
Abstract
Background:
Recent studies reported that omega-3 fatty acids may improve renal function in patients with chronic kidney disease (CKD). The aim of the present study was to assess the effect of omega-3 supplements on renal function indices in patients with CKD undergoing hemodialysis.
Methods:
This randomized controlled clinical trial was carried out on 120 CKD patients who were undergoing hemodialysis treatment in Rasht, Iran. The intervention group (n = 60) received 3 capsules of 1000 mg omega-3 fatty acid supplement capsules daily for 2 months. The control group (n = 60) received 3 placebo capsules containing 1000 mg of MCT. Renal function indicators included blood urea nitrogen (BUN), creatinine (Cr), sodium (Na), potassium (K), calcium (Ca), and phosphorus (P) were measured at baseline and after the intervention.
Results:
Omega-3 supplementation significantly improved BUN (68.26 ± 2.97 to 56.59 ± 2.14, P = .03) and Cr levels (8.94 ± 0.29 to 7.58 ± 0.41, P < .01) after adjustment for age, gender, body mass index (BMI), smoking, diet, and underlying diseases including diabetes and hypertension. However, no significant effect was found on serum levels of Na, K, Ca, and P.
Conclusion:
According to the present study, giving omega-3 supplementation to patients with CKD undergoing HD may enhanced their renal function. Additional research is required to verify these results.
Introduction
The rising prevalence of chronic kidney disease (CKD) worldwide increases the risk of death from specific cardiovascular diseases like heart failure, coronary artery disease, and stroke. This increased risk is driven by multiple factors such as increased oxidative stress, inflammatory factors, hypertension, dyslipidemia, anemia, and vascular calcification. 1 The mortality risk is particularly pronounced among hemodialysis patients with renal disease. 2 CKD impacts more than 10% of the worldwide population, encompassing about 800 million individuals. Globally, chronic kidney disease (CKD) is becoming more common; by 2040, it is expected to rank as the sixth most common chronic ailment. 3 A systematic review and meta-analysis including 70 605 individuals in Iran discovered an overall prevalence of CKD at 15.14%, with a higher prevalence among females compared to males. 4 Furthermore, approximately 4 million individuals worldwide are receiving kidney replacement treatment (KRT), with hemodialysis (HD) accounting for roughly 69% of all KRT and 89% of all dialysis cases. HD is becoming the most common modality used in KRT. 5
Chronic kidney disease (CKD) is frequently caused by diabetes, glomerulonephritis, hereditary vulnerability, and chemical toxicity. 6 Moreover, CKD is impacted by both macronutrients and micronutrients. Protein and energy should be customized for those with CKD to maintain muscle mass and prevent malnutrition. As the European Best Practice Guidelines, individuals receiving maintenance hemodialysis who are younger than 60 years should have dietary intake targets that do not exceed 35 kcal/kg/day for protein and no more than 30 kcal/kg/day for energy. 7 In addition, vitamins and minerals are essential micronutrients for the management of CKD. It has been demonstrated that hemodialysis patients who get adequate micronutrients have a lower risk of CVD. In a cohort study with a 12-year follow-up, dietary micronutrients such as magnesium, vitamin C, and vitamin E were associated with a decreased risk of CKD.7-9
Omega-3 fatty acids are an essential part of a balanced diet and considered a potential option for the managing the CKD complications due to their ability to modify several risk factors including the atherogenic risk profile and the levels of oxidative stress, inflammation, and arterial hypertension. 10 Numerous critical biological processes including the creation of eicosanoid, the function of cell membranes, the signaling of metabolic pathways, and the expression of different genes are influenced by omega-3 fatty acids. 11 Several studies demonstrated that people with CKD have substantially reduced blood levels of omega-3 fatty acids compared to the general population, possibly due to decreased food intake, inflammation, nutritional malabsorption, and metabolic abnormalities. 12 Additionally, individuals undergoing hemodialysis may have elevated oxidative stress, which could impact the bioavailability and decrease the levels of omega-3 fatty acids. 13 Thus, supplementation of omega-3 may be promising due to its anti-oxidative and anti-inflammatory properties. 14
On the other hand, one study reported that omega-3 fatty acids supplementation had no advantage in patients undergoing hemodialysis. 15 Despite a rise in scientific interest over the past few decades regarding the potential benefits of supplementing with these fatty acids in hemodialysis patients, omega-3 fatty acid supplementation is not commonly used in patients with CKD. This could be because there is a lack of information regarding its potential therapeutic benefits. While some of these studies have demonstrated that hemodialysis patients’ levels of inflammatory indices are decreased when they take an oral omega-3 fatty acid supplement, 16 other researchers have not observed any discernible impacts of omega-3 fatty acids. 17 So, the aim of this study was to establish the impacts of oral omega-3 fatty acid supplementation on kidney function in patients with CKD undergoing hemodialysis.
Materials and Methods
Study Design and Participants
We conducted a randomized controlled trial on 120 patients with CKD undergoing hemodialysis at a private center in Rasht, Iran. Sample size was calculated using OpenEpi software (alpha .05, beta .2, and power 0.8) to detect a change of 2 mg/dl in blood urea nitrogen (BUN) between groups. We used random block randomization via https://www.randomizer.org. the patients, researcher, and statistician were blinded to the group. Inclusion criteria were written consent, age 20 to 85 years, and above-standard KT/V for dialysis days. Exclusion criteria included concurrent research participation, psychiatric disorders, specific medical conditions including inflammatory diseases, active infections, and malignancies, recent immunosuppressive drugs/chemotherapy/warfarin, regular NSAIDs/corticosteroids, incomplete medical records in primary outcomes, non-compliance, peritoneal dialysis history, prolonged clotting times, recent surgery, fish allergy, pregnancy, and death.
Data Collection
Demographic, socioeconomic, and medical information were collected from patient records. Additional collected data included disease history, dialysis frequency, medication use, serum markers, blood pressure, blood sugar, and urine output. Height was measured using a stadiometer, and weight/body composition was assessed using a bio-impedance analyzer (OMRON-BF511). The records of dialysis department were used to evaluate the intake of dietary supplements. Missing data in the secondary outcomes were completed using the multiple imputation method. Dietary intake was assessed using a 24-hour dietary recall questionnaire and both groups were assessed for dietary omega-3 intake. To enhance data accuracy, participants were provided with detailed instructions and examples of food portions.
Intervention
Patients in the intervention group received 3 daily 1000 mg omega-3 capsules (180 mg EPA/DHA; Zahravi Co., Tabriz, Iran) for 2 months. The control group received 3 daily 1000 mg MCT oil placebo capsules (Zahravi Co., Tabriz, Iran). To ensure adherence to the study protocol, several measures were implemented. To ensure adherence, supplements were dispensed weekly in 21-capsule packs and monitored by phone calls. Medication compliance for the intervention group was assessed through weekly pill counts and patient self-reports. Participants were contacted by phone each week to verify supplement consumption and address any concerns. Research staff underwent standardized training on data collection procedures to minimize inter-rater variability. Regular data audits were conducted to identify and correct any inconsistencies. To maximize participant retention, study visits were scheduled at convenient times for participants, and regular contact was maintained through phone calls and reminders.
Biochemical Analysis
Pre- and post-intervention blood samples (10 cc) were collected from all participants. Serum was separated and analyzed for kidney function markers (eg, BUN, creatinine) at Razi Hospital laboratory, Rasht, Iran.
Data Analysis
Descriptive statistics (mean ± SD for quantitative data, percentages/counts for qualitative data) were used to describe demographic, social, and anthropometric characteristics. The Kolmogorov-Smirnov test assessed normality of the data. Baseline comparisons between groups were performed using t-test (normally distributed quantitative data) or chi-squared test (categorical data). The general linear model (GLM) repeated measure test was used to evaluate the effect of omega-3 supplementation on renal function markers in the intervention group, adjusting for the potential confounders including age, gender, BMI, smoking, diet, diabetes, and hypertension. P < .05 was considered statistically significant. Data analysis was performed using SPSS version 21.
Results
A total of 120 patients were initially examined, and 112 patients were finally assessed as the intervention group included 58 participants and the placebo group included 54 participants. The demographic and baseline characteristics of the participants are presented in Table 1. 18 No significant difference was found between the groups regarding age, weight, height, amount of sleep, Hemoglobin (Hb), hematocrit (HCT), platelet (PLT), gender, marriage, diabetes, hypertension, heart disease, tobacco use, and alcohol use.
The General Characteristics of the Participants. 18
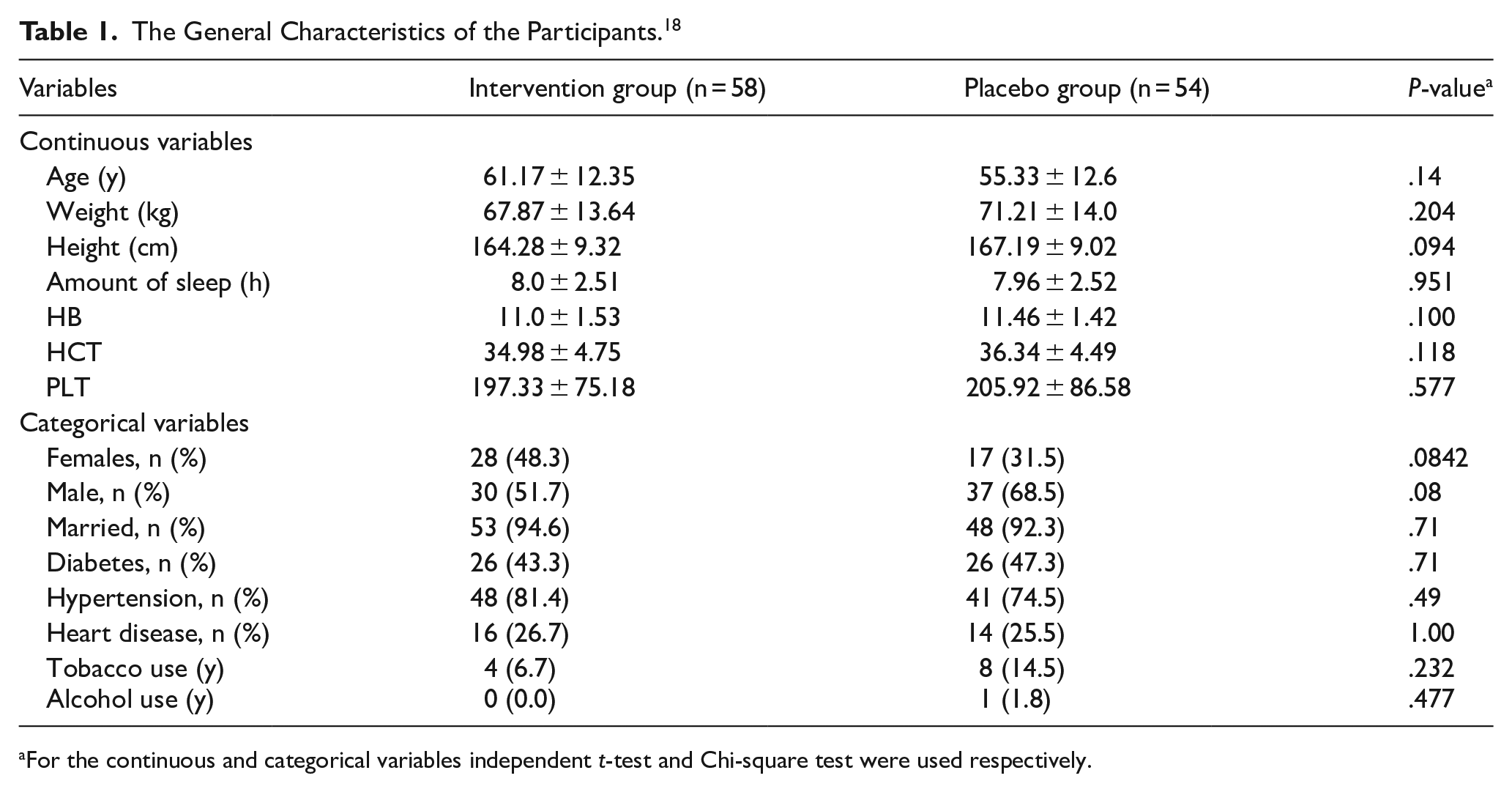
For the continuous and categorical variables independent t-test and Chi-square test were used respectively.
According to the Table 2, omega-3 supplementation significantly improved BUN (68.26 ± 2.97-56.59 ± 2.14 mg/dl) and Cr (8.94 ± 0.29-7.58 ± 0.41 mg/dl) levels (P < .05), but had no effect on serum levels of Na, K, Ca, and P (All P > .05).
Comparison of Indicators of Kidney Function Among the Intervention Group and Control Group.

Abbreviations: BUN, blood urea nitrogen; Cr, creatinine; Na, sodium; K, potassium; Ca, calcium; P, phosphorus.
Repeated measure ANOVA.
Discussion
The results of this randomized controlled clinical research indicated that BUN and Cr levels were dramatically improved by omsega-3 supplementation in patients with CKD. In line with the present study, the beneficial effects of omega-3 supplements were reported in some other studies. According to a previous study, after taking an omega-3 PUFA supplement, hemodialysis patients experienced improvements in their cardiovascular parameters, dry skin conditions, inflammation, and pruritus symptoms. 19 In another study, it was observed that individuals with higher levels of n-3 PUFA intake derived from seafood had a decreased risk of developing CKD. 20 A randomized controlled experiment found that increased consumption of seafood n-3 PUFAs was found to successfully lower blood pressure, which is a significant factor in the development of CKD. 21 In an experimental study, chronic renal failure was induced by nephrectomy in mice. After being supplemented with EPA and DHA for a period of 12 weeks, there was a noticeable decrease in tubulointerstitial injury due to reductions in fibrosis, inflammation, and oxidative stress. 22 Furthermore, 3 randomized controlled trials have demonstrated a notable enhancement in pruritus symptoms among CKD patients who received omega-3 supplementation, in contrast to those who received omega-6, omega-9, or placebo supplementation.23-25 Although a small uncontrolled pilot study did not find any positive impact of omega-3 supplements on alleviating symptoms of uremic pruritus. 26
In previous studies, several mechanisms were explained regarding the effects of omega-3 fatty acids on kidney function in patients with CKD. First, the EPA inhibited the activation of NF-kB, leading to the suppression of tumor necrosis factor-a (TNF-a) expression in human monocytic THP-1 cells. 27 A recent umbrella review found that TNF-α levels were reduced following omega-3 polyunsaturated fatty acids supplementation. 28 Also, another recent study found that n-3 PUFAs inhibit NF-κB/COX-2 induced production of pro-inflammatory cytokines. 29 Second, n-3 PUFAs may attenuate fibroblast activation and kidney fibrosis, which may be associated with the inhibition of mTORC2 signaling. 30 Third, research have shown that consuming omega-3 polyunsaturated fatty acids prolong bleeding duration and decreases platelet adhesiveness. In particular, it has been shown that docosahexaenoic acid (DHA) but not eicosapentaenoic acid (EPA) markedly reduced collagen aggregation in people with type 2 diabetes, indicating that DHA may have better antithrombotic qualities than EPA.31,32 Fourth, omega-3 polyunsaturated fatty acids have the potential to influence blood pressure by promoting enhanced vascular compliance and vasodilation. 33 Moreover, the results of a meta-analysis indicated that omega-3 supplementation significantly reduced serum TG and LDL level in dialysis patients 34 which may have a role in improving the kidney function and health outcomes in patents with CKD. 35
In the present study, we assessed the effect of omega-3 fatty acids on kidney function of patients with CKD under hemodialysis through a randomized controlled trial (RCT). RCT is a robust design for investigating the effects of omega-3 supplementation. The use of random block randomization and the blinding of patients, researchers, and statisticians added credibility to the study and reduced the potential bias. However, we had some limitations. First, although the present study boasts a relatively large sample size (120 patients), it would benefit from a larger cohort and longer follow-up period to evaluate the long-term effects of omega-3 supplementation on renal function. Second, the positive results observed in renal function markers (BUN, Cr) are promising, but the lack of significant change in Na, K, Ca, and P levels may suggest that omega-3 supplementation has a limited effect on electrolyte balance. Third, the study also does not address the potential interactions between omega-3 and standard CKD treatments, such as phosphate binders or antihypertensive medications. Third, serum omega-3 levels were not measured in this study. Using a more objective measure such as serum omega-3 fatty acid levels, instead of pill counts and phone follow-ups, would have provided better insight into adherence. Further studies should investigate the long-term effects of omega-3 supplementation, particularly in combination with other dietary or pharmacological interventions in patients with CKD in different stages. Additionally, future trials should aim to include more diverse patient populations and explore the role of omega-3 in reducing cardiovascular events, which are common in CKD patients (Figure 1).
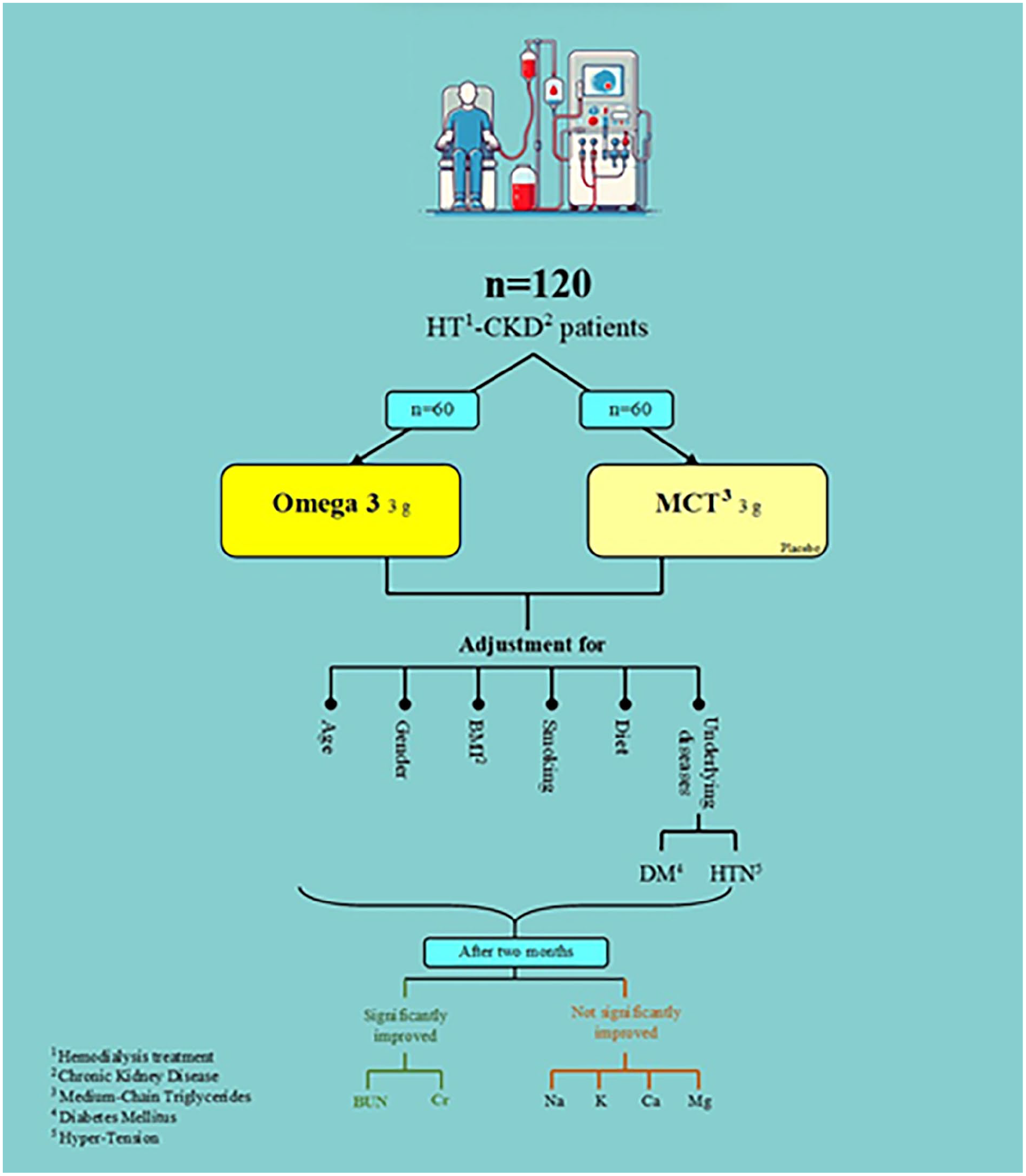
The association between: omega-3 and renal function.
Conclusion
The results of the present study indicated that omega-3 supplementation significantly improved BUN and Cr levels in hemodialysis patients compared to the placebo group. These findings are in line with previous studies suggesting beneficial effects of omega-3 on kidney proper function. The observed improvements may have potential implications for overall kidney health, patient outcomes, and the quality of life, even if dialysis continues. While this study provides promising results, it plays a role as a trigger point and further research is warranted to elucidate the underlying mechanisms of action and to assess the long-term effects of omega-3 supplementation on kidney disease progression. Additionally, larger-scale studies with longer follow-up periods are needed to confirm the findings and evaluate the potential clinical benefits of omega-3 supplementation in a broader patient population considering individual variability in response to omega-3, particularly concerning coexisting conditions like diabetes or hypertension. Also, beyond renal function markers, future studies should also consider the effects of omega-3 fatty acids on clinical outcomes such as cardiovascular events, hospitalizations, and quality of life, which are highly relevant for CKD patients.
Footnotes
Acknowledgements
We thank all the participants in this study for their good cooperation. This paper was taken from the approved research project of Gilan University of Medical Sciences, Rasht, Iran. Also, we would like to thank Zahravi Pharmaceutical Company for their nice cooperation.
Authors’ Note
Mahsa Shapouri is now affiliated to Department of Clinical Nutrition, School of Nutrition and Food Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Pouya Mirzaee is now affiliated to Department of Medicine, Faculty of Medicine, Semnan University of Medical Sciences, Semnan, Iran.
Majid Kamali is now affiliated to School of Nutrition and Food Sciences, Isfahan University of Medical Sciences, Isfahan, Iran.
Zahra Mahmoudi is now affiliated to Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran.
Saeid Doaei is also affiliated with Reproductive Health Research Center, Department of Obstetrics and Gynecology, School of Medicine, Al-Zahra Hospital, Guilan University of Medical Sciences, Rasht, Iran.
Ethical Considerations
This study was approved by the ethical committee of the cancer research center, Gilan University of Medical Sciences, Rash, Iran (Code: IR.GUMS.REC.1401.307) in accordance with the Declaration of Helsinki.
Consent to Participate
All experimental protocols were approved by a Gilan University of Medical Sciences, Rash, Iran and informed consent was obtained from all participants.
Consent for Publication
The authors declare that they have no competing interests.
Authors’ Contributions
SD, MZ, MSH, PM, MK, ZM, NN, ZS, SBA, KHAM, and MGH designed the study, and were involved in the data collection, analysis, and drafting of the manuscript.ZA, ASHG, HSH, BA, MKH and SD were involved in the design of the study, analysis of the data, and critically reviewed the manuscript. All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Gilan University of Medical Sciences, Rash, Iran (Code: 3954).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Name of the registry: National Nutrition and Food Technology Research Institute
Trial registration number: IRCT20151226025699N6
Date of registration: 2022-12-24