
Abstract
Due to limitations of neuroimaging, such as the isodense appearance of blood to neuronal tissue in subacute hemorrhagic stroke, a body of studies have been performed to evaluate candidate biomarkers which may aid in accurate determination of cerebrovascular accident type. Beyond aiding in the delineation of stroke cause, biomarkers could also confer useful prognostic information to help clinicians plan use of resources. One of the candidate biomarkers studied for detection of cerebrovascular accident (CVA) includes a class of proteins called galectins. Galectins bind β-galactoside through a highly conserved carbohydrate recognition domain, endowing an ability to interact with carbohydrate moieties on glycoproteins, some of which are relevant to CVA response. Furthermore, galectins-1, -2, -3, -9, and -12 are expressed in tissues relevant to CVA, and some exhibit characteristics (eg, extracellular secretion) that could render feasible their detection in serum. Galectins-1 and -3 appear to have the largest amounts of preclinical evidence, consistently demonstrating increased activity and expression levels during CVA. However, a lack of standardization of biochemical assays across cohort studies limits further translation of these basic science studies. This review aims to increase awareness of the biochemical roles of galectins in CVA, while also highlighting challenges and remaining questions preventing the translation of basic science observations into a clinically useful test.
Keywords
Introduction to Cerebrovascular Accidents
Interruption of arterial supply to the brain initiates a cascade of events, which present as neuronal and glial cell death, culminating as loss of function in neuron networks. 1 Histologic analysis of ischemic neuronal tissue shows characteristic features including presence of eosinophilic cell bodies and pyknotic nuclei. 2 The pathophysiology preceding these histologic findings is classified broadly into 2 distinct categories: ischemic cerebrovascular accident (CVA), which includes ischemic strokes and transient ischemic attacks (TIAs), and hemorrhagic CVA, which encompass hemorrhagic strokes. 3
Ischemic stroke comprises about 87% of total CVA cases and results from a thrombotic or embolic blood vessel blockage.4,5 Underlying atherosclerosis in arterial blood supply may lead to development of a thrombus that can obstruct vessels and precipitate ischemic stroke. 4 Ischemic strokes can also be caused by small vessel occlusions, called lacunar strokes, which are strongly associated with hypertension and diabetes.4,6 In addition, ischemic strokes can be caused by an embolus from a more distal part of the body, such as a left atrial embolus in a patient with atrial fibrillation, or as a venous embolus in patients with a patent foramen ovale. 4
Similar to an ischemic stroke, TIA is a neurological event in which stroke-like symptoms are displayed, but which resolve within 24 hours without persisting signs of infarction. 7 As seen in ischemic stroke, the cause of a TIA is temporary blockage of blood supply to the brain. 7 However, unlike in ischemic stroke, patients who develop TIA lack of permanent symptoms is due to a reperfusion of the penumbra, an area of shocked tissue, which remains viable after reperfusion. 3 In summary, the pathophysiology of TIAs is similar to that of ischemic strokes, with clinical differences manifesting due to differences in the response to the initial embolic or atherosclerotic lesion. 8
Hemorrhagic stroke comprises the remaining 13% of CVA cases and is defined as the atraumatic collection of extravascular blood within the cranial cavity, classified by anatomic involvement, such as intracerebral, subarachnoid, and intraventricular hemorrhages. 5 Intracerebral hemorrhage involves atraumatic bleeding into brain parenchyma or the ventricular system. 3 Causes include rupture of vascular malformations, aneurysms, and also other conditions that weaken vessel integrity. 8 Next, a subarachnoid hemorrhage is defined as atraumatic blood accumulation in the subarachnoid space.3,9 Possible causes of subarachnoid hemorrhage range from ruptured aneurysm, arteriovenous malformation, arterial dissection, cerebral vasoconstriction syndrome, cerebral amyloid angiopathy, and infective endocarditis (source of septic emboli) as well as other conditions that weaken vessel integrity.9-12 In summary, all mechanisms of hemorrhagic stroke lead to extravascular pooling of blood that elevates intracranial pressure and initiates inflammatory damage that culminates as regional ischemia and cell dysfunction. 13 Products of erythrocyte breakdown that occur after hemorrhagic stroke can trigger edema, further worsening neuronal and glial damage. 14
When a patient presents to the emergency department with suspected CVA, initial management centers on ruling out alternative conditions that may mimic a stroke, including hypoglycemia and electrolyte derangements. 5 Prompt evaluation of symptoms and signs concerning for a CVA is then performed, aided by standardized assessments such as the National Institutes of Health (NIH) stroke scale.4,15 Accurate diagnosis is critical, given that thrombolytic therapy for ischemic stroke worsens a hemorrhagic stroke. Among these patients, a history and physical examination affords a 91% sensitivity for detecting the presence of a CVA, but is only 48%-76% sensitive and 68%-96% specific in distinguishing the cause of the stroke as ischemic or hemorrhagic. 16
Therefore, to further define CVA cause, patients presenting with a new-onset focal neurologic deficit typically receive a computed tomography (CT) scan of the head without contrast to assess for hemorrhage or a large ischemic infarct. 17 An appropriate alternative or subsequent study is a magnetic resonance imaging (MRI) of the head, which yields superior sensitivity to CT of the head in detecting an acute ischemic infarct with the cost of requiring more time to perform. 17 Although neuroimaging plays a salient role in establishing a diagnosis of stroke, several shortfalls exist in sole reliance on 1 imaging modality. CT of the head has a low sensitivity for detecting lesions in the posterior fossa due to imaging artifacts from bony structures, yielding a 54.5% positive predictive value (PPV) (95% confidence interval [CI] 32.2-75.6) for detecting posterior fossa ischemia. 18 Further complicating diagnosis, a late subacute hemorrhagic stroke appears isodense to normal brain tissue on CT 8 days to 1 month following the initial event. 19 In summary, the low sensitivity and moderate specificity of the clinical examination, combined with the nuances in accurate interpretation of neuroimaging studies, suggests an opportunity to improve acute stroke care through development of biochemical assays that distinguish between the different types of stroke.
Given the described limitations of clinical examination and neuroimaging, biochemical tests with reasonable sensitivity and specificity in distinguishing the cause of the CVA (eg, hemorrhagic or ischemic) would address an unmet clinical need. Although many other biomarkers are under study, this review focuses on a class of proteins called galectins that have been implicated in multiple risk factors for CVA, including hypertension, atherosclerosis and hyperlipidemia, and diabetes mellitus. We assess the potential galectins may offer as biomarkers in CVAs, based on current literature describing the pathophysiologic and biochemical roles galectins assume within CVA.
Biochemistry of Galectins
A number of galectins, each encoded by a separate gene, have been identified in human tissues: galectins-1, -2, -3, -4, -7, -8, -9, -10, and -12.20-28 Galectins-1, -2, -3, -9, and -12 (Table 1) are each expressed in a number of tissues relevant to cerebrovascular disease. Galectin-1 has been determined to be expressed in various tissues including epithelium, vasculature (specifically fibroblasts), 29 mesenchyme, and thymus.30-33 Galectin-2 has been shown to be present in gastrointestinal epithelial tissue. 34 Galectin-3 is expressed in vascular tissue, specifically the adventitia 35 and in cardiac myocytes, 36 as well as in macrophages, monocytes, neutrophils, eosinophils, mast cells, and lymphocytes.37-42 Galectin-9 and -12 have each been shown to be expressed in adipose tissue.43,44 Because of their presence in select tissues deemed relevant to cerebrovascular disease, we focus on galectins-1, -2, -3, -9, and -12 and their physiologic roles.
Overview of the expression profile and function of galectins shown to be relevant to CVA.

Abbreviations: CVA, cerebrovascular accident; TIA, transient ischemic attack; GI, gastrointestinal; vWF, von Willebrand Factor; KO, knockout.
Galectins are a subclass of the lectin family of proteins that interacts with carbohydrates. Galectins share functional ability to bind to β-galactoside, mediated structurally by a common and conserved carbohydrate recognition domain (CRD). The CRD is a 130-residue sequence conserved across all 15 types of galectins. 45 Due to the presence of homologous CRDs, each of the 15 described galectins weakly interact with individual monosaccharides and instead typically function through multivalent interactions with oligosaccharides, which are also called glycans, as reviewed. 46 Accordingly, all galectins are able to form complex quaternary structures and then noncovalently interact to form lattice structures that enable multivalent interactions with carbohydrate moieties, as reviewed and portrayed elsewhere.45,46 In summary, galectins bind carbohydrates, including carbohydrate moieties added by post-translational modifications to proteins.
The cellular localization of galectins-1, -2, -3, -9, and -12 can affect the ability of biochemical tests to detect them. Galectin-1 is localized on the plasma membrane of cells as well as intracellularly and is known to be secreted.47,48 The secretion mechanism of galectin-1 and for galectins as a class of proteins does not involve the endoplasmic reticulum pathway as reviewed. 49 Galectin-3 is expressed in the plasma membrane of various cells and in the cilia of ciliated epithelial cells.47,50,51 Galectin-3 is secreted by cells and has been found to have intracellular and extracellular functions in modulating the immune response. 52 Galectin-2 is secreted by multiple cells in the gastrointestinal tract and has been determined to be a part of the detergent resistant portion of the enterocyte brush border membrane. 53 Galectin-9 is localized extracellularly, while also being found in the cytoplasm and is secreted by the Tim-3 pathway.54,55 Galectin-12 has been detected intracellularly in adipocytes, but has been shown to not be secreted in significant amounts.44,56 In summary, galectins-1, -2, -3, and -9 are secreted into the extracellular space, rendering them presumably more useful for study in biochemical tests performed on peripheral blood.
Despite the similarity of the CRDs, galectins are classified into 3 groups based on their tertiary structure: prototypical, tandem repeat, and chimeric, all of which appear to be relevant to CVA. Prototypical galectins have 1 CRD, tandem-repeat galectins have 2 CRDs, and lone chimeric galectin has a single CRD, but forms higher order oligomers (Table 1). Of the galectins observed to be relevant to CVA, galectin-1 (galectin-1) and galectin-2 (galectin-2) are prototypical, galectin-3 (galectin-3) is chimeric, and galectin-9 (galectin-9) and galectin-12 (galectin-12) are tandem-repeat galectins (Table 1). The unique quaternary structures and the distinct lattice structures, which each galectin can form, endow each of the galectins with distinct functions by affecting the 3-dimensional orientation of potential multivalent interactions. 46 The glycosylation of a broad range of proteins comprises a structural explanation for how galectins engage in a wide role of functions, as reviewed. 57 Galectins only possess 1 conserved known functional domain, the CRD, but galectins can be trafficked into either the extracellular compartment, cytosol, or nucleus. Galectin-1 and galectin-3 can be trafficked to the nucleus, where they interact with ribonucleoproteins that regulate RNA splicing via the CRD.58-60 In summary, most of the functions attributed to galectins occur through chemical interactions mediated through their CRD.
As an example, glycosylation is a post-translational modification that occurs on a broad range of proteins. Galectins bind N- and O-glycans that are present following glycosylation in the endoplasmic reticulum or Golgi apparatus. Given that glycoproteins are found in a wide array of pathways, the ability of galectins to bind to β-galactoside endows them a broad array of functions. For example, galectin-3 binds vascular endothelial growth factor receptor 2 and von Willebrand Factor (vWF) to modulate angiogenesis and hemostasis, respectively.61,62 Of note, novel functions of galectins have been identified recently, so future studies may elucidate additional pathophysiologic functions for galectins in CVA.63-65 In this review, the galectins involved in the biochemistry and pathophysiology of CVA are discussed, based on the published body of literature that shows galectin-1, galectin-2, galectin-3, galectin-9, and galectin-12 as relevant to CVA.
Risk Factors for CVA and Galectins
Atherosclerosis
Modifiable risk factors for stroke ordered by decreasing relative risk for stroke include hypertension, atherosclerosis, diabetes, smoking status, and cardiovascular disease. 66 The role of galectins in atherosclerotic disease was reviewed previously by Al-Ansari et al, 67 and we offer a brief overview of the pathophysiology of these risk factors before providing a summary of key roles for galectins in these processes. Dietary lipids enter into the blood stream, carried by chylomicrons absorbed in the gut. Free cholesterol esters, in a chemical equilibrium with the fraction bound to chylomicrons, are released into the blood and can diffuse through endothelial cell adhesions. Macrophages are known to scavenge these subendothelial spaces, endocytosing the chylomicrons. However, macrophages are unable to fully metabolize cholesterol esters, and the resultant lipid-laden macrophage is called a foamy cell. These foamy cells are directly involved in the pathogenesis of atherosclerosis as they release myriad signaling molecules that cause smooth muscle cells in the tunica media to proliferate, which leads to fibrosis. This causes an irreversible thickening and stiffening of the tunica intima, thus creating a structure that has the potential to rupture and form a thrombus. Risk factors for atherosclerosis include hypertension, hyperlipidemia, diabetes, smoking, obesity, and lack of exercise. 68 These are also aforementioned risk factors for stroke, highlighting the importance of understanding a very significant role of atherosclerosis in CVA.
Hypertension
A paucity of literature assesses the role of galectins in essential hypertension independent from other comorbidities such as diabetes and heart failure. However, uncontrolled hypertension confers a relative risk (RR) for CVA of 1.91 in men, 1.68 in women, rendering it the most significant of the aforementioned risk factors. 69 Hypertension contributes to hemorrhagic stroke by promoting rupture of small penetrating arteries deep within the brain. 70 Hypertension also increases risk for ischemic stroke through shear stress that worsens progression of atherosclerosis. 71 Finally, reduction in blood pressure to normotensive levels causes a 35%-40% reduction in total CVA risk. 72 Given the influence of hypertension on CVA risk, roles of galectins pertinent to CVA are assessed.
Clinical observational studies show correlation between serum galectin-3 elevation and events mediated by long-standing hypertension, such as adverse cardiac remodeling. Based the observations that galectin-3 is secreted by activated macrophages 73 and its levels peak with worsening fibrosis in patients with heart failure, 74 a single-center cross-sectional study was performed in China to assess whether galectin-3 levels correlate with worsening left ventricular (LV) hypertrophy. 75 The study enrolled 107 patients with essential hypertension, but who lacked other comorbidities that affect the vasculature, including renal disease, diabetes mellitus, and coronary artery disease. 75 These patients, alongside 108 age- and sex-matched controls underwent 2-dimensional echocardiography to evaluate LV posterior wall thickness, inter-ventricular septal thickness, and LV ejection fraction. Of the total 107 patients, 55 demonstrated LV remodeling, whereas 52 patients did not. Each of the 52 patients lacking adverse cardiac remodeling were on an angiotensin converting enzyme (ACE) inhibitor, which blocks conversion of angiotensin I into angiotensin II, leading to less secretion of aldosterone. 76 ACE inhibitors therefore decrease retention of salt and water to lower blood pressure, while also decreasing aldosterone-mediated signaling mechanisms that cause adverse cardiac remodeling, as discussed. 76 A multivariate regression analysis showed that serum galectin-3 and body mass index (BMI) were independent predictors of adverse LV remodeling, with an area under the receiver operating characteristic curve of 0.698 (P < 0.001), whereas b-type natriuretic peptide showed an area of 0.54 (P < 0.347). In summary, the authors of this cross-sectional study hypothesize that aldosterone-mediated adverse LV remodeling is at least partially mediated through a galectin-3-dependent mechanism.
In support of this hypothesis, inhibition of galectin-3 expression in a rodent model prevents aldosterone-mediated type I collagen synthesis, vascular fibrosis, and heart failure. 77 Further studies to assess whether elevations in galectin-3 occur via aldosterone-dependent mechanisms are warranted. In summary, galectin-3 likely represents a biomarker of fibrosis 78 and correlation has been observed between elevated serum galectin-3 and negative sequelae of hypertension such as adverse cardiac remodeling.
Hyperlipidemia
Preclinical studies suggest galectins play direct roles in the pathogenesis of plaque formation and rupture. Galectin-1 has been observed to enhance DNA synthesis and also interact with α1β1-integrins and extracellular matrix proteins to interrupt adhesion of smooth muscle cells, as observed in carotid endarterectomy samples. 79 These cell cycle changes are thought to promote smooth muscle cell migration, as reviewed elsewhere. 67 Galectin-1 has also been observed to cause lipoprotein-A accumulation within the sub-intimal plaque, which affects the likelihood of plaque rupture. 80 A genome-wide association study conducted as part of an autopsy study (n = 1503) found that elevations in galectin-2 were associated with severity of coronary atherosclerosis but that this did not correlate with clinical MI. 81 Galectin-2 can bind BRCA1-associated protein (BRAP), which is expressed on smooth muscle cells and macrophages in atherosclerotic plaques of Asian populations. 82 In summary, galectin-1 and galectin-2 appear to promote migration of smooth muscle cells, which results in disorganization of the 3-dimensional tissue structure within the tunica intima.
Further supporting a role for galectins in atherosclerosis, genetic studies have correlated allele variants in galectin-2 with increased risk for atherosclerosis. The sequence of lymphotoxin-α (LTA), a pro-inflammatory protein, putatively involved in atherosclerosis, was studied alongside galectin-2.83,84 The homozygous variants LGALS2 3279TT and LTA 252GG correlated with increases in expressed levels of galectin-2 protein and the pro-inflammatory protein LTA, respectively. 85 In an experimental group containing ischemic stroke patients, it was less common to have both genes (P < .0009, N = 74). 85 This observation suggests that galectin-2 function may positively influence ischemic stroke outcomes and prompts the need for animal model studies that can test for a mechanistic explanation for how alterations in galectin-2 levels affect stroke outcome. 85 The matter of a potential protective role for galectin-2 in this instance will require further investigation before more conclusions can be drawn.
Galectin-3 also appears to exhibit pro-atherogenic effects through promotion of monocyte migration 86 into tissue and through modulating their differentiation into macrophages. 67 Elevations in serum galectin-3 are reported both in rabbit models of atherosclerosis and also in human samples from patients with atherosclerosis. 87 Monocytes that differentiate into macrophages upregulate expression of galectin-3, 88 and galectin-3 subsequently is chemotactic at high concentrations, enabling recruitment of additional monocytes. 89 With additional macrophages present in the tissue, more foamy cells are generated via inevitable uptake and inability to process lipids, worsening atherogenesis. These foamy cells continue to secrete galectin-3, to thus continue recruitment of monocytes into the tissue. 90 To assess the potential for elevations in galectin-3 to aid in diagnosis and prognosis of atherosclerotic disease, a Dutch prospective cohort study (n = 7968) found that serum galectin-3 elevations correlate with all-cause mortality, age, and risk factors for cardiovascular disease (median follow-up of 10 years). 91 In summary, galectin-1 and galectin-2 aid migration of cells (eg, monocytes) between the endothelial cells, and galectin-3 is secreted by both activated macrophages and foamy cells to ultimately recruit more monocytes into the atherosclerotic plaque, and these galectins may serve as a useful prognostic marker for atherosclerosis.
Analysis of blood samples and surgically collected tissue from carotid endarterectomies, procedures that aim to reduce thrombotic stroke risk, suggest a prognostic role may be possible for galectin-3 and atherosclerosis. Galectin-3 measured in human blood samples was present in levels that correlate (P < 0.001, N = 199) with the thickness of tunica intima and tunica media in the carotid artery, a marker of atherosclerosis. 91 Galectin-3 is known to be expressed by inflammatory cells,38-42 can be found in vascular tissue, and already has established value as a diagnostically accurate marker of peripheral artery disease. 37 Other studies support the observation that increased tissue levels of galectin-3 correlate with unstable plaque regions (P < 0.01, N = 9), 92 (P < 0.001, N = 78). 93 In summary, given that atherosclerosis is a risk factor for stroke, the predictive value of galectin-3 found in plasma has the potential to be a valuable future test for assessing the presence of this risk factor.
Diabetes mellitus
Endothelial dysfunction is a sequela of both type 1 and 2 diabetes mellitus that results from oxidative stress secondary to hyperglycemia. The increase in reactive oxygen species is caused by overproduction of superoxide by mitochondria in the endothelial layer surrounding blood vessels. 85 Oxidative stress from hyperglycemia can lead damage to cellular structures, notably membranes. 92 The ensuing disruption in cellular signaling and transport could account for the increased vascular permeability that is seen in many patients with diabetes. 92 Non-enzymatic glycosylation of the endothelium positively correlates with worsening hyperglycemia and has been shown to have a direct relationship with endothelial dysfunction. 92
Nitric oxide synthase (eNOS) is synthesized in the vascular endothelium, and its product, nitric oxide, plays a role in the maintenance of vascular tone, membrane integrity, and coagulation as well as thrombosis. 93 Advanced glycation end products (AGEs) have been shown to form at higher rates in patients with hyperglycemia and to downregulate the production of eNOS, which the authors of the study speculate may be due to repression of expression. 39 In addition, diabetes mellitus may cause a hypercoagulable state in patients with metabolic syndrome compounding stroke risk factors. 92 In conclusion, hyperglycemia from diabetes mellitus creates an environment in which reactive oxygen species and AGEs are present in higher levels and thus cause damage to the endothelium.
Some studies suggest galectins may help to mitigate formation of AGEs through induction of mechanisms to alleviate hyperglycemia. In mice with diet-induced type 2 diabetes, deletion of galectin-3 was shown to downregulate glucose transporter type 4 (glut-4) in the endothelium by immunofluorescence studies, aggravating hyperglycemia. 94 Furthermore, galectin-3 knockout (KO) diabetic mice were shown to have increased clotting tendencies as well as greater levels of endothelial dysfunction. 94 Darrow et al 94 suggest additional studies are warranted to test whether galectin-3 plays a protective role in keeping the otherwise highly upregulated coagulation cascade at a lower level in diabetic mice.
Consistent with the putative protective function of galectins against hyperglycemia, elevations in serum galectins have been observed in models of diabetes. In a preclinical study, a homozygous Tie2-GFP mouse model with type 2 diabetes was fed a high-fat diet. Both the galectin-3 protein and its transcripts were upregulated by enzyme-linked immunosorbent assay (ELISA) and real-time polymerase chain reaction (PCR), respectively (P < 0.05), in the endothelium relative to the controls. 94 In addition, a positive correlation (P < 0.05 at 3 weeks and P < 0.01 at 8 weeks) between levels of galectin-3 and insulin resistance was observed in diabetic mice. 94 To ascertain whether galectin-3 is protective or harmful in diabetes pathogenesis, the authors of the study suggest the use of galectin-3 inhibitors and treatments with galectin-3 on mice to assess whether galectin-3 inhibition alters the natural course of the disease. The presence of some protective effect in similar studies on high-fat diets in diabetic mice may also be investigated because it was shown later that galectin-3 may provide endothelial protection due to attenuation of the coagulation cascade. 95 Similarly, galectin-1 is observed to be increased (P < 0.01) by real-time PCR in endothelial cells of rats with type 2 diabetes in which glucose was administered. Furthermore, in humans, galectin-1 was shown to be increased (P < 0.05) by 4.8 times in plasma samples obtained from type 2 diabetic patients. 96 These studies support association of elevations in galectin-1 and galectin-3 that correlates with diabetes pathogenesis.
Galectin-3 has previously been shown to bind AGEs. 97 AGEs can form in response to hyperglycemia and can cause endothelial dysfunction.92,98 In the retina, vascular endothelial growth factor (VEGF) mediates hyperglycemia-mediated hypervascularization, which leads to deleterious effects on the blood retinal barrier. Galectin-3 KO diabetic mice exhibited decreased VEGF levels relative to wild-type controls (P < 0.001). 97 However, this effect is not seen in all studies, suggesting the correlation needs further characterization. 95 The authors conclude that effects of galectin-3 KO in diabetic mice may vary with region of endothelium that is affected, an idea that raises questions about other regional differences in endothelium as it relates to galectin-3 expression. In summary, studies agree that elevations in galectin-1 and galectin-3 occur during the pathogenesis and progression of diabetes, but it is unclear whether the elevations in these galectins are a response that aims to protect against hyperglycemia-mediated adverse events, or which worsens them.
Lifestyle
Smoking
Galectin levels appear to vary with smoking status. Observational data enable an association between serum galectin-3 levels and smoking status through comparison of never-smoker, current smoker, and ex-smoker groups, with current smokers having the highest blood levels of galectin-3. 99 Current smokers compared with never-smokers showed an increase in galectin-3 levels in the acute exacerbation (P = 0.036) and convalescence (P = 0.045) phases of chronic obstructive pulmonary disease (COPD). 99 In the case of former smokers in acute exacerbation (P = 0.424) and convalescence (P = 0.578) phases, no significant difference between never-smokers and former smokers existed, indicating that after smoking cessation, an individual’s levels of galectin-3 return to baseline levels. 99
Diet and obesity
Galectin-3 serum levels appear to positively correlate with increasing BMI. Elevations in galectin-3 have been observed to correlate with obese BMI in humans (P < 0.05) and mice (P < 0.001) compared with normal weight controls. 100 In mice, addition of greater amounts of galectin-3 led to insulin resistance, whereas reduction of galectin-3 levels through galectin-3 inhibitor compound 47 or galectin-3 KO led to greater sensitivity to insulin (P < 0.01). 100 In humans, galectin-3 blood levels were shown to be positively correlated with BMI (R = 0.344, P < 0.05), suggesting a correlation between galectins and human obesity. 100 In contrast, another study involving galectin-3 KO mice showed increased body weight in the KO mice relative to controls (P < 0.05, N = 10) after weeks 19 and 20 of age. 101 Although findings reflected an improvement in insulin sensitivity through inhibition of galectin-3, 46 benefits of galectin-3 in diabetes also include improved control of coagulation cascade activation in a diabetic mouse model. 95 In conclusion, further studies could be performed to test the utility of galectin-3 inhibition in diabetes and to weigh the benefits and harms of galectin-3 administration verses inhibition in a diet-induced type 2 diabetic mouse model.
Mice with diet-induced obesity (DIO) have been shown to have higher levels of galectin-1 and galectin-3, but lower galectin-12, within their adipose tissue than lean mice. 44 In addition, a high-fat diet led to increased levels of galectin-1 (P < 0.01) and galectin-3 (P < 0.01) in both the lean and DIO groups, with the DIO group showing the largest jump. 101 Galectin-9 mRNA (no galectin-9 protein) was found to be increased (P < 0.01) in the subcutaneous adipose tissue of obese mice relative to visceral adipose tissue in response to the high-fat diet the mice were experimentally fed. 101 Galectin-12 was shown to be decreased (P < 0.01) in DIO mice relative to the control group. 101 In a study on the development of adipocytes in mice, galectin-12 levels were shown to be elevated in pre-adipocytes as they entered cell cycle arrest prior to differentiating into adipocytes. 43 Using galectin-12 siRNAs to bring about RNA interference, galectin-12 levels were significantly decreased in pre-adipocytes. This led to a lower level of lipid droplets in mature adipocytes (determined by fluorescence microscopy), indicating that galectin-12 is required for differentiation into adipocytes without defective lipid storage. 43 This study showed a role for galectin-12 in the development of adipocytes in mice and raises further questions about the role of galectin-12 in obesity. In summary, the tissue levels of galectins-1, -3, and -12 appear to be altered in obesity.
A study was conducted on obese children (N = 45) and healthy children (N = 35) to determine the relative levels of galectin-1 found in serum. 102 Galectin-1 was shown to be negatively correlated with fasting glucose levels in the obese subject group (P = 0.020). 102 Galectin-1 levels were also shown to be positively correlated with waist circumference (WC) (P = 0.027) and fat mass (P = 0.026) in obese children. 102 In healthy children, galectin-1 levels were determined to correlate with waist circumference (P = 0.031). 102 In addition, galectin-1 levels were shown to be significantly higher in obese children compared with healthy children in this study. 102 These observations suggest the elevation of galectin-1 seen in the tissue also manifests as elevations of galectin-1 within the serum.
Given the role of galectin-12 in adipocyte development, a murine in vivo study was conducted to assess the effects of various traditional Chinese herbs on levels of galectin-12 expression, while observing changes in weight. 103 It was determined by high-throughput screening that corn silk extract and β-sitosterol downregulated expression of galectin-12. 103 Furthermore, corn silk extract and β-sitosterol applied to pre-adipocytes led to diminished levels of lipid droplets in adipocytes. 103 Corn silk extract and β-sitosterol were each administered orally to mice resulting in decreased weight and decreased numbers of adipocytes. 103 In conclusion, this study in conjunction with earlier studies43,44 indicates a role for galectin-12 in obesity and adipocyte differentiation and that there are molecules that can modulate galectin-12 levels within murine adipocyte tissue.
Although galectins have been shown to be altered in conjunction with various risk factors for stroke (Table 2), their clinical value remains mostly unclear in this theater as further studies are needed. Of note is the role of galectin-12 in adipocyte formation and its relation to obesity and potential weight loss in mice. Downregulation of galectin-12 has been shown to lead to impaired adipocyte formation, and this has been applied in a study in which chemical extracts determined to downregulate galectin-12 levels in mice brought about weight loss.47,49 This finding warrants further investigation into galectin-12 as an obesity treatment. Recent studies on the role of galectin-12 specifically in obesity (a risk factor for CVA) have shown promise, but further investigation is also necessary before clinical conclusions can be drawn.
Alterations in tissue levels of various galectins, and their association with risk factors for CVA.

Abbreviation: CVA, cerebrovascular accident.
Green upward arrows denote increases and red downward arrows denote decreases. Grey-shaded boxes denote lack of data.
Although galectin-9 levels have been shown to vary within different tissues of obese mice, there was no variation shown between obese and healthy mice.
Exercise
Exercise has been shown to alter levels of galectin-3. Athletes have been shown to have higher (P = 0.006) baseline levels of galectin-3 mRNA in their blood than non-athlete controls. 104 In addition, galectin-3 levels were shown to increase in both groups after exercise (P < 0.001), with endurance athletes returning to baseline levels first. 104 The authors of the study suggest that elevation in levels of galectin-3, which is known to be associated with cardiovascular disease, may be similar to elevation in IL-6 levels that also occurs after exercise. 104 It was also noted that the 2 most experienced runners from the study showed the lowest increase in galectin-3 levels, with galectin-3 and IL-6 levels after exercise being inversely correlated with running experience. 104 It was proposed that this phenomenon may be due to the body adapting to long-term exercise by releasing less galectin-3. 104 This study shows the limitations of galectin-3 levels as a screening measure for cardiovascular health due to their correlation with patients who exercise. 104 Another study corroborated the finding galectin-3 levels increase (P < 0.001) above baseline following exercise. 105
Role of galectins in atherosclerosis-related inflammation
The role of inflammatory cells and activated macrophages in the development of atherosclerosis has been acknowledged previously and reviewed in depth in the past. 106 An aberrant immune response to smoking, obesity, and hyperlipidemia is considered to partially account for the contributions of these risk factors to atherogenesis. 107 As the macrophage response to lipid deposits is central to the mechanism of atherosclerotic plaque formation,107,108 it is intriguing to consider the possible roles of galectins in atherosclerosis pathogenesis. This seems likely because, so far, other than direct bacterial killing,109,110 galectins seem to be involved in regulating inflammation, particularly macrophage polarization and cytokine secretion.111-113
Galectin-1 has been demonstrated to have a role in attenuating inflammation from both an observed reduction in inflammatory cytokines 114 and from a disease presentation standpoint in the reduction of gross inflammation. 115 Galectin-1’s pro-inflammatory role has also been demonstrated through activation of the MAP-kinase pathway leading to increased levels of IL-6 and tumor necrosis factor alpha (TNF-α) among other pro-inflammatory cytokines. 116 Galectin-2 has also been demonstrated to have pro-inflammatory affects, promoting the expression of pro-inflammatory cytokines TNF-α, IL-6, and IL-12 in macrophages. 117 Conversely, galectin-2 has also been shown to act as a downregulator of inflammation by inducing apoptosis of CD8+ T-cells in the event of contact allergy in mice. 118 The effects of galectin-3 on inflammation have been widely studied 119 with the effects on inflammation being somewhat varied. Galectin-3 has been shown to act as a driver of alternative macrophage activation, 120 while having inhibitory effects on the production of reactive oxygen species in neutrophils. 121 In summary, galectins-1, -2, and -3 each modify macrophage-mediated secretion of cytokines associated with damaging pro-atherogenic inflammation (eg, IL-6).
In the pathogenesis of atherosclerosis specifically, galectin-3 has been demonstrated to promote inflammation in human umbilical vascular endothelial cells (HUVECs) treated with oxidized low-density lipoprotein (Ox-LDL), through activation of the β1-RhoA-JNK pathway. 122 A relevant observation given HUVECs are considered an in vitro model for human endothelium. 122 Evidence for activation of β1-RhoA-JNK was provided by Western Blot analysis that detected elevated levels of integrin β1, RhoA, and JNK after treatment of HUVECs (pretreated in both the control and experimental groups with Ox-LDL) with galectin-3. 122 Furthermore, the inflammatory role of the β1-RhoA-JNK pathway was examined through the measurement of inflammatory cytokine levels, including IL-6, IL-8, and IL-1β, by ELISA after integrin β1 knockdown and JNK inhibition, respectively. 122 The findings were that integrin β1 knockdown (P < 0.05) and JNK inhibition (P < 0.05) each led to significantly lower levels of IL-6, IL-8, and IL-1β, giving evidence that the β1-RhoA-JNK pathway is pro-inflammatory. 122 In conclusion, galectin-3 was shown to be a potential activator of the β1-RhoA-JNK pathway, which has demonstrated pro-inflammatory effects on oxidized low-density lipoprotein treated human vascular endothelial cells. 122
These results are supported by the observation that in vitro berberine (BBR) administration led to downregulation of galectin-3 in macrophages, which resulted in less macrophage activation, quantified by lower levels of Ox-LDL uptake, using red oil O stain, and inflammatory cytokine expression, using real-time PCR (P < 0.01). 123 The potential causal role of galectin-3 in this instance was evidenced by viral vector-induced overexpression of galectin-3 in macrophages that were also treated with BBR. 123 Subsequent measurement of Ox-LDL using red oil O stain and inflammatory cytokine levels, using real-time PCR (P < 0.01), revealed that viral vector-induced overexpression of galectin-3, compared with the control group treated with a null virus, negated the inhibitory effects of BBR on macrophage activation. 123
As endothelial damage from Ox-LDL is a step in the progression of atherosclerosis, 124 understanding the role of galectin-3 as an inflammatory activator is important. There is evidence demonstrated by in vitro studies that galectin-3 promotes inflammation implicated in the pathogenesis of atherosclerosis.122,123 Furthermore, the β1-RhoA-JNK pathway has been offered and demonstrated experimentally as a mechanism through which galectin-3 induces inflammation. 122 These data suggest that study of the impact of small molecule inhibitors to galectin-3, such as BBR, on quantification of the of Ox-LDL uptake by macrophages 123 in animal models would represent a rational future direction prior to future clinical studies.
In summary, galectins have been shown to be related to a number of modifiable stroke risk factors including hypertension, hyperlipidemia, atherosclerosis, and diabetes mellitus as well as various lifestyle aspects including smoking status and activity level. Many of these risk factors are also involved in the pathogenesis of atherosclerosis, which is strongly impacted by inflammatory states as a segment of its pathogenesis. 121
Activity of galectins in ischemic stroke
Following an ischemic stroke, cellular debris accumulates as cells undergo hypoxia-induced liquefactive necrosis, and thus, macrophages are required to respond to the accumulation of this debris. Macrophage inhibitory factor (MIF) is a cytokine with pleiotropic effects on the immune response to injury or foreign microbes, as reviewed. 125 MIF is widely expressed, including within monocytes, macrophages, and neurons. Neurons secrete MIF, causing tissue levels to increase after experimental stroke. 126 Mixed observations are available on the influence of MIF on ischemia. Studies pertinent to galectins include the observation that neurons lacking MIF were found to have a greater rate of survival following transient occlusion of the middle cerebral artery via decreased apoptosis; therefore, MIF expression is associated with less neuron survival. 127 To explore this mechanism, an MIF KO mouse model led to the observation that galectin-3 levels were upregulated, which suggests galectin-3 elevations (putatively from endothelial cells and immune cells) may correlate with the improved response to ischemia in these mice. 127 Accordingly, administration of galectin-3 to mice following cerebral ischemic infarction led to increased angiogenesis and proliferation of neural progenitors, perhaps explaining the previous findings. 128 These mechanisms are thought to be mediated by VEGF, to which galectin-3 binds and activates. In summary, this mouse model provides preclinical evidence that galectin-3 may foster improved neuronal and neuroglial survival following ischemia.
In humans, heritable deficiency in Adamts13 causes a thrombotic microangiopathy, with the canonical mechanism being mediated by large, uncleaved vWF that circulates and promotes thrombosis. Adamts13 deficiency therefore increases stroke risk. A murine Adamts13 KO model showed decreased neovascularization in mice following ischemic stroke, with a correlated decrease in galectin-3 in brain microvessels. Administration of recombinant galectin-3 normalized the ability of these mice to undergo angiogenesis in response to ischemic injury and therefore supports galectin-3 as a factor that promotes recovery after stroke. 129 Galectin-3 is able to promote phosphorylation of VEGFR-2 by a carbohydrate-dependent interaction and promotes its retention on the plasma membrane to lengthen duration of pro-angiogenic signaling.61,62 In summary, preclinical studies show that galectin-3 may play a role in capillary sprouting and angiogenesis, mechanisms key to resupplying penumbra with arterial supply following CVA.
Clinical studies assessing galectins in CVA tend to focus on galectin-1 and galectin-3. A prospective longitudinal cohort study enrolled 30 239 patients in the Southeastern United States between 2003 and 2007, and determined baseline plasma galectin-3 levels for 1453 participants selected by a stratified sampling method to include high-risk groups. 130 Within this cohort of 1453 people, by 2011, a total of 526 developed an ischemic stroke. Using a case-cohort study design, serum galectin-3 levels in the upper 2 quartiles were associated with 2.3-fold increased stroke risk (95% CI = 1.6-3.4). 130 Similarly, a nearly concomitant prospective cohort study, based on data analysis of a single-blind, blinded end-points, randomized controlled trial across 26 institutions in China and the United States (n = 3082), stratified patients with acute ischemic stroke by serum galectin-3 levels, collected at their baseline prior to CVA. 131 Multivariate odds ratios (OR), which adjusted for other patient characteristics that may be risk factors, showed elevations in serum galectin-3 correlate with increased risk for the primary outcome: major disability or death within 14 days following ischemic stroke, with a multivariate OR of 1.43 (1.05-1.93). 131 A positive, linear association between baseline serum galectin-3 and the primary outcome was observed, suggesting that high baseline galectin-3 may represent increased risk for ischemic stroke. However, notably, a lack of statistical significance was reported in the secondary outcome of 3-month all-cause mortality, OR = 2.10 (0.89-4.95). 131 The authors conclude that additional prospective studies—and potentially therapeutic trials of small molecule galectin-3 inhibitors 132 —are necessary to further elucidate the relationship of galectin-3 and ischemic stroke.
In a cohort of 558 Swedish patients who underwent carotid endarterectomy, an association between elevated galectin-3 levels and post-operative CVA risk was shown (hazard ratio 15.1, with 95% CI 1.3-172.2; P = 0.028). 133 However, in another study based on a cohort of 8444 participants, a clinically useful biomarker called NT-proBNP (N-terminal-pro-brain natriuretic peptide; a sensitive sign of ventricular dysfunction and volume overload 134 ) and galectin-3 both exhibited statistically significant predictive power for all-cause mortality, but with NT-proBNP having a higher power. 135 The hazard ratio for ischemic stroke in this study did not have statistical significance. 135 These results are congruent with the results of a pilot study that assessed whether galectin-3 is a predictive biomarker following ischemic stroke, based on a prior study showing galectin-3 is a predictive biomarker following intracerebral hemorrhage. 136 Although these aforementioned studies support the concept that galectin-3 serology may correlate with prognosis, a Nebraska community cohort study (n = 1824) found NT-proBNP and high-sensitivity cardiac troponin 1 to be superior to galectin-3 for prediction of “major adverse cardiac events” that included TIA or stroke. Galectin-3 did not produce a statistically significant hazard ratio in their clinical model. 137 In summary, galectin-3 appears to have a positive association with poor prognosis following ischemic stroke, and a meta-analysis assessing the utility of galectin-3 in diagnosis and prognosis of ischemic stroke may be warranted.
Galectins in TIA
Galectin-1 serum levels appear to increase during TIA. The chemical effects of transient forebrain ischemia were investigated in a rat model through study of the relationship between Fos-B and galectin-1. 138 Fos-B is initially activated during transient forebrain ischemia. 138 Fos-B is a component of the AP-1 complex (activator-protein-1), which binds to DNA to regulate transformation and growth of cells as well as apoptosis. 139 In rat embryonic cortical cells, higher expression of galectin-1 was demonstrated by immunofluorescence microscopy in the presence of Fos-B when compared with the control indicating that galectin-1 is expressed downstream of transient forebrain ischemia in response to Fos-B. 138 Furthermore, increased galectin-1 levels were shown to lead to higher (P < 0.05) proliferation in embryonic cortical cells when compared with controls. 138 In addition, higher levels of galectin-1 were detected by immunofluorescence microscopy following transient ischemia in the hippocampus of the rat brain versus the control. 138 These data suggest that galectin-1 has potential as both a chemical marker of forebrain ischemia and in stimulation of proliferation after transient ischemia. 138
Similar to galectin-1, elevations in tissue galectin-3 also appear to be positively correlated with TIA. An investigation into galectin-3 levels after transient middle cerebral artery (MCA) occlusion was conducted in a rat model of TIA. 140 Galectin-3 levels were shown to be increased in the striatum as determined by histological stain 1 day after the transient ischemia had been induced and reperfusion had occurred. 140 Based on chemical markers found in sections of the brain, it was suggested that activated microglial cells and macrophages were the primary source of elevated galectin-3 in the MCA occlusion induced transient ischemia. 141 Galectin-3 was shown to stimulate proliferation of endothelial cells and neural cell progenitors in cell culture on a dose-dependent basis (P < 0.05 for 5 µg/mL and P < 0.01 for 10 µg/mL). 140 The findings of this study indicated a role for galectin-3 released by microglia and macrophages in remodeling via enhancement of angiogenesis and neurogenesis following transient brain ischemia in rats. 140 Further studies conducted on rats in vivo could focus on the effects of administration of galectin-3 to further establish a causal link between galectin-3 and angiogenesis and neurogenesis.
In the event of stroke, body temperature increases have been shown to occur that are associated with poor patient outcomes, with the temperature increases also correlating with the severity of the stroke. 142 Knowledge of this has prompted interest in conducting studies that induce hypothermia as a therapy in an attempt to minimize damage. 142 A study was conducted to test levels of galectin-3 in connection with induced hypothermia and hyperthermia in a gerbil transient ischemia model. 143 Expression of galectin-3 was shown by immunohistostaining to only occur in the CA-1 region of the hippocampus (pyramidal neurons there are highly vulnerable to ischemia) after transient forebrain ischemia has occurred in gerbils.143-145 Furthermore, mild hyperthermia of increasing increments from 37°C to 39°C was demonstrated by immunohistochemical study to enhance the expression of galectin-3 following the transient forebrain ischemia. 143 In addition to this, levels of galectin-3 were determined by immunohistochemical study to be lower in the event of induced hypothermia after transient forebrain ischemia. 143 Because of increased neuron cell death that occurs in the induced hyperthermia group relative to the induced hypothermia group, and the increased galectin-3 levels in the hyperthermia group relative to the hypothermia group, the authors of the study suggested that galectin-3 expressed by microglia plays a role in influencing survival of CA-1 neurons in the hippocampus. 143 Given the connection between galectin-3 and survival of CA-1 neurons in the hippocampus, further tests could attempt to manipulate levels or activity of galectin-3 to evaluate the effects on the forebrain following transient ischemia and temperature changes. The extent to which neuronal cell death occurs in further studies would shed additional light on the role of galectin-3 in brain ischemia.
Expression of galectin-3 in the CA-2 region of the hippocampus was shown to be elevated in gerbils following transient forebrain ischemia. 146 Galectin-3 expression and cell death following transient forebrain ischemia were determined to be significantly decreased (P < 0.05) by hypothermia and anti-apoptotic agents such as Tosyl phenylalanyl chloromethyl ketone (TPCK), 2-Deoxy-D-Glucose (2DG), and Sham-operated control (Sham-op). 146 The authors concluded that the suppression of galectin-3 expression is correlated with a decrease in neuronal cell death. 146 Further studies into this specific scenario could include a direct inhibition or addition of galectin-3 to establish a causal link to neuronal cell death.
In summary, galectin-1 levels were shown to be elevated in the event of transient forebrain ischemia in gerbils. Furthermore, galectin-3 expression in gerbils was detected in the CA-1 region of the hippocampus specifically in the event of transient forebrain ischemia. Galectin-3 levels in gerbils have also been shown to be increased in the CA-2 region of the hippocampus in the event of transient forebrain ischemia. Finally, transient ischemia caused by MCA occlusion in rats resulted in increased galectin-3 levels in the striatum. Further investigation into the specific roles of galectin in each scenario is required, with potential focus being placed on a link between galectin levels and outcome both on a cellular response level and an animal model level. Additional studies on interventions to alter levels or activities of galectin-1 or galectin-3 and to show a causative role in improvement of outcomes are required before any clinical investigations are conducted.
Galectins in hemorrhagic stroke
After intracerebral hemorrhage, plasma galectin-3 has been shown to be elevated (P < 0.001) in patients relative to controls. 141 Galectin-3 was shown to have a strong correlation with C-reactive protein (an acute-phase reactant that acts as a non-specific marker of inflammation) levels and to correlate with blood volume contained within the hematoma created by the hemorrhage. 141 In addition, galectin-3 levels were also shown to act as a predictive biomarker, with higher levels correlating with mortality at the 1 week (P = 0.008) and 6 month (P < 0.002) marks following intracerebral hemorrhage. 141 Furthermore, higher levels of plasma galectin-3 were shown to be associated with lower 6-month survival (P = 0.001) and higher 6-month unfavorable outcome (P = 0.005). 141 Finally, when combined with National Institute of Health Stroke Scale (NIHSS) scores (a stroke scale to predict patient outcome based on risk factors) 147 and hematoma volumes, levels of galectin-3 were shown to improve the predictive value of each method. 141
After aneurysmal subarachnoid hemorrhage, patient plasma levels of circulating galectin-3 were shown to be higher than the controls (P < 0.001). 148 Galectin-3 levels were also shown to be higher in patients who survived 6 months after suffering an aneurysmal subarachnoid hemorrhage compared with patients who did not survive 6 months (P < 0.001). 148 In addition, levels of galectin-3 in patients who had suffered an aneurysmal subarachnoid hemorrhage were higher in patients with bad outcomes than patients with favorable outcomes (P < 0.001). 148 The predictive value that plasma galectin-3 levels offer regarding subarachnoid hemorrhage outcome was shown to be similar to that of World Federation of Neurosurgical Societies (WFNS) scores, which predict subarachnoid hemorrhage outcome (P < 0.001) 149 and modified Fischer scores, which also predict subarachnoid hemorrhage outcome (P < 0.001).148,150
In a study conducted on patients who had experienced non-severe subarachnoid hemorrhage, acute-stage levels of galectin-3 in blood were measured to investigate a relationship with neurovascular events and other bad outcomes. 151 Patients with bad outcomes were determined (P = 0.026) to have higher galectin-3 levels compared with patients that had positive outcomes. 151 In addition, levels of galectin-3 were determined to be an independent predictor of poor outcomes (P = 0.001). 151 Based on this study, plasma galectin-3 levels measured on days 1-3 after a non-severe subarachnoid hemorrhage may be valuable as a biomarker for determining the likelihood of bad outcomes in patients that have experienced non-severe subarachnoid hemorrhage (Table 3). 151
Changes in levels of galectin-1 and galectin-3 that occur in response to different types of cerebrovascular accidents.
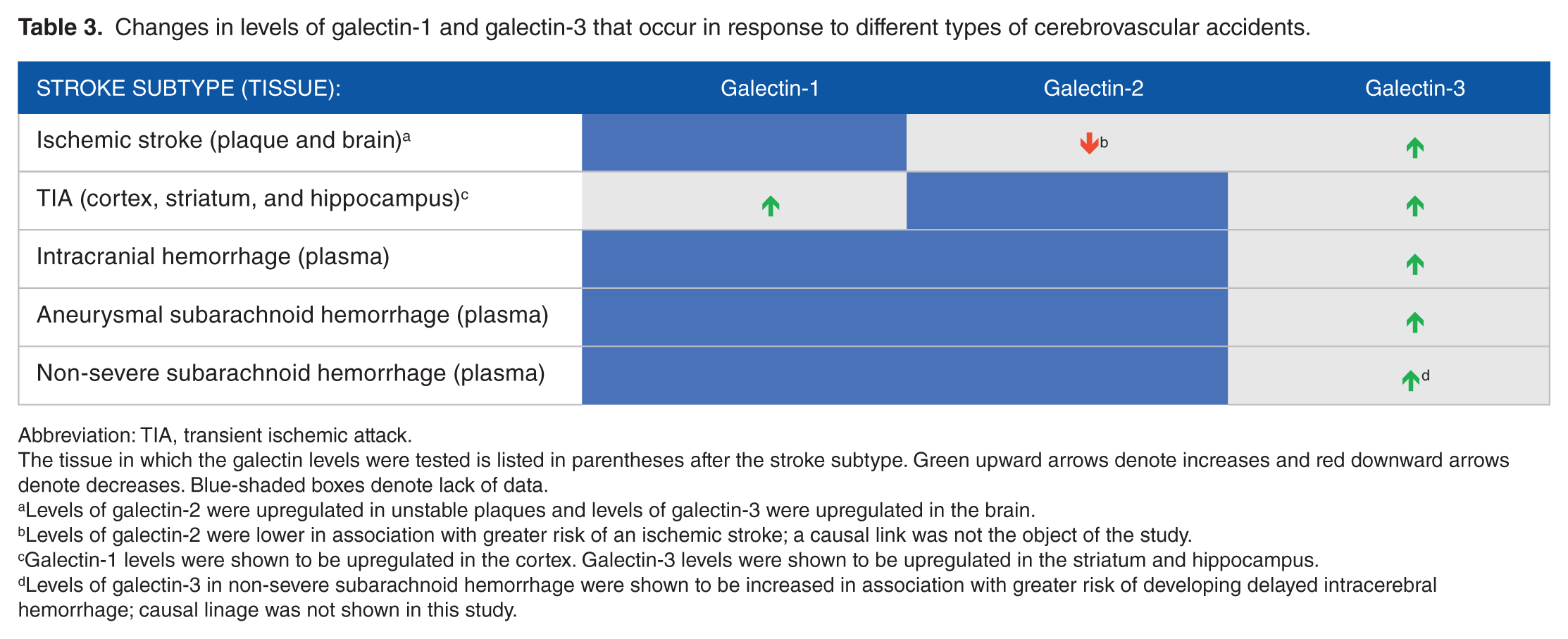
Abbreviation: TIA, transient ischemic attack.
The tissue in which the galectin levels were tested is listed in parentheses after the stroke subtype. Green upward arrows denote increases and red downward arrows denote decreases. Blue-shaded boxes denote lack of data.
Levels of galectin-2 were upregulated in unstable plaques and levels of galectin-3 were upregulated in the brain.
Levels of galectin-2 were lower in association with greater risk of an ischemic stroke; a causal link was not the object of the study.
Galectin-1 levels were shown to be upregulated in the cortex. Galectin-3 levels were shown to be upregulated in the striatum and hippocampus.
Levels of galectin-3 in non-severe subarachnoid hemorrhage were shown to be increased in association with greater risk of developing delayed intracerebral hemorrhage; causal linage was not shown in this study.
Conclusions
A body of preclinical studies appear to show elevations in plasma galectin-3 has potential value as a prognostic indicator across stroke types, including ischemic stroke, intracerebral hemorrhage, aneurysmal subarachnoid hemorrhage, and non-severe subarachnoid hemorrhage. Furthermore, tissue expression of galectins-1 and -3 is associated with improved outcomes following ischemic stroke, putatively due to enhanced angiogenesis and neurogenesis. However, measurement of tissue levels is not useful clinically. But additional preclinical studies that assess the effect of inhibitors of galectins on measurable stroke outcomes appear to be a rational next step. Once performed, these studies may inform rationale for a clinical trial assessing the effects of inhibiting galectins following CVA.
A significant challenge limiting the utility of the current body of clinical studies of galectins in CVA is an inconsistency in the type of biochemical assay used, as well as the threshold levels used to define elevations, as further reviewed elsewhere. 152 Makris et al., who authored a review of various biochemical markers in CVA, explain that variability of the individual assays confounds these results, even to the extent that meta-analysis is unlikely to be useful. 152 Although the preclinical science suggests that clinical study of galectin-1 and galectin-3 in CVA is warranted, ultimately a standardized assay needs to be defined to further increase the utility and comparison of these studies. With consistent and comparable studies, the sensitivity and specificity of galectin-based assays for either detecting CVA cause or determining prognosis can be developed, a critical step prior to translation to the clinic. Although galectin-1 and galectin-3 meet the criteria outlined for potential biomarkers,153-155 the employment of standardized assays in future investigation is necessary if any translation to the clinic is to occur.
Footnotes
Acknowledgements
The authors thank Dr Guy Benian, MD, and Dr Sergio Arce, MD/PhD, for comments and edits to the manuscript. W.F.A. and C.R.F. contributed equally and are co-first authors.
Funding:
C.R.F. was supported by a Howard Hughes Medical Research Fellowship.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
W.F.A. and C.R.F. wrote equivalent parts of the article, critically reviewed each other’s sections, and made all the revisions. A.V.B. conceived, supervised, was involved with all aspects, as well as performed general coordination of the project. All authors read and approved the final manuscript.