
Abstract
Aim:
To assess and explore the factors affecting willingness to undergo an early postpartum oral glucose tolerance test (OGTT) and receive postpartum lifestyle modification assistance.
Methods:
An explanatory sequential mixed-method design was used. A prenatal cross-sectional survey questionnaire (n = 216) was given to women diagnosed with GDM in a tertiary health institution in Singapore and followed up with postpartum semi-structured interviews (n = 30). Multivariate logistic regression and thematic analysis were conducted before merging the findings.
Results:
Despite universal GDM education, fewer than 75% intended to take the OGTT postpartum, and only 63% felt it was very important. The plan to take the OGTT postpartum was positively associated with a prenatal care provider’s specific recommendation. In contrast, Malay women were less likely to take the test. Most women interpreted a care provider’s recommendation as implying standard practice, which encouraged intended and actual compliance with testing after giving birth. The perception of moderate to high T2DM risk in the following decade, and subsidized prenatal care, and plan to take the OGTT postpartum were positively associated with willingness to receive postpartum lifestyle behavior support. A mobile application was the preferred method to receive support.
Conclusions:
In the early postpartum period, women with a history of GDM were willing to receive measures to reduce T2DM risk, primarily if it was under the supervision and recommendation of a care provider. A carefully designed but simple postpartum lifestyle intervention incorporating these preferences that can be integrated into mainstream diabetes prevention programs is warranted.
Introduction
Gestational diabetes mellitus (GDM) is one of the most common complications experienced by pregnant women. 1 GDM is characterized by glucose intolerance diagnosed for the first time during pregnancy and is a critical health complication. 2 It is clear that maternal risks extend beyond pregnancy, with GDM predisposing women to the development of type 2 diabetes mellitus (T2DM) mainly due to additional weight gain during pregnancy and failure to regain and maintain a healthy weight after childbirth.3-7
The leading health institutes such as American Diabetes Association (ADA) 8 and National Institute for Health and Care Excellence (NICE) 9 have recommended lifestyle improvements and diabetes screening (early postpartum oral glucose tolerance test [OGTT] and repeat diabetes screening) to assist in mitigating T2DM risk in women with prior GDM.10,11 The Agency for Care Effectiveness Singapore recommends women with a history of GDM to perform 2-point 75 g OGTT at 6 to 12 weeks after delivery and subsequent diabetes testing at least once every 3 years. 12 Although the recommended postpartum diabetes screening helps to confirm existing impaired glycemic activities, unfortunately, among women with a history of GDM, the uptake of postpartum OGTT appears to be universally poor. 13 In postpartum, apart from the responsibility for their new baby, cognitive and physical barriers can hinder their efforts to improve postpartum lifestyle behaviors.
According to previous findings, health-seeking and lifestyle improvements can be modified by the level of disease knowledge and awareness of personal disease risk. 14 Accurate risk comprehension and perceived susceptibility lead to improved lifestyle behaviors after childbirth. A thorough understanding of participation in health care utilization and co-creation of care among women with GDM is integral to patient-centered care. However, such an agreement to determine how women translate their diabetes prevention intentions into practice has been limited, mainly due to the lack of longitudinal studies. 15 Furthermore, although risk perception, personal health beliefs, social support, and self-efficacy influence the adoption of lifestyle behavioral modification postpartum, the generalizability of these influences is limited. 16
Asia is experiencing an increasing number of women diagnosed with GDM. 17 Singapore is a high-income multiethnic city-state in Asia. The evidence from a large cohort study supports that the GDM prevalence in Singapore is remarkably higher than in other developed countries such as the US.11,18 Further, the International Diabetes Federation ranks Singapore second only to the United States with the highest diabetes prevalence among developed nations. 19 By 2035, 1 in 4 residents over 21 years of age in Singapore are estimated to have prediabetes, with many people with diabetes remaining undiagnosed. 20
This study employed an explanatory sequential mixed-methods design to examine women’s intentions in the antenatal period and implementation in postpartum. This highlights 3 essential areas in postpartum behaviors relating to T2DM risk; women’s diabetes risk perception, participation in postpartum OGTT, and postpartum lifestyle assistance to reduce diabetes risk. Towards this aim, the specific objectives were
to quantitatively assess and qualitatively understand women’s perception of diabetes risk.
to quantitatively assess the predisposing, enabling, and need factors and qualitatively explore factors that are associated with intent to undergo the OGTT postpartum.
to quantitatively assess the predisposing, enabling, and need factors and qualitatively explore factors that are associated with willingness to receive postpartum lifestyle modification assistance.
Methods
Conceptual framework
Andersen’s 21 model is a behavioral approach that is used to understand health care utilization. Andersen and Newman suggested that population characteristics for health services utilization can be expressed as factors that predispose healthcare use, including barriers and/or facilitators, and the need for health care. We used the constructs of Andersen’s model of health behavior in this study to identify (1) predisposing, (2) enabling, and (3) need factors for the control of GDM and reduction of future T2DM risk (Figure 1).

Conceptual framework.
Design and study population
This study used an explanatory sequential design, including quantitative and qualitative components (Figure 2). 22 Public hospitals in Singapore follow the updated 2013 World Health Organization (WHO) diagnostic criteria 23 and offer universal screening to identify women with GDM. Women with abnormal test results are asked to attend an education session on GDM management given by an obstetrician/gynecologist specialized in GDM, a diabetes nurse educator, and a dietician. The key focus of these sessions is to advise patients on dietary control and periodic blood sugar testing. Women were asked to test blood glucose using a finger pricking device and record 7 times on 1 weekday and once over the weekend (pre-breakfast, post-breakfast, pre-lunch, post-lunch, pre-dinner, post-dinner, and post-late-night snack). GDM patients review these results with the specialist clinician every 2 weeks.

Explanatory sequential design.
A prenatal cross-sectional survey questionnaire was given to pregnant women aged 21 to 40 who were attending a GDM care clinic in National University Hospital (NUH), a tertiary health care institute in Singapore. The included women who had to have GDM diagnosed during the index pregnancy have attended the educational session delivered by a nurse educator and a dietician for GDM management. Women who could not speak English, with known pre-pregnancy type 1 diabetes or T2DM, were excluded. Women who gave their consent to be contacted in the postpartum were approached for semi-structured interviews.
Study tools
The prenatal cross-sectional survey consisted of 30 questions aimed to collect information on demographics, perception of T2DM risk, knowledge of T2DM, willingness to complete an OGTT postpartum, and to have lifestyle behavior support postpartum. The questions related to understanding and attitudes towards GDM and T2DM risk were adopted from work published previously.24,25 The survey included questions to ascertain perceived personal control related to future T2DM risk. There were 4 categories for the responses to these questions being “strongly agree,” “agree,” “disagree,” and “strongly disagree.” These were coded based on the way the question was worded.
The primary study outcomes were intent to complete the OGTT and willingness to receive lifestyle modification assistance postpartum. In the survey, women were asked “Are you intending to make a follow-up visit to repeat the OGTT after delivery as part of your postpartum care?” with the 3 answer options being “yes,” “maybe,” and “no.” They were also asked “After your child is born, would you be interested in receiving continued support related to diet and physical activity to reduce the risk of future type 2 diabetes?” with the 2 answer options being “yes” and “no.”
The topic guide for the semi-structured interviews was developed based on quantitative data and the Andersen behavior framework. It included sections on GDM and childcare support, postpartum OGTT visits, awareness and perceived risk for developing T2DM, adopting a healthy lifestyle and health-seeking behaviors, and postpartum lifestyle behavior intervention. The content was checked and verified by a field expert (J.Y.) and improved after pilot testing with 1 woman with a history of GDM.
Participant recruitment
Recruitment for the prenatal self-administered survey occurred from May 2015 to September 2015 (Phase I) and from August 2016 to May 2017 (Phase II). A study team member approached the women while they were waiting for their appointment with the specialist clinician at the GDM clinic at the GDM clinic. Phase I of the data collection offered the paper-based survey. In Phase II, women were able to choose between either paper or online-based surveys (SurveyMonkey Inc., San Mateo, California, USA). The participants were given S$25 reimbursement for participating in the survey.
Prenatal survey participants who consented to participate in the postpartum interviews were recruited using purposive sampling based on ethnicity and employment status. 26 Thirty face-to-face interviews were scheduled between May 2017 and March 2018, based on participant availability and location convenience. The researchers had no prior relationship with participants. After completing the informed consent procedure, the interviewer (a female Ph.D. candidate, S.S.H.) carried out the session in English and made notes. The sessions were audio-recorded and typically 30 to 50 minutes in duration. Finally, women completed a questionnaire, including details about demographics, GDM control, delivery outcomes, and current lifestyle behavior. All participants were given S$50 for their participation upon completion of the interview. The interviewer decided the point of data saturation and continued with 1 or 2 extra interviews for each ethnicity to verify data saturation. No repeat interviews were carried out.
Ethical approval was obtained from the National Healthcare Group Domain Specific Review Board, Singapore (NHG DSRB Ref: 2015/00196).
Data analysis
On average, 60 women attend the GDM clinic per month. In Phase I, 18.5% of the women visiting the clinic completed the prenatal survey. In Phase II, 67.2% of the women visiting the clinic were interested in the study. Out of those who were interested, 75.4% completed the survey in Phase II. The final survey completion rate of 44.0%. Among the nonparticipants, most declined to participate without reason. However, some women declined due to insufficient time.
Before pooling the 2 datasets from the prenatal cross-sectional survey, the participants’ characteristics of the 2 phases were statistically assessed. The results did not differ significantly between Phase I and Phase II (Supplemental Table 1).
Univariate analysis was conducted to describe the study participants. Factors associated with willingness to have postpartum behavioral assistance were analyzed using Student’s t-test for continuous variables, and Fisher’s exact test, and Chi-square test for categorical variables. Multivariate logistic regression models were developed to help understand the independent factors associated with postpartum behavior. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were obtained after controlling for significant covariates identified using bivariate statistical analysis (P < .1) and important covariates. The data were analyzed using STATA statistical software. 27
Forty-five women were approached to participate, with 30 undertaking the interviews postpartum. Lack of time after childbirth was the most common reason cited for not participating. For the qualitative data analysis, audio-recorded interviews were first transcribed verbatim and prepared for thematic analysis. 28 Two researchers (S.S.H. and A.S., a Ph.D. candidate experienced in qualitative research methods) coded the transcript using Atlas Ti Software (QSR International Pty. Ltd., 2012) and Microsoft Excel™. Codes were then identified from the data, and themes and subthemes were identified. Reliability checks were performed by reading and checking the transcripts independently and reaching an agreement on the meaning of the texts via discussion.
Finally, the quantitative and qualitative findings were compared, and the validation of the results was performed using triangulation. Our report follows the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement and the 32-item checklist of the Consolidated criteria for reporting qualitative research (COREQ).29,30
Results
Demographic and prenatal information
The mean age was 32 years, with most being Chinese (47.7%), were employed full-time or part-time (74.3%), and were university graduates (69.4%). Around half (49.8%) were in their first pregnancy and surveyed at a median of 31 weeks’ gestation. The majority (64.2%) were attending an unsubsidized clinic, perceiving their health as “good” (73.1%), while around half were either overweight or obese before their pregnancy (53.9%). Almost all participants managed GDM via diet control (97.2%), 47.7% used physical activity, and 9.7% used insulin. The demographic details of the participants are given in Supplemental Table 2.
The 30 postpartum interview participants were between 2 and 10 months postpartum. They had similar demographic details and prenatal care utilization to the survey participants. Moreover, most reported having a family history of T2DM and perceived their health quality as good. In terms of child delivery information, most had better pregnancy outcomes and had completed the postpartum OGTT with normal results, although only 3 had been informed of these.
Supplemental Table 3 shows the postpartum interview participants’ demographic information and GDM control and child delivery outcome details.
T2DM risk and knowledge
The vast majority (80.5%) of the survey participants stated that they had fair or good knowledge of T2DM, while 85.1% felt that they had either a slight or moderate chance of getting T2DM in the next ten years. Overall, the group had high perceived T2DM control (96.8%) (Table 1).
Perception of T2DM amongst survey participants.
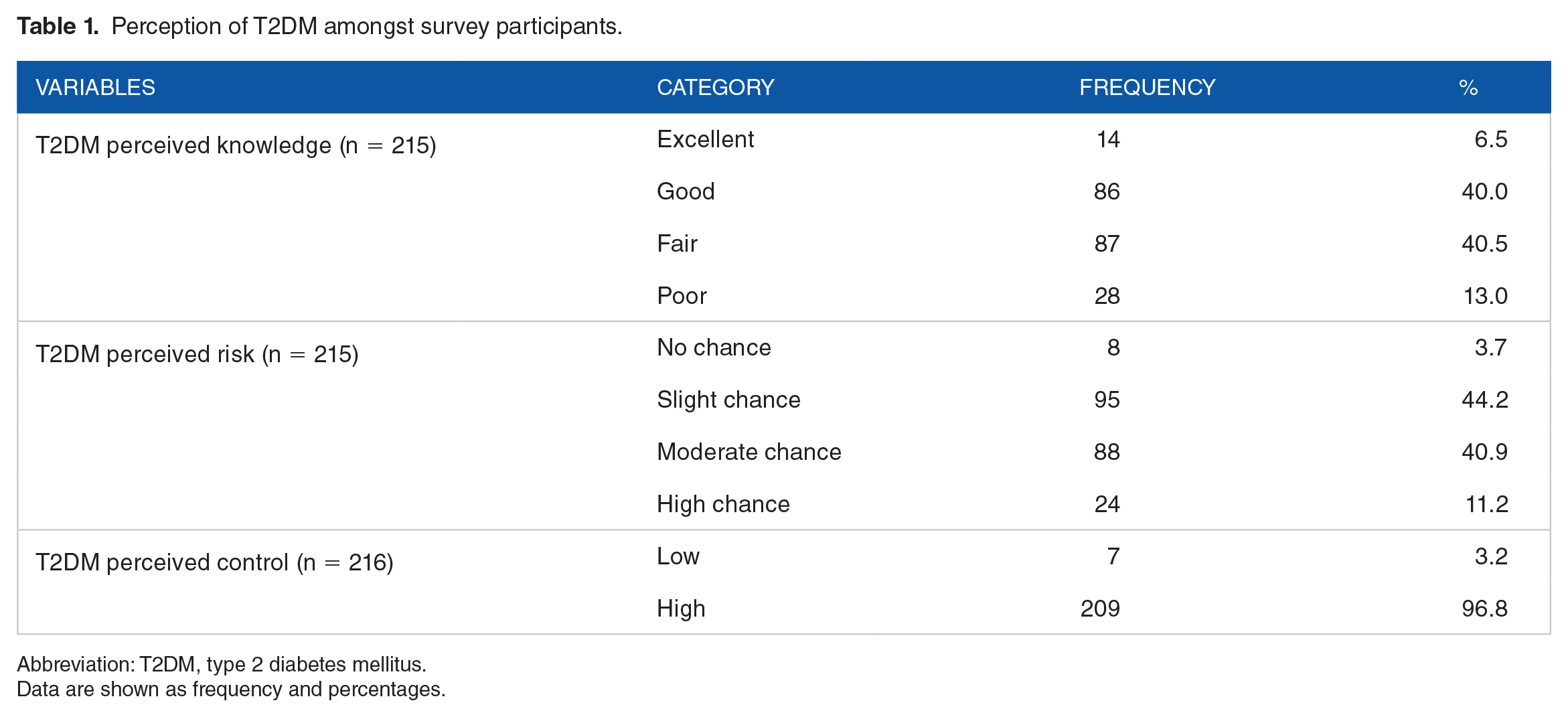
Abbreviation: T2DM, type 2 diabetes mellitus.
Data are shown as frequency and percentages.
Perception of T2DM risk after GDM
Similar to the quantitative findings, overall, the women felt that they had fair to good knowledge about diabetes. However, those who had a family history of diabetes did not seem to have marked knowledge of T2DM compared to women without any such history. In general, women recognized that having a history of GDM increased the future risk of diabetes (Table 3).
Those who seemed to worry about the T2DM risk often highlighted serious T2DM consequences. Most of the participants that reported having a family history of diabetes, and mostly Indian women seemed to be concerned about the risk and appeared to have initiated steps to improve their lifestyle.
The majority of participants had heard about the increased risk of diabetes from GDM prenatal care providers, or they had read about it in the GDM information provided. A few mentioned that their obstetrician was not overly concerned as their blood glucose readings were not in the higher range and their GDM was under control (Table 3).
Self-initiated lifestyle changes to reduce T2DM risk
Noticeably, most women believed that they could reduce the risk of T2DM. There was high awareness about the steps to minimize T2DM risk, mainly by controlling their diet and exercise. Such awareness was associated with changes made to their current diet patterns.
Conversely, normal postpartum OGTT results were considered by a few women to be a low risk for T2DM. Far fewer women felt that unhealthy lifestyle behaviors and family history of diabetes were more significant than GDM, resulting in the onset of T2DM (Table 3).
Postpartum OGTT completion
During pregnancy, most participants (62.8%) were recommended to perform the postpartum OGTT by their prenatal care physician at the time of the survey. However, 20.5% had not heard about the test. Similarly, 63.0% felt that completing the postpartum OGTT was very important, and 73.2% were planning to take the test. Hearing from a healthcare provider was significantly associated with women’s perception of postpartum OGTT priority (<0.05) (Table 2).
Details of postpartum OGTT of survey participants.

Abbreviation: OGTT, oral glucose tolerance test.
Data are shown as frequency and percentages.
Our unadjusted analysis suggested ethnicity, education (predisposing factors), perceived GDM knowledge after attending the clinic education session, and recommendation for postpartum OGTT (enabling factors) were significantly associated with planning to complete the postpartum OGTT. In our study, Malay women with GDM were 65% less likely (OR: 0.35, 95% CI: 0.16-0.75, P = .043) to plan to take the post-partum OGTT compared to Chinese women. However, compared to women without a degree, those with a degree were twice likely to plan to take the test (OR: 1.94, 95% CI: 1.03-3.66, P = .036). Women who reported good or excellent perceived GDM knowledge after attending the clinic education session indicated 2.5 times more likely to plan to take the test postpartum (OR: 2.53, 95% CI: 1.03-6.23, P = .038) than those who reported a poor or fair perceived GDM knowledge. Hearing about the test from a care provider had significantly higher odds of planning to take the postpartum OGTT (OR: 3.08, 95% CI: 1.65, 5.75; P > .05) than those who reported otherwise.
After adjusting for age, employment, and GDM knowledge after attending the GDM clinic, a doctor recommending the postpartum OGTT (OR: 4.01; 95% CI: 2.00-8.01) was associated with an increased likelihood of taking a postpartum OGTT. In contrast, Malay ethnicity (OR: 0.28; 95% CI: 0.12-0.69) was associated with a lower likelihood of completing a postpartum OGTT.
Twenty four postpartum interview participants had completed the postpartum OGTT at the time of the interview. A few were planning to complete the test in the future. One woman who was unaware of the test mentioned her plans to perform the test after the interview. One participant shared she had no intentions to complete the test because she was worried about the positive test results.
Perception of the importance of postpartum OGTT
During postpartum interviews, except for some Malay women, most participants mentioned they received advice from their prenatal care providers to repeat the OGTT postpartum. Some thought the test was part of routine prenatal care or had received a reminder from the clinic.
Out of the women who completed the postpartum OGTT, all except one participant had performed the test in the tertiary prenatal care clinic setting, particularly NUH. Almost all needed to reassure themselves that GDM had resolved. Only a few felt the test was unimportant but still completed it as a routine test. All except 3 of the women had normal test results. Most women who completed the postpartum OGTT did not have barriers that made it difficult to do the test. Among the few who were planning to complete the test reported difficulties in breastfeeding, lack of caregiver support, and conflicts in scheduling as barriers (Table 3).
Key themes of domains and participants’ responses.

Perception of OGTT follow-up
Most women did not know their test results. The standard clinic routine was only to inform women when results were abnormal. Women with normal test results did not receive further lifestyle advice.
Two trains of thought emerged. One group of participants felt that they wanted to know about their test results and the other felt it was sufficient to know that they were in the normal range, which they inferred by not receiving a phone call from the clinic.
Regarding advice on postpartum OGTT results, there was a perception of a lack of follow-up. Two women with normal test results actively contacted the clinic to learn of their test results, while only one woman with normal test results said that she was asked to repeat the test in 3 years. In contrast, along with the OGTT recommendation, a few Indian women mentioned that they were advised to improve and maintain their lifestyle behaviors.
Two women who had abnormal test results were given letters with basic details on improving diet and physical activity. These women expected further guidance, with 1 feeling anxious about insufficient direction (Table 3).
Willingness to receive postpartum lifestyle assistance
Of the study participants, 148 (69.8%) were willing to receive lifestyle behavior support after childbirth. The unadjusted analysis suggested that hearing about the postpartum OGTT from a care provider (OR: 1.81, 95% CI: 0.99, 3.31; P = .05) and moderate to high perceived T2DM risk in the next ten years (OR: 1.97, 95% CI: 1.08, 3.57; P = .026) and planning to take a postpartum OGTT (OR: 3.19, 95% CI: 1.68, 6.04; P > .05) (need factors) were significantly associated with willingness to have lifestyle intervention. Hearing about the postpartum OGTT from a care provider showed a strong relationship with planning to take a postpartum OGTT (P < .05), and thus it was excluded from the multiple logistic regression model. According to the final logistic regression model, after controlling for age, employment, and gravida, women who perceived themselves as having moderate to high T2DM risk in the next ten years (OR: 2.09; 95% CI: 1.10-3.94), visited a subsidized prenatal care clinic (OR: 2.07; 95% CI: 1.02-4.19) and planned to complete the postpartum OGTT (OR: 3.46; 95% CI: 1.76-6.78) were more willing to have lifestyle behavior support after childbirth.
Among women who were interested in receiving postpartum support related to reducing T2DM risk, approximately 26.6% ranked an application (“app”) for mobile devices as the first option, 27.7% ranked a website as the second option, and 29.1% ranked printed material as the third option. Most of the women (66.2%) preferred general tips on lifestyle change, but also some personal monitoring capabilities. Notably, social support from peers and personalized guidance or plans for lifestyle change ranked relatively low (24.5%).
Avenues for lifestyle and health-related information
During pregnancy, the GDM clinic helped the women to understand the basics about diabetes, especially that diet control was the key. Most thought they would need further assistance to control their diet and improve exercise, while a few women felt they had sufficient information.
Many women used the Internet for additional reading, but most did not follow a specific site, so it is unclear how credible the information was. In general, they used internet information as a guide or for comparison with several other websites, while only a few followed websites run by leading US health organizations.
In terms of social support, most women felt that they had help from their family (Table 3).
Preferred postpartum intervention for lifestyle behavior
In general, the participants were willing to receive postpartum behavioral support. They felt the need for a continuous program. A mobile application is their most preferred platform, mainly due to its convenience and integrability to their busy life. Any online program was identified as the second preferred option. The features expected from such a program were diet management, home-based exercise options, and reminders for continuous monitoring. Although many women did not have a preferred care provider, they expected a program with reliable information. Furthermore, most women preferred a session with a care provider so they could ask questions and get clarification.
Indian and Malay women were interested in a postpartum lifestyle program. Some mentioned that they were concerned about the schedule and childcare options. The primary motivators were their family and the desire to improve personal health. Cost, flexibility, and length of the program were the concerns raised (Table 3).
Discussion
This exploratory study examined postpartum women’s perception of diabetes risk and knowledge, postpartum OGTT completion, and willingness to receive postpartum lifestyle assistance. After triangulating the quantitative and qualitative data, converging findings suggest that enabling and need factors affect healthcare utilization behaviors in women with a history of GDM in Singapore. Our study revealed that there is an untapped potential to advance behavior change initiated after the diagnosis of GDM in the postpartum period.
We noted 3 promising factors essential for postpartum diabetes care for women with a history of GDM. First, there is a strong foundation and potential for knowledge interventions that may enable healthcare utilization. Women reported that their initial GDM knowledge improved significantly after attendance at the GDM workshop (Chi2 (9) = 53.97, P < .05). At the GDM workshop, they attained additional information on the postpartum OGTT and improved their knowledge and perception of T2DM risk after having GDM. Women reported fair to good knowledge and diabetes risk perception in both prenatal survey and postpartum interview data. Most planned to complete the postpartum OGTT and were willing to receive support to reduce the future risk of T2DM. The factors significantly associated with both these potential outcomes were common to prenatal care delivery and T2DM risk perception. Continuation of information flow from the prenatal to postpartum period could frame and improve risk perception. 31 However, as reported by Feig et al 32 and Kieffer et al, 33 even with greater risk perception, this high-risk group is likely to fail to make appropriate lifestyle changes to reduce diabetes risk.
Our findings point to the importance of the antenatal care provider as a vital source of information and the manner of delivery.34,35 Most participants searched for supplemental information primarily through online platforms, which have become a vital source of health information. However, unregulated advice and excessive detail can lead to misinformed action or complete in action. 36 Our findings highlighted the women’s need for streamlined information and healthcare providers to disseminate reliable information in a complex environment. 35
Second, hearing about the test from a reliable source can change an inconsequential decision to consequential results and help women understand the impact of their actions. In this context, it appears that women are more likely to comply with antenatal care providers’ recommendations even in the postpartum period. Women were more likely to plan to complete the postpartum OGTT if they had received a recommendation from a health care provider to have the test, consistent with other studies showing that the involvement of a health professional improved postpartum OGTT uptake.13,37,38 Dennison et al 39 reported that having a healthy relationship with the local healthcare system is a motivational factor to participate in postpartum OGTT. Our qualitative results suggest that this compliance is strengthened when women view postpartum OGTT completion as an extension of their routine antenatal care. Still, compared to the other two ethnicities, Malay women were less likely to plan their postpartum OGTT. Incorporating the postpartum OGTT into the prenatal care process as the “default” option may lead to improved uptake of OGTT. Moreover, proactive patient contact and system-based programs may increase both compliance and understanding. 40
Compatible with other studies, women who wanted reassurance that their GDM had resolved were more inclined to perform the test. 31 However, women, especially those with abnormal postpartum OGTT results, perceived that the follow-up was inadequate. Lack of OGTT follow-up is a common issue reported in various health systems, and as highlighted previously, it requires additional attention at the health system level.41,42 Without additional guidance and support regarding future screening and lifestyle improvement, women with normal OGTT results may become less concerned about T2DM risk, influencing their future lifestyle behaviors.
Finally, comprehension of personal risk led to the establishment of better lifestyle choices after childbirth. 43 Yet women in the postpartum period may encounter 2 major challenges; the focus of health shifted from mother to baby upon delivery and struggled to adjust to the new environment where they may experience limited cognitive functioning and lack of time. 31 One suggestion that emerged in the postpartum interviews was developing a simple smartphone intervention that can be incorporated gradually into their current lifestyle. 44 Such interventions may be effective and cost-effective and produce better effects among this high-risk group.45,46 The continuum of care needs to focus on a smooth transition from antenatal to postnatal period, with viable strategies to integrate long-term sustainable lifestyle modifications to reduce diabetes risk in this high-risk group. 47 However, little is known about the implementation and continuance of behaviors in postpartum. Therefore, research is required to understand postpartum women’s long-term behaviors to reduce diabetes risk in Singapore. 15
This research has explored the health-seeking behaviors of women with a history of GDM in Singapore. We reported participants’ point of view regarding their perception of the assistant needed to mitigate diabetes risk using qualitative methods that are valuable in patient-centered care. The study was designed to gather comprehensive data on 2 critical periods of women with a history of GDM, antenatal, and early postpartum. Our study used the explanatory sequential mixed methods design first to understand quantitatively pregnant women’s perceptions and behaviors. Second, we used qualitative data collected in the early postpartum period to augment the quantitative outcomes.
Our study has several limitations, which should be noted for interpretation. Data were collected from women attending 1 public hospital, which may have different prenatal care practices from the other public and private hospitals in Singapore. Second, the data were cross-sectional and primarily observational in nature, are not able to establish causality between exposure and outcome. Moreover, some of the data included self-reported responses and were not measured using objective tools. As a result, the findings may suffer from selection, volunteer, and social desirability biases. We used Andersen’s healthcare utilization model in the data analysis. However, this model may bear limitations. Furthermore, here we only considered the components of population characteristics to predict women’s healthcare use. Still, our qualitative explanations strengthened the quantitative findings and extended the understanding of their predicted healthcare use. Although we tried to maintain researcher reflexivity, researchers may have introduced reflexivity bias due to the socially dependent nature of qualitative research. Moreover, qualitative findings may have limited generalizability. We need to interpret the results with caution because of the wide confidence intervals. This uncertainty of the estimate could be due to the small sample size and, therefore, need future studies to verify the findings. Finally, our study focused on the intention to comply rather than observed compliance. Further understanding of the gap between intention and actual compliance in a larger study sample is critical and is a key topic for further research.
Conclusion
In conclusion, context, message framing, and delivery are important factors in motivating women to improve postpartum behaviors. Inherently, pregnant women are highly receptive to expert guidance because of the trust that they place in their caregivers. Essentially, such dependability appears to be an opportunity that antenatal care providers can use to leverage resources effectively to enhance the perception of the increased risk of T2DM associated with GDM. Considering the study findings, the health system must establish appropriate and long-term strategies to curb their lifelong risk for T2DM. As there are barriers that women face in the postpartum period, including a return to work, there is a need for an intervention that can be integrated into real life. The level of interest a woman has in reducing her T2DM risk is a promising start for early intervention to curb the growth of diabetes in Singapore. However, further studies with a large sample size are required to verify the current findings.
Supplemental Material
sj-pdf-1-nmi-10.1177_11786388211016827 – Supplemental material for Factors Associated with Intended Postpartum OGTT Uptake and Willingness to Receive Preventive Behavior Support to Reduce Type 2 Diabetes Risk Among Women with Gestational Diabetes in Singapore: An Exploratory Study
Supplemental material, sj-pdf-1-nmi-10.1177_11786388211016827 for Factors Associated with Intended Postpartum OGTT Uptake and Willingness to Receive Preventive Behavior Support to Reduce Type 2 Diabetes Risk Among Women with Gestational Diabetes in Singapore: An Exploratory Study by Sumali S Hewage, Su Aw, Claudia Chi and Joanne Yoong in Nutrition and Metabolic Insights
Footnotes
Acknowledgements
The authors thank the prenatal survey and postpartum interview participants, their family members, and health care providers at the GDM clinic, National University Hospital, Singapore.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current research study was supported by the National University of Singapore (NUS) Global-Asia Institute NUS Initiative to Improve Health in Asia Research Grant (Grant No. NIHA-2013-1-002).
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Cladia Chi has received research funding from the Jana Care project for the work related to the subject matters discussed in this manuscript.
Author Contribution
JY and SSH conceptualized and designed the study, established the research question and designed the interview guide, and obtained the necessary ethics approval. SSH collected the data. SSH and AS performed thematic analyzes. SSH prepared the graphics, assisted in drafting the manuscript, and finalized the draft based on comments from other authors’ feedback. CC assisted in participant recruitment and review of the manuscript. JY assisted by critically reviewing the manuscript. All authors approved the final manuscript as submitted.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.