
Abstract
Background:
Low hemoglobin level is the most common public health problem during pregnancy in developing countries including Ethiopia, which is affecting both mother and fetus. However, the determinants of anemia among pregnant women are not well studied.
Objective:
To assess the determinates of hemoglobin among pregnant women in rural agro-pastoralist communities in the South Omo zone, Ethiopia
Method:
Community-based cross-sectional study was done in rural agro-pastoralist communities. A multistage stratified sampling technique was used to select 526 pregnant women. Data were collected by using structured questionnaires. Hemoglobin level was measured by using HemoCue ® Hb301. Data were analyzed by using a statistical package for the social science version 26. Descriptive (Mean, standard deviation, frequency, range), bivariate and multivariate analysis was carried out to check the association between lower hemoglobin levels and independent variables. The output is presented in tables and figures.
Result:
The mean (±SD) of hemoglobin concentration was 11.8 ± 1.7. The overall prevalence of anemia was 39.9% [95% CI: 35.5, 44.4], 19.4% (95% CI: 16.0, 23.2) was mild, 19.6% (95% CI: 16.27, 2.5) was moderate and 0.9% (95% CI: 0.25, 2.25) was severe anemia. Not taking IFA (AOR = 5.7(3.3, 9.8)), severe under nutrition (AOR = 8.9(2.1, 37.3)), no fish food (AOR = 2.4(1.3, 4.5)), drinking coffee (AOR = 1.6(1.0, 2.6)), moderate food insecurity (AOR = 2.5(1.4, 4.6)), and no malaria infection (AOR = 0.6(0.4, 0.9)) were statistically significant with anemia.
Conclusion:
The anaemia is a public health problem in this study area. Therefore, nutrition education and counselling to enhance iron supplementation, dietary diversity and a flesh diets are very essential to enhance haemoglobin levels.
Introduction
Globally, Anemia is the most common public health problem during pregnancy. 1 It affects developing and developed countries. 2 In recent estimate of anemia globally, 1.8 billion people are living with anemia. 1 About 30% of non-pregnant women and 37% of pregnant women were anemic. 3 According to Karami et al 4 the burden of anemia particularly among pregnant women is high, thus, demanding targeted interventions in this population. Furthermore, the current evidence on anemia demonstrated that, there is high proportion of pregnant women affected globally.1,5-7
Moreover, systematic review and meta-analysis studies conducted in low- and middle-income counties had shown that, 42.7% of women experienced anemia during pregnancy.4,8 Besides, in 2017, and 2019, WHO stated iron deficiency during pregnancy was identified as the most significant public health problem.3,9
The documented evidence from 82 low and middle income countries on the burden of anemia among reproductive age is high, the developing country such as West Africa, Middle Easter and Asia, including Gambia 53.3%, Senegal 47.3%, Male 47.6%, Yemen 57.4%, India 49.9%, of prevalence was reported. 10 Besides, other study proof from global burden of disease demonstrated high prevalence of anemia. 1
In Ethiopia, demographic and health survey (DHS) report indicated that, 24% women had anemia. 11 Besides, different localized researches studies in Ethiopia have revealed a high burden of anemia among pregnant women range from 23.2%−33%.12-15
Pregnant women require supplementary iron and folic acid to meet their own nutritional needs as well as those of the developing fetus.16,17 Micronutrient deficits in iron and folic acid during pregnancy can possibly and undesirably impact the health of the mother, her pregnancy, as well as fetal development.18-20 Recent evidence has shown that the use of iron and folic acid supplements is associated with a reduced risk of iron deficiency and anemia in pregnant women.21-23 Moreover, failure to take iron-folic acid during pregnancy, possibly lead to iron deficiency anemia.19,24
Anemia is contributing significant public health consequences for human wellbeing and social and economic improvement.1,9,25 In addition, anemia in pregnancy increases the risk of low birth weight, preterm birth, perinatal and maternal mortality.8,26-28 Moreover, poor psychological and motor developments negatively affect productivity and economic growth.29,30
In Ethiopia, the government has exerting unlimited efforts to improve pregnant women nutritional status, despite of that, the burden of anemia is still a medical challenge. On top of that, the existing published evidence concentered in central and agrarian communities. However, there is no evidence in remote and pastoralist communities. Therefore, this study aimed to assess determinates of hemoglobin among pregnant women in agro-pastoralist rural communities in South Omo Zone, Ethiopia.
Materials and Method
Setting
This study was conducted in the South Omo Zone, 1 of 15 zones in the Southern Nations, Nationalities, and People’s Region (SNNPR) of Ethiopia. The zone capital is Jinka, a city in the Southern part of the SNNPR; 480 km from the regional capital of SNNPR, Hawassa; and 850 km from Addis Ababa, the capital of Ethiopia. 31 The Central statistical agency CSA estimates a population of 749 214 in the South Omo Zone, accounting for nearly 4% of the total population of the region, of whom 359 623 are males and 389 591 are women. 32 An estimated 26 531 of the population is pregnant women and 11 487 pregnant women 31 are residing in the study districts. The current study was conducted in 5 randomly selected districts of south Omo Zone such as Dasench, Hammer, Benytsemay, Malle, and South Ari.
The main food harvests produced in the Zone are maize, sorghum, “teff”, coffee, vegetables, root crops, pulses, and oilseeds. The communities in the Zone are mainly agro-pastoralist and their livestock include cattle, goat, sheep, horse, mule, and others. 33
Study design and period
The community-based, cross-sectional study design was used. This study was conducted from April to June 30, 2019.
Population
Source population
• Pregnant women aged 15 to 49 years who reside in the South Omo Zone.
Study population
Pregnant women aged 15 to 49 years who have been exposed to under nutrition in the previous year reside in randomly selected rural “kebeles” in the districts
Inclusion criteria and eligibility criteria
Inclusion criteria
• Pregnant women aged 15 to 49 years who exposed to under nutrition in the previous year
Exclusion criteria
• Pregnant women who were unable to respond or communicate due to critically illness during the data collection period.
• Pregnant women, who were unwilling to consent to blood testing
• Pregnant women who could not be found at home after 3 repeated visits
Sample size determination
The sample size was determined by using single population proportion formula: with the assumption of 95% confidence level and 5% margin of error, 5% of non-response rate, and 1.5 design effect, considering the previous proportion of 32% prevalence of anemia.
34
The final sample size considered for study was

Sampling technique
Multi-stage stratified sampling method used to stratify the ecological zones; the criteria used for ecological zone classification, considered altitude. Initially, all districts in the Zone were listed and stratified into 3 ecological zones based on their altitude: highland, midland, and lowland. For each stratum, districts were selected randomly and then kebeles (smallest administrative structure) were selected through computer based simple random sampling. The sample size was then allocated to the strata proportional to the population size. Pregnant women were registered in the kebele through a health extension program. Simple random sampling was used to select pregnant women age group of 15 to 49 years old from the registered list.
Data collection procedures
An interviewer administered, structured and pretested data collection tools were used to collect data. The socio-demographic aspect of the questionnaire was adapted from DHS 11 and food frequency component was prepared from existing literature and the dietary diversity assessment tool for pregnant women was also adapted from the Food and Agricultural Organization. 35 Moreover, a HemoCue ® Hb301 was used to measure blood hemoglobin levels. The samples were taken from pregnant women who had follow-up their pregnancy. Blood was taken from the fingertips of respondents using micro cuvettes and inserted into the Haemocue. The measurements were then recorded. The overall testing procedure was carried out by an experienced laboratory technician. Basic safety measures were taken during the collection of the blood samples. Initially, the questionnaires were developed in English and were later translated into the local language, and then the questionnaires were again translated back into English for language editing by experts. Eight trained nurses and 3 supervisors were recruited for data collection at field.
Operational definition
Data quality assurance
The researchers carefully designed data collection tools. Data collectors were selected and recruited based on their experiences, such as nurses and laboratory technicians. After recruitment process completed, 2 days training had given for the data collectors and supervisors. The pre-test was carried out in the nearby “Bakadewela” district in which a population with comparable socio-demographic attributes to the study population. The pre-test study was conducted among 52 pregnant women. After the pre-test study was carried out, the discussion was made for half day at Jinka town and minor instrument revision had done based on findings. Researchers and supervisors had conducted field data collection supervision in daily bases.
Data management and analysis
The researchers were manually checked the data completeness, consistency, missed values and unlikely responses before actual data entry initiated. Moreover, coded the responses and entered data into Epi info version 7 and then exported to SPSS software version 26, and then cleaned, analyzed, interpreted, and summarized data. The descriptive and bivariate analysis was done, and then multivariate logistic regression analysis was applied to assess the association of socio-demographic and other independent factors with anemia. The outputs of the regression analysis were presented with a crude odds ratio (COR) and adjusted odds ratio (AOR) with their respective confidence intervals (CI). The criteria for exporting variables to the multivariate model were P-value <.25. Furthermore, variables with P-value <.05 were used to declare statistically significant association.
In this study, the model fitness was checked by Hosmer-Lemshow’s goodness fit test which was found non-significant. Besides, Multicollinearity was checked between independent variables by using variance inflation factors (VIF < 10) test. This was found no collinearity identified.
Ethical consideration
Ethical approval was secured from the Ethics and Higher Degrees Committee of the University of South Africa (UNISA). A permission letter was secured from the South Nation Nationality People Regional Health Bureau and the South Omo Zone health department. The permission letters clear the details of the community-based research study; the purpose and objectives of the study, the risks, and benefits to the respondents; explain the roles and responsibilities of the study respondents; ensured informed consent. The individuals who were not interested to participate were given the right to do so. The confidentiality of the respondents was ensured throughout the study. Ethical principles were respected in the study process.
Results
Demographic characteristics of respondents
A total of 526 study subjects were carefully selected, of which, 469 pregnant women successfully completed the questionnaire voluntarily, yielding a response rate of 89.2%. The mean (±SD) age of the research respondents were 27.4 ± 4.9 with minimum and maximum ages of 15 and 42 years old, respectively. The median initial marital age was 18.0. The mean ± (SD) for the first marriage was 18.31 ± 1.88 and a range with a minimum value of 14 and a maximum age value of 24 years, respectively(Table 1).
Demographic characteristics of pregnant women presented in community of South Omo Zone, Southern, Ethiopia.

Majority of the respondents, 96.2% (n = 451) of the pregnant women were married. In this study area, >16 ethnic groups lived peacefully in cultural diverse settings. Nearly half of the respondents, 46.1% (n = 216) the pregnant women were cultural religion followers, followed by one-third of the respondents, 36% (n = 172) were protestant followers. The mean (±SD) for level of education attended was 1.26 (±2.77). A very large proportion, 78%(n = 366) of the pregnant women were illiterate. Similarly, 76% of the partner’s education were illiterate (Table 1).
Majority, 82.5% (n = 387) of the respondents were housewives. Besides, the mean (±SD) of the family size was 4.7(+2.7). Nearly, 50% of the partners were working as pastoralist, followed by 37.8% (n = 176) of the respondents were in farming, 6.5% (n = 30) were working as merchants, and 3.4% (n = 16) were working as employees. Almost all, 99.6% (n = 466) of the respondents were living within rural (Table 1).
Prevalence of anemia
The mean (±SD) of hemoglobin concentration adjusted for altitude was 11.8 ± 1.7 and smallest and largest values ranged from 6 to 16 g/dl. The overall prevalence of anemia was 39.9% [95% CI: 35.5, 44.4]; 19.4% (95% CI: 16.0, 23.2) was mild, 19.6% (95% CI: 16.27, 2.5) was moderate and 0.9% (95% CI: 0.25, 2.25) was severe anemia (Figure 1).

Prevalence of anemia among pregnant women in the rural community of South Omo Zone, South nation nationality people, Ethiopia.
The main reason for not taking iron sulphate
Of the total respondents, 64% (n = 300) of the research respondents reported that they did not take ferrous sulfate pills, whereas only, 36% (n = 169) respondents reported as they were taking iron-folic acid (IFA) supplementation. The respondents were requested to provide the major reason for not taking or not using the tables continuously, 62.3% (n = 292) of the research respondents indicated that they were experienced unwanted consequences (side effects) of the tablets, followed by 56% (n = 267) of the respondents had reported that, many of them forgot to take the pills. Similarly, 48% (n = 255) of the respondents reported that they were unaware of the benefits of the pills and one-third (31.6%) of the respondents revealed that they were afraid to take the tablet, may harm their newborn baby. Moreover, a significant proportion of the respondents, 13.9% (n = 65) indicated the costs, even though the service was free for pregnant women. Simultaneously, more than a quarter, 28.4% (n = 133) of the pregnant women reported that they lacked belief in the usefulness of the pills (Figure 2).

Reason for not taking or not using ferrous sulfate tablets among pregnant women at the community level, South Omo Zone, Ethiopia.
Predictors associated with anemia
Bivariate analysis was done to determine the significance level among following variables such as wealth quintile, ecology, religion, malaria infection, taking ferrous sulfate, dietary diversity, nutritional information, under nutrition, family size, pregnant women occupation, partner’s education, para, gestational age, ANC visit, knowledge score, nutrition practice score, workload, flesh meat, fish, drinking coffee /tea, health facility walking distance, awareness of anemia, iron-rich food, and food insecurity level were found to be statistically significant, with the P-value <.25 was accepted as the cut-off point for multivariate analysis.
Pregnant women who had low dietary diversity (LDD) in the 24-hour preceding the interview, indicated that there was a high prevalence of anemia (79.1%) when compared with pregnant women who consumed high dietary diversity (HDD) (4.0%). The prevalence of anemia decreased when the dietary diversity level increased and vice-versa.
Likewise, the prevalence of anemia was high (85.5%) among study respondents, who did not take iron sulfate when compared with those who took iron sulfate (14.4%) regularly. It was notable that, not taking/using iron sulfate was statistically significant with anemia (x2 = 61.3, P = .000). The odds of being anemic were 5.7 times higher among pregnant women who were not taking or using iron sulfate than the respondents’ groups who were taking iron sulfate (AOR = 5.7, 95% CI: 3.3, 9.8).
After bivariate logistic regression model analysis was carried out, the eligible variables, with P-values that were <.25 were entered in the logistic model (called multivariate analysis) to control confounder factors.
The risk of anemia was reduced in the respondents’ groups who reported walking a short distance daily that is, walking <30 minutes to get to the health facility, compared to respondents who walked long distances (a distance greater than 30 minutes). The odds of anemia were 60% less likely to occur among those who walked <30-minutes than those who walked distances greater than 30 minutes (AOR = 0.4, 95% CI: 0.3, 0.6).
Moreover, the odds of anemia were 40% less likely to occur among the respondents who had no malaria infection in the past 3 months compared with those who had malaria infection in the past 3 months. In addition to this, pregnant women who had gestational age in the first and second trimesters were negatively associated with anemia (AOR = 0.5, 95% CI: 0.3, 0.9).
Table 2 indicated that pregnant women reported that the odds of being anemic were 8.9 times higher among the severely under-nutrition groups compared to those who had no under nutrition (AOR = 8.9, 95% CI: 2.1, 37.3). Moreover, pregnant women who had not consumed fish as a meal, had 2.4 times (AOR = 2.4, 95% CI: 1.3, 4.5) increased risk of having anemia. Moreover, the chance of developing anemia was 2.5 times higher among the “moderate food insecure” group compared with their food secured counterpart respondents [(AOR = 2.5,95% CI:1.4, 4.6) (Table 2).
Multivariate Analysis Variables Characteristics Among Pregnant Women in Rural Community of South Omo Zone, Ethiopia.
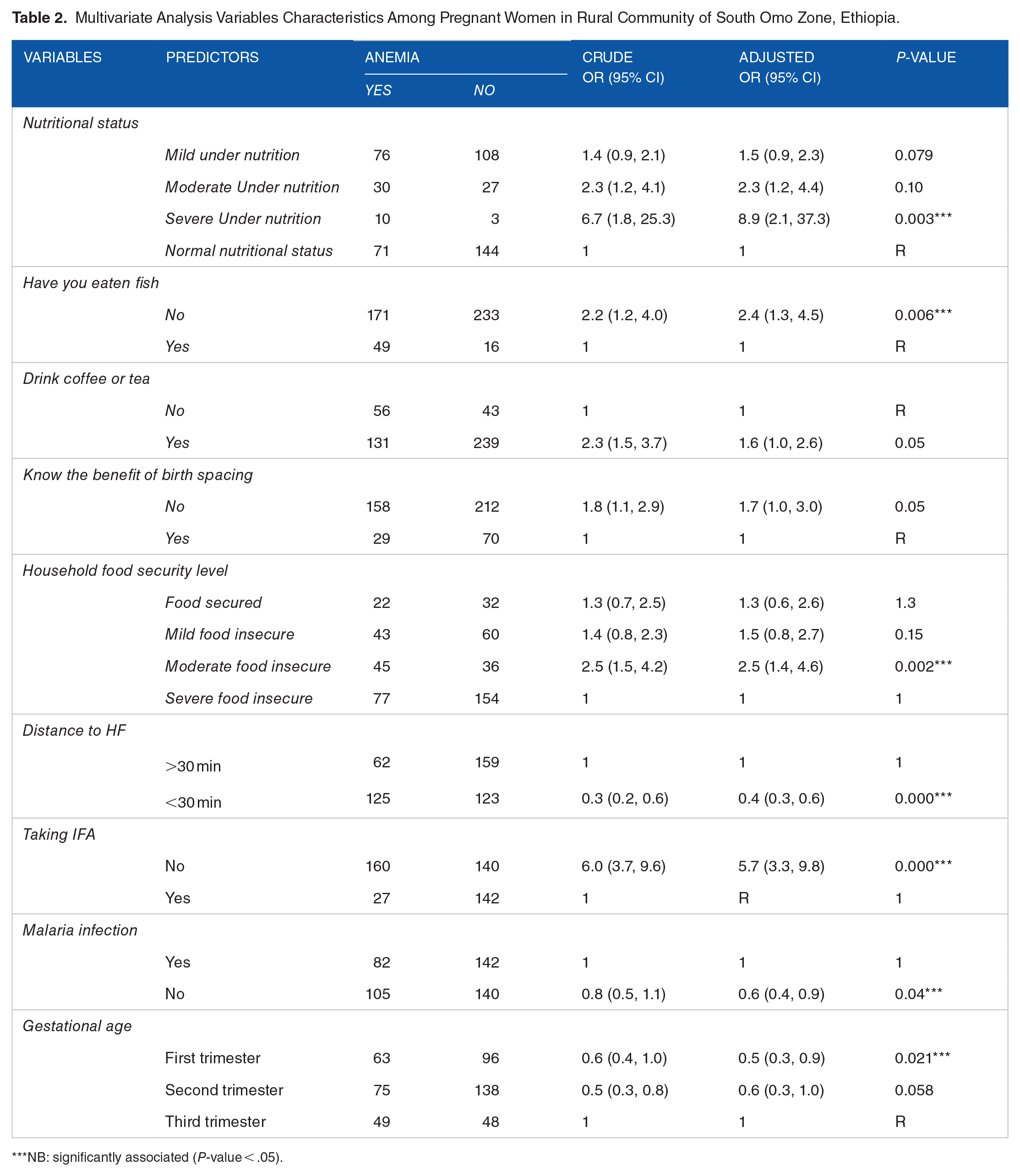
NB: significantly associated (P-value < .05).
Discussion
In the current study, the overall prevalence of anemia was 39.9% [95% CI: 35.5, 44.4], which was a very high burden and categorized as having severe public health significance in the study area. 9 This result was similar to the previous study evidence in Lao PDR, 39.2%, 38 Ghana, 40.8%, 39 and also study report from the local context, pastoralist communities of Ethiopia, 39.8%, 40 and Southern, Ethiopia, 39.94%. 41
Our study had revealed a higher prevalence of anemia when compared with previous studies conducted by Enawgaw et al 12.9%, 42 Lebso et al 23.2%, 12 Geta et al 26.4%, 14 Getahun et al 27.6%, 43 Bekele et al 32.8%, 44 Kejela et al 33%, 45 Gebre and Mulugeta 36.1%, 46 Alemayehu et al 36.1%, 47 Karami et al 36.8%, 4 and Animut and Berhanu 37.5%. 48 The possible explanations for higher burden of anemia in the study setting could be seasonal, socioeconomic, study respondents were movable communities, and agro-ecological variation may contribute for higher burden.
This finding had lower prevalence of anemia than the previous study conducted by Liyew et al 41.82%, 49 Shitu and Terefe 44.28%, 50 Wemarkor 50.8%, 51 Meda et al 63.1%, 52 Ekpe et al 72.6%, 53 Saaka et al 70%, 54 Bereka et al 63.8%, 55 and Gibore et al 80.8%. 56 The possible justification for prevalence difference could be socioeconomics, geographical/a study-setting discrepancy, and study respondent’s variations.
The proportion of anemia was higher (41.2%) among severe food-insecure households compared to food secured households (11.7%). The chance of developing anemia is 2.5 times higher among the modest food insecurity category compared with food secured respondents. This finding is comparable with other studies conducted elsewhere in Pakistan, 57 in Brazil, 58 and also from the local context, the Amhara region Ethiopia, 59 and North East Ethiopia. 15 In contrast, anemia is not associated with Food insecurity. 60 The possible justification for this could be the lack of adequate and preferable food that is rich in iron nutrients lack may lead to malnutrition and then lead to anemia.
The finding of this study showed that, those who were under-nourished respondents were 8.7 times more susceptible to develop anemia than well-nourished respondents. This study was consistent with study conducted elsewhere in Gondar, Ethiopia, 37 West Shewa Zone, Oromia Region, Ethiopia, 61 Wollega Oromia, Ethiopia 62 and Dessie town, northern central Ethiopia, 63 Bench, Ethiopia, 64 and Jigjiga. 65 The likely explanation for this could be lack of adequate nutrition during pregnancy leads to deficiency of micronutrients so that there is a higher chance of developing anemia.
The results of this study demonstrated that pregnant women who did not consume fish are 2.4 times higher odds to have anemia than those who consumed fish. This finding was comparable with the existing studies conducted in Ghana, 39 Louisiana,66,70 South Africa 67 and Jigjiga, Ethiopia. 65 The possible clarification can be, fish/meat has a rich source of iron and is better absorbed from the body.
This finding revealed that, pregnant women who had low dietary diversity (LDD) in the 24 hours, had a high prevalence of anemia (79.1%) when compared with pregnant mothers, who had high dietary variety (HDD) (4.0%). The prevalence of anemia decreases when dietary diversity levels increase and vice-versa. Researchers could not find any other significant associations from multivariate analysis. This finding is comparable with the Study conducted in Ghana, 54 in India moderate/severe anemia not significantly associated dietary diversity. 68 However, the recent findings were contradict the previous study result which was conducted in Wollega Zone, Oromia, Ethiopia, 62 West shewa, 61 Hossana, Ethiopia, 69 Tanzania, 56 Sub-Saharan Africa 14 and Zanizibar 56 dietary diversity was associated with anemia. The possible disparity could be lower socioeconomic status, pastoralist communities, and also nutritional taboos affecting dietary diversity levels.
The burden of anemia was higher in respondents who did not take iron sulfate when compared to their counterpart. Pregnant women who did not take iron sulfate had 5.7 times higher anemia than those who took it. This study is consistent with study conducted in various countries.12-14,48,58,62,70,71 The possible reason could be that during pregnancy the physiological iron desire is high and the measure of iron assimilated from the routine eating is not adequate to fill numerous pregnant women’s requirements. Therefore, iron supplementation is a very important component of programs to control iron inadequacy anemia and it also increases the hemoglobin concentration.
Our study demonstrated that pregnant women in the early gestational period have a lesser probability of becoming anemic than those in the third trimester. This study finding is comparable with study conducted in various study settings.12,41,64,70,72 The possible rationale for this could be pregnancy increases iron demand to compensate their physiological needs. Besides, there is a rapid growth of the embryo during this period that could decrease hemoglobin levels.
Malaria infection during pregnancy is a serious public health and life-threatening emergency in Ethiopia. Developing nations, particularly Africa, have a higher load of malaria. 73 Malaria causes severe anemia in sub-Saharan Africa during pregnancy. 74 The current study had shown that, pregnant women who had no history of malaria infection in the previous 3 months had a 40% lesser probability of becoming anemic than those who were infected. This finding is consistent with study conducted various countries.13,39,75 The possible justification could be malaria species especially Plasmodium falciparum attacks red blood cells and consequentially cause anemia.
The proportion of lower hemoglobin level had higher among those who drank coffee when compared to their counterpart. Pregnant women who drank coffee immediately after a meal had 1.6 times higher risk to becoming anemic than those who did not. This result was consistent with existing evidence,56,61,64,71,76 it showed a positive relationship between drinking coffee and becoming anemic in pregnant women. The possible justification is coffee inhibits iron absorption and that facilitates iron inadequacy in the body consequently leading to anemia.
Strengthen and limitation
The researchers considered adequate sample size, and multiple variables. However, this study didn’t show temporal relationship; data collected at 1 season, and study conducted at rural community that may not represent town are the limitation of this study.
Conclusion
In general, 4 out of 10 pregnant women had lower hemoglobin level, which is a severe public health problem in the study area. No taking Iron Folic Acid (IFA), severe under nutrition, no fish food, moderate food insecurity, drinking coffee and having no malaria infection history were a contributing factors. Therefore, it desires particular attention to invest and promote in food security, dietary diversity, nutritional status, iron-folic acid supplementation, and nutritional information provision for the pastoralist and agrarian community to alleviate the anemia.
Footnotes
Acknowledgements
The manuscript part is taken from thesis submitted to University of South Africa (UNISA), The development of a community based prevention model for under nutrition among pregnant women in Southern, Ethiopia by Tsegaye Alemu Gute available at ![]() . Besides, we would like to extend our heartfelt appreciation to laboratory technicians and nurses who took part in blood sample and data collections at field. We would like to forward special thanks to Mr. Mintesnote Melka and TemsgenTefera who facilitated a finical support in-field data collection. Lastly, we would like to appreciate pregnant women who took part in this study.
. Besides, we would like to extend our heartfelt appreciation to laboratory technicians and nurses who took part in blood sample and data collections at field. We would like to forward special thanks to Mr. Mintesnote Melka and TemsgenTefera who facilitated a finical support in-field data collection. Lastly, we would like to appreciate pregnant women who took part in this study.
Abbreviation
● DHS = Demography and health survey
● MUAC = Mid upper arm circumference
● SNNPR = South nation nationality people Region
● IFA = Iron Folic Acid
Authors’ Contributions
TA: Conceptualizing, methods, literature review, participated in data collection at the field, conducted data analysis and interpretation, draft result writing.
ZZN: Methodology, Supervising, validation of the research, resources, reviewing, editing, and writing the manuscript.
TY: Methodology, the literature reviewed, validation of the research, reviewing, editing, and writing the manuscript. All authors have read and approved the manuscript.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
Data used for this study interpretation is available at the hand of the authors