
Abstract
Objectives:
To explore the perceived effectiveness of pictorial health warning (PHW) labels required by the Gulf Cooperation Council, to compare them with the Food and Drug Administration–approved PHW labels, and to determine factors affecting their perceived effectiveness.
Methods:
A cross-sectional study using a convenience sample of adult smokers and nonsmokers was conducted. The data were collected through a self-administered online questionnaire. The perceived effectiveness scores of PHW labels were calculated and compared among different subgroups using the Kruskal-Wallis test and the Dunn multiple comparison test at a .05 significance level.
Results:
Of the 90 people invited to participate in the survey, 77 (86%) completed it, with 39 (50%) nonsmokers, 22 (29%) smokers, and 16 (21%) former smokers. Overall, labels having graphic images of illness or pathology are perceived to be most effective. Smokers generally perceived labels significantly less effective compared with former smokers and nonsmokers. Also, 55 respondents (71%) suggested that the presence of a telephone quit-line would be effective.
Conclusions:
Smoking status and image type had the most effect on the perceived effectiveness of the PHW labels on cigarette packs. Pictorial health warning labels with graphic images of pathology and a telephone quit-line are perceived to be most effective.
Introduction
Tobacco consumption is the leading cause of preventable death worldwide. 1 Despite great prevention efforts and increasing awareness of its health hazards, globally, tobacco still kills almost 6 million people yearly. 1 In 2010, the World Health Organization (WHO) estimated that the prevalence of smoking was 11%, 16%, and 25% in Oman, Saudi Arabia, and Bahrain, respectively. If tobacco control efforts continue at the same intensity, WHO projects that in 2025 around 23% to 60% of the population in those countries will be smokers. 2 Gulf countries were classified as high consumption where mean consumption per daily smoker was greater than or equal to 20 cigarettes per day. 3
Tobacco control efforts have been advocated by the WHO through the Framework Convention on Tobacco Control articles and guidelines. Article 11 sets the guidelines for implementing and regulating packaging and labeling of tobacco products. 1 It requires to adopt and implement effective measures to prohibit misleading tobacco packaging and labeling and to ensure that tobacco product packages carry large, clear, rotating health warnings and messages that cover 50% or more, but not less than 30%, of principal display areas and that are in the countries’ principal language(s). 1
One of the important requirements of the 2009 US Food and Drug Administration’s (FDA) Family Smoking Prevention and Tobacco Control Act was to require a pictorial health warning (PHW) consisting of both a written warning and a graphic image on cigarette packs. 4 In 2009, the US FDA had required 1 of 9 colored images paired with health text warnings to appear on every cigarette pack, carton, and advertisement by September 2012. 4 However, tobacco industry litigation has prevented the 2009 Act from being implemented. 5 Therefore, cigarette packs in the United States only contain the text warning labels which have been on packs since 1985. 5
Pictorial warnings became mandatory on cigarette packages in all Gulf Cooperation Council (GCC) countries as of August 9, 2012. The GCC consists of Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates. In 2011, the GCC Standardization Organization adopted a standard, titled Labelling of Tobacco Product Packages, which requires picture-based health warnings to cover 50% of the cigarette package, front and back, with an Arabic warning on the front and an English warning on the back. 6 Currently, there are 3 different PHW labels appearing on cigarette packages sold in GCC countries.
In Qatar, Awaisu et al 7 surveyed 500 people to evaluate their awareness, beliefs, and perceptions on antitobacco PHW labels on cigarette packs before the new regulation was implemented. About one-third of respondents had no idea that there were any specific text warning messages on tobacco products, and nearly 45% did not know what a PHW was. More than 20% of the respondents did not believe that PHWs would change smoking behavior. 7 Nonsmokers tended to believe that PHWs would be more effective than did smokers. 7
These PHW labels were thought to reduce the influence of brand imagery on the pack and make smoking less appealing.4,8 Also, pictorial labels are essential in communicating health warnings to populations with low literacy rates. 7 In many countries, both smokers and nonsmokers perceived PHWs to be more effective than text-only messages.9–12 Prominent health warning labels that combine both pictures and text were more effective than text-only labels in educating smokers about the risks of tobacco, as well as promoting the idea of quitting,13,14 and in reducing the demand for cigarettes. 15
Different countries have used a variety of visual themes, including graphic depictions of health effects, symbolic or abstract images, and graphic depictions of human suffering or loss. 16 In addition to pictures, some countries have also required the package to contain a telephone quit-line—a phone number to a society or an organization that helps smokers quit. The quit-line is an important tool in tobacco control because it aids in cessation by increasing public reach to those services.17,18 Call volumes have increased after the implementation of warning labels that included these quit numbers.19–21 In some of the GCC countries, Kuwait and United Arab Emirates, a smoking cessation helpline exists; however, it is not included on cigarette packs.
The purpose of PHWs is to deter youth and young adults from starting to smoke, to encourage smokers to quit, and to reduce exposure to secondhand smoke.1,22 Therefore, it is essential to determine the most effective PHW labels in these groups 16 and the ones most culturally appropriate.22,23 There is need for further research to evaluate the effectiveness of PHW labels on cigarettes in the Middle Eastern region, especially in Gulf countries, where PHWs’ legislations are at its infancy. 7
Ideally, the actual effectiveness would be assessed by measuring the changes in attitude, belief, or behavior of the target population in observational studies to have high external validity. 24 However, isolating the effects of PHW labels on smoking behavior in such studies is difficult because governments often introduce the warnings alongside other tobacco control policies, such as changes in price/taxation, mass media campaigns, and smoke-free legislations. 25 In addition, testing the actual effectiveness is expensive, time-consuming, and often difficult and impossible to obtain. 26 Dillard et al 26 conducted a meta-analysis and concluded that the association between the perceived effectiveness and actual effectiveness was substantial and positive. Therefore, this study aimed to assess the perceived effectiveness of PHWs.
The objectives of this study were to explore the perceived effectiveness of the PHW labels required by the GCC, to compare them with the FDA-approved PHW labels and to determine factors affecting their perceived effectiveness. This study was conducted to test the following null hypotheses: PHW labels introduced by GCC are perceived to be equally effective as PHW labels approved by the FDA, smoking status does not affect the perceived effectiveness of PHW labels, and type of image does not affect the perceived effectiveness of PHW labels.
Methods
The research study was approved by the ethical research committee at the Faculty of Dentistry at King Abdulaziz University.
Survey development
The questionnaire consisted of 40 questions written specifically for this study. Written in English and Arabic, it included questions on demographic characteristics, financial status, and smoking status. The financial status was categorized as follows: inadequate and we need to take a loan, inadequate but we do not need to take a loan, adequate but we cannot save, and adequate and we can save. The smoking status was categorized as follows: smoker, former smoker, and nonsmoker. Finally, questions evaluating the PHWs were also included. These questions were adapted from Hammond et al 4 and slightly modified. The participants’ awareness of the quit-line and the participants’ opinion to include the quit-line on PHW labels were evaluated. The quit-line is not included on the cigarette packages sold in Saudi Arabia and Gulf countries.
To test the clarity and length of the questionnaire, a focus group of 20 people with both smokers and nonsmokers was done. Some modifications in the Arabic translation and the decision to reduce the number of PHW labels used due to length were made. Participants in the focus group were asked to select the 4 PHW labels they perceived as least effective. Therefore, the final questionnaire only included 3 PHW labels, which appear on cigarette packs sold in Saudi Arabia and introduced by the GCC, and 5 of the FDA labels.
The 8 PHW labels used in this study are identified by the photographic image they contain: (1) a child, (2) oral cancer, (3) healthy and cancerous lungs, (4) a man in an oxygen mask, (5) a corpse after autopsy, (6) a cigarette with a skull, (7) burned fingertips, and (8) a pregnant woman (Figure 1). The text messages on the FDA labels were translated into Arabic in the Arabic version questionnaire. These labels were presented in the same order for all participants.

Eight pictorial health warning labels used in the study to determine which would most deter smoking: (1) child, (2) oral cancer, (3) diseased lungs, (4) oxygen mask, (5) corpse, (6) a cigarette with a skull, (7) burned fingertips, and (8) pregnant woman.
Participants rated each of the 8 PHW labels on a 4-point Likert scale. The following question was asked for each of the PHW labels: Please rate the effectiveness of the following pictures in relation to the statements using a scale from 1 to 4, where 1 means that it is not effective at all and 4 means that it is very effective: (1) the picture is effective in smoking prevention, (2) the picture is effective in delivering the written message on the cigarette pack, (3) the picture makes smokers avoid buying the cigarette pack, and (4) the picture makes people more concerned about the health risk of smoking.
By adding the scores of all 4 items, dividing this score by the theoretical maximum (16 points), and multiplying the product by 100, we created a score that estimated the overall perceived effectiveness for each PHW label (in which a score of 100 was the highest and a score of 25 was the lowest). Participants also chose the most effective 3 images of the 8 PHW labels and ranked them in order of effectiveness.
The questionnaire was pretested before the study for clarity and to confirm that the questions were interpreted as intended.
Research design
A cross-sectional study using a convenience sample of adults was conducted and the target population was current smokers, former smokers, and nonsmokers who were at least 18 years old. Participants were recruited via WhatsApp and Facebook social media of the authors. An initial request regarding the smoking status (nonsmokers versus former smokers or smokers) was made. The first 45 nonsmokers and 45 former or current smokers were sent an invitation with a link to their social media account or the e-mail address linked to the account. Participants volunteered to complete the survey without any compensation.
The data were collected through an anonymous, self-administered online questionnaire (http://www.surveymonkey.com/). A link to the survey’s Web page was sent to the participants via e-mail. Three follow-up reminder messages were sent. A cover letter explaining the aim of the study, its voluntary nature, and a guarantee of anonymity was shown at the beginning of the online questionnaire. All participants consented to participate by completing the questionnaire.
Statistical methods
A priori power calculation with Stata software, version 13.1 (StataCorp, College Station, TX, USA), indicated that a sample of 70 respondents would have a 90% power of detecting a 0.4-point difference in mean rating scores. 16 Accounting for anticipated 20% nonresponse rate, 90 people were invited to participate in the study.
The internal consistency of the rating scale for each PHW label was assessed with Cronbach alpha. The perceived effectiveness of the PHWs across different subgroups was compared for the following variables: sex, smoking status, education level, and income. The Shapiro-Wilk test was used to check for normality of data distribution among the groups. The scores of labels were compared between men and women with the Wilcoxon rank sum test. Comparison of the scores for nonsmokers, former smokers, and smokers was conducted using the Kruskal-Wallis test and the Dunn test to adjust for multiple comparisons. The Kruskal-Wallis test and the Dunn test were also used to compare different groups with respect to education level and income. Alpha was set at 0.05, and all tests were 2-tailed. All data were analyzed with IBM SPSS version 22 (SPSS Inc., Armonk, NY, USA).
Results
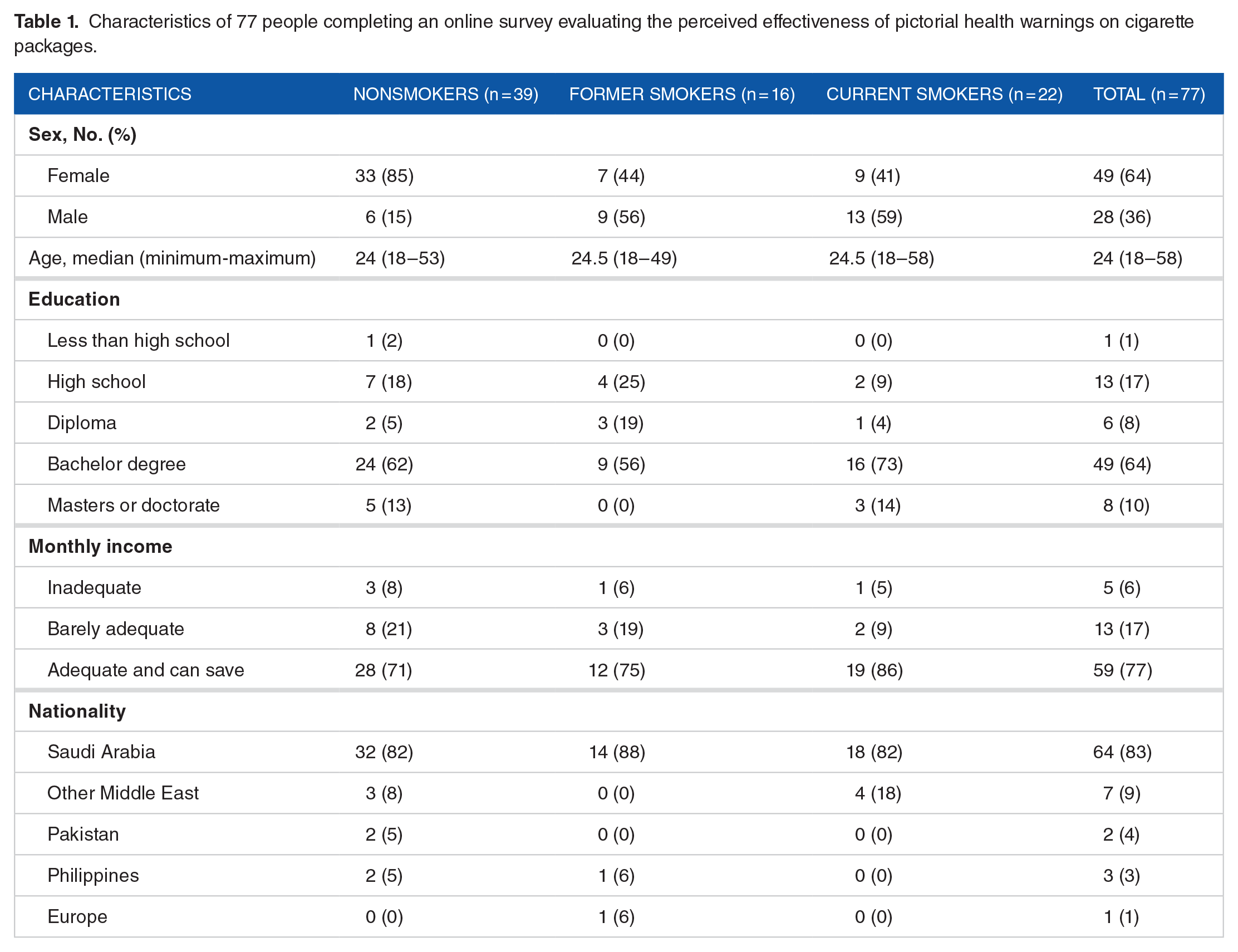
Of the 90 people invited to participate in the survey, 77 (86%) completed it, with 39 (50%) nonsmokers, 22 (29%) smokers, and 16 (21%) former smokers (Table 1). Sample characteristics of respondents who completed the online survey are presented in Table 1. In total, 71 respondents (92%) were from the Middle East and 49 (64%) were women, and the median age was 24 years with a range of 18 to 58 years (Table 1).
Characteristics of 77 people completing an online survey evaluating the perceived effectiveness of pictorial health warnings on cigarette packages.
Perceived effectiveness of PHW labels
Cronbach alpha for each of the 8 PHW labels ranged from 0.91 to 0.95, indicating excellent internal consistency of the rating scale for each PHW label. 27 The modal score of the item rating scale and the aggregate median and interquartile range of the 8 PHW labels are presented in Table 2. Labels 2, 4, and 5 (oral cancer, oxygen mask, and corpse, respectively) had the highest total scores (Table 2). Labels 6 (a cigarette with a skull) and 7 (burned fingertips) had the lowest total scores. When participants were asked to choose the 3 most effective PHW labels, participants ranked labels 2, 3, and 5 (oral cancer, diseased lung, and corpse, respectively) as the most effective.
Perceived effectiveness scores of 8 pictorial warning labels on cigarette packs.
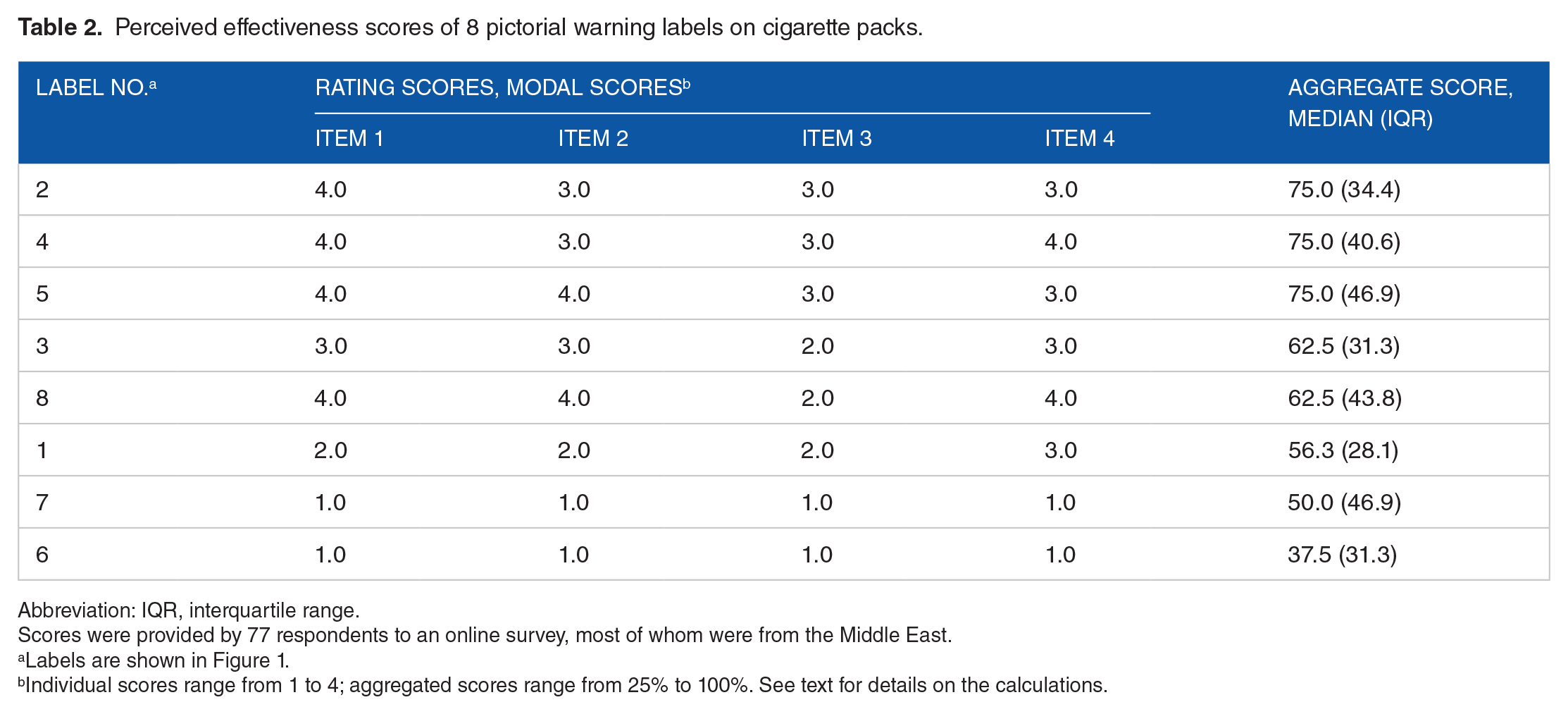
Abbreviation: IQR, interquartile range.
Scores were provided by 77 respondents to an online survey, most of whom were from the Middle East.
Labels are shown in Figure 1.
Individual scores range from 1 to 4; aggregated scores range from 25% to 100%. See text for details on the calculations.
Perceived effectiveness of PHW labels by smoking status
All groups rated labels 2 and 4 (oral cancer and oxygen mask) to be highly effective (Table 3). The scores of smokers, former smokers, and nonsmokers did not differ significantly in these ratings. However, the perceived effectiveness of PHW labels 3 (diseased lungs), 5 (corpse), and 8 (pregnant women) differed significantly by smoking status. In general, these 3 labels were perceived to be less effective by smokers than by nonsmokers and former smokers, and smokers differed significantly from former smokers (P = .01). In addition, smokers perceived PHW label 5 (corpse) to be less effective relative to nonsmokers and former smokers (P = .02 and P = .002, respectively). Similarly, smokers perceived PHW label 8 (pregnant woman) to be less effective than nonsmokers (P = .049).
Differences in the perceived effectiveness of pictorial health warning labels on cigarette packs between smokers, nonsmokers, and former smokers.
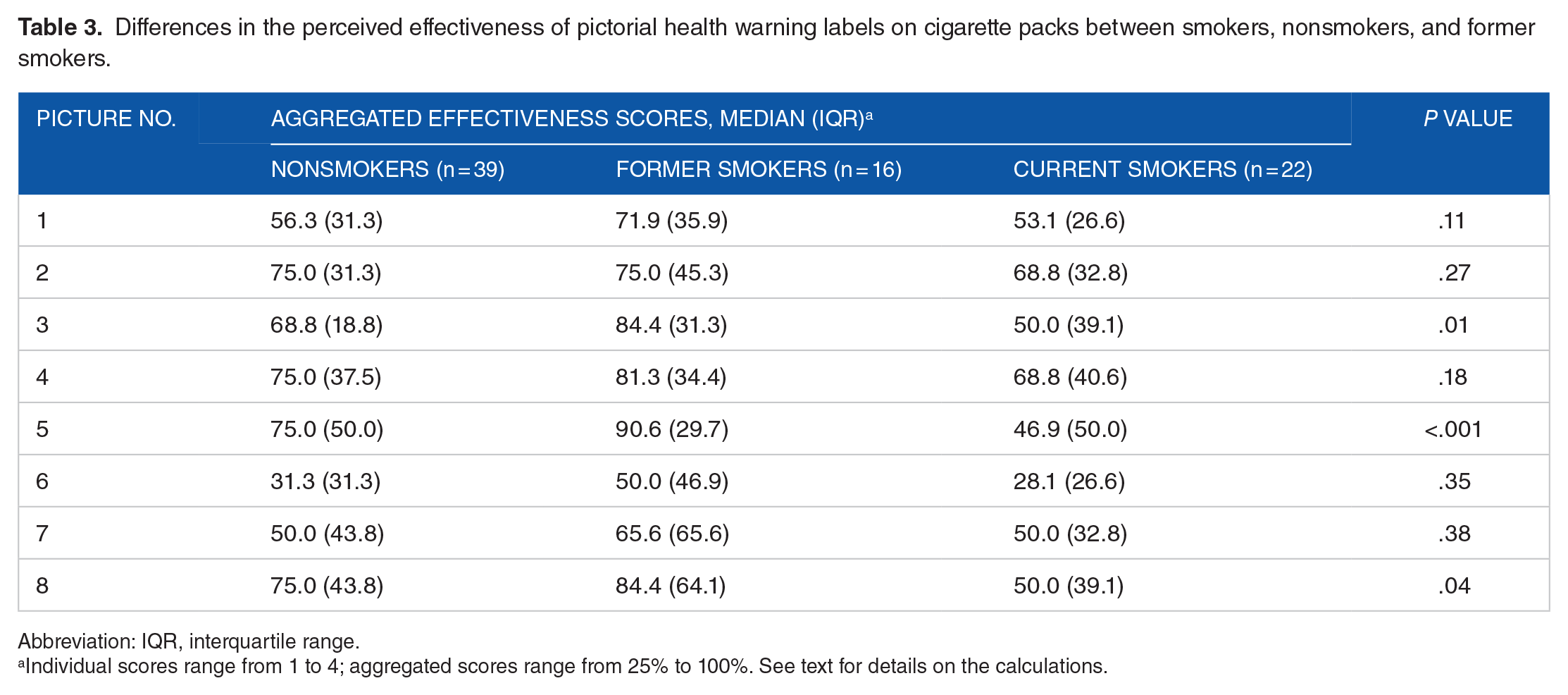
Abbreviation: IQR, interquartile range.
Individual scores range from 1 to 4; aggregated scores range from 25% to 100%. See text for details on the calculations.
Perceived effectiveness of PHW labels by sex, educational level, and income
Label 8 (pregnant woman) was the only label for which ratings differed by sex (P = .009)—women found it more effective than men—or by educational level, and even then only marginally significant (P = .049). Income did not affect the perceived effectiveness of the labels.
Characteristics associated with the perceived effectiveness of PHW labels
Of the 77 respondents, 55 (71%) identified the graphic images of illness or pathology (labels 2-5) as being most effective, whereas only 4 (5%) thought that abstract images (labels 6 and 7) were more effective.
Only 10 (13%) respondents knew what a telephone quit-line was, of which 7 of them did not know the exact number. Despite this poor awareness, 55 (71%) suggested that such numbers would be helpful.
Discussion
The findings of this study provide insights about the perceived effectiveness of PHW labels introduced by GCC compared with the ones approved by the US FDA and factors affecting their perceived effectiveness, such as image characteristics and smoking status. This study indicated that the type of image affects the perceived effectiveness of health warnings. More than 75% of our respondents thought that labels containing graphic images of pathology or illness would be highly effective, whereas only 5% found abstract symbolic images to be effective. This is consistent with the findings of Cameron et al, 28 which suggested that warning labels with images of diseased body parts are more effective than metaphorical images in eliciting fear-related reactions and discouraging young adults in the United States from smoking.
Labels 2 (oral cancer) and 4 (oxygen mask) had the highest total scores and were perceived equally effective by all groups. Both labels have graphic images showing pathology or illness. However, labels 6 (a cigarette with a skull) and 7 (burned fingertips) had the lowest scores and both used symbolic, abstract images. In a study in Mexico City, pictorial warnings featuring images of physical health effects either internal or external were also shown to be significantly more effective than symbolic images or experiences of human suffering. 12 Similar results were also reported in other studies in India, 10 Bangladesh, 10 and Southwest Nigeria. 29
Smoking status is another factor that may affect the perception to PHW labels’ effectiveness. Our study suggests that the perceived effectiveness of labels differed among smokers, former smokers, and nonsmokers. In general, smokers found some of the labels to be less effective than former smokers and nonsmokers. For example, labels 3 (diseased lungs), 5 (corpse), and 8 (pregnant women) differed significantly by smoking status and were perceived to be less effective by smokers than by nonsmokers and former smokers, and smokers differed significantly from former smokers. Only labels 2 (oral cancer) and 4 (oxygen mask) were rated highly by all groups. A study in Sarawak City, Malaysia, suggested that the Malaysian PHW labels were not very effective for certain target population. They may deter nonsmokers and early smokers from smoking, but they do not effectively increase the desire to quit, especially among current smokers. 30
In general, the perceived effectiveness of different PHW labels did not differ significantly by sex except ratings for label 8 (pregnant woman) which women perceived to be more effective compared with men. Other studies reported similar results where women rated pregnancy labels to be more effective compared with men.31,32 A study among adolescents in Southwest Nigeria found no association between perceived effectiveness and sex for images containing airway cancer, harm to children, stroke, or impotence. 29 Similar results of no significant association between sex and effectiveness ratings of PHW were also reported in Mexican youth. 12 However, female Mexican adults rated warnings significantly higher than men. 12
Similarly, the educational level had no effect on the perceived effectiveness of PHW labels except label 8 which people with higher education levels perceived to be more effective than people with lower education. This might be because PHW label 8 is complex, and this may be difficult to understand when initially viewed. Finally, income did not have an effect on the perceived effectiveness of PHW labels. However, the small sample size might have affected the power to detect a statistically significant difference.
Results for the telephone quit-line awareness revealed that more than 75% of the participants did not know what a quit-line number was. Despite this poor awareness, almost 75% suggested that its presence on the cigarette pack would be helpful in reducing tobacco use. A study of young adults in the United States suggested that adding a telephone quit-line number also significantly increased perceived effectiveness of the warning. 4 Another study in Canada, Australia, and Mexico reported that quit-line information and health warning labels on cigarette packs were independently and positively associated with calls to the quit-line. 33 The authors concluded that awareness of quit-lines and Web sites created by health warning labels was associated with increased use of these resources. 33
Study limitations and recommendations for future research
The study used a convenience sample which might not represent smokers and nonsmokers in different settings, and this limits the generalizability of the study results. There was a 13% nonresponse rate in the study; nonrespondents might have been smokers and held different views from those of respondents. The small sample size may have limited our statistical power to detect differences in the perceived effectiveness of PHWs in some factors, such as income and education level. Nevertheless, this study used an anonymous questionnaire to decrease response bias and social agreeability bias.
The novelty of FDA images compared with the PHW labels introduced by the GCC countries and sold in Saudi Arabia may have affected the perceived effectiveness of the PHW labels; however, the results of this study showed that even the FDA PHW labels were perceived differently. In addition, some of the participants were from non-GCC countries and would therefore not be influenced by this factor.
The perceived ineffectiveness of the PHWs introduced by the GCC is an important factor to consider. We need further research on a larger scale to explore the most effective health warning for the Gulf countries’ population and to include a quit-line on cigarette packages and to further support the findings of this study.
Conclusions
Our data support the conclusions that smoking status and image type had the most effect on the perceived effectiveness of PHW labels on cigarette packs. Graphic images of pathology or illness were perceived to be more effective than symbolic or abstract images. Therefore, these findings demonstrate that some warnings introduced by the GCC could be improved for greater impact and also provide useful insights for exploring the policy of including graphic images of pathology, illness, or suffering, along with a quit-line, on cigarettes sold in Saudi Arabia to increase the effectiveness of health warning labels.
Footnotes
Peer Review:
Five peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1773 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AM contributed to the questionnaire and study design, participant recruitment, statistical analysis, and initial and final draft. ZB contributed to the questionnaire and study design, participant recruitment, and initial and final draft. All authors read and approved the final draft.
Disclosure and Ethics
As a requirement of publication, author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including, but not limited to, the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.