
Abstract
Background:
This study aimed to assess the importance of selected kynurenines measured in peritoneal fluid, lavage washings, and blood serum in patients with advanced gastric cancer (GC) based on the clinical and pathological staging of TNM for a more precise evaluation of the stage of the disease.
Methods:
Data were collected from a prospectively maintained database of all patients operated on advanced GC between July 2018 and August 2020. In total, 98 patients were eligible for the analysis according to the REMARK guidelines.
Results:
Among the various kynurenines analyzed in this study, we found that the median concentration of anthranilic acid (AA) in the peritoneal lavage washings was significantly higher in patients with positive nodes (pN1-3) compared to those with negative nodes (pN0) (P = 0.0100). Based on the ROC analysis, AA showed diagnostic utility in the differentiation of the pN staging (P = 0.0047). Furthermore, there was a positive correlation between AA in peritoneal fluid with stage pN (P = 0.0116) and a positive correlation between AA in peritoneal lavage washings with stage cT (P = 0.0101). We found that the median concentration of kynurenine (Kyn) in peritoneal lavage washings was significantly higher in patients with cM1 compared to cM0 patients (P = 0.0047). Based on the ROC analysis, Kyn showed diagnostic utility in cM staging differentiation (P < 0.0001). There was a positive correlation between peritoneal Kyn and stage of cM (P = 0.0079).
Conclusions:
AA and Kyn measured in peritoneal lavage indicate advanced GC and may be considered in the future as valuable adjunct tools in TNM staging of advanced GC.
Introduction
With more than 1 million new cases estimated annually, gastric cancer (GC) remains one of the most common malignancies diagnosed worldwide. Furthermore, GC mortality is the fourth most common cause of cancer-related deaths, 1 mainly due to the advanced stage at diagnosis. 2
Gastrectomy with adequate lymphadenectomy and perioperative or adjuvant chemotherapy remains the main treatment for advanced GC. 3 Except lymph node (LN) dissection (the only surgery-dependent prognostic factor in GC), there is no other clinically useful method to increase the effectiveness of surgical treatment, and most local failures are believed to be sustained by insufficient nodal clearance. 4 Furthermore, an accurate evaluation of LN involvement can allow the selection of patients who could benefit from an extended nodal dissection. 5 Explorative laparoscopy to detect peritoneal metastases is recommended for patients with GC at stage 1B or higher for whom surgical resection is planned. 6 Patients with positive cytology on peritoneal lavage have high rates of disease recurrence after surgery, although the conversion to negative cytology after chemotherapy could be associated with better survival outcomes. 7 There is a need for other, that is, molecular indicators of disease progression, that could improve the assessment of cancer status and allow for more appropriate decision during surgery.
The degradation of tryptophan (Trp) through the kynurenine pathway (KP) has been recognized as an important process involved in immune tolerance within tumor microenvironment. 8 It produces several metabolites (kynurenines) including kynurenine (Kyn), 3-hydroxykynurenine (3HKyn), 3-hydroxyanthranilic acid (3-HAA), quinolinic acid (QA), kynurenic acid (Kyna), anthranilic acid (AA) and finally produces nicotinamide adenine dinucleotide (NAD+)—a vital cofactor of several enzymes. 9 In the tumor microenvironment, the enzymes tryptophan-2,3-dioxygenase (TDO) and indoleamine-2,3-dioxygenase 1 (IDO1) are primarily responsible for KP activation and have been associated with anti-tumor immune suppression. 10 TDO and IDO1 initiate Trp degradation to Kyn, the first stable metabolite of KP, which has been shown to inhibit T-cell proliferation and induce T-cell apoptosis.11,12 Furthermore, Kyn has been identified as an endogenous ligand of the human aryl hydrocarbon receptor (AHR), the crucial factor in the regulation of the immune response regulation and cancer progression. 13 Kyn can be further metabolized by Kynureninase A (KynA) to AA, the concentration of which increases in neurological and other disorders. Moreover, the potential therapeutic ability of AA derivatives as anti-inflammatory and anticancer agents is currently the subject of increasing number of investigations.9,14-18
In 90% of human gastric carcinomas, there is IDO1 overexpression that promotes immune escape and tumor invasion.19,20 High expression of IDO1 (leading to the delivery of sufficient amounts of NAD+ for DNA repair) predicted poor postoperative outcome of patients with GC 21 and resistance to therapy independently of immune suppression. 22 The contribution of KP to other gastrointestinal tumors has also been demonstrated. 23 Kyn was reported to be a prognostic factor in some cancers, such as peripheral T-cell lymphoma 24 or hepatocellular carcinoma 25 showing a potential for kynurenines to become cancer biomarkers. The concentration of different kynurenines in patient serum, plasma, and gastric juice is considered a biomarker for GC diagnosis.26-28 The relationship between systemic and local Kyn concentration remains to be described in detail, however, our preliminary studies showed differences in Trp and some KP metabolites concentrations between blood and peritoneal fluid obtained from GC patients. 29 Importantly, locally generated KP metabolites impact the tissue microenvironment and contribute to the immune escape of the tumor creating an inflammatory environment. 30 In gastric cancer, IDO1 has also been shown to promote metastasis involving KP-metabolites-mediated changes in the composition of the extracellular matrix, especially upregulation of collagen 12A1. 31 To our knowledge, the predictive role of KP metabolites in advanced GC staging, particularly in the peritoneal setting, has not been evaluated.
Our study aimed to evaluate the significance of selected kynurenines measured in peritoneal fluid, peritoneal lavage washings, and blood serum in advanced GC patients based on clinical and pathological TNM staging. To take advantage of the samples routinely collected during diagnostic laparoscopy, peritoneal fluid or lavage washings were used as the material to determine the kynurenines generated locally by tumor cells.
Materials and Methods
Study design
The study was carried out according to the Declaration of Helsinki guidelines and was approved by the Institutional Review Board of the Bioethical Committee of the Medical University of Lublin (Ethic Code: KE–0254/182/2018). Informed consent was obtained from all participants. Data were collected from a prospectively maintained database of all patients operated on advanced gastric adenocarcinoma between July 2018 and August 2020 in the Department of Surgical Oncology of the Medical University of Lublin, Poland. Inclusion criteria focused on cM0 GC patients scheduled for staging laparoscopy or curative gastrectomy, according to abdominal and pelvic computed tomography (CT) diagnostic imaging. Exclusion criteria included lack of intraoperative peritoneal lavage washings or collection of peritoneal fluid. Diagnosis included cytology performed on the peritoneal fluid according to the routine diagnostic procedure. In total, 98 patients were eligible for analysis.
Assessment of Trp and kynurenines in body fluids
Trp and KP metabolites were evaluated in peritoneal fluid (ascitic) and blood serum collected from operated patients. In the absence of ascitic fluid, peritoneal lavage was collected at the beginning of the staging of laparoscopy or gastrectomy. On the contrary, in the presence of ascitic fluid, peritoneal lavage washings were not obtained. During peritoneal lavage washings, the abdominal cavity was washed with 50 mL of physiological saline solution and gently stirred, followed by aspiration of the washings from the tumor area. The material obtained was then divided into 2 equal samples. The first sample was sent to pathology for centrifugation, followed by Papanicolau staining of the sediment to identify cancer cells. The second sample was intended for quantitative analysis of Trp and its metabolites including Kyn, 3-HKyn, AA, 3-HAA, Kyna, XA, and QA. Serum samples were obtained from blood collected at the beginning of the surgical procedure. Before analysis, serum was pretreated with a 15% (w/v) aqueous solution of trichloroacetic acid (TCA) for protein removal and peritoneal fluid (395 µL) or lavage washings (790 µL) were subjected to solid phase extraction (SPE) according to the protocol described earlier. 29
The determination of Trp and kynurenines was performed with an Ultra-High Performance Liquid Chromatography-Electrospray Ionization-Tandem Mass Spectrometry system (UHPLC-ESI-MS/MS, Agilent Technologies) as described earlier. 29 Quantitative analysis was based on matrix-matched calibration using the MassHunter Quantitative Analysis software v.B.07 (Agilent Technologies). Standard calibration solutions were prepared in BSA (for blood serum) or peritoneal fluid pretreated with activated charcoal. Matrix-matched standards were prepared similar to experimental samples and contained a fixed amount of 3-nitrotyrosine (3NT, an internal standard) and various concentrations of analytes. The electrospray ionization source was operated in positive ion mode (ESI+), and ion acquisition was performed in the dynamic multiple reaction monitoring (DMRM) mode. Other measurement conditions were detailed in Sadok et al. 29
Statistical analyses
Data were analyzed using Statistica software version 13 PL. We retrospectively assessed the size of the sample. Due to the post hoc retrospective method, only statistically significant results according to the purpose of the study were considered in the calculation based on the primary endpoint as the correlation between continuous variables (pN and AA concentration). To reject the null hypothesis, an error of type I (alpha) of 0.05 was used. In the case of type II (beta) error, the beta cut-off value was established at 20% to achieve 80% power. Taking into account the correlation set as primary endpoint (rho = 0.365), it was calculated that the minimum number of samples that provide credible confirmation of the test hypothesis should be at least 56. As the data had non-normal distribution (assessed using the Shapiro-Wilk test), the correlations were assessed using the nonparametric Spearman’s rank correlation test, and comparisons were made using the U-Mann-Whitney (2 groups) Kruskal-Wallis ANOVA test (multiple) and p < 0.05 was considered statistically significant. The diagnostic usefulness of the investigated markers was assessed using ROC curve analysis.
Results
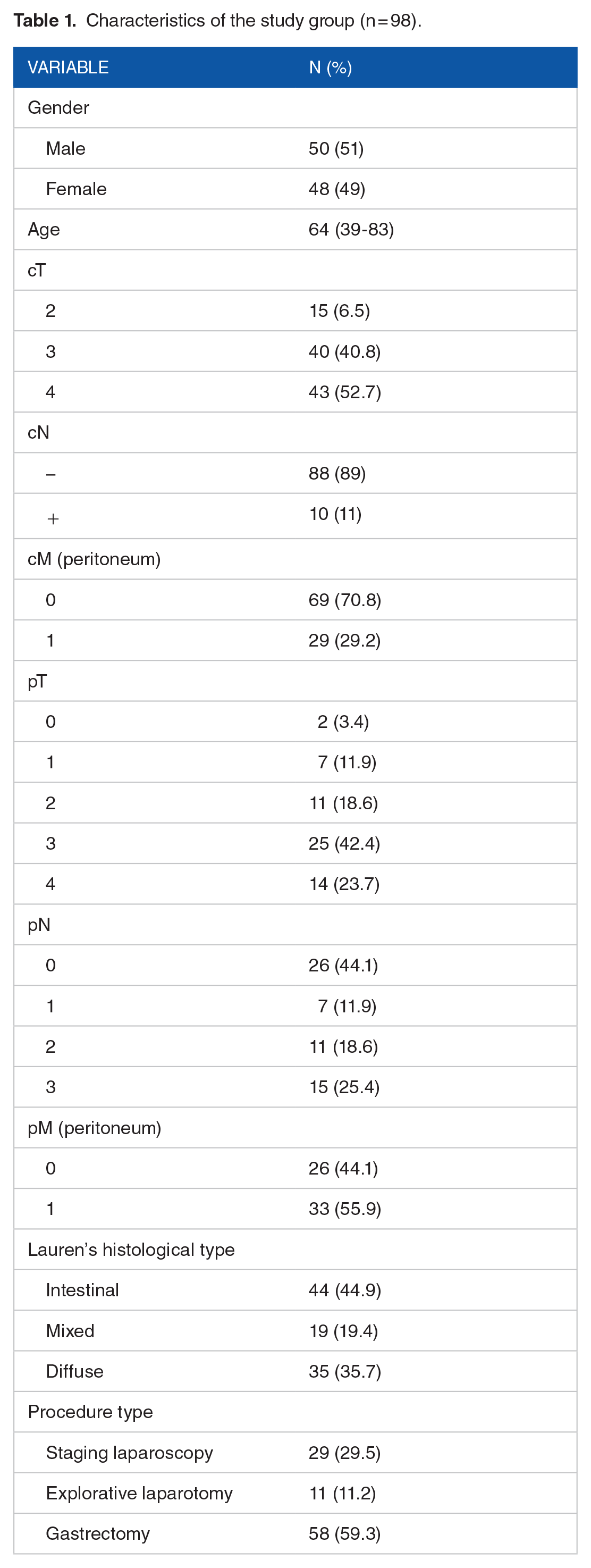
Characteristics of the study group are summarized in Table 1. Using the UHPLC-ESI-MS/MS approach, peritoneal fluid samples (Table 2), peritoneal lavage washing (Table 3) were tested to determine a panel of 7 KP metabolites (3-HKyn, Kyn, XA, Kyna, QA, 3-HAA, AA) and Trp. In the blood, all metabolites except 3-HAA and AA were evaluated (Table 4) due to the method restrictions, as we described earlier. 29 Among the different KP metabolites present in the peritoneal fluid or peritoneal lavage washings analyzed in this study, AA and Kyn were identified as the most significant biomarkers determining the selected clinical and pathological staging parameters of TNM (Figure 1), while changes in other kynurenines were not significant.
Characteristics of the study group (n = 98).
Spearman rank correlation between kynurenine pathway metabolites and selected clinicopathological variables in advanced GC patients assessed in peritoneal fluid.

bold indicates changes for the most significant biomarkers.
Spearman rank correlation between kynurenine pathway metabolites and selected clinicopathological variables in advanced GC patients assessed in peritoneal lavage washings.
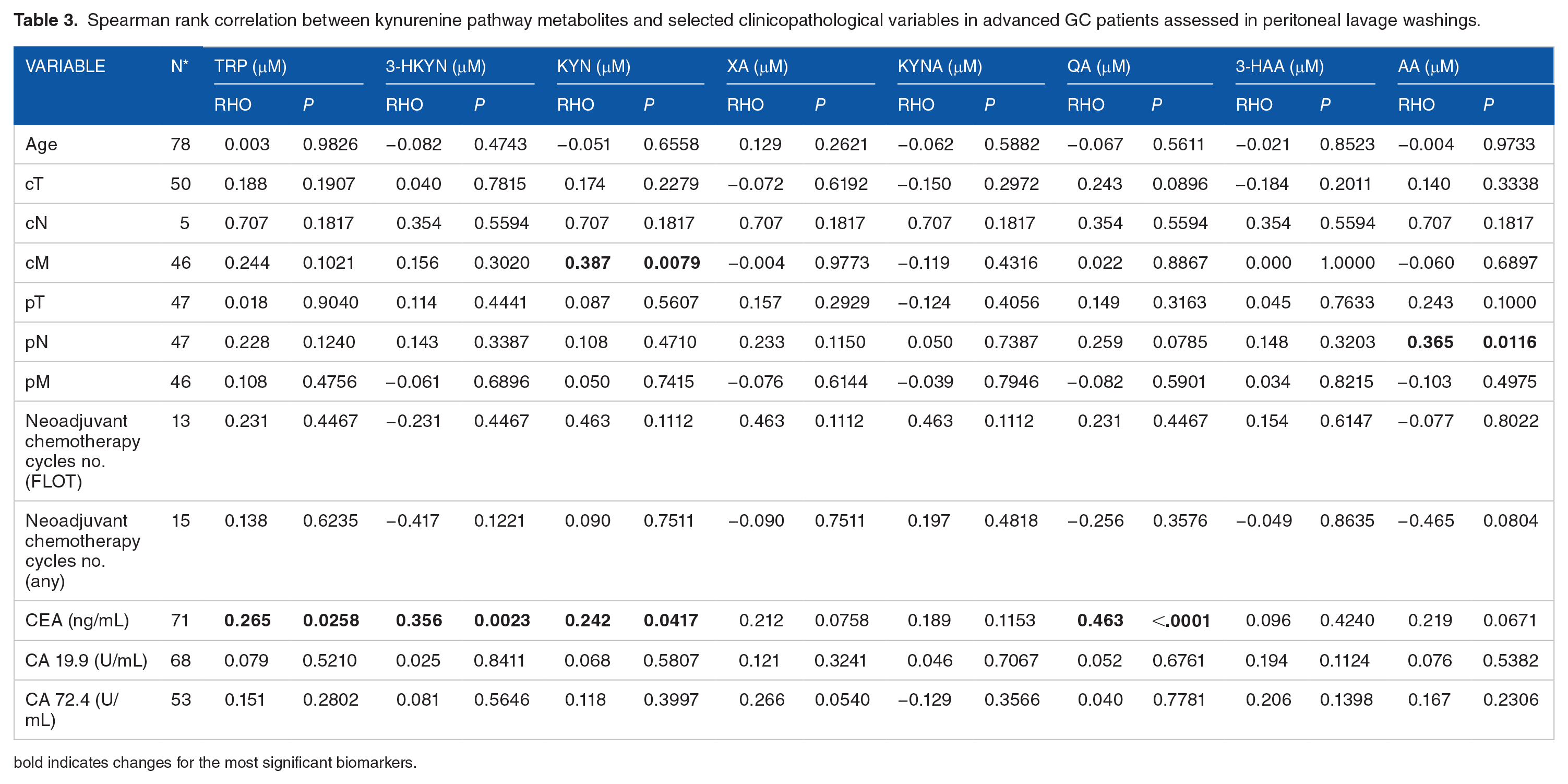
bold indicates changes for the most significant biomarkers.
Spearman rank correlation between kynurenine pathway metabolites and selected clinicopathological variables in advanced GC patients assessed in serum blood.

bold indicates changes for the most significant biomarkers.

Diagnostic utility of KP metabolites assessed in peritoneal fluid. Box-whisker plots presenting peritoneal kynurenines according to the TNM staging (A and D). ROC curves showing diagnostic utility of selected kynurenines in differentiation of TNM stages (B and E). Scatterplots representing Spearman’s correlation between selected kynurenines and TNM stages (C and F).
The median concentration of AA in the peritoneal lavage washings was significantly higher in patients with positive nodes (pN1-3) compared to patients with negative nodes (pN0) (0.05 vs 0.03 µM; P = 0.0100; Figure 1A, Table 3). Based on the ROC analysis, AA showed diagnostic utility (cut-off: >0.049 µM; sensitivity: 58.3%, specificity: 85.5%) in the differentiation of the pN stage (pN0 vs pN1-3; AUC = 0.72, 95%CI 0.57-0.84; P = 0.0047; Figure 1B). Furthermore, there was a positive correlation between AA in peritoneal fluid with stage pN stage (rho = 0.365, P = 0.0116; Figure 1C) and a positive correlation between AA in peritoneal lavage with stage cT stage (rho = 0.734; P = 0.0101). The median concentration of AA in peritoneal fluid was significantly higher in patients with positive cytology compared to patients with negative cytology (0.5 vs 0.3 µM; P = 0.0431). Based on the ROC analysis, AA showed diagnostic utility (cut-off: >0.033 µM; sensitivity: 81.8%, specificity: 75%) in positive and negative cytology differentiation (AUC = 0.78, 95%CI: 0.54-0.94; P = 0.0178). Furthermore, there was a positive correlation between the median concentration of AA in peritoneal fluid and cytology (rho = 0.480, P = 0.0346).
Assessment of Kyn
We found that the median Kyn concentration in peritoneal lavage washings was significantly higher in cM1 patients compared to cM0 patients (0.20 vs 0.05 µM; P = 0.0047; Figure 1D, Table 3). Based on ROC analysis, Kyn showed diagnostic utility (cut-off: >0.117 µM; sensitivity: 87.5%, specificity: 69.9%) in differentiation of the cM staging (pM0 vs pM1; AUC = 0.79, 95%CI: 0.65-0.90; P < 0.0001; Figure 1E). There was a positive correlation between Kyn and the stage of cM (peritoneum) stage (rho = 0.387; P = 0.0079; Figure 1F). Furthermore, we have identified a positive correlation of Kyn with cT (rho = 0.353; P = 0.0053) and a negative correlation of 3-HKyn and XA with cM (rho = −0.345; P = 0.0086 and rho = −0.261; P = 0.0498, respectively) in the blood serum of the operated patients (Table 4). There was no significant association of Trp or other evaluated metabolites (Kyna, QA, and 3-HAA) with clinical variables, regardless of the material studied (peritoneal fluid—Table 2, peritoneal lavage washings—Table 3 or serum—Table 4).
Discussion
Our study focused on advanced gastric cancer and the utility of peritoneal material in disease staging. To our knowledge, this is the first report on the association between selected KP metabolites and peritoneal lavage from patients with advanced GC. The correlation between AA and positive cytology suggests that KP metabolites may serve as useful biomarkers during GC staging.
Recent discoveries in the field of genetics, surgery, and targeted therapies have not yet modified the well-established treatment protocol for GC patients. 32 Although a worldwide consensus has been established on the extent of lymphadenectomy has been established,6,33,34 a patient-tailored treatment is being pursued 35 in order to minimize unnecessary interventions and their side effects. Recently developed surgical techniques (fluorescence-guided surgery) can assist the surgeon in making decisions about extended lymphadenectomy. 36 However, due to histological heterogeneity, tumor behavior throughout the clinical management of GC remains uncertain, thus novel diagnostic opportunities are highly desired for appropriate disease staging. Meanwhile, some studies in the field of metabolomics have been conducted to identify new potential biomarkers for early diagnosis of GC.37-41 Based on the available literature, KP metabolites seem to be promising biomarkers in advanced GC patients.26-29
The results of this study indicate an association between some KP metabolites and the clinical and pathological stage of advanced GC. The most important finding of our analysis was that AA concentrations in peritoneal lavage were correlated with pathological nodal staging (Figure 1A-C). Thus, AA should be considered a potential adjunct tool for tailoring lymphadenectomy in surgical treatment of GC. Furthermore, in agreement with previous results showing that IDO1 and KP metabolites mediate changes in extracellular matrix composition and upregulation of collagen 12A1 to promote metastasis, 21 we found that an increase in Kyn amount was indicative of metastatic peritoneal spread (Figure 1D-F). The results are summarized in Figure 2 and suggest enhanced KP activity toward AA in advanced disease. These novel findings imply a potential future use of these markers in clinical practice. Although the role of metastasectomy in addition to gastrectomy for stage IV GC has not been evaluated in a prospective randomized setting, conversion treatment is frequently proposed followed by restaging imaging and staging laparoscopy. In selected patients with oligometastatic GC, surgical resection is then advocated. 42 Presumably, selected kynurenines could serve as a predictive factor during the re-staging process. Since Kynureninase A (KynA) in addition to IDO activity could be responsible for the increase in AA generation in these patients, it remains to be explained whether these enzymes play a role in the progression of GC.

Kynurenine pathway activity assessed by quantification of kynurenines in peritoneal lavage washings (A), peritoneal fluid (B), and blood serum (C) obtained from patients with GC. All KP metabolites assessed in this study are in bold. The blue arrows show a positive or negative correlation of the boxed kynurenines (AA, Kyn) with TNM staging factors.
Interestingly, there was also a positive correlation of Kyn measured in blood serum with cT (Figure 2C). If confirmed in a prospective setting, it could suggest the potential utility of serum blood as analytical material for clinical GC staging, rather than peritoneal fluid. At the same time, we found a negative correlation of 3-HKyn and XA with cM that needs to be further studied to understand whether KP activity is directed toward AA production, as we found in peritoneal fluid. Such scenario is likely, in the case of less active kynurenine monooxygenase, KMO (less efficient generation of 3-HKyn and XA), in favor of KynA producing AA.
As reported by Choi et al, 28 the local concentration of KP metabolites (gastric juice) was a magnitude higher than that measured in blood. In the same report, the level of some metabolites in the blood was correlated with the level in the gastric juice, however, a decrease in Kyn was observed in the blood of cancer patients, while in the gastric juice it was increased, suggesting that systematically generated Trp metabolites (by hepatic TDO) might not reflect a local status of kynurenines. Recently, we have reported differences in the accumulation of Trp and KP metabolites among the blood serum and peritoneal fluid of patients with GC. We observed that the concentrations of Kyn, 3-HKyn, and QA appeared to be higher in peritoneal fluid than in blood serum, while XA and Kyna were more abundant in serum. 29 In this paper, AA was not quantified in blood serum due to the sample preparation approach that made it impossible. 29 In the future, the determination of AA in blood serum should be performed in parallel with the peritoneal lavage analysis to assess the correlation between the KP level in the blood and the local tumor microenvironment of GC.
We also acknowledge the fact that level of Trp metabolites might be influenced by the microbiome status, in particular H. pylori infection (known GC risk factor). Therefore, such infection should be considered in the patient’s inclusion criteria. However, it should be noted, that in our study during the qualification for the surgery, the active infections were not found in our patients.
The evaluation of kynurenines in peritoneal fluid and lavage washings presented here sets the stage for the potential application of this approach in advanced GC diagnostics, that is, staging. Reported for the first time, the positive correlation between the AA concentration of peritoneal lavage and the stage of pN will be confirmed in future studies conducted on a greater number of samples that will make the cohort and analyzed subgroups more homogeneous. In addition, the clinical value of the AA concentration in blood serum will also be studied for the GC staging.
Conclusions
The concentration of some KP metabolites in peritoneal lavage washings presents future valuable adjunct tools in the nodal (N) and distant (M, peritoneal) staging of advanced GC. Since a positive correlation was found between AA and peritoneal fluid cytology, further studies on KP metabolites in advanced GC are warranted.
Footnotes
Acknowledgements
The authors thank Ilona Jonik from the Centre for Interdisciplinary Research of the JPII Catholic University of Lublin for her assistance with sample collection and preparation.
Authors Contributions
Conceptualization, K.R.P., W.P.P., and M.S., methodology, K.RP., I.S., R.M., W.P.P., and M.S.; software, R.M.; formal analysis, I.S.; resources, M.S., W.P.P.; data curation, K.G., K.R.P., I.S.; writing—original draft preparation, K.RP., I.S., R.M., W.P.P., M.S.; writing—review and editing, K.RP., I.S., R.M., W.P.P., M.S.; supervision, W.P.P., M.S.; funding acquisition, M.S. All authors have read and agree to the published version of the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has received funding from the European Union from the European Regional Development Fund under the Eastern Poland Operational Program Development 2007-2013 (agreement POPW.01.03.00-06-003/09-00). The study was supported by the Polish National Science Center, OPUS13 grant (2017/25/B/NZ4/01198 for Magdalena Staniszewska, Principle Investigator), Interdisciplinary Grant from JPII Catholic University of Lublin, nr 15/2019 for Magdalena Staniszewska, Principal Investigator, and internal grant from JPII Catholic University of Lublin for Ilona Sadok, Principal Investigator.
Institutional Review Board Statement
The study was carried out according to the Declaration of Helsinki guidelines and was approved by the Bioethical Committee of the Medical University of Lublin (Ethic Code: KE–0254/182/2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.