
Abstract
Keywords
Introduction
Obesity is a predominant and progressive disease.1,2 Regaining weight after weight loss is a common problem. 2 After 1 year, nearly half of the lost weight is regained and 70% to 80% of dieters regain their weight within 3 to 5 years. 3 A variety of weight loss methods are used ranging from self-help attempts at dieting or physical activity, professional counseling, pharmacological interventions, surgical interventions, and commercial proprietary weight loss programs.4-15
Balancing energy intake with energy expenditure is important for weight maintenance. 16 Individual characteristics and eating behaviors can be critical when determining the risks for gaining and/or regaining weight. Behavioral risk factors are linked with exposure to weight gain resulting in a long-term energy imbalance where energy intake is greater than energy expenditure.17,18 Some individuals’ eating patterns/behavior and weight gain are related to neurocognitive responses caused from food. 19 Understanding the neurocognitive response to food and associated type of eating behavior of an individual may be useful for those who are involved in weight loss counseling.
Schembre et al 17 posit that there are 4 eating behaviors that influence energy intake (routine restraint, compensatory restraint, susceptibility to external cues, and emotional eating) and have developed the Weight-Related Eating Questionnaire (WREQ) to measure these behaviors. The 4 constructs measured in the WREQ are based on 3 main psychological theories. Routine restraint and compensatory restraint are represented by the dietary restraint theory.20-22 Routine restraint is defined as intentional repetition of restricting food to control or maintain weight. 17 Dietary restriction has to result in a balance between intake and output for weight maintenance or negative energy balance for weight loss. 23 Compensatory restraint is defined as intentionally restricting the intake of food following a period of overeating. 17 Compensatory restraint has been shown to have an inverse association with body mass index (BMI). 17 Susceptibility to external cues is explained by the theory of externality and is described as eating in response to an external stimulus regardless of the internal state of hunger or satiety. 24 Herman and Polivy 25 posit that susceptibility to external cues has an effect on individuals with obesity and/or those that are dieting. Those who are obese and/or dieting tend to eat more in response to external cues.19,25 Emotional eating is based on the psychosomatic theory and is defined as eating in response to negative emotions. 26 Bourdier et al 27 reported a positive relationship between emotional eating and BMI. Understanding the association of the eating behaviors on the impact of energy intake may be useful for weight maintenance counseling.
Proprietary meal replacement programs (MRPs) are a popular method used by many for weight loss. Meal replacement programs have been shown to be more effective than education and counseling alone for weigh loss. 28 However, those who participate in the programs are not immune to the weight regain. There is a need for improving long-term weight-loss success in MRPs and identifying the eating behaviors that affect weight loss and maintenance. This information may be useful for those MRPs that include a health coaching component. These MRPs with a health coaching component provide access to a health coach that individually works with their members to help them adopt healthy nutrition, physical activity, and lifestyle practices. Being able to identify the weight-related eating behaviors (WREBs) that are associated with success in weight loss may be used to inform the health coaching process to support short and long-term success of the participant. However, there is limited research published focusing on eating behaviors of participants on MRPs. The aim of this article is to evaluate the WREB of participants on a proprietary weight loss program and determine which behaviors are associated with clinically significant weight loss (CSWL).
Methods
Sample
Data from participants actively or previously enrolled in a nationwide (United States) proprietary MRP that used health coaching were used for this cross-sectional study. This MRP with a health coaching component was designed to help participants lose weight and provide sustainable long-term success. In total, 20 000 participants were emailed and requested to complete an electronic questionnaire. Inclusion criteria included must be 18 years of age, nonpregnant, and must be enrolled in the program for greater than 1 month. Questionnaires were completed by 1482 participants. Participants who completed the questionnaire were given the option to provide their contact information to be entered in a drawing for a chance to win 1 of 20 US$200 Amazon gift cards. The study was approved by the Institutional Human Subjects Review Board at South Dakota State University.
Data collection
The questionnaires were self-administered via an online survey. Participants were queried for demographics and WREB using the weight-related eating questionnaire developed by Schembre et al 17 which included a total of 16 questions. The weight-related eating questionnaire queried 4 constructs: routine restraint (3 questions, Cronbach Internal Consistency alpha: .756), compensatory restraint (3 questions, Cronbach Internal Consistency alpha: .844), susceptibility to external cues (5 questions, Cronbach Internal Consistency alpha: .844), and emotional eating (5 questions, Cronbach Internal Consistency alpha: .899). 17 The question responses were Likert-type scales with response options as not at all, slightly, more or less, pretty well, and completely. The questions in each eating behavior category were scored 1 (not at all) to 5 (completely). The scores were calculated as the average of the sum of each WREB category. 17 A lower score indicates an individual is less likely to possess the respective eating behavior.
Data analysis
Participants with complete WREB data were dichotomized into those who achieved CSWL (n = 988) and those who did not (non-CSWL) (n = 494). The CSWL was defined as losing at least 10% of one’s body weight, when comparing current weight to program start weight.18,26 This definition was chosen as the benchmark for assessing differences that may occur in WREB. Comparisons in demographics between weight loss categories were evaluated using chi-square analysis or t tests and those that differed significantly were included in the regression analysis, with the exception of age, which was included due to its wide range. Variables associated with the outcome but with sample sizes too small to allow for comparison among groups were excluded (n = 28, nonwhite). Individuals who had been in the program for less than 1 month (n = 84) and who were no longer in the program (n = 13) were excluded, resulting in a final sample size of n = 1357. Logistic regression was used to determine WREB scores and odds of CSWL. Statistical significance was set at P ⩽ .05. Data were analyzed using Stata/SE 14.
Results
Demographics are presented in Table 1. There were no differences in age, education, marital status, income, or employment status between CSWL groups. Average age for individuals in the CSWL group was 48.0 ± 12.1 years and non-CSWL was 47.1 ± 12.7 years. Participants in both groups were predominantly female, married, and college graduates, which includes bachelor’s degree, master’s degree, professional school degree, and doctoral degree. Approximately one-third of participants in both groups earned a household income between US$30 000 and US$79 000, whereas another one-third earned a household income between US$80 000 and US$119 000. Most participants (>85%) were employed.
Participant baseline demographics.
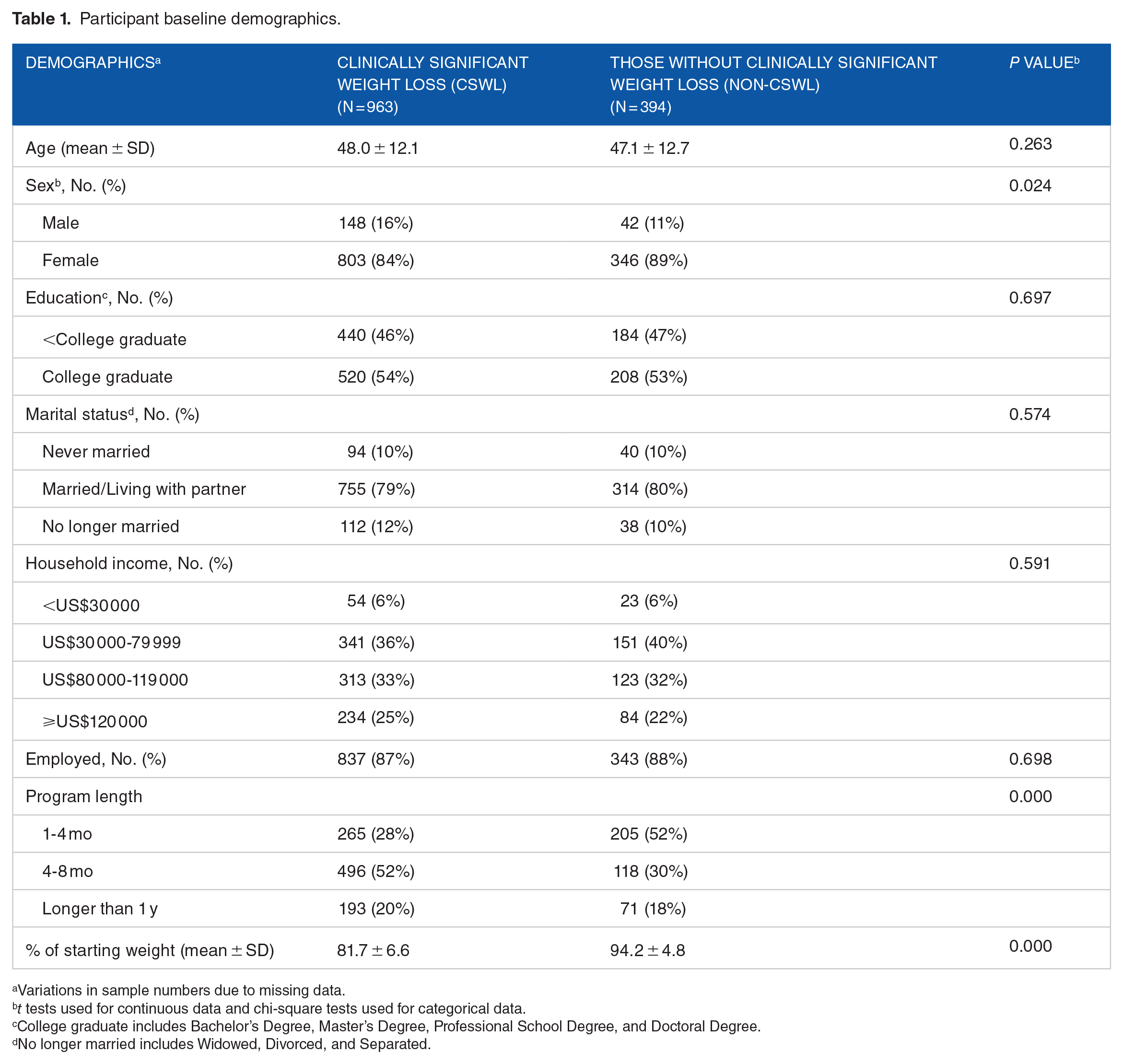
Variations in sample numbers due to missing data.
t tests used for continuous data and chi-square tests used for categorical data.
College graduate includes Bachelor’s Degree, Master’s Degree, Professional School Degree, and Doctoral Degree.
No longer married includes Widowed, Divorced, and Separated.
The WREB scores of routine restraint, compensatory restraint, susceptibility to external cues, and emotional eating scores by weight loss groups are reported in Table 2. Individuals with routine restraint had greater odds of having achieved CSWL (odds ratio [OR] = 1.21, confidence interval [CI] 1.05-1.41). There were no significant association with the compensatory restraint scores and weight loss. Individuals with higher scores in susceptibility to external cues and emotional eating behaviors had lower odds of having achieved CSWL (OR = 0.75, CI: 0.66-0.85 and OR = 0.78, CI: 0.70-0.86, respectively).
The weight-related eating behavior scores and their association with clinically significant weight loss.

Abbreviations: WREQ, Weight-Related Eating Questionnaire.
Analyses controlled for sex, age, and length of time in program.
Higher scores indicate greater frequency of measured behavior.
Significance was set at P ⩽ .05.
Discussion
The primary objective of this study was to evaluate the WREBs of participants on a proprietary weight loss program and the behaviors association with CSWL. The WREBs assessed in this study were routine restraint, compensatory restraint, susceptibility to external cues, and emotional eating. The WREBs of routine restraint, compensatory restraint, susceptibility to external cues, and emotional eating have been reported to influence weight. Our results indicate that participants with routine restraint eating behavior are more likely to lose weight while on a MRP versus those who display weight-related eating behaviors of susceptibility to external cues and emotional eating behavior.
Research regarding WREBs in participants who specifically are engaging in MRPs to control weight is limited. The participants in this article were enrolled in a MRP to lose weight. Although the sample was cross-sectional, there was an association between weight loss and those who had higher scores in routine restraint. Hartmann et al 29 conducted a study evaluating the eating behaviors and nutrition knowledge of individuals who consume meal replacements. Meal replacement users in this adult sample were more likely to report restrained eating and emotional eating behaviors than nonusers of meal replacements and both behaviors were correlated with BMI. The restrained eating behavior but not the emotional eating behavior was similar to the results reported in our study in which those with CSWL possessed the WREB of routine restraint. However, there was an inverse association with emotional eating and CSWL in meal replacement participants in our study. There are reports about the WREBs in cross-sectional samples of those who report dieting, as well as young adults not specifically dieting. In a cross-sectional sample of students who reported dieting, Nguyen and Polivy 30 reported similar associations between restrained eating and BMI. The chronic dieters who reported restrained eating had lower BMIs. Schembre et al 17 reported similar relationship in routine restraint but not compensatory restraint in a sample of young adults recruited from health-related classes at a university. Those who reported higher scores in the weight-related behaviors of routine restraint and compensatory restraint had lower BMIs. The differences in Schembre et al 17 and those reported in this article may be due to the characteristics of the sample. Those in our article were enrolled in a weight loss program versus those in the article by Schembre et al were not specifically recruited for weight loss.
Susceptibility to external cues and emotional eating has been found to complicate the relationship between dietary restraint, food intake, and changes in body weight.31-35 The susceptibility to external cues may affect what, how much, and where a normal weight individual eats, and in individuals with obesity, the internal state is irrelevant and food intake is predominantly determined by external cues. An individual with obesity is more likely to eat a larger amount of food than a normal weight individual when external cues are present. 34 Moreover, Masheb and Gril reported that individuals are more likely to overeat when experiencing emotions of anxiety and less likely to overeat when experiencing emotions of happiness. Also, emotional overeating is associated with the occurrence of episodes of binge eating. 35 These results, although are not from individuals on MRPs, are in concordance with the results from the results reported in this article which found that those who engage in the eating behaviors of susceptibility to external cues and emotional eating are less likely to achieve CSWL on a proprietary weight loss program. In the study by Hartmann et al, 29 it was concluded that individuals who engage in the eating behavior of susceptibility to external cues are less likely to consume meal replacement products.
Understanding the eating behavior that supports weight loss enriches the knowledge of the health coach to aid in an individual’s weight loss while on a proprietary weight loss program. The results from our study imply that those with routine restraint eating behavior contribute to the adherence of a proprietary weight loss program and those with eating behaviors of susceptibility to external cues and emotional eating are less likely to experience CSWL while on the MRP.
Due to the limitations, the results make not be generalized to all weight loss programs. First, the results are from a cross-sectional sample which prevents firm causal relationship. Second, the results are from a convenience sample of participants who were enrolled in a proprietary weight loss program that included meal replacements and health coaching. Third, there may be selection bias due to the sampling. Although the proprietary weight loss program is nationwide and all participants at the time of the study were invited to participate, the results are from participants who chose to answer the survey and may not be representative. In addition, due to lack of response from nonwhite participants, these results should not be generalized to other ethnicities. Another limitation is that height and weight were self-reported. However, as a component of the proprietary weight loss program, health coaches encourage self-monitoring of weight and others have reported concordance of self-reported weight and height with measured weight and height. 36
Conclusions
The aim of this article was to evaluate the WREB of participants on a proprietary weight loss program and determine which behaviors are associated with successful weight loss. In this study, individuals with higher scores for the eating behaviors of routine restraint had higher odds of achieving CSWL, whereas individuals with higher scores for susceptibility to external cues and emotional eating had lower odds of achieving CSWL. This knowledge on the type of eating behavior that is related to weight loss may be useful for health coaches in tailoring the coaching sessions to assist participants in being successful with weight loss in a proprietary weight loss program.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this project was provided by the Sanford Health South Dakota State University Collaborative Research program and by the SD Board of Regents R&D Innovation program. Partial funding was also supported by South Dakota Agricultural Experiment Station.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JS and LM drafted the design and collected the data. LM analyzed the data. MT and KKK drafted the manuscript. All authors reviewed and contributed to the writing of the manuscript.