
Abstract
While the poor and the uninsured are at increased risk for tobacco use, up to two thirds of these patients express interest in near-term quitting. Nonetheless, tobacco counseling rates remain low in clinics serving these patients. As part of a larger tobacco intervention project in North Carolina free clinics, we gathered baseline data on patient characteristics in six randomly selected facilities affiliated with the North Carolina Association of Free Clinics. An exit interview was completed by 231 patients; 126 (54%) were tobacco users. Among all patients, 71% had been asked by a clinician about tobacco use in the past 3 months. Among tobacco users, 68% had received at least one other counseling step (assessment; advice; or assistance). Patients with asthma and current tobacco users had a two-fold increase in being asked about tobacco use. Patients' diagnoses–-in particular asthma–-can remind clinicians of tobacco intervention.
Introduction
Minorities, the poor and the uninsured are at increased risk for tobacco use compared to their majority counterparts. 1 For the same levels of tobacco use, these populations also suffer a greater burden of tobacco-related morbidity and mortality. 1 Furthermore minorities, the poor and those with low education attainment receive tobacco cessation assistance less frequently then their more advantaged peers.2–5 This lack of tobacco intervention occurs despite the fact that up to two thirds of medically underserved patients express interest in quitting within the next six months.6,7 Indeed when offered smoking cessation education materials, 61% of smokers in a clinic for the medically underserved availed themselves of these resources. 8
Because many of these patients without medical insurance cannot afford medical treatment in other settings, free clinics have been established to attend to these needs.9–11 Here we report baseline analysis of predictors of clinicians' counseling (Ask, Assess, Advise and Assist) over the past 3 months in six free clinics for the uninsured across the state of North Carolina at the beginning of a clinic-based tobacco intervention in these locations. This project was approved by the Institutional Review Boards of Wake Forest School of Medicine and Davidson College.
Methods
Clinic Selection
Among the 74 free clinics which are members of the North Carolina Association of Free Clinics, we identified 13 clinics meeting the following eligibility criteria to participate in a clinic-based tobacco intervention: being within 3 hour driving distance to the research team; being open at least 2 days per week; providing medical and/or dental care; and not providing comprehensive tobacco services as defined by the US Public Health Service Tobacco Treatment Guidelines. 1 One clinic declined to participate. Six of the remaining 12 clinics were randomly selected–-three intervention clinics and three delayed intervention clinics.
Data Collection
Before the intervention, we gathered patient baseline data by exit interviews about the demographics, medical history, and reason for today's visit after participants' health care appointments. We also queried patients about clinicians' provision of the tobacco cessation counseling: Ask: “During the past 3 months, did any doctor, nurse, or other health professional ask if you use tobacco, including cigarettes, snuff or other types of tobacco?”; Assess: “Ask if you were willing to quit?”; Advise: “Advise you to quit using tobacco?”; Assist: “Prescribe or recommend any kind of medicine to help you quit, such as Zyban, Wellbutrin, Chantix, nicotine gum, nasal spray, nicotine patch? help you set a specific date to stop using tobacco? suggest you go to a class about quitting, call a quit line, or seek counseling to help you quit? provide you with booklets, brochures, or other materials to help you quit?” Institutional review board approval was obtained for this study, and all participants signed informed consent agreements.
Statistical Analysis
Descriptive, bivariate and multivariable logistic regression analyses were performed evaluating prevalence and predictors of clinicians' counseling. To assess predictors of clinicians' counseling, we employed a two-step procedure and repeated this process for each outcome, being asked for the entire sample of participants and the remaining 3 steps (advised, assessed, and assisted) for the sub-sample of current tobacco users. In the first step, we examined bivariate associations between each risk factor and the outcome variable. Variables with P < 0.10 in our bivariate analysis were entered into the multivariable models. Since patients within a free clinic are likely to be more like one another than they are to be like patients in other free clinics, 12 we used a random-effects logistic regression model with adaptive Gaussian quadrature in SAS PROC GLIMMIX Version 9.2 to account for within-clinic correlation.
Results
Sample characteristics.

P-value from chi-square statistic.
Importantly, 71% of patients had been asked by a clinician about tobacco use in the past 3 months. Demographic characteristics, reason for today's visit, and diagnoses were not associated with being asked about smoking status except for patients with asthma and heart disease, 83% and 100% of whom were asked within the past three months (P < 0.03 and P < 0.004 respectively) (Table 1).
Of the 126 tobacco users, 67.5% had received at least one of the remaining counseling steps (advised, assessed, and assisted). In particular, 62% had been advised to quit; 43% had been assessed for their willingness to quit; and 35% had been assisted in their quit attempt. The following variables were included in the multivariable model for being asked about tobacco use: asthma, diabetes, age and current tobacco user. In multivariable logistic regression modeling among all participants (Table 2), patients with asthma were 2.30 times (P = 0.04) more likely to be asked in the past 3 months if they used tobacco, and current tobacco users were 2.10 (P = 0.02) times more likely to be asked when compared to their non-asthmatic and non-current user counterparts, respectively. There were no significant predictors for patients receiving one of the remaining 3 counseling steps (beyond being asked) in bivariate analysis, so no multivariable analysis was performed.
Multivariable logistic regressing analysis * (outcome variable: being asked), N = 227.
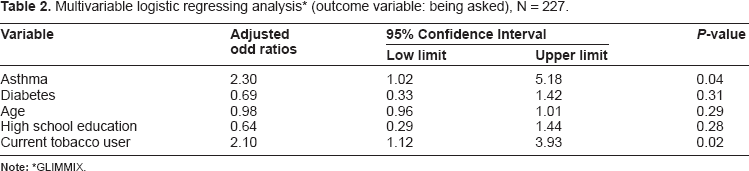
GLIMMIX.
Discussion
In this sample of patients receiving health care at six free clinics in North Carolina, 54% used tobacco, over twice the prevalence (20.6%) among adults nationally. 13 Only 71% of all patients had been asked by a health care provider in the past 3 months if they used tobacco. This rate varies little from the 67% identification of smoking status by physicians nationally two decades ago, 14 indicating the need for progress to reach 100% tobacco status ascertainment of every patient at every visit. Additionally, our finding of a 62% rate of tobacco advice given smokers in past 3 months is on par with that reported nationally among African Americans (61%) but higher than that reported among Hispanics (50%).2,15 While the current study indicates that tobacco counseling in free clinics is “no worse” than that reported nationally, every patient at every clinic visit should be asked if they use tobacco. Additionally, advising tobacco-using patients to quit, assessing readiness to quit, assisting in setting a quit plan and/or providing pharmacotherapy dropped off in this study. These findings highlight the need for clinicians to go beyond merely asking about tobacco use.
Barriers exist to the delivery of tobacco intervention in low-income clinics. These include lack of time during an encounter, patients not being currently motivated to quit, inadequate patient financial resources, inadequate clinic resources such as printed materials, and inadequate clinician training in cessation intervention skills. 16 An additional barrier is the fact that homeless patients have high rates of tobacco use and co-morbid psychiatric disease, making intervention in this population particularly challenging.7,17–19 This is because tobacco is often used to self-medicate an individual's psychiatric symptoms. 19 These patients also have high rates of substance abuse besides tobacco and poly-substance abuse is a challenging situation in which to intervene to accomplish tobacco cessation.1,18,19
Despite barriers in such clinics, Pendleton et al. show that when low income patients are offered smoking cessation education delivered by electronic kiosks in waiting rooms, 61% of smokers take advantage of this resource. 8 Patients who accessed the kiosk information varied by race (61% white), diagnosis (range: 2.6% of patients with cancer to 30.2% of patients with obesity), education (56% with high school education) and gender (56% female). In contrast to our study, fewer patients with “lung” disease (14%) accessed this information. These differences are likely explained by differing methods between the two studies, e.g., an intervention (kiosk) versus our baseline survey. Regardless, these researchers show that there is interest among low income patients in tobacco cessation education. 8
Pendleton et al. also review barriers unique to low income clinics relying on volunteer clinicians. 8 As in the free clinics which we studied, these volunteers often represent multiple specialities and might not view tobacco intervention within their purview. Volunteers also typically spend limited time in clinics, and might not become accustomed to a clinic's “culture” of prevention. Further-more, patients often present with multiple medical problems and usually will not see the same provider in follow up. These factors might make an individual clinician less likely to provide preventive care including smoking cessation advice. Pendleton et al. conclude that “[i]ncreasing patient-provider discussions and providing appropriate patient education materials are necessary first steps to increasing healthy behaviours.” 8
Although medically underserved patients are interested in quitting tobacco use,6,7 and access tobacco cessation materials when offered, 8 the provision of counselling based on patient factors has not been evaluated in free clinic populations. This is despite the fact that brief interventions have been shown to increase tobacco cessation, 1 and thus is especially important in a population at high risk for tobacco-related diseases.
Conclusions
Although our findings are limited by the small sample size and pilot nature of this project, it is clear more work needs to be done in delivering tobacco counselling by providers in free clinic settings. Lessons from the current study indicate that clinician focus on patients' diagnoses–-in particular asthma–-can serve as a trigger to remind clinicians of tobacco intervention. Research is needed to point out methods that work best among low-income populations without health insurance such as having a tobacco champion at each clinic, provision of patient resources, and provider/volunteer training in tobacco intervention.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Author Contributions
Conceived and designed the experiments: KLF, ELS, JGS, EYS, CJ, DH. Analysed the data: EYS, JGS. Wrote the first draft of the manuscript: JGS. Contributed to the writing of the manuscript: JGS, EYS, JRP, ELS, DH, KLF. Agree with manuscript results and conclusions: JGS, EYS, JRP, ELS, DH, CJ, KLF. Jointly developed the structure and arguments for the paper: JGS, EYS, JRP, ELS, DH, CJ, KLF. Made critical revisions and approved final version: JGS, EYS, JRP, ELS, DH, CJ, KLF. All authors reviewed and approved of the final manuscript. JGS, EYS, JRP, ELS, DH, CJ, KLF.
Footnotes
Acknowledgement
This publication was supported by NCI 1 R21 DA024631-01 Implementation and Dissemination of Tobacco Cessation Strategies in Free Clinics.
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.