
Abstract
In the last decade or more, there have been reports suggesting a rise in the incidence of stroke in young adults. Presently, it appears that the risk factors associated with the cause of stroke in young adults remain relatively constant across different geographic regions of the world. Moreover, the endogenous rhythm of a neurohormone such as melatonin is known to play certain roles in the modulation of some of the risk factors that are associated with an increased risk of stroke in young people. Whereas animal studies have shown that melatonin plays diverse roles in stroke, only a limited number of human studies examined the roles of exogenous melatonin administration in the prevention of stroke, attenuation of neuronal damage, and improving outcome or well-being in stroke patients. In this review, first we summarize existing studies of stroke in the young adult and then provide insights on melatonin and stroke. Thereafter, we discuss the role of melatonin in models of stroke and how melatonin can be regulated to prevent stroke in young adults. Finally, we highlight the possible roles of melatonin in the management and outcome of stroke, especially in the young adult stroke population.
Introduction
Cerebrovascular disease is a spectrum of disorders that include defined entities like stroke and cerebrovascular anomalies/malformations. 1 In the last half decade or more, stroke has continued to be named as the second and the third most common cause of mortality and morbidity, respectively.2,3 Despite the fact that the age-standardized incidence of stroke-related mortality is decreasing, the rise in stroke burden continues globally 4 ; also becoming significant are racial and geographic differences in stroke burden. 5 Although generally less common, stroke in the pediatric age groups may be particularly associated with high morbidity and mortality. 6 Several studies7-9 suggest a gradual rise in the incidence of cerebrovascular disease in young adults, especially in low- and middle-income economies. This suggests an increase in research into the causative factors and better modalities to prevent stroke among young adults.
Modulations of the established stroke risk factors or the presence of under-recognized risks such as sleep deprivation have been reported to be directly associated with an increasing incidence of stroke in young adults. 10 Observational and experimental studies11-13 demonstrate the possible roles of sleep and sleep disorders in stroke irrespective of age categories. A recent study also reported evidence of racial and sex disparities in the association between sleep duration and stroke incidence among persons aged 45 years and above. 14 Sleep disorders are also known to affect treatment outcomes, rehabilitation, and stroke recovery. 15 The influence of sleep on long-term recovery from stroke is associated with the effect of stroke in disrupting pineal melatonin secretion to alter melatonin/circadian rhythms. 16 Even when melatonin rhythm was maintained post stroke, a delay in the phase of melatonin secretion was noticeable. 17 In this context, how the sleep-wake cycle influences stroke onset especially during shift work and how melatonin, a key modulator of the circadian rhythms, fits into this puzzle, especially in young adults, are important issues of this review.
In general, melatonin is a very important antioxidant and free radical scavenger. 18 Its neuroprotective functions 19 and role in stem cell therapy have also been reported. 20 Findings indicate the importance of melatonin in stroke management and the prevention of stroke recurrence. However, current knowledge on the link between the circadian rhythm, sleep disorders, and melatonin on stroke in young adults is still fragmentary. This review examines the possible roles played by melatonin in neuroprotection against ischemic injury in young adults and future translation in the treatment and prevention of stroke. However, it is important to emphasize that the views advanced here are from some of the initial and current attempts to conceptualize how understanding the impact of the circadian rhythm and melatonin can be translated to prevention and management of stroke in young adults.
Stroke in young adults
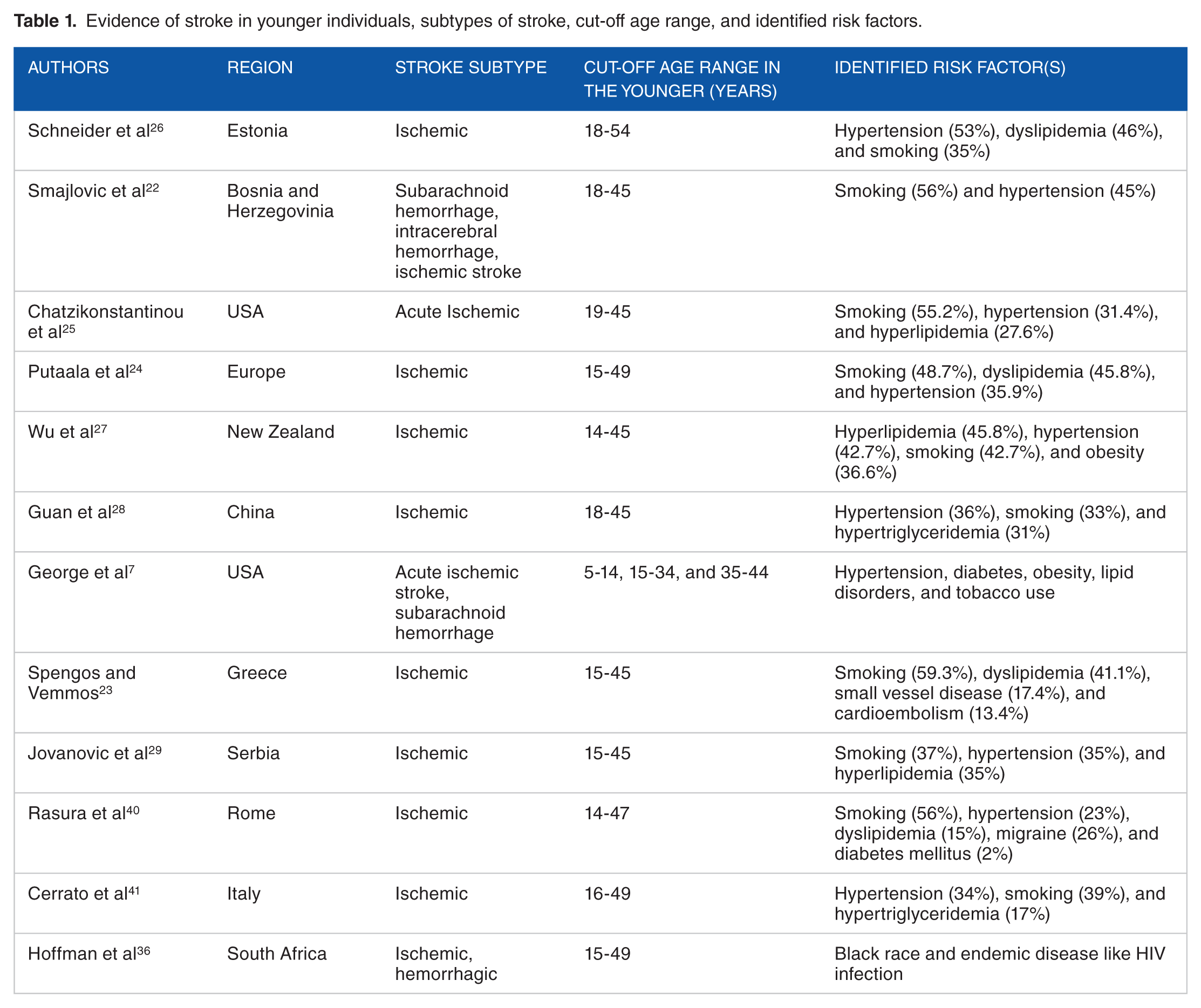
Stroke is usually not associated with young age; a period of life supposedly “filled” with health and vibrancy. Commonly, epidemiology would associate the development of stroke with aging, and as such younger individuals with stroke had previously been described as “invisible.”21-23 Although the perception of stroke as a disease of aging still persists within the larger population, research has continued to show a gradual rise in stroke incidence in persons younger than 55 years. 7 However, there is no specific definition of the term “Stroke in the young adult”, neither is there a unified age limit for the classification of stroke in young individuals. Although different studies used varying age cut-offs, the upper age limit for most studies through the years rarely exceeds 55 years.7,24,25 Table 1 summarizes the evidence of stroke in younger individuals, subtypes of stroke, cut-off age range, and identified risk factors.
Evidence of stroke in younger individuals, subtypes of stroke, cut-off age range, and identified risk factors.
In the last few years, there have been suggestions of a rising incidence of acute stroke events in adolescents and young adults, 9 with an increase in the incidence of acute ischemic strokes in both male and female young adults. 32 Although previous epidemiological reports had generally linked higher occurrences of hemorrhagic strokes in young adults, 33 more recent reports are attributing the rise in strokes in this age group to an increased incidence of ischemic strokes, rather than hemorrhagic stroke.7,9 The risk factor patterns of stroke in the young adults have also been reported to differ, when compared with older persons.9,34,35 Although the incidence of traditional stroke risk factors like cigarette smoking continues to decline in the overall adult population, obesity, metabolic syndrome, diabetes, dysmetabolism, and hypertension have shown little difference or worsened in the young adult population. 36 The rise in the incidence of ischemic stroke in young adults has been attributed to the increasing trends of multiple traditional risk factors including obesity, dyslipidemia, diabetes, and hypertension in young adults.7,37,38
In young adults between the ages of 15 and 44, approximately 50% of stroke events have been reported to be ischemic, 20% arise from an intracerebral hemorrhage, whereas 30% are subarachnoid hemorrhage. 31 Irrespective of the subtype or severity, the functional outcomes and recovery of younger patients with stroke are known to be better when compared with the elderly.28,39 However, despite the evidence of a better physical recovery in younger stroke victims, the impact of stroke on social, emotional, and economic well-being of younger patients is significant.40,41 The increasing incidence of stroke among young adults calls for more innovative research to reduce this problem. Most especially, the development of a standardized methodology that focuses on multicenter design and clarification of the term “young adults” with specific diagnostic and classification criteria will strengthen the existing epidemiologic data. The resulting data will allow comparison of the incidence of stroke and trends among young adults across different countries.
Shift work, the circadian rhythm, and stroke in young adults
The circadian rhythm has a periodicity of 24 hours and involves daily cycles of behavior and physiology that are synchronized by non-photic and photic stimuli. 42 The rhythm regulates biological processes such as the cell cycle, sleep-wake cycle, energy homeostasis, hormone secretion, body temperature, and blood pressure. 43 Studies in young adults30,44 indicate that alterations in sleep architecture, quality, and rhythm that occur in obstructive sleep apnea increase the risk of stroke independent of the other factors. This is directly associated with shift work which is common in young adults.45,46 More than 15 million Americans fall within this middle-aged or young adult populations of 18-55 years. Most individuals in this population group do not work the typical 9-to-5 working hours and are referred to as shift workers. 47 Their rotating shifts make them susceptible to different health hazards that include cardiovascular problems, obesity, and stroke. The rotating shift work schedules also alter their internal body clocks such that they present with irregular sleep-wake patterns. 48 Irregularities in their timing of sleeping or waking deregulate the body clocks, making it difficult to maintain the normal 24-hour cycle. This shift work schedules can lead to severe ischemic strokes in the young adult working population. 49 Of interest to the current review is that there are sex differences among young adult men and women in the extent to which stroke was aggravated by the disruption of the circadian rhythm. 50 Precisely, the effect was worse in young men when compared with women. These differences might be associated with differences in sexual reproductive hormones. 50 For example, young men are more likely to suffer strokes when compared with women of the same age, and the stroke outcomes are likely to be more severe. 51 In women, estrogen is associated with more neuroprotection, as estrogen protects the brain in response to stroke. 52 However, older women when compared with older men of the same age present with an increased incidence of ischemic stroke and poor prognosis, especially when approaching menopause. Several attempts have been made to determine how modulation of the internal body clocks and inflammatory responses can affect cerebral blood supply.53-55 The circadian rhythm is chemically regulated, 56 and a disruption of its regulation may result in inflammatory responses which alter the circadian rhythm, and can lead to stroke or increased stroke severity. This area of research could identify the therapeutic targets that could be translated to reduce damage after a stroke in young shift workers. Also, this type of research focus will have clear implications for the young adult shift workers with odd schedules and could even be extended to older shift workers.
Melatonin and Stroke
In humans and other mammals, the tryptophan-derived neurohormone, melatonin, is secreted by the pineal gland to regulate the circadian rhythms as a part of its wide physiological functions. Although the nighttime increase in sleep propensity coincides with nighttime endogenous melatonin production, the duration of sleep has also been linked to the suprachiasmatic nucleus activity via the duration of nocturnal melatonin. 57 Other functions of melatonin include neuroprotection, 58 neurogenesis, and maintenance of oxidant/antioxidant balance. 18 Melatonin secretion undergoes 24-hour rhythmicity as shown by changes in its plasma and urinary levels, which depends on the time of the day, 57 and its production is reduced by light exposure and increased during the nighttime. Apart from the 24-hour variations in plasma and urinary melatonin levels, its secretion is also known to decrease with advancing age. 59
Melatonin is also found in extra-pineal tissues including astrocytes, glial cells, and retinal cells which are also capable of biosynthesizing indoleamines. 60 Moreover, extra-pineal melatonin synthesis has been reported in the brain. 56 In the central nervous system (CNS), melatonin is associated with the regulation of the circadian rhythm, modulation of the blood pressure, and promotion of sleep. 56 Melatonin’s roles in age-related neurodegenerative disorders have also been demonstrated by in vivo and in vitro studies. 61 However, no direct associations have been reported in young adults. A step-wise reduction in the circadian rhythm of salivary melatonin beginning around the age of 40 years has been reported, 62 with a prolonged duration of the melatonin peak levels and the lowest daytime levels also observed in young adults.62,63 These studies provide important clues on potential neuroprotective functions of melatonin. Table 2 summarizes some existing studies on melatonin in stroke therapy studies.
Melatonin in stroke therapy studies.

MCAO, middle cerebral artery occlusion; TFCI, transient focal cerebral ischemia; OGD, oxygen glucose deprivation.
The circadian rhythm of pineal melatonin in stroke patients has been investigated.17,65,78 Findings from these studies indicate that the melatonin rhythm is extensively preserved in cortical strokes. It then implies that in extensive cortical lesions, there could be a delay in melatonin secretion during the first post-stroke days, and this could subsequently revert to a normal pattern. 17 This is because melatonin synthesis is regulated by the ambient light/dark cycle, 77 and in extensive cortical ischemic stroke without notable edema, the melatonin surge may still be delayed. In this context, a change in the phase of the melatonin peak would suggest improper entrainment with the ambient light/dark cycle in the first post-stroke days. The mechanisms involved and the production rhythm of melatonin in stroke patients need further investigation.
It has been shown that chronic exogenous treatment with melatonin76,79 and pineal gland transplant in experimental models of stroke facilitate neuroprotection.67,80 In addition, melatonin receptor type 1A is involved in the neuroprotection of stem cells in in vivo models of stroke. 64 This ability is linked with melatonin’s direct free radical scavenging effect on neurons,20,64,73 as it directly protects neural tissue from free radical toxicity. 27 However, protection from free radical toxicity is not melatonin’s only tool against stroke, because melatonin renders the effect of harmful low-density lipoprotein (LDL) cholesterol and normalizes elevated blood pressure. 81 Animal studies27,75,82,83 have shown that melatonin improves the recovery of brain tissues affected by stroke. 66 Although melatonin’s roles are not yet fully defined when it comes to promoting rapid recovery post stroke, its role in increasing neuron plasticity has been proposed.69,84,85 This implies that melatonin not only helps prevent strokes, but it also induces cellular activities that reduce damage associated with strokes. In acute ischemic stroke, the common pathway of neuronal injury is also a target for anticoagulants or thrombolytics to dissolve blood clots. 86 However, many of the experimentally identified neuroprotective agents have failed in clinical trials. This is because many of the agents have a very narrow therapeutic window to induce protection during stroke. Thus, the urgency to develop novel neuroprotectants with a wide therapeutic window may give melatonin a chance as a novel neuroprotective agent in stroke. Because most of the existing studies do not provide clues about the general physiological effects of different doses of melatonin in the associated protection, future studies are necessary to address this issue. Moreover, improved protection of the brain after stroke may be better achieved when melatonin is combined with cellular molecules that regulate brain energy supply and demand to achieve homeostatic therapy in the treatment of stroke.
Melatonin and stroke in the young adult
A rising trend in the incidence of ischemic stroke in young adults has been reported, and this rise has been associated with certain identifiable risk factors. In a study of more than 1000 young stroke patients in Finland, dyslipidemia, smoking, and hypertension were the most common vascular risk factors. 24 However, the results of a more recent study in Estonia, Eastern Europe, revealed that the most frequently associated risk factors were hypertension, dyslipidemia, and smoking, in that order. 26 Existing studies indicate that a relatively constant set of modifiable risk factors play a large role in the pathogenesis of ischemic stroke in young adults. Moreover, these risk factors have been reported to be generally associated with ischemic or hemorrhagic stroke in the young adult.29,87 Also, they appear highly prevalent in young adult stroke patients and do not appear to be significantly affected by differences in geography, climate, or genetic diversity.
Oxidative stress is a major cause of neuronal damage in ischemic stroke, and melatonin may play a role in the antioxidant response. The decreased melatonin levels seen in acute ischemic stroke and in the experimental models indicate the potential therapeutic importance of this neurohormone. 88 Moreover, melatonin supplementation to restore the antioxidant capacity has been proposed for clinical assessment. 74 In the context of young or old stroke, there is growing evidence that connects oxidative stress and inflammation with an increase in age. This indicates that chronic treatment with melatonin is able to regulate oxidative stress and inflammation in aged brain reminiscent to a younger brain. 74 It then appears that melatonin may have a unique capability of regulating many mechanisms in the inflammatory cascades68,71 to initiate neuroprotection against ischemic insults. Indeed, existing studies have been able to advance the concept of melatonin’s neuroprotective capability that includes oxidative stress, differentiation, and secretion of specific growth factors in the brains of young stroke patients.20,65 Therefore, a potential hypothesis to test is how melatonin catabolism is linked with the overproduction of free radicals during acute ischemic stroke. From such a study, one can now envision a melatonin receptor metabolism technology in translational and clinical research. Because the levels of endogenous melatonin are associated with age, it is possible that dietary supplementation with melatonin may reverse the adverse effects in an aged cerebral ischemic brain. In this context, a melatonin supplementation to restore the antioxidant capability may deserve clinical assessment in young stroke. In support of this idea, melatonin treatment of aged mice regulated the gene expression profile of immune-related mRNAs in a pattern similar to younger animals. 89 The mechanisms involved require more investigation in future studies. Findings may reveal how melatonin regulates senescent brain into a response profile that resembles that of the younger brain, especially in regulating the immune system.
The possible protective roles and/or mechanisms of action of melatonin in ischemic stroke have also been examined extensively.72,90,91 In addition to its antioxidant properties, there are suggestions that melatonin is able to reduce or modulate the impact of the different levels of stroke pathophysiology, including Ca2+ dyshomeostasis, excitotoxicity, inflammation, and apoptosis. In separate studies, Borlongan et al 65 and Kilic et al 92 reported improved motor skills and a reduction in infarct size in a rat model of acute ischemia following pineal gland transplantation 65 and exogenous melatonin administration. 92 The possible mechanisms that are responsible for melatonin’s effects in acute ischemia include melatonin’s ability to maintain Ca2+ homeostasis by preventing acid-induced or glutamate-dependent alteration in Ca2+ levels.93,94 Melatonin also regulates the levels of extracellular glutamate by inhibiting glutamate release following ischemic injury. 95
In a young adult’s central nervous system, melatonin is well distributed in the brain and spinal fluid; however, levels decline progressively with an increase in age such that adults aged more than 80 years have only half the melatonin levels in their spinal fluid as young people. 80 This review supports the notion that melatonin secretion is generally adequate in the young adult population; hence, our central theme is that activities of endogenous melatonin could be enhanced to modulate some of the risk factors and prevent stroke in the young adult. If stroke occurs in the young adult brain, a melatonin-based therapy may also regulate the pathogenesis and its management. However, whereas melatonin secretion is generally believed to be adequate in the young adult population, significant individual variations in its secretion or activities are known to exist.96,97 The onset of step-wise reduction in melatonin rhythm has been reported to commence in the young adult age. 62 In general, melatonin appears to have a large role to play in the pathogenesis, and probably management of stroke in the younger age groups.
Management of Stroke in Young Adults and Potential Roles of Melatonin
Several concerns have been raised about the increasing rate of vascular risk factors in young adults and their roles in increasing the risk of ischemic stroke and its recurrence. To date, few research attempts have been made to address stroke problems in the young adult. Early diagnosis could be very challenging due the lack of awareness and the relative irregularity of stroke when compared with stroke mimics. Indeed, the causes of ischemic stroke in the young adult are diverse and can be comparatively uncommon, resulting in doubts about diagnostic assessment and raising concerns about specific management. There is no doubt that the incidence of ischemic stroke is rapidly increasing in the young adult population, whereas modalities for its management remain limited. Therefore, newer and better agents are constantly being investigated. Currently, the use of recombinant tissue plasminogen activator (r-tPA) is a Food and Drug Administration (FDA)-approved therapy for acute ischemic stroke. However, its use is not devoid of limitations, such as its narrow window of possible therapeutic benefit and eligibility of few patients for the therapy.70,98 The implication of this is that, to date, we are yet to develop anything close to an “ideal” drug for the management of ischemic stroke. As highlighted earlier, results of studies conducted with experimental animals may point in the direction of possible use of melatonin for stroke management in humans. There is a general belief that melatonin may be able to prevent more brain damage by protecting neurons occupying the ischemic penumbra, which is adjacent to the infarcted core. 72 A thorough review of stroke prevention with a general focus on specific causes and the general use of melatonin in stroke is outside the scope of this article. That said, the hope for the development of effective melatonin-based therapy for stroke has endured and in the last few years has been encouraged by the neuroprotective functions of melatonin for reducing the brain’s intrinsic susceptibility to ischemic insults. Thus, the ability to protect the brain from free radicals and its possible prophylactic effects may give melatonin a chance as a homeostatic therapy in the treatment of stroke. Also, the individual benefits derivable from melatonin may be cumulative in reducing the risk of developing stroke in young adults.
Conclusion
Although melatonin has been found to be beneficial in several animal models of stroke, its possible benefits in humans with stroke are still being investigated. In young adult stroke patients, little is known about the clinical benefits of melatonin use, despite its link to some of the associated risk factors. Melatonin’s antiapoptotic, antioxidative, and neuroprotective effects might make it uniquely applicable in this context. However, although there is a dearth of human studies evaluating the safety of melatonin in stroke, cautious application will allow an understanding of the interactions between exogenous melatonin and its endogenous rhythm, and how these interactions may affect outcomes in young adult stroke patients. Also, the different mechanisms that may be responsible for melatonin’s neuroprotection in humans will be better understood, and the influence of age on them will be better studied. Therefore, as the world experiences changes in the demographics of stroke, attention should be paid to design and conduct of clinical trials that explore the safety and potential applications of melatonin in young stroke patients.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed equally to the writing of this manuscript.