
l. Jacomet et al. 2016
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
No
m. Celeen et al. 2012
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
n. Chariot et al. 2014
Yes
Yes
Yes
Yes
No
No
Yes
Yes
Yes
No
Yes
Other
Other
No
o. Mannociet al. 2015
Yes
Yes
Yes
Yes
No
No
Yes
Yes
Yes
Yes
Yes
Other
Other
Yes
p. Vera-Remartínez (2014)
Yes
Yes
Yes
Yes
Yes
No
No
Yes
Yes
No
Yes
Other
Other
No
q. Ritter and Elger 2013
Yes
Yes
No
No
No
No
No
Yes
Yes
No
Yes
Other
Other
No
r. Mir et al. 2015
Yes
Yes
Yes
Yes
No
No
Yes
Yes
Yes
No
Yes
Other
Other
No
s. Sahajian et al. 2012
Yes
Yes
Yes
Yes
No
No
Yes
Yes
Yes
Yes
Yes
Other
Other
Yes
t. Sahajian et al. 2017
Yes
Yes
Yes
Yes
No
No
No
Yes
Yes
No
Yes
Other
Other
Yes
Appendix VI. Metaprop command for pooled estimate of smoking prevalence
study
studyquality
country
gender
age
N
n
prisoners
genpop
Bania et al. 2016
good
Greece
mixed
43
552
552
79
44
Vainionpaa et al. 2019
good
Finland
mixed
35
110
100
88
18.5
Geitona and Milioni 2016
fair
Greece
female
37.5
135
101
83.8
30.8
Muller et al. 2018
good
Norway
mixed
32.8
1499
1464
81.3
21.6
Lind et al. 2019
fair
Finland
mixed
37.3
312
96
84
20.2
Nobile et al. 2011
good
Italy
male
39.8
908
650
67.5
30.8
Jacomet et al. 2016
fair
France
mixed
30
702
357
83.8
24.7
Ceelen et al. 2012
good
Netherlands
mixed
41
402
264
76
26.7
Chariot et al. 2014
fair
France
male
24
13317
10276
70
27.9
Makris et al. 2012
good
Greece
male
33.6
204
204
75.5
55.7
Mannocci et al. 2015
good
Italy
male
35
121
121
69.7
29
Vera-Remartinez et al. 2014
fair
Spain
male
37.4
1170
1022
71
29.9
Vera-Remartinez et al. 2014
fair
Spain
female
37.4
1170
55
58.2
22.3
Ritter and Elger 2013
poor
Switzerland
male
35
120
31
84
27.9
Mir et al. 2015
fair
Germany
female
34.3
338
150
81
23.3
Sahajian et al. 2012
good
France
female
31.5
851
535
57.9
22.6
Sahajian et al. 2017
good
France
mixed
31.6
710
457
74.4
24.7
Appensix VII. Reasons for excluding eligible studies
Study Author
Reasons for exclusion
1. Semple et al. 2017 (50)
This study focused only on nicotine concentration affecting prison staffs.
2. Jaka et al. 2014(51)
Though the study was on the prevalence of tobacco used but it was in Albania which is not in western Europe(the review’s target population).
3. Brown et al. 2019(42)
Opinions about prisoners and prison staff view on smoking ban.
4. Jayes et al. 2016(52)
Nothing on prevalence as it only portrayed particulate matter concentration in four English prisons.
5. McCaffrey et al. 2012(45)
Study was on exposure of prison staff to environmental tobacco smoke and opinions on whether there should
be a complete smoking ban. Although in the study discussion, prevalence of smoking in a 2000was mentioned to reference a point.
6. Robinson et al. 2018(53)
Thematic analysis.
7. Moffat et al. 2019(54)
Focused on prevalence of chronic oedema (CO) and wound in two vulnerable population.
8. Sweeting et al. 2019(55)
This study was on different structure of opinions with respect to prison smoking bans.
9. Caravaca-Sanchez et al. 2015(56)
Full text not in English; it was in Spanish.
10. Carnie and Broderick 2015(57)
Didn’t fit to eligibility criteria because it was a survey report.
11. Pinto et al. 2015(58)
Full text wasn’t open access as it was asking for authorization. Author tried accessing with the institution interlibrary loan access but access was denied.
DECLARATION OF CONFLICTING INTERESTS:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING:
The author(s) received no financial support for the research, authorship, and/or publication of this article.