
Abstract
People with disabilities (PWD) are more likely to use tobacco and less likely to access tobacco cessation programs compared with people without disabilities. Living Independent From Tobacco (LIFT), an evidence-based intervention designed for PWD, was piloted with dyads of PWD (n = 5) and their caregivers (n = 7). As an important source of practical and social support for PWD, caregivers also impact health-related attitudes, knowledge, and behaviors of PWD. Caregivers who smoke may unwittingly interfere with cessation efforts of the people they support. We found that LIFT could be offered to dyads of PWD and their caregivers with fidelity. The intervention was associated with increased use of coping strategies and self-efficacy to reduce smoking. Tobacco use decreased at post-test (−34.94%), with further reduction 6-months after the intervention (−50.60%). Implications for offering inclusive health promotion interventions to both PWD and their caregivers are discussed.
The cost to society of tobacco use is estimated to amount to hundreds of billions of dollars for direct medical care expenses and loss of productivity among people who smoke or use tobacco. 1 The harms of smoking cigarettes disproportionately impact some groups more than others. One such group, people with disabilities (PWD), is nearly twice more likely to smoke cigarettes than people without disabilities, even after adjusting for sociodemographic factors. 2 These disparate smoking rates are compounded by a myriad of other health disparities faced by PWD including, but not limited to, poor access to healthcare, poor health behaviors such as eating unhealthy diets and lack of physical activity, increased rates of obesity and cardiovascular disease, poor emotional and social support, and higher rates of negative social determinants of health such as poor education, unemployment, and low household income. 3 Disparate rates of smoking among PWD offers an opportunity to improve and promote health; however, a lack of effective tobacco cessation programming for PWD likely contributes to these tobacco-related disparities. 4 To address this issue, Pomeranz et al 5 developed an accessible tobacco cessation intervention for PWD, Living Independent From Tobacco (LIFT).
LIFT is an evidence-based smoking cessation program developed for PWD with input from PWD and disability experts. 5 The LIFT curriculum addresses health education about the harmful effects of tobacco and benefits of tobacco cessation. Participants also learn about the addictive properties of nicotine and are taught coping strategies to manage nicotine withdrawal. 5 Participants are encouraged to augment the LIFT class with nicotine replacement therapy to support the quit process. Indeed, nicotine replacement therapy, together with behavioral counseling, was found most effective in helping PWD reduce smoking or quit altogether. 5 To this end, LIFT has been found effective in reducing tobacco use among PWD. 5 Yet, the problem of smoking disparities among PWD is only partly addressed by effective tobacco cessation interventions such as LIFT.
Because of physical or cognitive impairments, some PWD use caregivers such as paid staff or family members to assist with daily living activities. Previous research shows that PWD form strong social and emotional connections to these caregivers and view them as important sources of emotional as well as practical support.6,7 Moreover, recent research has documented that caregivers may impact the health behaviors of PWD they support. 8 This research aligns with Social Cognitive Theory, which posits that role modeling of peers in one’s social network reinforces day-to-day behaviors, including health-promoting and health-compromising behaviors such as smoking. 9 Moreover, Social Cognitive Theory extends that peers hold one another accountable, serving to reinforce and support meaningful behavior change for the better or for the worse. 9 Previous work has documented that many paid caregivers engage in health-compromising behaviors, including smoking, and impact the health-related attitudes, knowledge, and behaviors of the PWD they support.7,8 That is, caregivers are in a unique position to facilitate or impede the health behavior choices of PWD. With support and training, caregivers could adopt and facilitate positive health behavior changes that could lead to reduced tobacco use for both themselves and the people they care for.
We piloted LIFT with PWD and their caregivers, and we evaluated changes in knowledge of health risks of tobacco use, attitudes and self-efficacy pertaining to tobacco reduction, and coping skills to manage nicotine withdrawal among both PWD and their caregivers. Breath carbon monoxide (CO) tests were used to measure tobacco use. It was hypothesized that both PWD and caregivers would reduce smoking after the intervention and maintain smoking reduction at 4-week and 6-month follow-ups. Finally, we evaluated the fidelity of the LIFT intervention when offered to dyads of PWD and their caregivers.
Method
Participants
Participants were recruited online and through statewide disability networks. Eligible participants either provided care to a person with disabilities at least 3 times a week (caregivers) or were PWD who had a caregiver; were at least 18 years of age; were able to understand and speak English; and were able to breathe into a CO monitor. For this study, disability was defined as a state of impairment(s), activity limitation(s), and/or participation restriction(s), consisting of limitations that impacted physical, mental, and/or behavioral health. 10 Participants were currently using tobacco on a daily basis and agreed to limit their involvement in tobacco cessation programs to LIFT for the duration of the study. Eligibility criteria were later broadened to allow caregivers who did not themselves smoke to participate. This change was made to meet the needs of PWD who wanted to participate and were otherwise eligible but did not have a caregiver who smoked. Three non-smoking caregivers completed the LIFT program and were included in these analyses.
A total of 7 dyads (PWD and caregiver) were recruited; however, 2 PWD dropped out of the study for non-program-related reasons, resulting in a total of 12 participants who completed the LIFT curriculum and evaluation protocol. See Table 1 for participant demographics. All caregivers in this study were paid staff who had provided care for an average of 10.80 years.
Participant demographics.

CP, cerebral palsy; LIFT, Living Independent From Tobacco.
Individual did not complete the LIFT intervention.
Measures
Living Independent From Tobacco surveys
Pre-test, post-test, and 4-week and 6-month follow-up surveys were administered in writing or verbally according to participant preference to evaluate knowledge about tobacco, attitudes about tobacco use, self-efficacy to quit smoking, strategies to cope with tobacco cessation, and tobacco use. 5 Surveys consisted of 57 items in total which included 9 demographic items, 21 items related to overall health status including tobacco use, 7 items related to tobacco awareness, 10 items related to beliefs about smoking, and 10 items related to strategies for achieving and maintaining smoking cessation. Post-test, 4-week, and 6-month follow-up surveys included an additional 11 items specific to smoking cessation behaviors. Most items were rated on a 1-to-5 Likert scale to indicate improvement in behavior, attitudes, or to identify barriers to quitting. Where possible, survey items were adapted from validated tobacco instruments including the Perceived Stress Scale, the national Adult Tobacco Survey Questionnaire, and the National Youth Tobacco Survey.
Carbon monoxide breath tests
Carbon monoxide breath tests were used to measure tobacco use. Participants were instructed to inhale and exhale into the CO monitor according the instructions of the device read aloud by a trained research staff.
Procedure
This study was approved by our university’s institutional review board and written informed consent was obtained from all participants. The LIFT program was offered in 3 Midwestern cities by 3 facilitators using the manualized LIFT curriculum. A third-party evaluator attended all LIFT sessions and documented fidelity. Evaluations were administered at pre-test, post-test, and 4-weeks and 6-months after the LIFT intervention.
Intervention
LIFT is an evidence-based smoking cessation intervention developed for PWD. 5 The manualized LIFT intervention consisted of eight classes over four weeks conducted in groups of PWD by a facilitator. For this study, we modified the LIFT curriculum in one respect: we included PWD and their caregivers together in LIFT. Our goal was to evaluate whether LIFT could be offered to both PWD and their caregivers without modification to the manualized curriculum. The LIFT curriculum addressed the harms of tobacco and the benefits of cessation, as well as the benefits of nicotine replacement therapy. LIFT incorporated a behavioral counseling approach that taught skills to cope with cravings, nicotine withdrawal, and social situations. Nicotine replacement therapy was offered to all participants.
Results
Fidelity
An external evaluator observed all sessions and documented fidelity to the manualized LIFT curriculum and instructional quality. In total, 79 components of the curriculum were evaluated for fidelity and instructional quality. The external evaluator concluded that the LIFT curriculum was offered to dyads with 100% fidelity across all sessions and research sites. Instructional quality was defined as interactions where the facilitator gave examples and engendered participant discussion. Of the 79 components evaluated, 71% were rated as demonstrating high instructional quality.
Effectiveness
Effectiveness data examined knowledge about the harmful effects of tobacco use, attitudes toward tobacco use, self-efficacy, coping skills, and tobacco use. Effectiveness was evaluated at four time points evaluated at time points: pre-test, post-test, and 4-week and 6-month follow-ups.
Knowledge about harmful effects of tobacco
Participation was associated with increased awareness that tobacco was addictive (+2.85%), dangerous (+15%), harmful even if used infrequently (+13.90%), and harmful if exposed secondhand (+20.61%) at post-test. Most of this knowledge was retained through the follow-up period, although at 4-weeks participants reported less awareness of the addictive properties of tobacco (−2.89%) while still acknowledging that tobacco was dangerous (+14.82%), harmful when used infrequently (+13.67%), and when exposed secondhand (+5.89%) compared with pre-test. Knowledge of chemicals in tobacco products increased at 4-weeks (+10.05%) and at 6-months (+10.33%) compared with pre-test.
Attitudes toward tobacco use
Participants were more likely to regret having starting smoking at post-test (−13.65%) and maintained this belief at 6-months (−12.50%) compared with pre-test. Participants were less likely to endorse the belief that smoking reduces stress (−16.92%) and helps in social situations (−17.94%) at post-test; however, participants were more likely to report that smoking helps control weight (+16.28%) at post-test. Beliefs about the benefits of smoking to reduce stress were maintained at 4-weeks (−4.69%) and 6-months (−4.69%); however, beliefs about the benefits of smoking in social situations returned to baseline.
Self-efficacy
Participants reported increased confidence in their ability to quit (+16.4%) and refuse cigarettes if offered (+8.5%) at post-test; however, confidence returned to baseline levels at 4-weeks and 6-months. Participants were less likely to succumb to temptation to smoke first thing in the morning (−13.58%), when anxious/stressed (−13.03%), when needing a boost (−11.28%), and when dealing with anger (−7.90%) at post-test. At 6-months, participants were less likely to turn to smoking to deal with anger (−13.17%) or for a boost (−20.16%).
Coping skills
Participants reported using coping skills to manage craving, withdrawal symptoms, and social situations without cigarettes. At post-test, skills reported included breathing and/or stretching exercises (+37.50%), relaxation methods (+38.89%), a healthy substitute (+29.31%), spending time outside (+39.89%), and eating healthy snacks (+21.81%). On average, participants reported using 4 coping skills at post-test, a 30% increase from pre-test. See Figure 1 for information about the type and frequency of skills used.
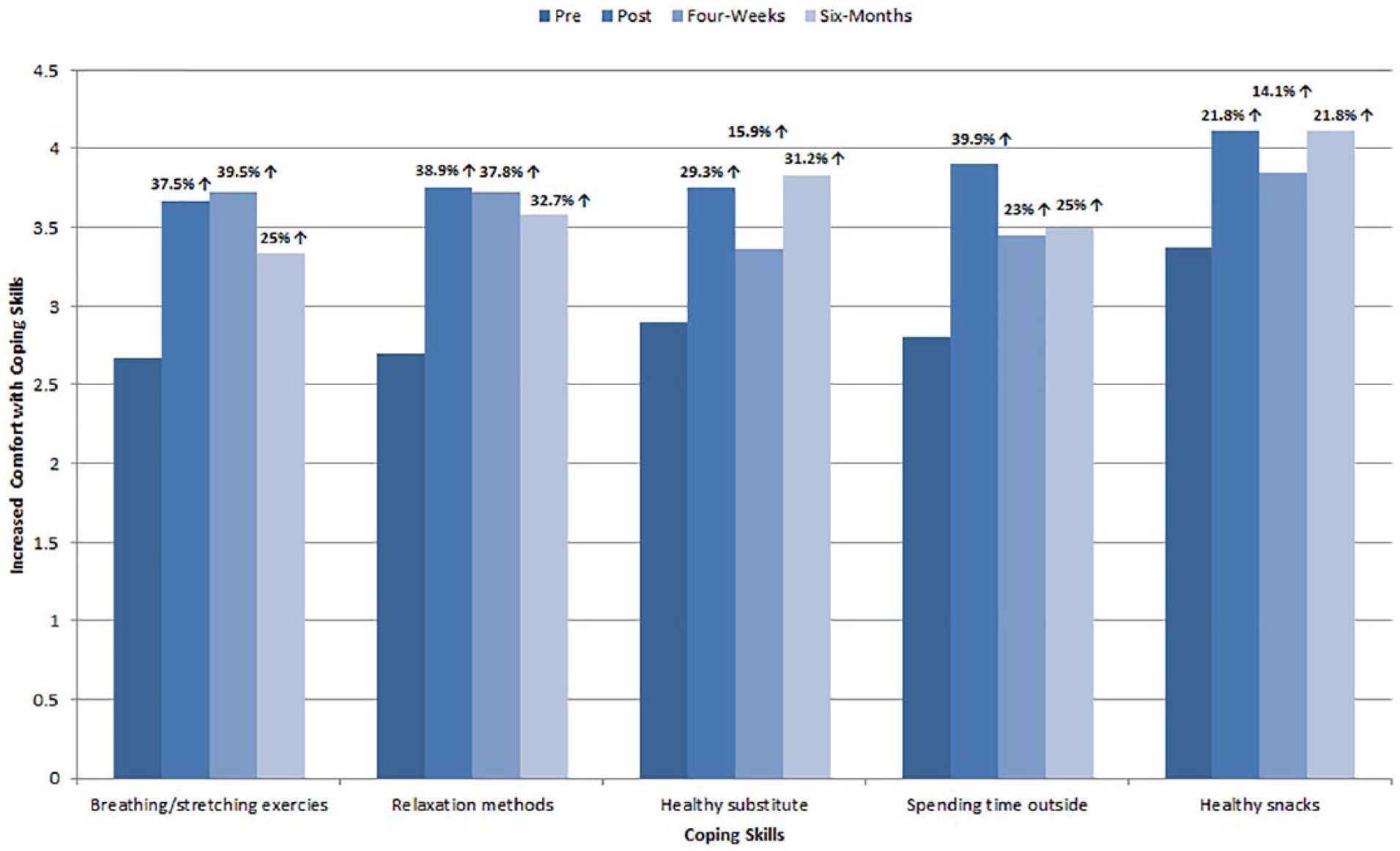
Comfort with coping skills across combined participants and time.
Tobacco use
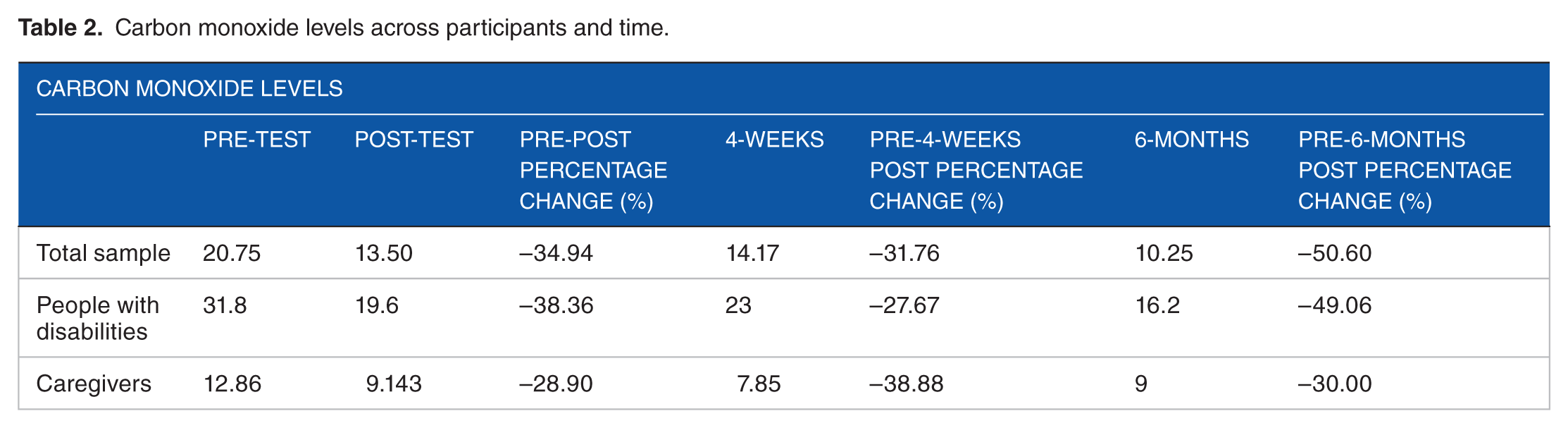
Carbon monoxide levels decreased from pre-test to post-test for PWD (−38.36%) and for caregivers (−28.90%). Tobacco use decreased further from pre-test to 6-months for PWD (−49.06%) and caregivers (−30.00%). Across the participant groups, we observed a 50% reduction from baseline to 6-month follow-up in tobacco use (see Table 2).
Carbon monoxide levels across participants and time.
Discussion
The LIFT curriculum was offered with fidelity to PWD and their caregivers. Participants gained knowledge about the harmful effects of tobacco and gained confidence in their ability to quit smoking. Importantly, participants reported a 30% increase in using coping skills to resist nicotine cravings. The increase in coping skills is important because once learned these skills can be used now and in future to manage cravings, nicotine withdrawal, social situations, and emotional distress associated with tobacco cessation.11-13 Tobacco use decreased during the LIFT class and continued to decrease 6-months following the intervention. These continued effects are likely due to the coping skills learned, practiced, and adopted during LIFT.
Although participants in this study did not quit tobacco altogether, they reduced tobacco use by 50% at 6-months, the equivalent of 10 fewer cigarettes per day. This finding is significant for several reasons. Reducing tobacco use is associated with a parallel reduction in smoking-related health risk.14-16 These benefits are particularly striking for vulnerable populations such as PWD who experience significant health disparities. 3 In addition to benefits to health, tobacco reduction is also important if considered from an economic standpoint. In Ohio alone, a pack of cigarettes costs on average $6.10. 17 Cutting smoking by half notably reduces this daily economic burden, especially when considered over the long term. Over a month, the difference between buying 1 pack of cigarettes per day versus buying 1 pack of cigarettes per 2 days is a gain of $91.50. These savings are particularly meaningful for people with limited income, such as PWD and their caregivers.3,17 Taken together, LIFT was observed to reduce smoking by half in both PWD and their caregivers, and this tobacco reduction has lasting, positive health and economic benefits.
There were limitations to this study that should be considered when interpreting our results. First, the small sample size limited our power to detect statistical significance and tempered the generalizability of findings. Surprisingly, given the high rates of smoking in these groups, we found it difficult to recruit dyads of PWD and caregivers that were both ready to embark on tobacco cessation. Future research should attempt to evaluate readiness to quit tobacco in participants prior to intervention implementation to better understand each person’s unique place in the quit process. It may be the case that LIFT is best suited for people in the later stages of readiness to quit tobacco instead of people early in the process. Second, future research should attempt to empirically test the impact of including dyads of PWD and their caregivers in this and other health promotion interventions. Given that these relationships are powerful, intimate,6,7 and influence health behaviors, 8 it is important to test the potential for these relationships to support meaningful and lasting positive health behavior changes. Third, our decision to recruit 3 caregivers who did not smoke may have limited our ability to detect change in CO levels among caregivers. Fourth, our sample was fairly homogeneous and lacked racial and ethnic diversity. Further studies should aim to oversample from diverse populations to determine the extent to which LIFT materials resonate with various populations. Finally, future research is needed to explore the applicability of these findings to different disability populations and diverse types of caregivers (e.g., young versus old, paid versus non-paid, etc.). It is important to discern specifically who LIFT works for and who it does not to best situate researchers, educators, and policymakers to make informed decisions on effectively combating tobacco use in vulnerable populations such as PWD and their caregivers.
This study contributes to evidence on the importance of relationships between PWD and caregivers.6,7 Health behaviors of caregivers could either facilitate or impede health behaviors of PWD,18,19 and in the case of smoking behavior, a caregiver who smokes likely will impede cessation efforts of PWD they support. Our innovative approach of offering LIFT to PWD and their caregivers proved both feasible and effective. Inclusive health promotion programs, such as the LIFT dyad approach, are critical to achieve health equity, eliminate disparities, and improve population health.
Footnotes
Acknowledgements
The research team would like to thank the individuals who participated in this study and our external evaluator, Crane Research and Development, whose collaboration made this project possible. We are also grateful to Lindsay Gerhart, Sabrina M Moxcey, and Jamie L McGrath for their contributions to this study. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Ohio Department of Health.
Funding:
This project was supported by the Ohio Department of Health Cooperative Agreement No. RFP CSSP904017.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SMH, WRB, DE, EC, and IKR designed and coordinated the study protocol. SMH and WRB drafted the manuscript. WRB, DE, EC, and IKR collected the data. AL and CNWS conducted the statistical analyses and helped in drafting the manuscript. All authors read and approved the final manuscript.