
Abstract
Background:
Childhood eating behaviors arise from the interaction of socio-demographic, emotional, and environmental influences that shape food-related responses early in life. Guided by a behavioral–ecological perspective, this study explored key determinants of emotional, physical-activity-related, and social-interaction-based eating behaviors among school-aged children in Bangladesh.
Methods:
A cross-sectional study was conducted among 420 school-going children (aged 4-12 years) across urban, semi-urban, and rural areas in Bangladesh. Data were collected through structured interviews with guardians. Statistical analyses were performed using Stata 17. Descriptive statistics summarized participant characteristics, while Chi-square tests and multivariate logistic regression estimated adjusted odds ratios (AOR) with 95% confidence intervals.
Results:
Behavioral changes were most frequent in the emotional domain (90.5%), followed by physical activity-related (88.1%) and social interaction-related behaviors (86.2%). Parental education and urban residence were consistent predictors of greater behavioral variation. Higher household income was associated with lower odds of physical-activity-related changes (AOR = 0.09, P < .05), while religion was linked to social eating differences (AOR = 0.32, P < .05).
Conclusion:
Parental education, residence, income, and religion significantly shape children’s eating behaviors. These findings highlight the importance of integrating emotional and environmental perspectives in designing child nutrition programs, particularly for low-income and less-educated families.
Introduction
Dietary habits established during childhood play a crucial role in shaping health outcomes throughout an individual’s life.1,2 Poor dietary choices in early life can lead to a range of chronic diseases in the future, which include obesity, type 2 diabetes, and cardiovascular conditions.3 -5 According to the World Health Organization (WHO), nearly 39 million children under 5 years of age were overweight or obese, while over 45 million suffered from wasting, reflecting the double burden of malnutrition globally. 6 The global rise in childhood obesity and malnutrition is particularly alarming, with significant health implications that may extend into adulthood. 7
Recent studies have highlighted a concerning shift toward increased consumption of processed and fast foods among children worldwide. 8 Global market data show that sales of packaged snack foods and sugary beverages have risen by over 40% in LMICs since 2010, driven by rapid urbanization and aggressive food marketing. 9 This trend is facilitated by urbanization and economic changes that transform food landscapes, making unhealthy options more accessible and appealing. 10 In South Asia, for instance, over 60% of school-aged children reportedly consume fried or processed snacks at least 3 times per week, replacing traditional, home-cooked meals with convenience foods. 11 Despite the growing body of evidence on the adverse effects of such dietary patterns, there is a significant gap in specific knowledge about the dynamics of these patterns among school-going children, particularly in developing countries like Bangladesh. 12
Beyond nutritional and environmental determinants, eating behavior is also a psychosocial and emotional process. Children’s food choices are shaped by cognitive factors (attitudes, perceived norms, self-control) and emotional regulation mechanisms that govern responses to stress, reward, and social cues. 13 According to the Theory of Planned Behavior, dietary actions stem from intentions influenced by beliefs, family and peer expectations, and perceived control over available foods. 14 Prior research has shown that emotional and restrictive eating patterns often emerge as coping responses to mood fluctuations or environmental pressure. Prior research demonstrated that emotional eating and body mass index jointly predict maladaptive eating among university students, providing a multidimensional model that integrates emotional, environmental, and cognitive domains. 15 Although their sample involved adults, similar psychological mechanisms, such as emotional reactivity and social modeling, are likely to shape children’s eating patterns in family and school environments. Building upon this conceptual precedent, the current study explores how emotional, physical-activity-related, and social-interaction-related dimensions manifest in the eating behaviors of Bangladeshi children.
Furthermore, while numerous interventions have been implemented globally to promote healthy eating among children, there remains a substantial need for targeted research that addresses the localized factors influencing dietary habits. Studies have shown that the effectiveness of nutritional interventions can vary greatly depending on cultural, economic, and environmental contexts.16 -18 This variation points to the necessity of understanding the specific drivers of dietary behaviors in different settings to inform more effective public health strategies.
In Bangladesh, rapid socioeconomic transformations have notably impacted the nutritional landscape, making the study of children’s dietary habits both timely and critical.19 -21 The Bangladesh Demographic and Health Survey (BDHS 2022) reported that 13.6% of school-aged children are overweight or obese, while micronutrient deficiencies persist among nearly one-third of this age group.22 -24 However, existing research often lacks a comprehensive focus on the nuanced factors that specifically affect children’s eating behaviors in the Bangladeshi context. Moreover, the majority of existing studies do not adequately address how these behaviors are influenced by broader socio-demographic factors such as parental education, household income, and urban versus rural settings. Equally, the emotional and behavioral mechanisms underlying these patterns remain under-explored in the local literature. Given this backdrop, the current study aims to fill these critical gaps by systematically investigating the socio-demographic determinants that influence the eating behaviors of school-going children aged 4 to 12 in Bangladesh. The research will particularly focus on identifying the key factors that shape children’s dietary patterns and nutritional status without delving into the direct impacts of specific dietary components. By doing so, it seeks to provide a robust framework for understanding the complex interplay of influences that guide children’s dietary habits.
The novelty of this study lies in its approach to combining a comprehensive socio-demographic analysis with the specific dietary outcomes of children in an evolving economic landscape. This approach is expected to yield insights that can directly inform the development of targeted nutritional interventions and policies tailored to the unique socio-economic and cultural fabric of Bangladesh. Ultimately, the findings from this research are anticipated to contribute significantly to the global discourse on child nutrition and public health, offering actionable data that can guide interventions to improve child health outcomes both locally and globally. By addressing these research gaps and focusing on these aims, the study not only adds to the academic literature but also serves a practical purpose in shaping public health initiatives designed to foster healthier eating behaviors among children. This dual contribution highlights the study’s potential to impact significantly on public health practices and policies, particularly in settings similar to Bangladesh.
Methodology
Study Design and Population
This cross-sectional study utilized a quantitative data collection approach, focusing on school-going children aged 4 to 12 years, including those in kindergarten. Since the children were too young to provide the data themselves, their guardians were interviewed to gather information about the children’s eating behaviors. The data collection was carried out in various schools across Bangladesh, covering urban, semi-urban, and rural regions. These areas were selected using standard area codes to ensure representation of different socio-economic contexts. Including schools from diverse geographical locations helps capture a wide range of experiences and behaviors within the study population, providing a comprehensive view of the factors influencing children’s eating habits.
Study Period and Inclusion/Exclusion Criteria
The study was conducted over a 6-month period, from June 2023 to November 2023. Inclusion criteria for the study required that participants be school-going children aged 4 to 12 years, including those enrolled in kindergarten, with their guardians present to provide the necessary information during the interview process. Guardians needed to be available and willing to participate in the data collection process to ensure the accuracy of the responses. Exclusion criteria involved children whose guardians were not present or unwilling to participate in the study, as well as incomplete data entries that would compromise the validity of the analysis.
Sampling Technique and Sample Size
Convenience sampling was utilized in this study due to practical considerations, allowing for the collection of data from various schools across Bangladesh. This method was chosen due to time and resource constraints, allowing for efficient data collection. Schools were selected based on accessibility and cooperation from school authorities, making it practical to gather data within the study’s timeframe. While this method may limit the generalizability of the findings, it provided a practical solution for capturing a diverse sample and overcoming logistical challenges associated with school schedules and the availability of guardians during data collection. The sample size was determined using the standard formula [Z2*P*(1 − P)/d2] for cross-sectional studies, which calculates the required number of participants based on the estimated prevalence of eating habit changes among school-going children. With a Z-value of 1.96 for a 95% confidence interval, an assumed prevalence of 50% to maximize variability, and a margin of error set at 5%, the estimated sample size was calculated to be 384 participants. To accommodate potential non-responses and incomplete data, the initial target was set at 450 participants. After applying the necessary inclusion and exclusion criteria, and accounting for missing values, the final sample size for analysis was 420 participants.
Variable of Interest
The variables of interest in this study focused on children’s eating behaviors and how emotions, physical activity, and social interactions shaped these behaviors. Guardians were asked whether their child’s eating behavior had increased, decreased, or remained unchanged in relation to these dimensions. Responses of “increased” or “decreased” were categorized as “Yes,” indicating a change, while “unchanged” was classified as “No.” The emotional dimension explored how shifts in mood or emotional states affected eating habits, while physical activity referred to whether changes in the child’s level of physical exertion influenced their eating patterns. Social interaction considered whether involvement with peers or other social engagements led to noticeable changes in the child’s eating behavior. This approach ensured that each variable was assessed independently, providing a clear understanding of the various influences on children’s eating habits.
Independent Variable
The independent variables in this study were categorized as follows: the age of the child was divided into 3 groups, Early Learners (4-5 years), Lower Primary (6-9 years), and Upper Primary (10-12 years) corresponding to key developmental stages in both cognitive and social skills. Early Learners were at the foundational stage of social and cognitive development, Lower Primary children focused on building basic academic skills, while Upper Primary students began grasping more advanced concepts, a crucial time for developing eating habits. The area of residence was categorized as rural, semi-urban, and urban, based on standard area codes used in Bangladesh. Religion was classified into Islam and Hinduism, reflecting the composition of the study sample.
The educational status of both parents was assessed separately, and categorized into no education, primary, secondary, and higher education for both the father and mother. Household income was divided into 4 categories: low income (<20 000 BDT), lower-middle-income (20 000-50 000 BDT), upper-middle income (50 001-100 000 BDT), and high income (>100 000 BDT), representing the total household income of the family. The type of house was classified as either owned or rented.
Parental eating habits were evaluated by asking whether both the father’s and mother’s eating behaviors influenced their child’s eating habits, with responses recoded into binary outcomes (Yes/No). Additional factors included the child’s personality type, categorized as extrovert, introvert, or mixed, and peer influence, determined by whether the child experienced peer pressure regarding food choices (Yes/No).
Media influence, particularly television habits, was also considered. The type of TV program was categorized into “Don’t watch TV,” “Entertainment,” “Advertisement,” and “Others,” while changes in the child’s eating behavior based on TV-watching habits were also recorded in Yes/No format.
Data Collection
Data collection was conducted using a structured questionnaire administered to the guardians of the children. The questionnaire was developed with input from 2 field experts to ensure clarity and relevance. A pilot study involving 20 participants was conducted to test and refine the questionnaire, leading to final adjustments to improve its suitability for gathering accurate information. Once finalized, data collection began across selected schools. The process was closely monitored to maintain the quality and consistency of responses. Collected data were carefully recorded, securely stored, and managed in a digital format to ensure data integrity and confidentiality throughout the research process.
Data Analysis
Stata 17 software was used for data analysis. The demographic characteristics of the study participants were presented using frequencies and percentages. The Chi-square test was applied to assess the association between independent variables and the dependent variables, which were changes in children’s eating behaviors based on emotion, physical activity, and social interaction. Results of the Chi-square tests were presented with both x² values and p-values, accompanied by ψ symbols to indicate the strength of the associations, with an increasing number of ψ symbols signifying a stronger relationship. After Chi-square tests, any independent variable showing a P-value of less than .2 with any of the dependent variables, was retained for inclusion in the multivariate logistic regression models. This ensured that no potential influencing factors were excluded, as it allowed the retention of variables showing any association with the dependent variables, preventing the risk of overlooking important associations. Multicollinearity among the independent variables was assessed using a correlation matrix with a threshold of .8. As no multicollinearity was identified, all variables could be included in the regression models. Logistic regression models were then employed to assess the factors influencing changes in each of the eating habits. The results were presented with adjusted odds ratios (AOR) and corresponding 95% confidence intervals, and the strength of the AORs was indicated using star (*) symbols, where more stars denoted stronger associations. Hosmer-Lemeshow goodness-of-fit tests with the group cut point set to (10), were conducted for each model, with P-values greater than .05 confirming the model’s fit.25,26 The findings were summarized and visualized through tables and graphs to provide a clear understanding of the results.
Results
The study included 420 guardians of school-going children aged 4 to 12 years, who provided data on behalf of the children. Figure 1 shows the prevalence of changes in children’s eating behaviors, with emotional dimension being the most prevalent, observed in (90.5%) of children, followed by physical activity-related changes at (88.1%), and social interaction-related changes at (86.2%).
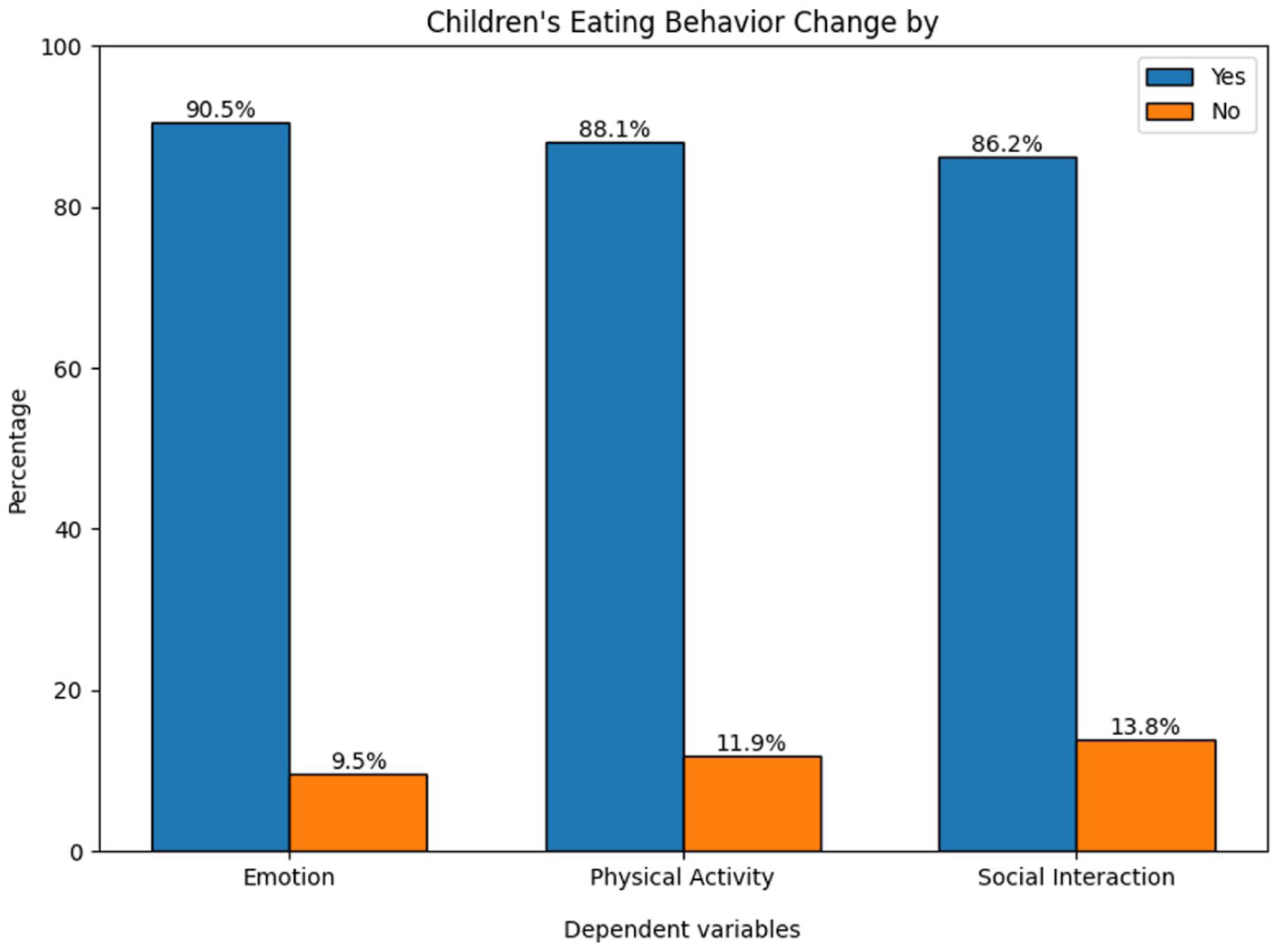
Prevalence of changes in children’s eating behaviors by emotional, physical, and social factors.
Table 1 shows the demographic profile, showing that most children were in the Lower Primary group (75.2%) and lived in urban areas (74.3%), with Islam as the dominant religion (90%). A large proportion of fathers (84.5%) and mothers (70.7%) had higher education, and 38.6% of families belonged to upper-middle-income households. Over half (55.7%) lived in rented homes, indicating socio-economic diversity. Moreover, Table 2 shows that during tiffin time, fast food (19.3%) and roadside food (12.4%) were the most commonly consumed items among children.
Socio-demographic Characteristics of School-Going Children in Bangladesh (n = 420).

Distribution of Food Types Commonly Consumed During School Tiffin Among Children.

In Table 3, the analysis revealed several significant associations between independent variables and changes in children’s eating habits. Father’s education showed the most consistent and highly significant associations across all 3 dimensions: emotional (χ² = 32.59, P = .000), physical activity (χ² = 23.63, P = .000), and social interaction-based eating habits (χ² = 33.54, P = .000). Similarly, the mother’s education was highly significant for emotional (χ² = 29.88, P = .000), physical activity (χ² = 32.33, P = .000), and social interaction-based eating habits (χ² = 15.41, P = .001).
Bivariate Association Between Selected Socio-Demographic Characteristics and Domains of Eating Behavior.

Chi² significance: ΨP < 0.05, ΨΨP < 0.01, ΨΨΨP < 0.001.
The residence also played a significant role, particularly for emotional (χ² = 11.04, P = .004) and social interaction-based eating habits (χ² = 12.63, P = .002). Other significant associations included the Child age group, which was associated with emotional eating habits (χ² = 6.58, P = .037), and TV program categories, which were significant for emotional eating habits (χ² = 8.50, P = .037). Additionally, religion showed a notable association with social interaction-based eating habits (χ² = 6.01, P = .014), while personality type was linked to physical activity-based eating habits (χ² = 6.44, P = .040).
After identifying suitable variables for analysis through bivariate tests, significant associations were further explored using multivariate logistic regression models. Table 4 shows that residence emerged as a significant factor. Children living in rural areas had notably lower odds of experiencing emotional eating changes (AOR = 0.19, 95% CI: 0.06-0.67, P < .01), physical activity-related eating changes (AOR = 0.34, 95% CI: 0.12-0.99, P < .05), and social interaction-based eating changes (AOR = 0.19, 95% CI: 0.08-0.50, P < .001) compared to urban counterparts. Similarly, children from semi-urban areas exhibited significantly lower odds of emotional eating changes (AOR = 0.20, 95% CI: 0.08-0.54, P < .001).
Multivariate Analysis of Factors Influencing Children’s Eating Behavior Domains.
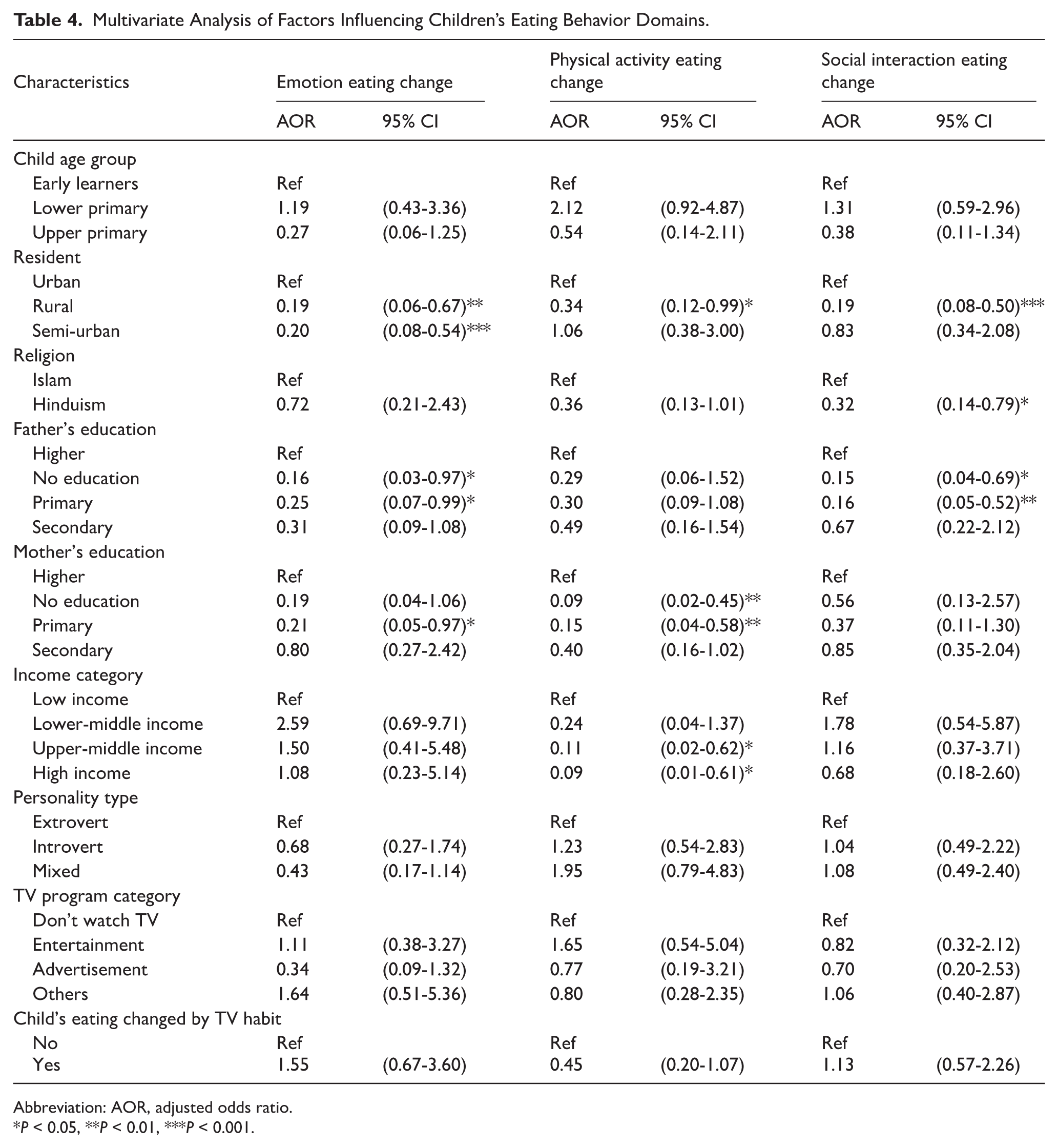
Abbreviation: AOR, adjusted odds ratio.
*P < 0.05, **P < 0.01, ***P < 0.001.
Parental education, particularly both the father’s and mother’s education, plays a critical role in shaping children’s eating behaviors. Fathers with no education had children who were significantly less likely to exhibit changes in emotional eating habits (AOR = 0.16, 95% CI: 0.03-0.97, P < .05) and social interaction-based eating habits (AOR = 0.15, 95% CI: 0.04-0.69, P < .05), compared to those with higher education. Similarly, fathers with only primary education had children who were less likely to display changes in emotional eating (AOR = 0.25, 95% CI: 0.07-0.99, P < .05) and social interaction-based eating habits (AOR = 0.16, 95% CI: 0.05-0.52, P < .01). Mothers’ education level mirrored the following pattern, as children of mothers with no education were less likely to experience changes in physical activity-related eating behaviors (AOR = 0.09, 95% CI: 0.02-0.45, P < .01), and those with primary-educated mothers followed a similar trend for physical activity-based eating habits (AOR = 0.15, 95% CI: 0.04-0.58, P < .01).
Religion was another notable determinant, with children from Hindu families significantly less likely to experience social interaction-based eating changes compared to their Muslim counterparts (AOR = 0.32, 95% CI: 0.14-0.79, P < .05). Additionally, household income showed a significant influence on physical activity-related eating habits. Children from upper-middle-income families were less likely to exhibit changes in eating habits related to physical activity (AOR = 0.11, 95% CI: 0.02-0.62, P < .05), with a similar association observed in high-income families (AOR = 0.09, 95% CI: 0.01-0.61, P < .05) when compared to those from low-income households.
Discussion
This study identifies several distinct patterns that influence children’s eating behaviors, focusing on emotional, physical activity-related, and social interaction-related changes. Among these, emotional eating changes were the most prevalent, followed by those linked to physical activity and social interaction. This pattern indicates correlation rather than causation, suggesting that children’s emotional regulation and coping responses strongly interact with environmental and familial contexts. The prominence of emotional eating habits suggests that children’s emotions play a critical role in shaping their food choices and eating patterns.
A key pattern identified is the influence of parental education, especially fathers’ education, on children’s eating habits. The findings indicate that children of parents with higher education levels both fathers and mothers are more likely to experience changes in their eating habits across all 3 dimensions: emotional, physical, and social. This is likely because educated parents are more aware of healthy eating practices and place a higher value on the emotional and social aspects of their children’s development. 27 Parents with more education may also have better access to resources, such as nutrition information and healthier food options, which enables them to make more informed choices about their children’s diets. Moreover, parental education may indirectly affect children’s eating patterns through emotional modeling and family meal dynamics, where emotionally responsive parents model regulated eating behaviors. Studies have shown that emotional and binge-eating patterns are linked to emotion-based coping styles, reinforcing how family-level emotional climate can shape children’s food attitudes and responses.15,28 Additionally, these parents may be more attuned to their children’s emotional well-being, fostering environments that encourage healthier eating habits. 29
The study also found a significant association between where children live and their eating behaviors. Children living in urban areas were more likely to experience changes in their eating habits across all 3 dimensions compared to children living in rural areas. Urban environments often expose children to more processed and convenience foods, which are readily available and frequently advertised. 30 At the same time, urban children may have fewer opportunities for physical activity due to limited outdoor spaces, contributing to changes in their eating habits.31,32 On the other hand, children in rural areas may have more access to home-cooked meals, fewer fast-food options, and greater opportunities for outdoor physical activities, which may explain their lower likelihood of emotional, physical, and social eating changes. 33
Income level further contributed to the variation in children’s eating habits, with children from higher-income families being less likely to exhibit physical activity-related changes in their eating behaviors. Wealthier families typically have greater access to recreational activities, sports facilities, and healthier food choices, contributing to more stable eating patterns.34,35 In contrast, families with lower incomes may prioritize convenience and affordability, leading to greater consumption of processed and fast foods, which can disrupt regular eating behaviors. Lower-income families also experience higher psychosocial stress, which has been associated with emotional and compensatory eating as a coping mechanism, as reflected in several behavioral nutrition studies. 36 This finding aligns with previous research that suggests a strong correlation between socioeconomic status and dietary habits, where higher income levels often correlate with healthier, more consistent eating practices. 37
Religion was also found to influence children’s social interaction-related eating habits, with Hindu children being less likely to experience changes in this area compared to Muslim children. This difference may be due to variations in religious practices, cultural traditions, and communal meals that influence social eating behaviors. For instance, religious festivities, dietary restrictions, and communal gatherings may play a significant role in shaping how children from different religious backgrounds approach food and social interaction.38,39 Such socio-cultural structures foster shared mealtime rituals that reinforce behavioral norms and emotional stability around eating, acting as a protective factor against irregular or stress-driven eating. These findings highlight the importance of considering cultural and religious contexts when studying eating behaviors, as these factors can greatly influence how food is consumed and shared in social interaction.
The study’s findings highlight the need to address key factors that influence children’s eating behaviors when designing interventions. Specifically, urban families with lower educational attainment or income levels may face greater challenges in maintaining healthy eating patterns for their children. These families are more likely to encounter processed foods and sedentary lifestyles, making their children more susceptible to unhealthy eating habits.40,41 Therefore, policies should focus on supporting these vulnerable groups through targeted initiatives.
Public health programs should prioritize promoting healthy eating habits by providing nutritional education and emotional well-being support for parents, particularly those with lower levels of education. By engaging parents and caregivers, these programs can help create environments that encourage healthier food choices and foster positive eating behaviors in children. Integrating emotional literacy, family-based meal interventions, and culturally sensitive approaches could make these programs more sustainable and contextually effective.
Limitation & Strength
This study has several limitations that should be acknowledged. The use of convenience sampling may have affected the representativeness of the findings, as participation depended on school and parental consent, possibly excluding children from less privileged or non-school-attending backgrounds. Reliance on parental or guardian reports to assess children’s eating behaviors may have introduced recall or social desirability bias, with respondents potentially underreporting unhealthy habits or overstating positive behaviors. The cross-sectional design also limits causal inference, and unmeasured factors such as parental dietary practices, food insecurity, and exposure to food marketing may have influenced the observed associations. In addition, the study did not employ standardized or validated instruments to measure emotional or behavioral constructs, which may affect measurement reliability. This limitation arose because no culturally adapted and age-appropriate validated tools were available for Bangladeshi children within the studied age range. Instead, the questionnaire was developed from previous literature and refined through expert consultation and pilot testing to ensure content relevance and clarity within the local context. Self-reported data are further subject to potential cultural and interpretation biases, and several contextual influences, such as school food policies, family meal routines, and children’s screen time, were not controlled for, which could have shaped eating behaviors in meaningful ways.
Despite these limitations, the study offers several important strengths. It draws on a large and diverse sample of school-going children from urban, semi-urban, and rural settings, allowing for a comprehensive understanding of dietary behaviors across different socio-economic contexts. The inclusion of emotional, physical activity-related, and social interaction-related aspects of eating behavior provides a multidimensional perspective that is rarely explored in Bangladeshi research. The use of multivariate logistic regression enhances the robustness of the findings by accounting for confounding variables. Overall, this study contributes valuable evidence to guide local, informed, school and family-based nutrition interventions aimed at promoting healthier eating behaviors among children in Bangladesh.
Conclusion
This study shows that emotional factors have the strongest influence on children’s eating behaviors, followed by those related to physical activity and social interaction. Parental education, particularly fathers’ education, plays an important role, with higher education levels associated with healthier eating patterns. Urban residence was linked to greater variation in eating habits, while higher household income was associated with more stable behaviors. Religion also appeared to influence social interaction-related eating habits, reflecting cultural differences.
These findings indicate that children’s eating behaviors are shaped by both socio-demographic and emotional factors. Patterns of emotional eating may begin developing in early life, underscoring the need for supportive family and school environments that promote emotional well-being and healthy eating practices.
Footnotes
Acknowledgements
We would like to express our gratitude to all the parents for their participation. Without their support, it would have been difficult to get the data.
Ethical Considerations
This study was conducted in accordance with institutional and international ethical standards, ensuring participant well-being, confidentiality, and informed consent. Ethical approval was obtained from the North South University Institutional Review Board (IRB No. 2025/OR-NSU/IRB/0330). Provisional approval was granted before data collection to allow supervised initiation, and final approval was received before data analysis. All procedures adhered to the principles of beneficence, non-maleficence, and transparency, and no ethical deviations or violations occurred during the study.
Author Contributions
MD Nahid Hassan Nishan, Asif Hossain: Conceptualization. MD Nahid Hassan Nishan: Data curation. MD Nahid Hassan Nishan: Formal analysis. MD Nahid Hassan Nishan, Ahsan Uddin, Asif Hossain, Sharmin Jahan: Methodology. All Authors: Writing- original draft. All Authors: Writing- review & editing. Saidur Rahman Mashreky: Critical review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.