
Abstract
Background:
Observational studies have shown that insoluble fiber (IF) can be effective in preventing type 2 diabetes (T2D), but there is a lack of experimental data on the effect of short-term consumption of IF on metabolic parameters. We tried to investigate whether there was an improvement in glycemia and body composition in individuals at risk for T2D after 3 months of IF consumption.
Methods:
This “Type 2 Diabetes Mellitus Prevention Ukraine (T2DPUA)” study describes participants with impaired fasting glucose (IFG) as determined by ADA criteria. The study involved 30 people, including 21 women (70%). Daily, 15 g of IF derived from wheat was used. T2DPUA did not have a placebo group and the intervention lasted 3 months. Evaluation of fasting plasma glucose (FPG) and 2h plasma glucose (2hPG), glycated hemoglobin (HbA1c), total cholesterol, HDL-cholesterol, triacylglycerols, uric acid, and γ-glutamyl transferase was performed. The baseline and 3-monthly anthropometric examinations included measurements of weight, waist and hip circumference. Fat mass was assessed by bioelectrical impedance analysis. Paired samples t-test or Wilcoxon test were used.
Result:
A decrease of FPG (P = .042), HbA1c (P < .001), 2hPG (P = .005), weight (P < .001), body mass index (P < .001), the proportion of body fat (P = .006), and the absolute amount of fat (P < .001), increases in systolic (P < .001) and diastolic (P = .008) blood pressure was shown. The number of people with hypertension did not change. The absolute amount of body fat decreased by almost 5% and tolerance to the standard glucose load improved by 15%. The dynamics of other metabolic parameters were not revealed.
Conclusion and Recommendation:
Data about improvement of glycemia and body composition over a short period of using IF by individuals with IFG are new and deserve larger studies.
Primary prevention of type 2 diabetes mellitus (T2D) remains one of the most important tasks of medical science and practice. In 2010, evidence-based European guidelines were published. 1 According to these recommendations, people with impaired glucose tolerance and/or impaired fasting glucose should be intensively intervened, that is, active measures should be taken to prevent the transition of hyperglycemia to the stage of diabetes. Insoluble cereal fibers have been shown in large prospective cohort studies to be highly effective in preventing T2D,2,3 but there is a lack of interventional data. Optimal Fiber Trial (OptiFiT) in 2 year randomized double-blind prospective intervention study compared the effect of an insoluble oat fiber extract with that of placebo on glucose metabolism and incidence of diabetes. It did not provide strong evidence for a beneficial effect of insoluble cereal fiber on glycemic metabolism. OptiFiT demonstrated a small effect on HbA1c as a secondary outcome, while the primary outcome on diabetes incidence was not achieved and 2-h glucose levels only reached statistical significance in women. 4 Meanwhile a secondary analysis of the OptiFiT suggested that fiber-related hypoglycemic effect might be limited to subjects with impaired fasting glucose (IFG). 5 It should be noted that the intervention within the OptiFiT Study lasted 1 and 2 years and included the use of starch as a placebo. Starch is not a glycemically neutral substance because it has a glycemic index of at least 40, 6 as well as a certain caloric content while slowly digested starch may have even therapeutic applications, such as control of diabetes. 7 A long period of intervention in the OptiFiT study increased the need for and value of placebo. Our aim was to investigate whether glycemic and anthropometric changes occurred in individuals in the IFG group after 3 months of consuming insoluble dietary fiber without using the placebo group in such an assessment.
Methods
Study population and design
Randomly selected adult rural residents of Kyiv region (Ukraine) who had not previously been registered as T2D patients, signed an informed consent form, and oral glucose tolerance test (OGTT) was performed. This population sample was repeatedly investigated in the context of T2D and other blood glucose categories.8-11
A present “Type 2 Diabetes Mellitus Prevention Ukraine (T2DPUA)” study describes participants with impaired fasting glucose (IFG) as determined by ADA criteria, 12 which were the inclusion criteria of the study. Exclusion criteria were T2D diagnosis or absence of signed informed consent. The study involved 30 people, including 21 (70%) women and 9 (30%) men. Patients’ age ranged from 38 to 72 years, mean 57.5 ± 10.3 years (X ± SD). For the sample size estimation, G*Power 3.1.9.7 12 was used (also see Supplemental Material 1). The minimal sample size was equal to n = 21, for the non-parametric Wilcoxon signed-rank test (matched pairs) minimal sample size was equal to n = 29.
Dietary supplements
The supplements were provided as drinking powders every month, when the individuals attended a primary care unit, and participants were instructed to take the supplements twice daily. To enrich the high-fiber supplement with insoluble cereal fiber, a purified fiber extract derived from wheat was used (VITACEL Wheat Fiber WF 600-30, containing 96% insoluble fiber). This supplement added 15 g of mainly insoluble fiber per day (7.5 g per serving) to the normal nutrition. The volunteers were provided with instructions on how to use the drinking powder: the recommended intake was twice daily dissolved in 300 mL of water, preferably before breakfast and dinner. This protocol is very similar to the one used in the OptiFiT Study. 4 OptiFiT Study used 15 g (fiber group) or 1.6 g of insoluble fiber daily as placebo for 2 years. Unlike the above, T2DPUA study did not have a placebo group and the intervention lasted just 3 months.
Some characteristics of the studied population
All studied persons did not receive medications to lower blood glucose. Some lifestyle information was collected before the start of the intervention by filling out a questionnaire. The majority of respondents (86%) confirmed the daily use of fruits and vegetables fresh or freshly cooked at least 500 g/day, which may indicate a sufficient supply of soluble fibers. All persons confirmed the level of daily physical activity recommended by T2D prevention guidelines, 1 most of the interviewed persons did not smoke and consumed alcohol very moderately (see details in the Supplemental Material 2).
The trial T2DPUA was registered at clinicaltrials.gov (NCT04283201).
The study protocol was approved by the ethics committee of the Institute of Endocrinology and Metabolism, National Academy of Medical Sciences, Ukraine. After signing an informed consent form, the participants filled out questionnaires, providing information about current treatment and lifestyle. All of those involved, including family physicians, took part in the study as volunteers.
Blood glucose measurements and categorizations
Thirty participants with IFG were enrolled into the T2DPUA between July 2020 and June 2021. IFG was defined as a fasting plasma glucose concentration of 5.6-6.9 mmol/L. 13
OGTT was performed according to WHO recommendations, 14 and blood plasma glucose was measured by the enzymatic method. The blood sampling was done after at least 10 hours of fasting and 2 hours after taking a glucose solution (75 g of glucose in 200 mL of water). Blood plasma was separated by centrifugation and stored in a cold environment for 24 hours for further testing.
Other measurements
Evaluation of HbA1c was performed using a rapid analyzer and test cartridges “Clover A1c” (“Infopia Co., Ltd.,” Korea), which uses the method of boronate affinity to fix HbA1c. Blood samples were analyzed for total cholesterol, HDL-cholesterol, triacylglycerols, uric acid; and γ-glutamyl transferase by standard methods in the research laboratories of the Institute of Endocrinology and Metabolism, National Academy of Medical Sciences, Ukraine.
The baseline and 3-monthly anthropometric examinations included measurements of weight to the nearest 0.1 kg (in light indoor clothes without shoes), height to the nearest 0.5 cm, and waist and hip circumference. Fat mass was assessed by bioelectrical impedance analysis (BIA; Body Impedance Analyser Bodystat, Advantage Health Care Pty Ltd Braeside Victoria 3195 Australia). ActiGraph devices and software were used to objectively assess physical activity (https://www.actigraphcorp.com/).
Statistical analysis
For the analysis, statistical package MedCalc® Statistical Software version 20.027 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2022) was used.
To present quantitative variables the arithmetical average (Mean) and (±SD) standard deviation (normal distribution) or the median (Me) and (Q1-Q3) interquartile range (non-normal distribution) were calculated. Paired samples t-test or non-parametric Wilcoxon test (paired samples) to define the change of the parameters after the intervention were used. Frequency (%) was calculated for presentation of the qualitative variables. McNemar’s test to define the change of the nominal data after the intervention was used.
The critical level of significance in the analysis was accepted as α = .05.
Results
Analysis of metabolic biochemical parameters of persons at risk of developing T2D before and 3 months after the intervention (intaking insoluble dietary fiber) indicates the dynamics of glycemic levels. In particular, a statistically significant decrease in the level of FPG (P = .042), HbA1c (P < .001), 2hPG (P = .005) was shown, which indicates an increase in glucose tolerance according to OGTT (Table 1). Unfortunately, one of the subjects at the last moment abandoned the standard glucose load, and one sample was hemolytic, so the total number of subjects (n = 29) in the case of glycemic analysis decreased to 28. The absolute amount of body fat decreased by almost 5% (Figure 1), and tolerance to the standard glucose load improved by 15% (Figure 2). The dynamics of other metabolic parameters were not detected.
Metabolic parameters of persons at risk of developing T2D before and 3 months after the WF intervention (insoluble wheat fiber intake).
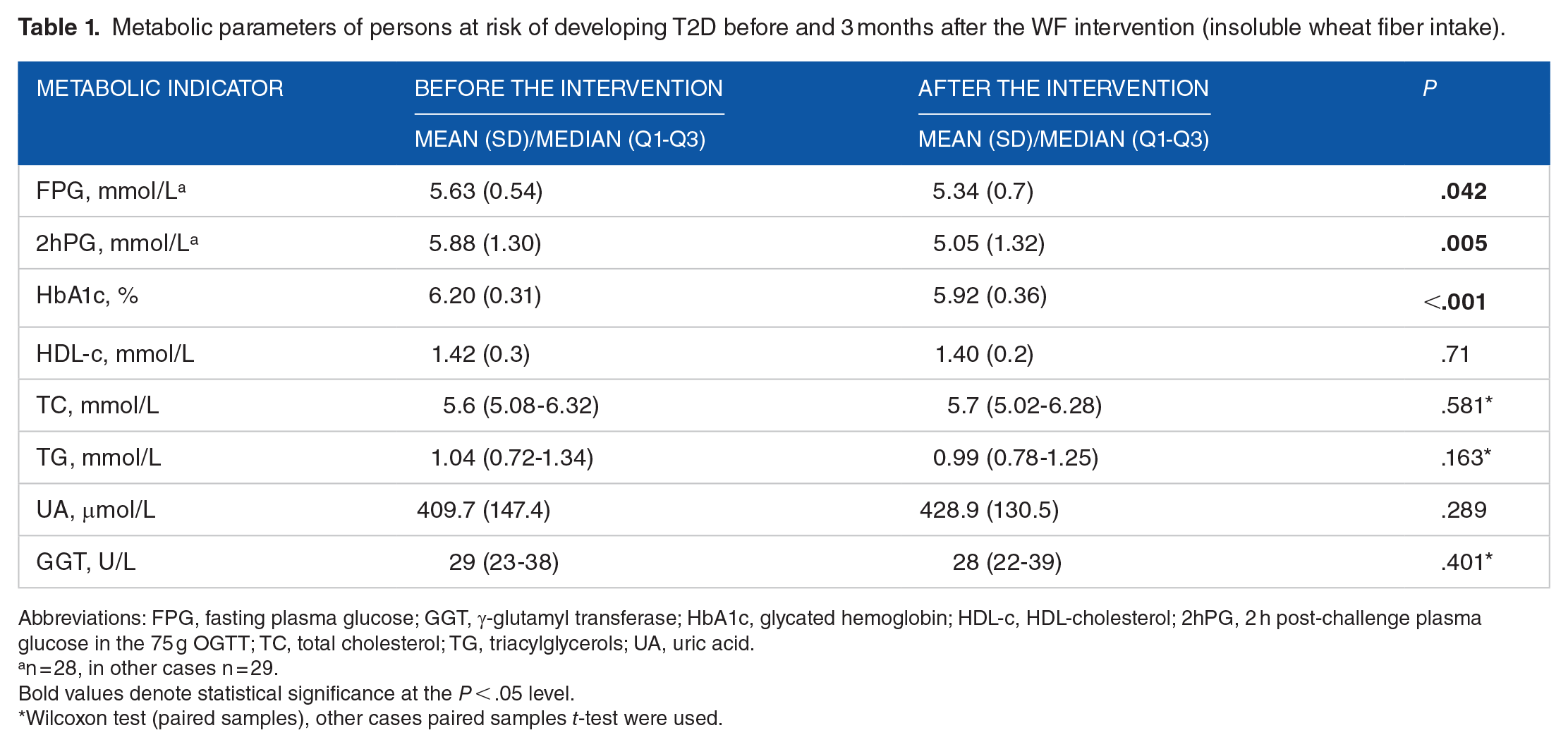
Abbreviations: FPG, fasting plasma glucose; GGT, γ-glutamyl transferase; HbA1c, glycated hemoglobin; HDL-c, HDL-cholesterol; 2hPG, 2 h post-challenge plasma glucose in the 75 g OGTT; TC, total cholesterol; TG, triacylglycerols; UA, uric acid.
n = 28, in other cases n = 29.
Bold values denote statistical significance at the P < .05 level.
Wilcoxon test (paired samples), other cases paired samples t-test were used.
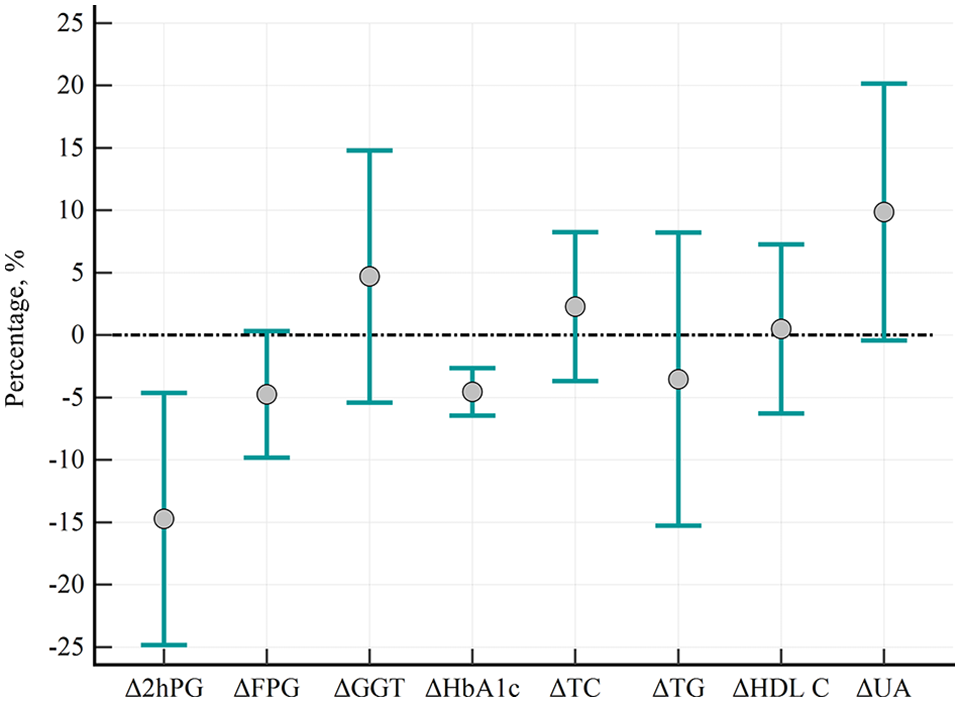
Changes in biochemical parameters (∆, %) after consumption of insoluble dietary fiber, average value and 95% CI are presented.
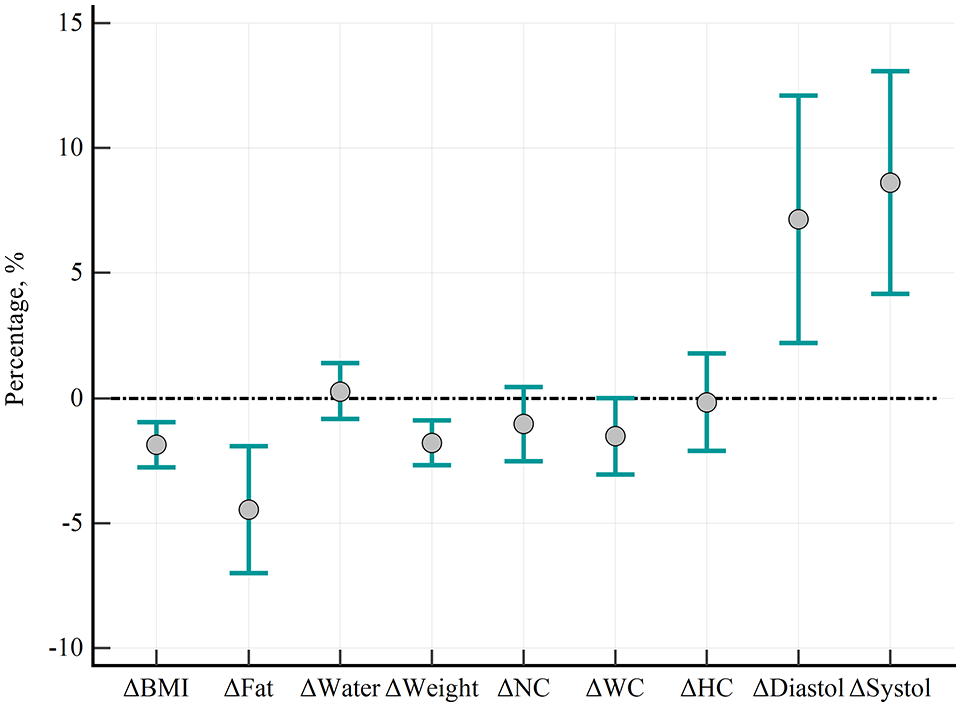
Changes in anthropometric parameters (∆, %) after consumption of insoluble dietary fiber, average value and 95% CI are presented.
The study of anthropometric indicators revealed the dynamics of body composition under the influence of 3-month WF intervention (insoluble wheat fiber intake). In particular, there was a decrease in weight (P < .001), body mass index (P < .001), the proportion of body fat (P = .006) and the absolute amount of fat (P < .001) and a tendency to decrease waist circumference (P = .063) with increasing the share of total water in the body (P = .006) according to the bioelectric method, increase in systolic (P < .001) and diastolic (P = .008) blood pressure. Physical activity indicators were low and did not change after the intervention (Tables 2 and 3). The number of people with hypertension (blood pressure more than 140/90 mm Hg) after 3 months of intervention, did not change with any statistical significance (Table 4, P = .617).
Anthropometric and physical activity parameters of 29 persons at risk of developing T2D before and 3 months after the WF intervention (insoluble wheat fiber intake).
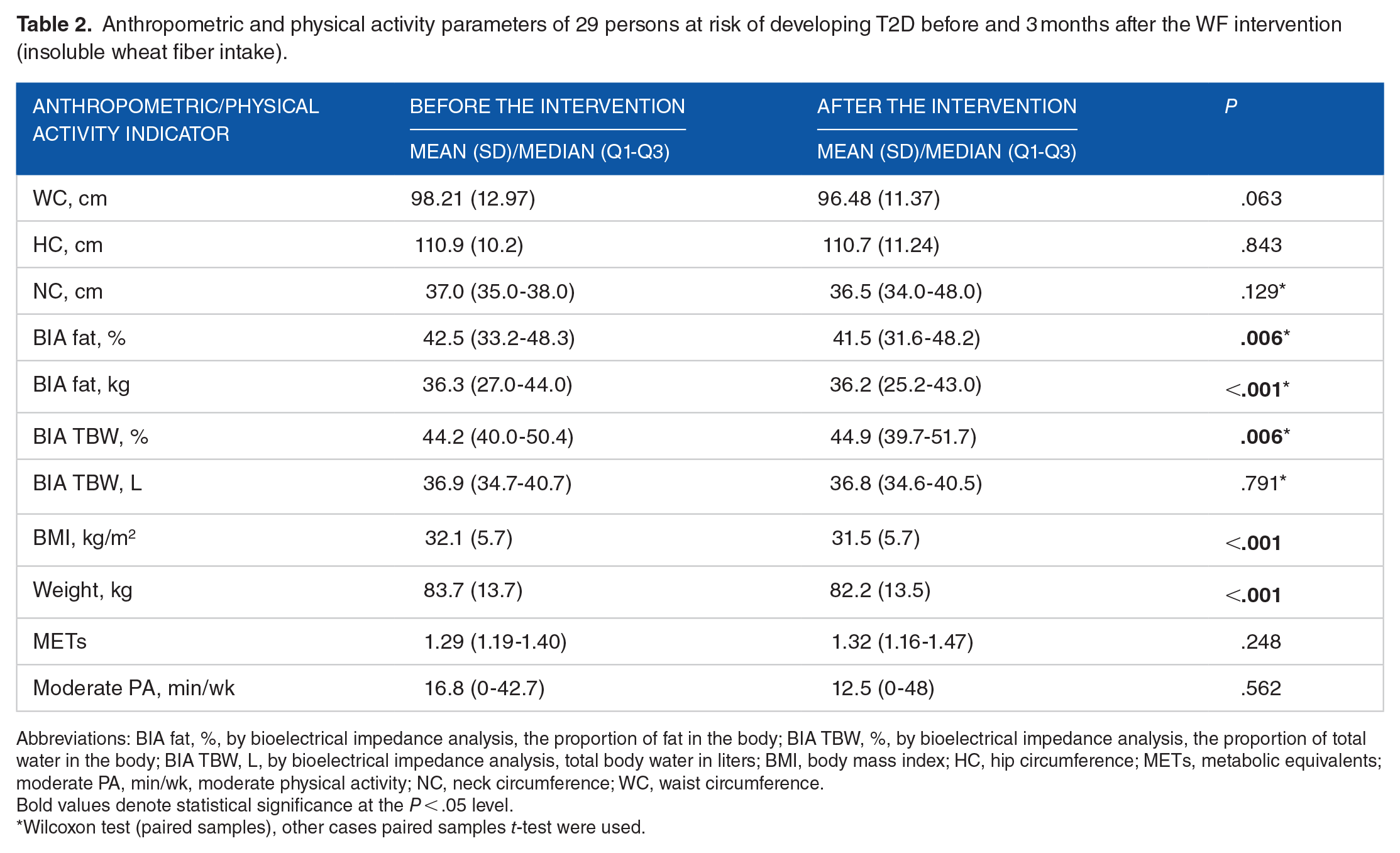
Abbreviations: BIA fat, %, by bioelectrical impedance analysis, the proportion of fat in the body; BIA TBW, %, by bioelectrical impedance analysis, the proportion of total water in the body; BIA TBW, L, by bioelectrical impedance analysis, total body water in liters; BMI, body mass index; HC, hip circumference; METs, metabolic equivalents; moderate PA, min/wk, moderate physical activity; NC, neck circumference; WC, waist circumference.
Bold values denote statistical significance at the P < .05 level.
Wilcoxon test (paired samples), other cases paired samples t-test were used.
Dynamics of blood pressure (BP) of persons at risk of developing T2D depending on the use of antihypertensive drugs before and 3 months after the WF intervention (insoluble wheat fiber intake).

Bold values denote statistical significance at the P < .05 level.
Wilcoxon test (paired samples), other cases paired samples t-test were used.
Dynamics of hypertension before and 3 months after the WF intervention (insoluble wheat fiber intake).
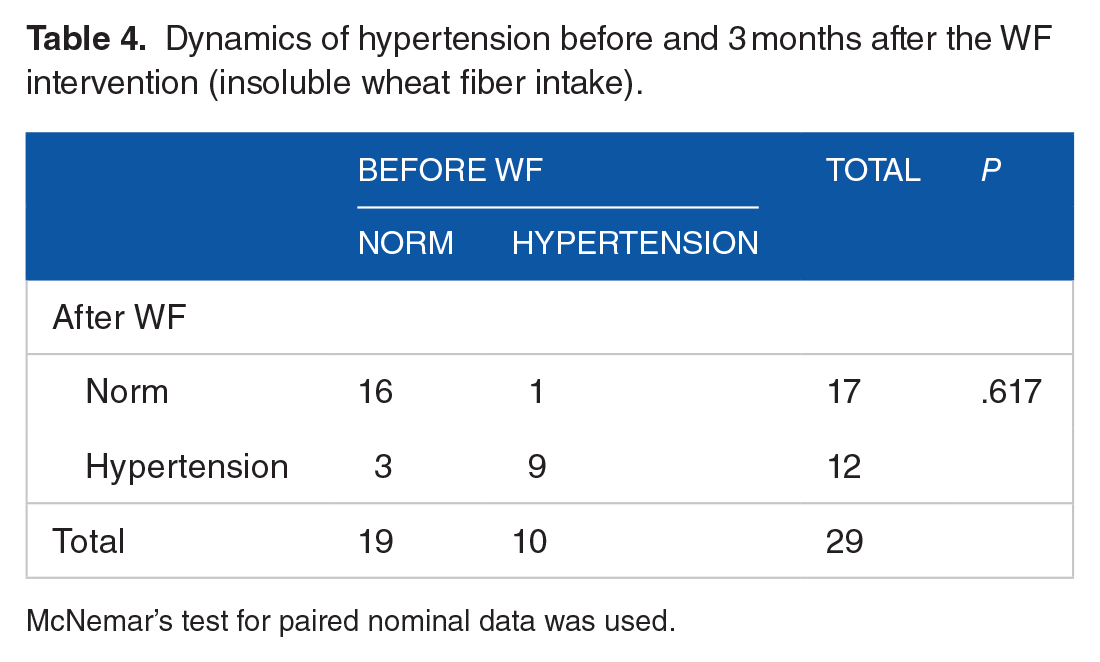
McNemar’s test for paired nominal data was used.
Discussion
Thus, a study of biochemical parameters of individuals in the IFG group before and after 3 months of intervention by consuming wheat insoluble fiber (WF) indicates a decrease in 2hPG, FPG, and HbA1c, indicating increased glucose tolerance and reduced fasting glucose.
The study of anthropometric indicators revealed the dynamics of body mass and composition: loss of weight, body mass index, fat content, and absolute body fat with increasing proportion of total water in the body according to the bioelectric method. These data significantly correspond to the results of the OptiFiT Study: within the IFG stratum, 2-h glucose, HbA1c, and γ-glutamyl transferase levels decreased more in the fiber group and compared to normal fasting glucose subjects, IFG subjects had larger benefits from fiber supplementation with respect to FPG. 5 OptiFiT Study does not suggest any difference between anthropometric indicators between placebo and fiber groups, whereas our T2DPUA Study revealed a decrease of body mass index and body fat after a 3-month long intake of WF.
It is quite possible that these differences can be explained by different design of the study—the absence of the placebo group and a shorter period of the intervention in T2DPUA. It should be noted that OptiFiT Study used 15 g (fiber group) or 1.6 g of insoluble fiber daily as placebo for 2 years, that is, the placebo group also received a considerable amount of insoluble fiber.
Also, unlike the OptiFiT Study we have noticed a certain increase of arterial blood pressure that requires confirmation and explanation through further research. It is necessary to find out whether a small but statistically significant increase in blood pressure after taking WF is associated with impaired absorption of drugs taken by T2DPUA Study participants.
A likely strength of our study is that we were able to supplement some recent experimental findings regarding the metabolic effect of insoluble dietary fiber intake by persons related to IFG. Even after 3 months of WF intervention, we found improvements in blood glucose and body composition.
The weaknesses of our study include the small number of participants and the lack of a placebo group. However, we believe that finding the ideal version of the placebo in this case is very difficult, and the relatively short period of intervention is a factor that can reduce the likelihood of erroneous estimates of its results. The number of studied couples (n = 29) is minimal but sufficient to achieve the necessary statistical power of our study (Supplemental Material 1). We hope that when scientific studies at the population level soon become possible again in Ukraine, they will be able to clarify our results.
Studies in context
Recently we have found that after 2.8 years of follow-up, the individuals who were impaired glucose regulation (prediabetes)—positive and who confirmed their adherence to lifestyle-based preventive recommendations had a significantly lower risk of identifying screen-detected diabetes mellitus. This effect appears to be related to recommendations to reduce the daily intake of sugar to less than 25 g. 11 Our other study 15 shows that persons with impaired glucose tolerance (IGT), but not IFG had lower indicators of physical activity than those, with normal glucose tolerance. The revealed extremely low level of physical activity indicates a significant potential of lifestyle modification that can be used for preventing diabetes mellitus among persons with IGT. However, increasing of physical activity by persons with isolated IFG may be unproductive. 16 Instead, for those with IFG, dietary modification may be an effective means of preventing T2D.
The BioCycle Study findings suggest that a diet high in fiber is strongly associated with decreased hormone concentrations and a higher probability of anovulation and further study of the effect of fiber on reproductive health and of the effect of these intakes in reproductive-aged women is warranted. 17 On the other hand, the observational research by Ma et al 18 indicated that higher intake of isoflavones and tofu was associated with a lower risk of developing Coronary Heart Disease. Isoflavones and related compounds act through the estrogen receptors (ERs) and are often used in postmenopausal women. 19 A clinical trial showed that genistein, which is the most abundant and active isoflavone in soy, acting as a natural selective ER-modulator, can improve surrogate endpoints associated with risk for diabetes and CVD in postmenopausal women with metabolic syndrome.19,20 Most of the individuals with IFG studied by us were women of menopausal age, therefore, when planning further studies on the dietary prevention of T2D, it is advisable to study the effect of not only the use of dietary fibers, but also isoflavones. It is possible that the addition of soy products, such as tofu, may counteract the possible hormonal effects of dietary fiber.
Nutritional studies in persons with metabolic syndrome living in urban and rural areas of Ukraine have revealed increased fat consumption from 37.7% to 44.4% of daily energy intake, high intake of mono- and disaccharides, and low fiber intake. 21
Currently, the nutrition of Ukrainians does not meet the criteria for known types of traditional diets (Mediterranean-style diet, Plant-based diet, Nordic dietary pattern, Oriental diet, etc.).
The only large-scale study on nutrition in Ukraine was STEPS by WHO. This study showed that two-thirds (66.4%) of the population did not consume enough fruits and vegetables (5 servings daily). 22 However, other significant nutritional features were not disclosed in this study. So further large-scale studies are needed to attribute the nutrition of the Ukrainian population to a certain type.
Dietary fibers may also play an important role in glucose homeostasis influencing the gut microbiota composition. 23 In Ukraine, there is some seasonality in food products, especially fiber intake, which can also affect the gut microbiota. For example, in the Ukrainian population, seasonal fluctuations in the main microbial types of intestines were revealed, which, according to the authors, may be associated with seasonal changes in fiber intake. 24 The interaction between nutrition and the gut microbial community composition in the Ukrainian population has been little studied to date. So, the gut microbiota is an important factor to be considered in our future research of T2D prevention and treatment.
Conclusion
Data about improvement of blood glucose and body composition over a relatively short period of use of insoluble dietary fiber by individuals with IFG are new and deserve larger studies to possibly prevent T2D.
Supplemental Material
sj-docx-1-nmi-10.1177_11786388221125181 – Supplemental material for Metabolic and Anthropometric Parameters of Persons at Risk of Developing Type 2 Diabetes Mellitus Before and After 3 Months of Consuming Insoluble Dietary Fiber
Supplemental material, sj-docx-1-nmi-10.1177_11786388221125181 for Metabolic and Anthropometric Parameters of Persons at Risk of Developing Type 2 Diabetes Mellitus Before and After 3 Months of Consuming Insoluble Dietary Fiber by Mykola D Khalangot, Vitaly G Gurianov, Tamara F Zakharchenko, Yurii M Pysarenko and Victor I Kravchenko in Nutrition and Metabolic Insights
Supplemental Material
sj-docx-2-nmi-10.1177_11786388221125181 – Supplemental material for Metabolic and Anthropometric Parameters of Persons at Risk of Developing Type 2 Diabetes Mellitus Before and After 3 Months of Consuming Insoluble Dietary Fiber
Supplemental material, sj-docx-2-nmi-10.1177_11786388221125181 for Metabolic and Anthropometric Parameters of Persons at Risk of Developing Type 2 Diabetes Mellitus Before and After 3 Months of Consuming Insoluble Dietary Fiber by Mykola D Khalangot, Vitaly G Gurianov, Tamara F Zakharchenko, Yurii M Pysarenko and Victor I Kravchenko in Nutrition and Metabolic Insights
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Academy of Medical Sciences of Ukraine grant 0119 U 001082.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MK and VK conceived the study design. TZ and YP participated in data collection and measurements. MK, TZ and VG participated in data analysis and interpretation. VG carried out the final statistical analysis. MK and VG drafted the manuscript and designed the figures. All authors approved the final version of the paper. All authors are grateful to Ms. Oksana Opanasenko and Ms. Maria Samusenko for technical assistance in conducting this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.