
Abstract
Objectives:
We assessed whether social inequalities in smoking observed among young adults born in Canada were also apparent in same-age immigrants.
Methods:
Data were drawn from an investigation of social inequalities in smoking conducted in an urban setting (Montreal, Canada). The sample included 2077 young adults age 18 to 25 (56.6% female; 18.9% immigrants who had lived in Canada 11.6 (SD 6.4) years on average). The association between education and current smoking was examined in multivariable logistic regression analyses conducted separately in young adults born in Canada and in immigrants.
Results:
About 19.5% of immigrants were current smokers compared to 23.8% of young adults born in Canada. In immigrants, relative to those with university education, the adjusted odds ratios (OR) (95% confidence interval) for current smoking were 1.2 (0.6, 2.3) among those with pre-university/vocational training and 1.5 (0.7, 2.9) among those with high school education. In non-immigrants, the adjusted ORs were 1.9 (1.4, 2.5) among those with pre-university/vocational training and 4.0 (2.9, 5.5) among those with high school.
Conclusion:
Young adults who had immigrated to Canada did not manifest the strong social gradient in smoking apparent in young adults born in Canada. Increased understanding of the underpinnings of this difference could inform development of interventions that aim to reduce social inequalities in smoking.
Introduction
Tobacco use accounts for half the difference in life expectancy across groups with low and high socioeconomic status (SES). 1 Although the prevalence of cigarette smoking has declined in the last several decades, studies in Western countries including Canada show an enduring social gradient in smoking.2-4 Further, a recent review suggests that tobacco control interventions have unequal effects on smoking behavior across social strata. 5 Reducing health inequalities in tobacco use is an imperative and public health programs and policies targeting smoking should be designed with attention to reducing these inequalities.
Young adulthood is increasingly viewed as a vulnerable period in the life course due to the dynamic changes in education, employment and housing that characterize the transition from adolescence to adulthood. 6 In Canada, young adults ages 18 to 34 have the highest prevalence of smoking (19.2% in 2019) across all age groups 7 and unlike other age groups, smoking initiation in young adults has not decreased over the last decade. 8 Smoking behavior also differs in young adults. Hammond 9 for example, reported that smokers ages 18 to 29 smoke fewer cigarettes per day and were more likely to be occasional smokers than older adults. During this period in the life course, the combined effects of family background, social deprivation and multiple life transitions could contribute to smoking rates becoming increasingly stratified by SES, 10 adding impetus to studying young adult smokers as a unique and important group.
Because immigrants account for over 20% of the population in Canada, immigrant status could represent another important underpinning of social inequalities in smoking. 11 Immigrants are defined herein as persons currently residing in Canada (including permanent residents and people who obtained Canadian citizenship by naturalization) who were born outside Canada. 12 Immigrants are sometimes viewed as a “vulnerable population,” 13 with the assumption that they are at higher risk of multiple health issues because of limited access to resources and programs that allow the promotion and maintenance of good health. 10 On the other hand, there is a considerable literature on the “Healthy Immigrant Effect” (HIE), which posits that immigrants are healthier than Canada-born individuals on arrival in their new host country. 11 This health advantage, however, may decrease over time and across generations as immigrant health status tends to converge toward that of their Canada-born counterparts. 14
In concert with the HIE, there is evidence that fewer immigrants smoke compared to their Canada-born counterparts.15-17 Street 18 reported that both recent and older-established immigrants in the province of Québec are less likely to smoke than Canada-born adults (14%-16% vs 21%), and O’Loughlin et al 19 reported that smoking prevalence was lower among immigrant than Canada-born children (15% vs 24%) but increased with number of years spent in Canada.
Although the prevalence of smoking may be lower overall among immigrants, it is not known whether social inequalities in smoking affect immigrants in the same way as non-immigrants. Increased understanding of whether there is a social gradient in smoking among immigrants could inform the development of preventive interventions that take immigrant status into account. This current study investigates whether the social gradient in smoking apparent in Canada-born young adults manifests in same-age young adults who have experienced immigration. The specific objective was to assess whether the association between level of education and current smoking status differs between young adult immigrants (as a collectivity regardless of country of origin) and their non-immigrant counterparts.
Methods
Data were drawn from the baseline cycle of the Interdisciplinary Study of Inequalities in Smoking (ISIS), a longitudinal investigation that aimed to identify individual and contextual factors underpinning social inequalities in smoking in young adults in an urban context. 20 The target population was non-institutionalized persons ages 18 to 25 years, proficient in English or French, who had resided at their current address in Montréal, Canada for at least 1 year at the time of first contact. From an initial sample of 6020 persons randomly selected from among beneficiaries of Québec’s provincial health insurance program (ie, the Régie de l’assurance-maladie du Québec), 2093 were eligible for inclusion and completed the baseline questionnaire administered either online or assisted (in-person or by telephone) in 2011-2012. The baseline response proportion was 37.6%. Full details on sampling and data collection procedures are available elsewhere. 20 For this paper, analyses were restricted to participants at baseline for whom data on immigrant status were available (n = 2077). The Interdisciplinary Study of Inequalities in Smoking received ethics approval from the Commission d’accès à l’information du Québec and the Comité d’éthique de la recherche en santé de la Faculté de Médecine, Université de Montréal.
Study variables
Immigrant status was measured by: “Were you born in Canada?” Participants who responded “yes” were categorized as “non-immigrants.” Those who responded “no” were categorized as “immigrants.”
Level of education is generally accepted as an SES indicator for this age group. 21 However, many young adults are in the process of completing their studies and expected level of education better approximates later SES in young adults. 22 Level of education in this study was therefore measured as expected level of education. Specifically, we asked participants to report the highest level of schooling they had completed, with 12 response options ranging from “no schooling” to “earned doctorate” (note that in Québec, grade 11 is the last year of high school. Students then attend CEGEP (Collège d’enseignement general et professionnel) for 2 years of pre-university education or 3 years of vocational training). Current full- or part-time students and those in internship programs were asked to name the program in which they were currently enrolled, and the institution attended. If the program would eventually yield a higher level of education than the highest completed degree indicated by the participant, participants were coded according to that level (under the assumption that they would complete that program). Attained or expected level of education was categorized as: (1) high school (completed or not completed); (2) pre-university/vocational training completed; or (3) university completed.
Current smoking status was measured by asking participants whether they had smoked at least one whole cigarette in their lifetime, and whether they currently smoked “every day,” “occasionally” or “never.” Occasional and daily smokers were categorized as current smokers. Former and never smokers were categorized as non-smokers.
Covariates included age, sex (male, female) and among immigrants only, number of years since immigrating to Canada. Number of years since immigrating was measured by asking participants at what age they had immigrated to Canada and subtracting age at immigration from current age.
Data analysis
Immigrants and non-immigrants were compared using descriptive statistics. In early multivariable logistic regression analyses with smoking status as the dependent variable and controlling for age and sex, the confidence intervals for an interaction term between immigrant status and attained or expected level of education excluded 1 (OR (95% CI) = 0.59 (0.42, 0.85). Therefore, for ease of interpretation, we examined associations in analyses stratified by immigrant status. Specifically, the association between level of attained or expected education and current smoking status was estimated in multivariable logistic regression models controlling for age and sex among non-immigrants. Among immigrants, we controlled for age, sex and number of years since immigrating. Age and number of years since immigrating were used as continuous variables in the models.
Results
A total of 2077 participants, including 392 immigrants (18.9%) and 1685 non-immigrants (81.1%), completed the baseline questionnaire and were included in the analyses. Mean (SD) age was 21.5 (2.3) and 56.6% of participants were female. Immigrants were older on average than non-immigrants, a higher proportion was male and the proportion with or expected to obtain a university degree was higher (Table 1). Among immigrants, the mean (SD) number of years since immigrating was 11.6 (6.4) years (range 1-24); 52.8% had immigrated more than 10 years ago.
Sociodemographic characteristics of young adult participants according to immigrant status, Interdisciplinary Study of Inequalities in Smoking, Canada, 2011-2012.

Excludes participants missing data.
One-fifth (19.5%) of immigrants were current smokers, compared to 23.8% of non-immigrants. Although the proportion that smoked was similar in males (11.7% in immigrants vs 10.9% in non-immigrants), relatively fewer female immigrants smoked than non-immigrants (7.9% vs 12.8%). Length of time since immigrating was not associated with smoking (21.1% of those who had immigrated 1-10 years ago smoked, compared to 18.0% of those who had immigrated 11-24 years ago).
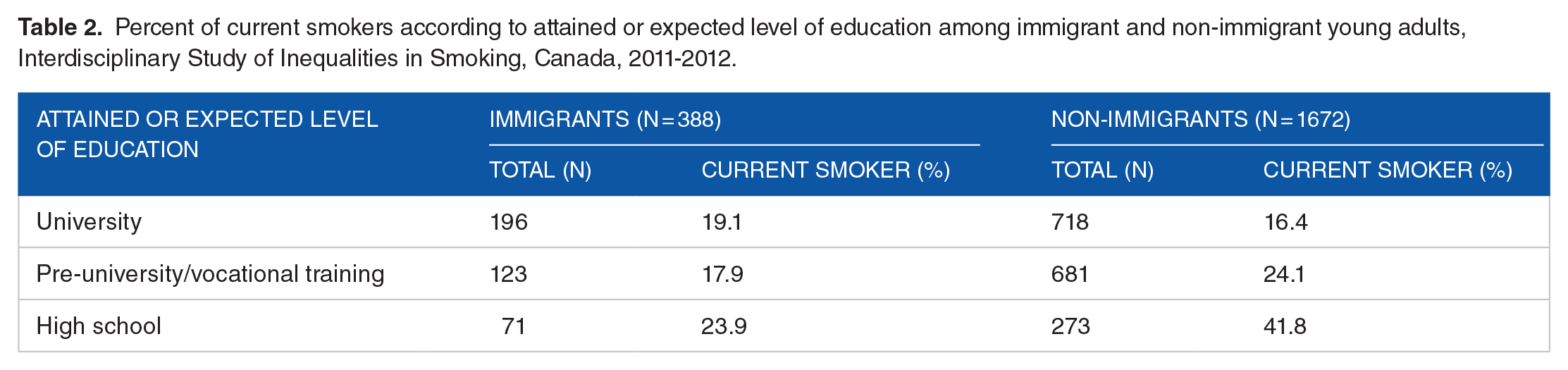
The proportion of smokers was somewhat higher among immigrants with high school education than among those who reported pre-university/vocational training or university education (Table 2). In contrast, there was an apparent dose response among non-immigrants—the proportion of current smokers declined markedly as attained or expected level of education increased.
Percent of current smokers according to attained or expected level of education among immigrant and non-immigrant young adults, Interdisciplinary Study of Inequalities in Smoking, Canada, 2011-2012.
Results of the multivariable modeling (Table 3) concurred with findings from the cross-tabulations and interaction analyses, suggesting that there was effect modification by immigrant status in the association between level of education and current smoking. The odds of current smoking were higher among immigrants with high school education relative to those who were university-educated, although the confidence intervals included 1. However, the odds of current smoking were markedly elevated among Canada-born young adults with either pre-university/vocational training or high school education relative to those who were university-educated. Our data thus support the existence of a marked social gradient in smoking among Canada-born young adults, but not among immigrants. Sensitivity analyses using a 4- rather than 3-level education variable, and with addition of an “experiencing financial difficulties” variable in the model yielded similar results (Supplemental Tables 1 and 2).
Crude and adjusted odds ratios (OR) and 95% confidence intervals (CI) for the association between attained or expected level of education and current smoking among young adult immigrants (n = 388) and same-age non-immigrants (n = 1672), Interdisciplinary Study of Inequalities in Smoking, Canada, 2011-2012.
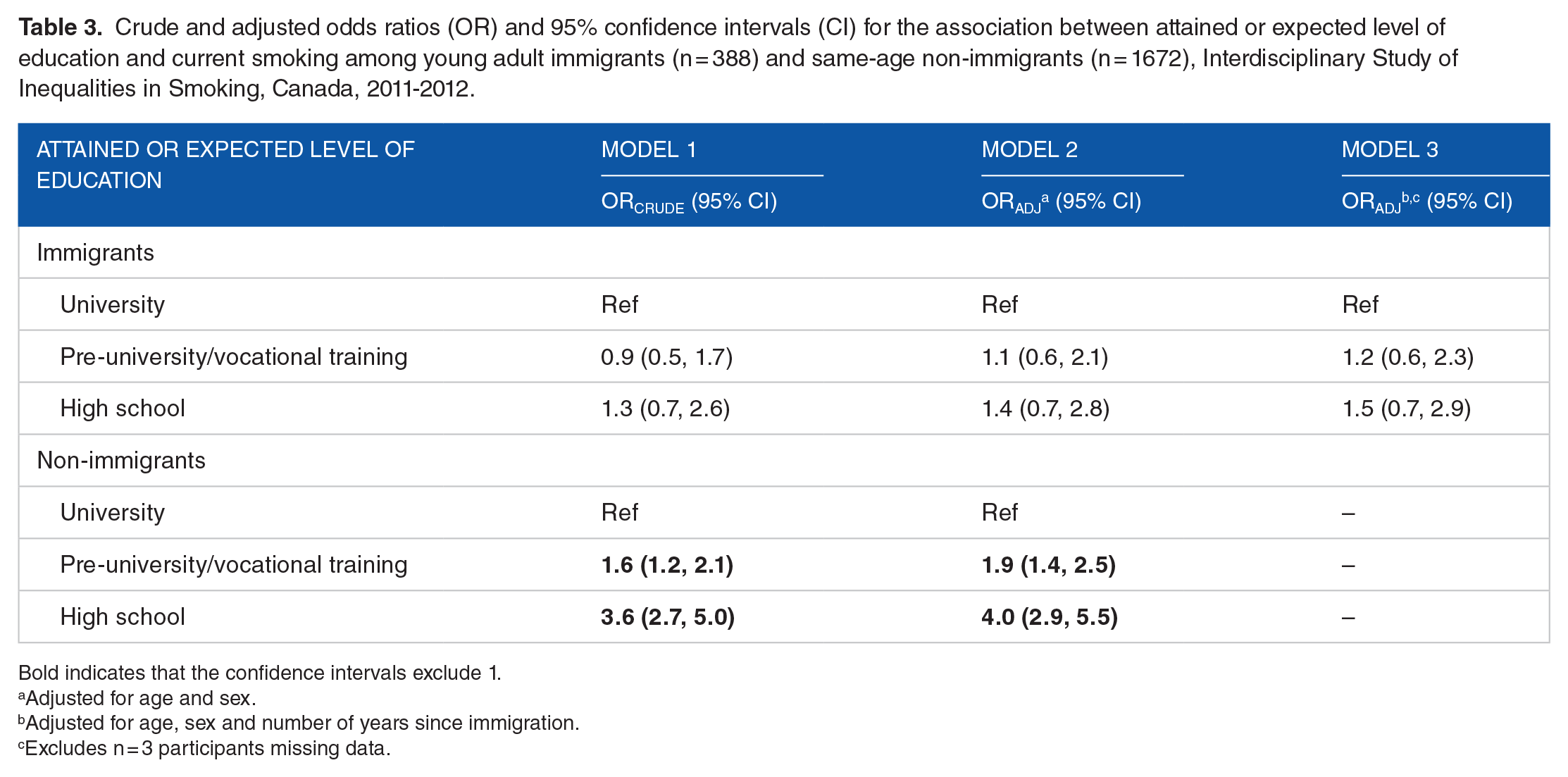
Bold indicates that the confidence intervals exclude 1.
Adjusted for age and sex.
Adjusted for age, sex and number of years since immigration.
Excludes n = 3 participants missing data.
Discussion
Numerous studies in Western countries document social inequalities in smoking, 23 but it is not known whether these inequalities also affect immigrants. Despite the HIE 11 and even though the prevalence of smoking is generally lower, 17 immigrants are generally believed to be disadvantaged in part because of the immigration experience. The stress of uprooting the family into a new social and cultural context as well as possibly experiencing discrimination increases the risk of social and material deprivation. 15 “Acculturation” refers to a process during which immigrants adopt the practices and values of the host country culture as they adapt to living in that society. Through acculturation, unhealthy behaviors of the host culture such as cigarette smoking may be emulated, contributing to poorer health. 14 However it is not known whether social inequalities apparent in the host population manifest in the acculturation process. In this current analysis, we queried whether social inequalities in smoking apparent in Canada-born young adults, manifest in same-age immigrants who had been in Canada 11 to 12 years on average.
Similar to previous reports15-17 including a recent study of adults age 18 or older in Québec, 18 the prevalence of smoking was lower among immigrants in this current study of young adults compared to non-immigrants (19.5% vs 23.8%). Street 18 also reported that in 2014-15, 14% to 15% of immigrants in Québec smoked occasionally or daily, compared to 21% of non-immigrants, and similar to our study, the differences were due primarily to fewer immigrant women smoking. Explanations for the lower prevalence of smoking among immigrants offered in previous studies include that positive health behaviors are carried over from the country of origin, that selection in pre-immigration health screenings reduces the number of smokers who immigrate, and immigrant self-selection (ie, those most likely to migrate are wealthier and healthier).11,17 In the Canadian context, economic immigrants are selected using a point system based on higher education, work experience and language proficiency, among other criteria. 24 These characteristics are linked to better health and may also contribute to healthier behaviors in immigrants.
In addition to these explanations, exposure to common risk factors for smoking may be lower among immigrants. For example, smoking is known to be an intergenerational phenomenon. 25 Because immigrant parents smoke less than Canada-born parents, their children are less exposed to family smoking, which is a strong early determinant of smoking onset. Further, strong family ties within immigrant families could protect against external influences and exposure to other tobacco risk factors.
Finally, country of origin could also underpin differences in smoking prevalence between immigrants and non-immigrants. In a study which differentiated immigrants from English- and non-English speaking countries, more important differences in prevalence were noted in the latter. Smoking prevalence among immigrants from non-English speaking countries differed by 4% to 6% from that of non-immigrants, 16 which is similar to the difference observed in our study. Further a study of the HIE in the United States, Canada, Australia, and the United Kingdom, suggested that immigrants from continental Europe and the Middle East did not always have a lower smoking prevalence than the native-born. 17
Social inequalities in smoking
As in other countries, the WHO Framework Convention on Tobacco Control was ratified by Canada in 2006, 26 and the province of Québec had already, by 2005, prohibited smoking in public indoor spaces as well as public display and advertisement of tobacco products. 27 Other large-scale actions targeting youth in Québec included awareness campaigns, school-based interventions, and free counselling and cessation programs.28,29 Our data suggest that these tobacco control measures may have been more effective in higher SES groups, since strong social inequalities in smoking were evident among young adults. However immigrants in our sample did not manifest these strong inequalities, despite having spent their formative years in Canada during which they were exposed to the prevailing cultural and health practices in Québec. It is possible that more time is required for smoking behaviors to be adopted and for them to impact more disadvantaged immigrants disproportionately. Although this challenges the notion that if immigrants arrive in their new host country at a younger age, they are more sensitive to acculturation, 30 it is possible that as immigrants age, economic, and social resources influence either initiation or cessation, widening the gap between advantaged and disadvantaged sub-groups. 10 In a broader perspective, the HIE has been linked to stronger social capital in immigrants through promotion of positive health practices in the family, 31 and it may take several generations for social inequalities in health behaviors including smoking, to manifest.
Alternatively, level of education may not be as strong an indicator of social inequality among immigrants as it is among non-immigrants. In Québec, intergenerational reproduction of social inequalities has been documented and the rate of young adults going to university is 3 times higher among those whose parents have a university education, compared to those whose parents completed high school only. 32 Although parental and household indicators are appropriate measures of SES during childhood, several authors suggest that these are likely to become less relevant in young adulthood as individuals become progressively independent and transition to their own SES. 33 In this study, we used a measure of expected level of education 22 for our youth participants to investigate the social gradient in smoking. However, if the underpinnings of level of educational attainment in immigrants differ from that in non-immigrants, this indicator may not be able to capture the link between SES and smoking among young adult immigrants.
Future research
Studies are needed to discern whether parental education, smoking in social networks, attitudes and beliefs about smoking or neighborhood-level variables19,34 protect against social inequalities in smoking among young adult immigrants. Results of these studies could inform the development of smoking prevention programs that address social inequalities in smoking. Immigrants are highly heterogeneous with unique ethnic and cultural backgrounds and smoking prevalence in their countries of origin is widely diverse.24,35 Although outside the scope of our study, future research could provide deeper insight into specific immigrant groups from different countries. Longitudinal studies are needed to describe whether and how acculturation affects social inequalities in smoking among immigrants and whether social inequalities become more apparent later in life. Quit success may increasingly relate to SES factors in both immigrants and non-immigrants in later adulthood. 23 Finally, surveillance could shed light on long-term trends in smoking among immigrants.
Limitations
The cross-sectional design of the current study limits causal inference. Although similar in age and sex, our sample was better-educated than the same-age Québec population 36 and persons not proficient in French or English were under-represented among study participants since these groups were excluded. Although low, our response proportion represents a conservative estimate since it is unknown how many non-respondents were actually eligible (ie, had not moved from the current address, accurate mailing address, interested in participating). 20 Data on household SES or parent’s education were not collected from parents in the first wave of ISIS data collection and thus could not be used in sensitivity analyses. Finally, because the sample was primarily urban, the findings may not be generalizable to young adults living in suburban or rural contexts.
Conclusion
In this sample from the Interdisciplinary Study on Inequalities in Smoking, 19.5% of young adults who had immigrated to Canada were current smokers compared to 23.8% of same-age non-immigrants. There was a strong inverse association between level of education and current smoking among Canada-born young adults, but this gradient was less evident among same-age immigrants. If replicated in future research, the reasons for the lack of strong social inequalities in smoking among young adult immigrants need to be identified since they may point to factors protective of social inequalities in smoking; a finding that could be remarkably beneficial to both tobacco control and immigrant health research.
Supplemental Material
sj-pdf-1-tui-10.1177_1179173X20972728 – Supplemental material for Do Social Inequalities in Smoking Differ by Immigration Status in Young Adults Living in an Urban Setting? Findings From the Interdisciplinary Study of Inequalities in Smoking
Supplemental material, sj-pdf-1-tui-10.1177_1179173X20972728 for Do Social Inequalities in Smoking Differ by Immigration Status in Young Adults Living in an Urban Setting? Findings From the Interdisciplinary Study of Inequalities in Smoking by Jodi Kalubi, Zobelle Tchouaga, Adrian Ghenadenik, Jennifer O’Loughlin and Katherine L Frohlich in Tobacco Use Insights
Footnotes
Acknowledgements
The authors wish to thank the Interdisciplinary Study of Inequalities in Smoking team, and especially Josée Lapalme, for their contributions.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Interdisciplinary Study of Inequalities in Smoking (ISIS) study was supported by a grant from the Canadian Institutes of Health Research (CIHR# MOP-110977—PI: KLF). JK holds a Doctoral Scholarship from the Québec Order of Nurses (Ordre des infirmières et infirmiers du Québec). JOL holds a Canada Research Chair in the Early Determinants of Adult Chronic Disease. KLF is the co-holder of the Myriagone-McConnell-University of Montreal Research Chair on Youth Knowledge Mobilization.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
KLF and AG collected the data. ZT, JOL and KLF conceived and designed the analysis. JK and ZT performed the analysis. JK wrote the manuscript with support from JOL and KLF. All authors discussed the results and contributed to the final manuscript.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (The University of Montreal’s Health Research Ethics Committee, 11-019-CERFM-D) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.