
Abstract
Background/Aims:
Guided imagery is an evidence-based, multi-sensory, cognitive process that can be used to increase motivation and achieve a desired behavior. Quitlines are effective, standard care approaches for tobacco cessation; however, utilization of quitlines is low. Using guided imagery-based interventions for smoking cessation may appeal to smokers who do not utilize traditional quitline services. This paper reports the development of program materials for a randomized controlled feasibility trial of a guided imagery-based smoking cessation intervention. The objective of the formative work was to ensure that program materials are inclusive of groups that are less likely to use quitlines, including men and racial/ethnic minority tobacco users.
Methods:
A three-phase process was used to complete formative assessment: (1) integration of evidence-based cessation practices into program development; (2) iterative small group interviews (N = 46) to modify the program; and (3) pilot-testing the coaching protocol and study process among a small sample of smokers (N = 5).
Results:
The Community Advisory Board and project consultants offered input on program content and study recruitment based on their knowledge of minority communities with whom they conduct outreach. Small group interview participants included members of underserved quitline populations (52.37% non-white; 55.56% men). Only 28.26% of participants had prior experience with guided imagery, but others described the use of similar mindfulness and meditation practices. Participant feedback was incorporated into program materials and protocols.
Discussion:
Iteratively collected feedback and pilot testing influenced program content and delivery and informed study processes for a randomized controlled feasibility trial of a telephone-delivered, guided imagery-based intervention.
Keywords
Background and purpose
Guided imagery is a mind-body technique that involves the visualization of specific images, thoughts, emotions, and senses that occur in the absence of actual experience and are closely tied to the memory or anticipation of some event.1,2 Guided imagery is also referred to as “visualization” or “seeing in the mind’s eye” and may be accompanied by deep breathing or relaxation, 3 followed by images of achieving health-related goals and elicitation of emotions associated with achieving those goals. This visualization/relaxation combination increases self-efficacy and motivation. 4 The formative work reported here focused on developing a guided imagery-based quitline intervention to increase quitline reach to all smokers, paying special attention to underserved smokers such as men and racial/ethnic minorities.
Emerging research points to the potential for guided imagery interventions to effect smoking behavior change. 5 Using the cognitive-motivational framework of guided imagery, 6 imagery is predicted to facilitate users’ smoking cessation by building self-efficacy for quitting, increasing confidence in coping with cravings, and helping to create an image of being smoke-free to prevent relapse. Previous research has supported the use of the cognitive-motivational framework behind guided imagery. 7 Cognitively focused images may include seeking and using resources to quit smoking (eg, avoiding people who smoke), identifying and using skills to maintain cessation (eg, relaxation for coping with cravings), and making plans to be a non-smoker (eg, how to deal with a smoking “slip”). Motivationally oriented images include emotions associated with smoking and quitting (eg, reasons and benefits), cravings (eg, ability to overcome cravings), and confidence-enhancing messages (eg, enhancing and maintaining motivation over time).
Guided imagery has been used to promote health in diverse populations, such as men in the Veterans Administration, 8 Latino adolescents, 9 and African American women. 10 While most research does show less use of complementary and alternative medicine (CAM) by minorities, others have shown equal usage or predominant usage of CAM practices in some groups,11,12 particularly among groups who report experiencing discrimination in health care. 13 Other research indicates interest in use of CAM by racial/ethnic minorities.14,15 Finally, distrust in conventional tobacco cessation approaches (eg, NRT) among racial/ethnic minority populations 16 could make guided imagery an appealing alternative cessation tool.
Using a guided imagery approach may be a method for increasing quitline use among underserved tobacco users 17 and promoting cessation among men, who are less likely to use smoking cessation services, 18 and among racial/ethnic minorities, who are less likely to quit smoking than non-Hispanic/Latino Whites. 19 Although they are available in all 50 states, quitlines reach a small percentage of the smoking population,20–22 making them an effective but underutilized method for disseminating cessation programs. Most employer-based and insurance-based cessation programs are contracted to the same quitline providers that deliver state-contracted quitline services, and utilization of these programs is low, with most participants using nicotine replacement therapy (NRT) alone. 23 Moreover, due to limited funding, quitlines often triage services to primarily serve the uninsured and underinsured (ie, groups with high rates of tobacco use and limited access to cessation treatment).
The low uptake of quitline services indicates a low reach of quitlines among underserved populations nationwide, 17 including racial/ethnic minority populations, 21 and the potential to increase services to these groups. Several studies have recommended using “non-traditional” program delivery and outreach methods to appeal to racial/ethnic minorities and other underserved populations of tobacco users.24–26 Standard quitline treatment uses a combination of behavioral treatment (focusing on motivation and goal setting) and nicotine replacement therapy. It does not include visualization or other complementary/integrative approaches in the standard protocol. 27
This paper reports the findings from formative work to develop a quitline-delivered guided imagery smoking cessation intervention. The parent study was a two-group randomized controlled feasibility trial (RCFT) with eligible participants randomized to the control (standard care) or the intervention (guided imagery) condition (both groups included optional nicotine replacement therapy). The main objective of this formative work was to develop program materials that were inclusive of the diversity of smokers, by ensuring their appeal to groups who do not typically use quitlines, including racial/ethnic minorities and men. The secondary objective of this formative work was to test study procedures and address any problems before RCFT participants engaged in program and study activities. The research team developed the “Be Smoke Free” program in order to appeal to the general population of smokers, with special attention to and recruitment of smokers who are underrepresented among callers to quitlines nationwide.
Methods
This formative assessment was conducted in 3 phases using qualitative and mixed methods. We integrated input from cultural brokers (individuals who advocate on behalf of a particular group) 28 and tobacco users about evidence-based coaching methods and materials.
Phase I: Integration of evidence-based practice with input from Community Advisory Board and Consultants
A Community Advisory Board (CAB) comprised of 9, racially/ethnically diverse, community health advocates with expertise in developing culturally sensitive materials for underrepresented quitline callers (eg, racial and ethnic minorities and men), reviewed intervention condition content and assisted in developing recruitment strategies. The group met twice during the development phase of the project with additional input collected via emails and phone calls. At the meetings, the draft program name and materials were discussed, and notes taken to capture members’ input. The materials were refined through an iterative process of seeking feedback from the CAB until reaching saturation (eg, no new themes or concerns).
We also consulted with 2 nationally recognized experts in designing, delivering, and testing the effectiveness of tobacco cessation interventions for African American and American Indian/Alaska Native populations. They are practitioners with expertise in treating tobacco dependence in underserved populations, and they have worked to inform local and national policies for addressing tobacco use among these populations. The consultants reviewed all study materials, including recruitment/program materials and study measures.
Phase II: Integrate input from smokers, with a focus on priority populations
Small group and individual structured and semi-structured interviews (N = 46) were conducted to understand how participants perceived the program’s messaging, content, and design. A purposive sample of smokers participated in a 90 to 120 minute, one-on-one or group interview in Tucson, Arizona (N = 42) or Morgantown, West Virginia (N = 4), where one of the study investigators (PG) is based. The 2 locations allowed us to examine perceptions of program content and messages with a more diverse sample of smokers (and smoking prevalence in Appalachia is particularly high). 29 Keeping in mind our long-term plan to expand the study nationwide for efficacy testing, the team planned to include a small West Virginia sample to determine study interest and potential methods for recruitment. Recruitment in West Virginia focused on print/digital media outlets with which PG had previous success. Given the projected small sample size for in-depth interviews, we did not conduct wide-scale community recruitment in West Virginia As a result of this small WV sample, no WV-specific findings are reported.
The team conducted 3 waves of Phase II data collection to inform modifications to program materials, which included recruitment scripts, program name and logo, supplementary materials, and intervention protocols (Figure 1). We also identified several broader recurring themes that informed the iterative modifications. Interviews included a structured survey to gather Likert-style ratings of program elements (eg, definition of guided imagery) and a semi-structured questionnaire for participants to elaborate on program materials, and facilitators and barriers to their participation in the program. Program material revisions were prioritized based on participant ratings, and modifications were based on participants’ thematic feedback.

Iterative data collection and program material revisions (Phase II – Qualitative Data Collection).
To ensure input from specific priority populations, the recruitment plan involved specific outreach to local (Tucson, Arizona) organizations and media outlets that would provide an audience of men and racial/ethnic minorities. This included: presentations at cultural centers and construction work sites; flyers posted in health centers, child care centers, libraries, ethnic supermarkets, and other community centers; postings on university and community online media; and advertisements in the Arizona Bilingual Newspaper. In West Virginia, we posted recruitment information on Craigslist and placed advertisements in the Morgantown newspaper and The Dominion Post.
Inclusion criteria were: 18+ age, speak English, smoked (“even a puff”) within the last 30 days, and at least 5 on the readiness to quit scale (1–10). Exclusion criteria were: <18 age, do not speak English, have not smoked (“even a puff”) within the last 30 days, and <5 on the readiness to quit scale. Group interviews were organized by self-identified race and gender. Figure 1 shows the data collected in each phase.
Participants completed a written survey and then answered semi-structured open-ended questions about elements of the guided imagery intervention. Interviewers took detailed notes and recorded the meetings to ensure accurate notetaking. After the interview, study staff drafted a brief analytical memo about the interview, which included the most salient points from the discussion. Analytical memos and notes were reviewed for themes, which the team interpreted after each wave and applied the findings.
Formative interviews aimed to learn participants’ perspectives on guided imagery as a strategy to help individuals quit smoking, to ensure that program messaging and content was understandable and useful. We paid special attention to developing a clear definition of guided imagery along with examples that highlight this skill (eg, among athletes), and ensuring that the intervention program materials (eg, web site, booklet/guide, and protocols) were acceptable. We were also interested in smokers’ pre-existing understandings of quitlines, so that we could create appealing and helpful recruitment and program materials.
Phase III: Pilot test the study design with smokers who want to quit
The final study procedures and recruitment process were pilot-tested in a RCFT (ClinicalTrials.gov Identifier: NCT02968381) during the first week of study recruitment (April 24–May 1, 2018). Ten pilot testers were recruited through the Arizona Smokers’ Helpline (ASHLine) and enrolled into the 6-month RCFT protocol prior to the launch of the actual trial (final pilot tester finished the study on 11/1/2018). Process data from these participants were used to refine study procedures; pilot data were not reported in RCFT outcome data. 30 See Figure 2 (CONSORT diagram) for details. Program and study data were collected and managed using REDCap (Research Electronic Data Capture). REDCap is a secure, web-based application designed to support data capture for research studies. 31
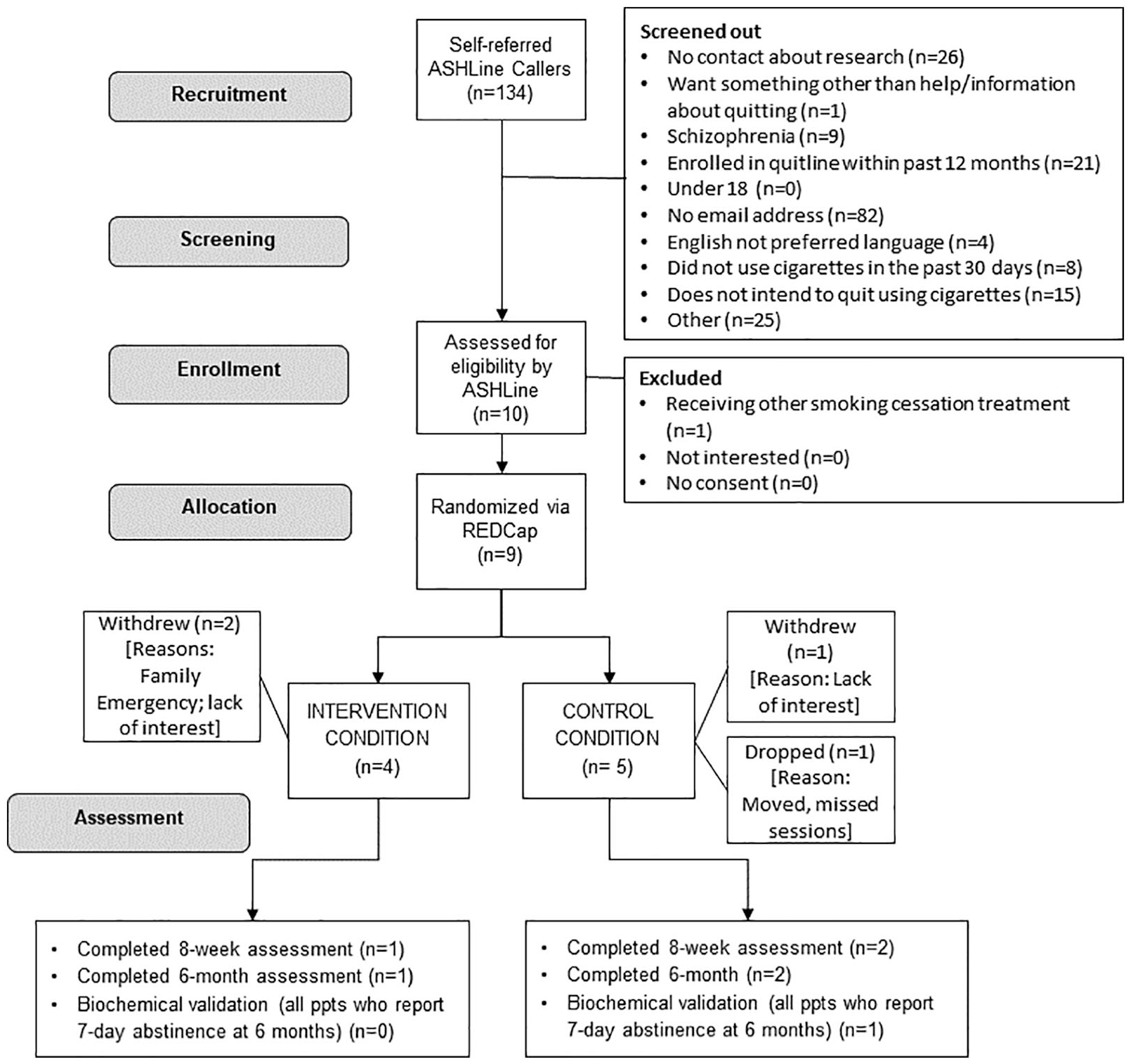
Plot Testing Study Flow (Phase III of formative assessment) 4/24 to 5/1/2018.
Results
Phase I: Integration of evidence-based guided imagery practice and tobacco cessation with input from Community Advisory Board and Consultants
We created matched control and intervention condition protocols based on evidence-based tobacco cessation programs, including motivation and skill building, triggers, coping with cravings, coping with withdrawal, problem solving/relapse prevention, and the use of nicotine replacement therapy (NRT). 32 Each condition featured 6 sessions that covered the same topics in sequence. 32 However, the control condition used an approach guided by cognitive behavioral theory (CBT) and the intervention condition used a guided imagery approach, including personalized guided imagery scripts. To create these scripts, trained coaches elicit sensory and emotion-rich information from participants related to quitting smoking, and work with participants to craft this information into a vivid guided imagery script which is recorded for repeated listening. For further information about the program content, see our protocol paper. 33 Recommendations from the CAB and project consultants on the content and structure of the intervention are presented in Table 1. Their input, which centered on enhancing the cultural appropriateness of the intervention, was incorporated into study materials before and during Phase II.
Community advisory board and consultant recommendations to enhance cultural appropriateness (Phase I of Formative Assessment, Tucson, Arizona; March 2017–June 2017).
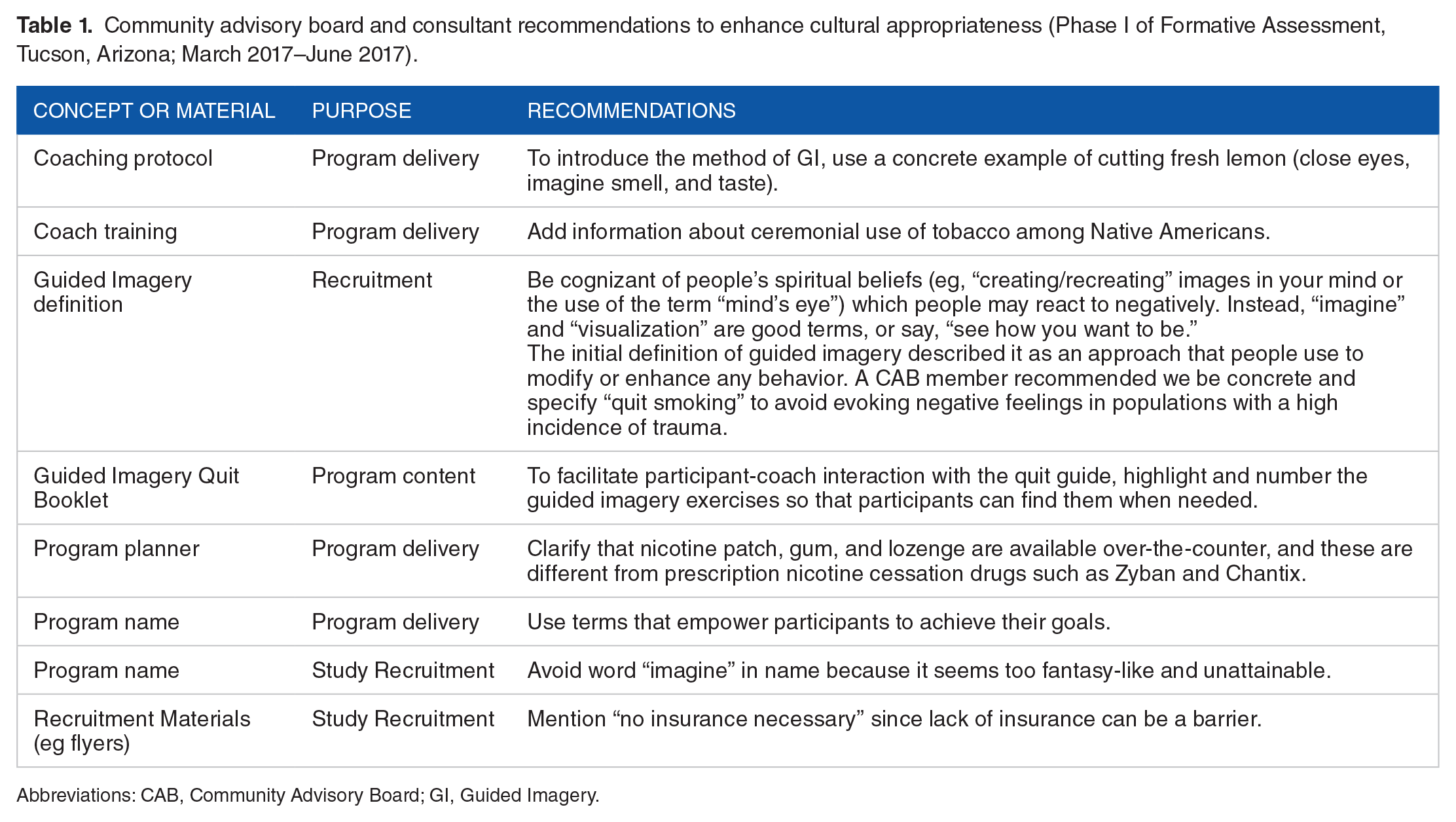
Abbreviations: CAB, Community Advisory Board; GI, Guided Imagery.
Phase II: Integrate input from smokers, with a focus on priority populations
Phase II participant demographics are in Table 2. Participant interviews elucidated several important themes, including: pre-existing understandings of guided imagery may or may not reflect the actual practice; misperceptions about how quitlines work; smokers may want to take responsibility for quitting while they seek support; distrust of the unknown (eg, guided imagery) or large, impersonal institutions (eg, government-sponsored programs) influences understanding of the program materials; and accommodate low-literacy levels when developing and editing program content. These themes guided program material modifications as follows: provide step-by-step outlines of the program to manage participants’ expectations of the program, of guided imagery, and of their coaches; emphasize that individuals have control over quitting but that coaches, as experts in the field of smoking cessation, provide guidance; and engender trust in coaches and the program by communicating authentic messages, which include testimonials from people who have used guided imagery or a quitline to quit smoking. The key themes are described below and displayed in Figure 1.
Participant demographics – Phase II Qualitative Data Collection (n = 46). Tucson, Arizona & Morgantown, West Virginia. August 2017 to December 2017.

Abbreviation: GI, Guided Imagery.
Participants’ understanding, use of, and trust in guided imagery
While more than half of participants reported no experience with guided imagery (58.70%), several participants described using a practice similar to guided imagery. Several participants identified practices in which they managed stress, visualized a scenario to make it happen, or pictured a better way of doing things to succeed (eg, envisioning a “game plan”). Several small group interview participants described using something like guided imagery for anger management, describing the process of pausing between impulse and action to replace the impulsive action with an alternative. One participant commented, “It’s almost like an out of body/mind experience. You put yourself in another place. You’re looking at yourself from the outside.”
The initial definitions of guided imagery developed by the research team produced mixed responses, with some participants becoming skeptical of the approach and others expressing concern about having the expertise or understanding necessary to develop the images. Overall, initial drafts elicited expressions of distrust about guided imagery and the motive of the coaches. One participant commented that the team’s description of guided imagery “seems like I’m being controlled and moved into a place that I’m unfamiliar with.” In contrast, other participants acknowledged guided imagery’s capacity for personalization in partnership with a coach. A particularly skeptical participant argued that the definition made guided imagery seem too good to be true: “You cannot tell me, ‘see yourself next year, you’re going to be driving a luxury car because you quit smoking!’” Another participant echoed the concern about the general description of guided imagery, suggesting more specificity (eg, imagining something associated with not craving a cigarette). See Figure 1 regarding how this feedback was incorporated into program branding (eg, definition, tagline) and web site content (eg, testimonials from athletes).
Misperceptions about quitlines, coaching, and individual responsibility
Participants who did not have experience with a quitline were unclear about the role of the coach. Several participants commented that a call to the quitline is “just talking” (eg, “it doesn’t seem logical to just talk to someone”). Participants with a history of participation in Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) thought quitlines followed the same model of support, with coaches as sponsors. One participant noted that if a coach is not an ex-smoker, that person is not qualified to help her quit. Another participant thought quitlines operate like suicide hotlines, which offer support and resources during a crisis.
Participants conveyed a lack of understanding about the role of the coach. Many felt that a coach would try to convince a person to quit, rather than provide expertise in behavioral and pharmacotherapy to those who already want to quit. They described feeling that they should have enough motivation to quit so that coaching is unnecessary. One participant articulated a sense of failure in calling the quitline, “I was ashamed because I felt like I should quit myself. I didn’t like to admit that I needed help not to smoke.” In talking about “will to quit” and discussing successful quit attempts, participants highlighted personal responsibility and the importance of making the decision to quit and sticking to it. Conversely, they also emphasized the role of the coach as partner and supporter during discussions about program materials.
Distrust also emerged as a theme. Participants described a quitline as an impersonal entity without an interest in individual smokers’ well-being. One individual who identified as Native American commented, “[The quitline is] not going to help us—we’re way out here [living on rural tribal lands], what are they going to do?. . .I’ve never seen any results personally myself, or anyone who’s gone through [the quitline].” Participants suggested that it would be difficult to develop a relationship with or trust a stranger on the phone. One participant noted unease with people calling him to try to sell him things. While participants liked the fact that quitlines are free, they expressed concern about many “free” services charging callers for specific “add-on” resources or services. They acknowledged that quitlines seem easy to access. See Figure 1 for details about program material modifications for enhancing understanding of quitlines and coaches.
Accommodate low-literacy levels among participants
In our last group interview, participants agreed that the program materials’ literacy level was too high, despite investigators’ attempts to address this issue in previous iterations (Figure 1). One participant with a 6th grade reading level suggested simplifying some of the ideas in the written materials. The team further refined the language in all materials to be approximately 5th grade reading level. In the same group, the definition of randomization (“. . .you will be randomly assigned (50-50 chance) to 1 of 2 interventions. . .”) in the informed consent document was misunderstood by at least one-third of the group. Participants interpreted this as only being given a 50-50 chance of succeeding with quitting and they felt they deserved better odds. We resolved this by dropping the “(50-50 chance)” portion of the sentence.
Phase III: Pilot testing the protocol with smokers who want to quit
Figure 2 outlines the flow of 10 pilot testers, which included 3 withdrawals, 1 dropped participant, and 1 lost participant due to a technical “glitch.” The reasons for withdrawal included: lack of interest and a family emergency. We developed a process for transferring a dropped participant to the ASHLine after the individual missed >4 weeks of pilot study sessions due to a home move; the technical problem that led to the lost participant was also fixed. The 5 remaining pilot testers completed an average of 4.2 sessions (range = 0–6). The pilot testers who completed the 8-week follow-up survey (n = 3) reported being satisfied or very satisfied (4–5 on a scale of 1–5, not at all satisfied to very satisfied) with the Be Smoke Free program.
Pilot testing enabled the study team to adjust program delivery and study protocol issues. Study protocol changes included: the creation of a two-step consent process to ensure understanding of study requirements; and a contact protocol for coaches and study staff to define the number of phone calls, texts, and emails for non-responsive participants. We were also able to fix technology-related problems, such as automated survey delivery in REDCap and recruitment and data transfer from ASHLine’s enrollment system to REDCap. We developed a procedure for “turning on/off” recruitment from the ASHLine when participant volume exceeded study staff capacity. We also refined coaches’ program delivery. One coach was replaced due to scheduling constraints and the inability to achieve competency, and we hired replacement coaches with experience in phone-based coaching and a flexible schedule. Importantly, coaches’ practice sessions with pilot testers enabled them to master the protocols and streamline calls to reduce their duration.
Discussion/implications for practice and future research
The purpose of the study was to develop and pilot test a guided-imagery, telephone-based intervention for smoking cessation. Program material development was an iterative process informed by experts, community members, and small group interviews and focus groups in Arizona and West Virginia. This ensured the program’s appeal to a diverse population of smokers, with a particular focus on men and racial/ethnic minorities. Pilot testing enabled the team to adjust RCFT procedures and systems (eg, recruitment, survey administration) to improve program delivery.
Program development considered the scalability to quitlines nationwide. Traditional quitlines are an effective treatment for tobacco cessation but there is limited reach due, in part, to perceptions of quitlines as a “last resort” method for people who cannot quit on their own. 34 Our formative work confirms prior research that smokers may not understand the role of quitlines and are concerned about the stigma of seeking help.17,35 Like other researchers, we found varied perceptions and concerns about the role of quitline coaches, 34 which indicates the need to define the role of the coach to optimize intervention acceptability. This lack of understanding may be a barrier to use of the quitlines among underserved populations. In response to this lack of understanding, we modified our program materials to better describe quitline services and manage participants’ expectations about quit coaches. Our recruitment and program materials included language and images that emphasized quitline coaches’ role as experts who work with callers to develop a caller-directed plan for quitting, while providing support during the process.
We used recruitment materials and advertisements to address these gaps in understanding. Mass media marketing and referrals via health care providers are primary means for generating calls to quitlines. Only a few studies have been published addressing the relative effectiveness of alternative advertising strategies, 36 but the evidence suggests there is work to be done in encouraging underserved groups to engage with quitlines. Studies have noted that media campaigns are not likely to diminish differences in call rates across underserved groups. 37 Moreover, given smokers’ misperceptions of quitlines, special programming may provide an opportunity to attract a more diverse group of smokers.
To our knowledge, we are the first to explore individuals’ understanding of the use of guided imagery for smoking cessation. Research suggests that complementary and alternative medicine (CAM) techniques may appeal to people with health concerns 38 and provide an opportunity to engage individuals in behavior change. 39 Our formative research indicates the need to build on smokers’ understandings of CAM techniques, such as meditation or mindfulness, to make guided imagery an appealing tool for smoking cessation. Further, it is important to use language that is non-threatening, accessible and concrete in describing guided imagery.
Our findings may be limited by the design of our phase III pilot testing and a lack of representativeness of our sample. In phase III, we enrolled pilot-test participants who engaged in all RFCT activities just ahead of the RFCT participants. While this allowed us to modify program and study procedures “in real time,” the necessary rapidity of revisions limited our ability to make significant changes that might have improved program outcomes. However, the phase III testing did allow us to make many meaningful changes to the intervention and control protocols and study procedures. The qualitative methods used in our study are useful for highlighting variation within populations, which can optimize cultural sensitivity and relevance. This is the first study to utilize a qualitative approach to develop a telephone-based, guided imagery intervention for smoking cessation. By utilizing a CAB, consultants, and our priority populations in program development, we aimed to ensure that the program materials and recruitment approach respected cultural diversity and represented inclusiveness.
Footnotes
Acknowledgements
We would like to recognize Anh Vu for her contributions to organizing and formatting the manuscript’s references. Moreover, we would like to acknowledge the important contributions of Gayle Povis, MS, RD to this project and to this manuscript before she passed away in May 2019. We are grateful for the input of our Community Advisory Board members and our research participants, whose insights are reported in this manuscript. The study was conducted at the University of Arizona Collaboratory for Metabolic Disease Prevention and Treatment.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Center for Complementary and Integrative Health (#R34AT008947, PI: Gordon). No copyrighted material was adapted or reused in this manuscript. All study activities were approved by the Institutional Review Board at the University of Arizona.