
Abstract
Background:
This study was conducted to identify major dietary patterns and their association with level of asthma control among patients with asthma in Gaza Strip, Palestine.
Methods:
This cross-sectional study was conducted among a representative sample of Palestinian patients with asthma (both sex, aged 19-64 years) receiving care in chest department at Al-Shifa Medical Complex. Asthma control level was obtained using asthma control test. Data regarding other variables were obtained using an interview-based questionnaire and a semi-quantitative food frequency questionnaire. Statistical analysis was performed using SPSS version 20.
Results:
Two major dietary patterns were identified including (1) Prudent pattern characterized by a high intake of whole grains, beans and legumes, fish and shellfish products, vegetables, tomatoes, fruits, and vegetable oils, and (2) Western pattern characterized by a high intake of refined grains, red meat, poultry, fast foods, eggs, low-fat dairy product, high-fat dairy products, hydrogenated fats, olive, sugar, sweets, desserts, and snacks. After adjustment for confounding variables, patients in the lowest tertile (T1) of Prudent pattern had a lower odds for poorly controlled asthma (odds ratio [OR] = 0.044, 95% confidence interval [CI] = [0.002-1.316], P value < 0.05), whereas patients in the lowest tertile (T1) of Western pattern had a higher odds for poorly controlled asthma (OR = 2.499, 95% CI = [1.288-4.850], P value < 0.05), compared with those in the highest tertile (T3).
Conclusion:
A Prudent pattern may be associated with a lower prevalence of poorly controlled asthma, whereas a Western pattern may be associated with a higher prevalence of poorly controlled asthma.
Background
Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families, and the community. 1 It causes respiratory symptoms, limitation of activity, and exacerbations that sometimes require urgent health care and may be fatal. 2 Globally, asthma affects approximately 300 million people, and this number is expected to reach 400 million by 2050. 3 In Palestine, the prevalence rate of asthma in children living in villages, cities, and refugee camps were 17.1%, 8.8%, and 9.4%, respectively, with urban area having higher prevalence rate than rural areas. 4 Asthma is a serious global health problem affecting all age groups, with increasing prevalence in many developing countries, rising treatment costs, and a rising burden for patients and the community. 5 Asthma still imposes an unacceptable burden on health care systems and on society through loss of productivity in the workplace, and it still contributes to many deaths worldwide. 2 A number of factors including genetic predisposition, environmental factors, and lifestyle factors including dietary habits influence the development and expression of asthma. 6 The goal of asthma treatment is to achieve and maintain clinical control, which can be achieved in most patients with pharmacologic intervention strategy. 7 However, asthma control is still difficult to attain in all patients. 8 When asthma is uncontrolled, it has dire consequences for health and well-being. 9 Asthma Control Test (ACT) is a short, simple, patient-based tool for identifying patients with poorly controlled asthma; it is reliable, valid, and responsive to changes in asthma control over time, and in a clinical setting. 10 The ACT is a useful tool to help physicians identify patients with uncontrolled asthma and facilitate their ability to follow patients’ progress with treatment. 10 Asthma and its complications impact harshly on the finances of individuals and their families and on health systems and national economies through direct medical costs and loss of work and wages. 1 Dietary patterns is an approach that has been used to investigate diet-disease relations. 11 Studying dietary patterns instead of specific foods or nutrients is a new approach in nutritional epidemiology to assess the effects of overall diet. 12 Dietary patterns is usually determined by factor analysis and has been used to investigate the role of diet in several chronic diseases,13,14 but rarely in respiratory diseases. 15 Dietary pattern is potentially useful in making dietary recommendations because overall dietary patterns might be easy for the public to interpret or translate into diets. 16 Diet is one of the lifestyle factors that may play an important role in development and expression of asthma. 17 However, few studies have explored the relationship between dietary patterns and the level of asthma control. Most studies have examined the associations between individual foods or food groups and nutrients and the level of asthma control,18-20 instead of focusing on dietary patterns which is the most sensible approach to test the role of the overall diet on nutrition-related diseases. Therefore, understanding the association between dietary patterns with the level of asthma control may be helpful in reducing asthma-related premature mortality and improving outcomes among patients with asthma. To the best of our knowledge, this is the first study that examined this association among patients with asthma in Gaza Strip, Palestine. This study was conducted to identify major dietary patterns and their association with the level of asthma control among patients with asthma at Al-Shifa Medical Complex in Gaza Strip, Palestine.
Methodology
Study population
This cross-sectional study was conducted in the year 2018, among a representative sample of Palestinian patients with asthma. Patients were randomly selected using the systemic random sampling method. We recruited 105 patients with asthma, both sex, aged 19 to 64 years, receiving care in the chest department at Al-Shifa Medical Complex in Gaza Strip, Palestine. This hospital had the biggest chest department in Gaza Strip with 26 beds. 21 Pregnant women; lactating mothers; patients with other type of serious diseases such as cancer, acute myocardial infarction, end-stage kidney disease, and septicemia; and patients with other type of respiratory diseases were excluded from the study.
Asthma control test
The ACT was used to determine the level of asthma control. 22 The ACT is a patient completed questionnaire with 5 items assessing asthma symptoms (daytime and nocturnal), use of rescue medications, and the effect of asthma on daily functioning. Each item includes 5 response options corresponding to a 5-point Likert-type rating scale. In scoring the ACT, responses for each of the 5 items are summed to yield a score ranging from 5 (poor control of asthma) to 25 (complete control of asthma).10,23 Then, patients with asthma were classified into 2 groups: (1) well-controlled asthma (ACT scores: >19) and (2) poorly controlled asthma (ACT scores: 19 or less). 22
Assessment of anthropometric measurements
Weight was measured using a standard scale (Seca); the scale was placed on a hard floor surface; patients were asked to remove their heavy outer garments, and weight was measured and recorded to the nearest 0.1 kg. Height was measured in all patients (patients bare footed and head upright) with a measuring rod attached to the balanced beam scale; the height was reported to the nearest 0.5 cm. In addition, a stretch-resistant tape was used for measuring waist circumference (WC); WC was measured at the approximate midpoint between the lower margin of the last palpable rib and the top of the iliac crest. The body mass index (BMI) was calculated by dividing weight in kilograms by the square of height in meters.
Dietary assessment
A comprehensive data regarding dietary patterns were collected by an expert nutritionist, using a validated semi-quantitative food frequency questionnaire (FFQ). The FFQ is relatively easy and inexpensive to administer and can be used to measure dietary intake over a prolonged time period. 24 In this study, the FFQ contains a list of 98 food items; it was developed and validated among Palestinian population in 2014. 25 In our study, the method of dietary patterns assessment was published as in the previous study. 12 Furthermore, the major dietary patterns were obtained using factor analysis after the classification of food items into 25 groups (Table 1). The food grouping was based on the similarity of nutrient profiles and was somewhat similar to that used in previous studies.26,27
Food groupings used in the dietary pattern analysis.

Assessment of other variables
The socioeconomic, demographic, behavioral, and medical history data were collected through an interview-based questionnaire. Reports and all relevant documentation, including medical records, were also checked. Data about physical activity were obtained using the International Physical Activity Questionnaire (IPAQ short version). 28 The internationally accepted protocol was used to estimate the weekly calorie expenditure expressed as metabolic equivalents per week (MET/wk). 28 Pilot study was conducted on 15 patients to evaluate the tools of the study. Then, the tools of the study were modified according to the result of the pilot study.
Statistical analysis
All statistical analysis was performed using SPSS version 20. The major dietary patterns were obtained using factor analysis. Then, the obtained dietary patterns scores are expressed as tertiles. The chi-square test was used to determine the significant differences between different categorical variables. The differences between means were tested by independent-samples t test and one-way analysis of variance (ANOVA). Moreover, the odds ratio (OR) and confidence interval (CI) for the ACT across tertiles categories of dietary pattern scores were tested by binary logistic regression. P value less than 0.05 was considered as statistically significant.
Results
A total of 105 patients with asthma aged 19 to 64 years old (52.4% women, 47.6% men) were recruited in this study. The characteristics of the study population by sex are shown in Table 2. The results revealed that the mean age (years) for male patients was 41.90 ± 14 vs 46.21 ± 10 for females. In addition, for the following factors—age, educational level, employment history, history of smoking, multivitamin supplement use, height, BMI, and physical activity level—the difference was statistically significant in both sexes (P value < 0.05 for all). On the contrary, the results of ACT for the study population by sex are shown in Table 3. The collected data demonstrate that the mean total scores for ACT in male patients was 15.44 ± 4.1 vs 13.65 ± 3.6 for females. In addition, only 9.5% of the patients were classified as having well-controlled asthma (ACT scores: >19), while 90.5% of the patients were classified as having poorly controlled asthma (ACT scores: 19 or less), and the difference was statistically significant in both sexes (P value = 0.033). Furthermore, the food consumption data for the 25 food groups (Table 1) were entered into the SPSS for factor analysis. The scree plot of eigenvalues indicated 2 major patterns: (1) Prudent dietary pattern characterized by a high intake of whole grains, beans and legumes, fish and shellfish products, vegetables, tomatoes, fruits, and vegetable oils as well as a low intake of snacks and (2) Western dietary pattern characterized by a high intake of refined grains, red meat, poultry, fast foods, eggs, low-fat dairy product, high-fat dairy products, hydrogenated fats, olive, sugar, sweets, desserts, and snacks as well as a low intake of fish and shellfish products. The factor loading matrixes for major patterns are shown in Table 4. These 2 major dietary patterns explained 14.01% and 12.56% of the total variance, respectively. Then, the dietary pattern scores were classified as tertiles, and the characteristics of the study population were evaluated within the tertiles. Table 5 shows that patients in the lowest tertile (T1) of Prudent pattern were older (48.9 ± 12.7 vs 37.5 ± 10.8, P value < 0.001), 38.1% vs 18.1% were female (P value < 0.005), had a lower education level (52.8% vs 11.1%, P value < 0.05), had a high weight (kg) (83.5 ± 15.5 vs 78.5 ± 15.9, P value < 0.05), had a high WC (cm) (106.1 ± 13 vs 93.3 ± 15, P value < 0.005), and had a lower physical activity level (MET/wk) (1373 ± 1446 vs 2304 ± 1944, P value < 0.05), compared with those in the highest tertile (T3). On the contrary, only the distribution of patients regarding having a meal plan for asthma, who describe diet regimen, number of meal per day, and height (m) was significantly different across the tertiles of Western dietary pattern (P value < 0.05). Finally, the OR and CI for well-controlled asthma (ACT scores: >19) and poorly controlled asthma (ACT scores: 19 or less) across tertile categories of dietary pattern scores were computed (Table 6). Our findings revealed that, after adjustment for confounding variables, patients in the lowest tertile (T1) of Prudent dietary pattern had a lower odds for poorly controlled asthma (OR = 0.044, 95% CI = [0.002-1.316], P value < 0.05), while patients in the lowest tertile (T1) of Western dietary pattern had a higher odds for poorly controlled asthma (OR = 2.499, 95% CI = [1.288-4.850], P value < 0.05), compared with those in the highest tertile (T3). No significant associations were found between these 2 major dietary patterns with well-controlled asthma.
Characteristics of the study population by sex.

Abbreviations: BMI, body mass index; MET, metabolic equivalents.
Data are expressed as means ± SD for continuous variables and as percentage for categorical variables. The differences between means were tested by using independent-sample t test. The chi-square test was used to examine differences in the prevalence of different categorical variables. P value less than 0.05 was considered as statistically significant.
The asthma control test for the study population by sex.

Abbreviations: ACT, Asthma Control Test.
Data are expressed as means ± SD for continuous variables and as percentage for categorical variables. The differences between means were tested by using independent-sample t test. The chi-square test was used to examine differences in the prevalence of different categorical variable. P value less than 0.05 was considered as statistically significant.
Factor loading matrix for major dietary patterns.

Values less than 0.3 were omitted for simplicity. Total variance explained by 2 factors: 26.583.
Characteristics and dietary intakes of study population by tertile (T) categories of dietary pattern scores.
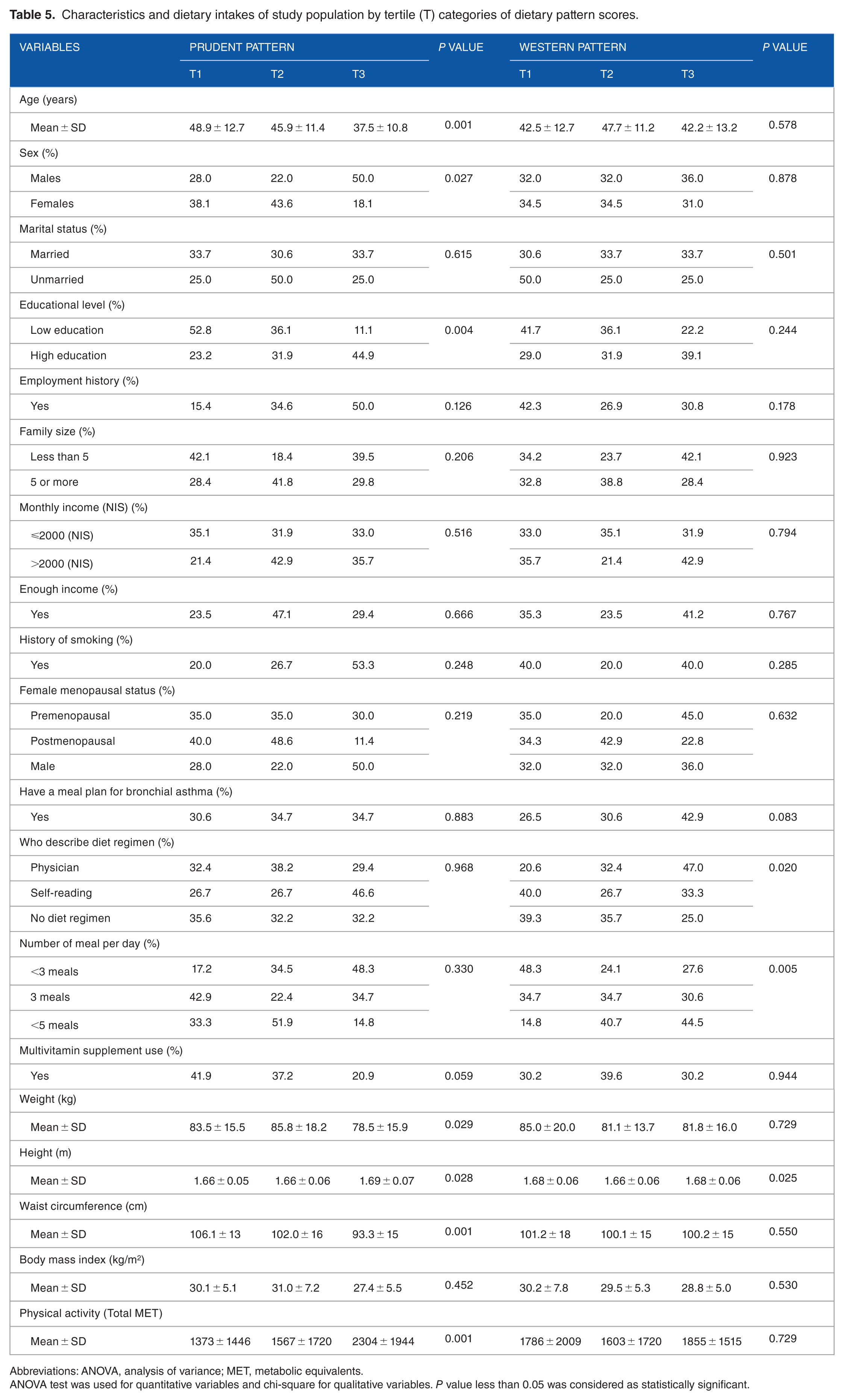
Abbreviations: ANOVA, analysis of variance; MET, metabolic equivalents.
ANOVA test was used for quantitative variables and chi-square for qualitative variables. P value less than 0.05 was considered as statistically significant.
Odds ratio and confidence interval for the asthma control test across tertile categories of dietary pattern scores.
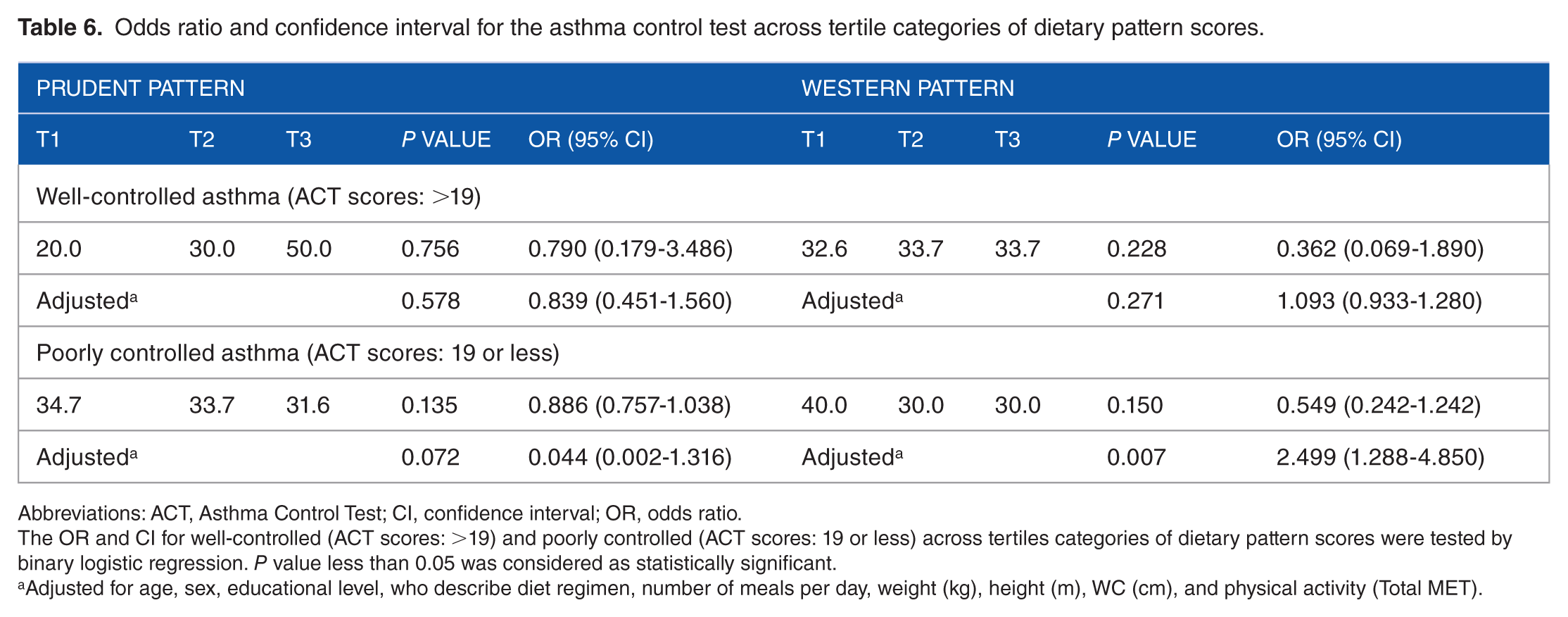
Abbreviations: ACT, Asthma Control Test; CI, confidence interval; OR, odds ratio.
The OR and CI for well-controlled (ACT scores: >19) and poorly controlled (ACT scores: 19 or less) across tertiles categories of dietary pattern scores were tested by binary logistic regression. P value less than 0.05 was considered as statistically significant.
Adjusted for age, sex, educational level, who describe diet regimen, number of meals per day, weight (kg), height (m), WC (cm), and physical activity (Total MET).
Discussion
Asthma is a common and potentially serious chronic disease that imposes a substantial burden on patients, their families, and the community. 1 Uncontrolled asthma is associated with decreased quality of life and increased health care system use. 9 Our study was conducted to determine the associations between major dietary patterns and the level of asthma control among patients with asthma at Al-Shifa Medical Complex in Gaza Strip, Palestine. To the best of our knowledge, this is the first study that examined this association among patients with asthma in Gaza Strip, Palestine. In our study, 105 patients with asthma (52.4% women, 47.6% men) were divided into 2 groups according to the results of ACT (poorly controlled asthma and well-controlled asthma). Our results revealed that only 9.5% of the patients had well-controlled asthma (ACT scores: >19), while 90.5% of the patients were classified as having poorly controlled asthma (ACT scores: 19 or less). Previous studies reported that poorly controlled asthma was found among a sizable percentage (40%) of US adults with asthma. 29 Lee et al 9 in a cross-sectional study show that, among patients with asthma, more than half of patients (54.4%) had very poor or not well-controlled asthma. In addition, Chapman et al 30 show that most (59%) of patients with asthma treated in general practice were uncontrolled. In our study, lack of asthma control can be due to a complex web of factors including genetics factors, types of asthma drugs, adherence, intrinsic factors, psychological factors, and environmental exposures, which could contribute to these results.
On the contrary, with the use of dietary data from the FFQ, 2 major dietary patterns were identified by factor analysis: (1) a Prudent dietary pattern characterized by a high intake of whole grains, beans and legumes, fish and shellfish products, vegetables, tomatoes, fruits, and vegetable oils as well as a low intake of snacks, and (2) a Western dietary pattern characterized by a high intake of refined grains, red meat, poultry, fast foods, eggs, low-fat dairy product, high-fat dairy products, hydrogenated fats, olive, sugar, sweets, desserts, and snacks as well as a low intake of fish and shellfish products. The main findings of this study indicate that, after adjustment for confounding variables, a Prudent dietary pattern may be associated with a lower prevalence of poorly controlled asthma, whereas a Western dietary pattern may be associated with a higher prevalence of poorly controlled asthma among patients with asthma in Gaza Strip, Palestine. In fact, studying the overall effect of dietary patterns on asthma control is an emerging literature; an overall approach based on dietary patterns could provide some insight into the combination of foods that might be beneficial or detrimental to asthma control. 31 In addition, very few population-based studies have been conducted to investigate the association between dietary patterns and the level of asthma control, which made the comparison of our results with previous studies difficult. Most studies have examined the associations between individual foods or food groups and nutrients and asthma outcomes.18-20 Poongadan et al in a cross-sectional study show an increased consumption of vegetables and cereals in patients with total controlled asthma in comparison with partially and poorly controlled asthma. In addition, the author revealed increased consumption of sugar, non-vegetarian, fast food, salted, and fried snacks in patients with poorly controlled asthma. 17 Garcia-Marcos et al 32 in a meta-analysis of 8 cross-sectional studies in children concluded that the Mediterranean diet might protect against asthma ever and current wheeze. Furthermore, a positive correlation exists between consumption of diet rich in vegetables and fresh fruits along with lifestyle habits as periodical exercise and good asthma control. 33 Iikura et al 33 in their study in Japanese population concluded raw vegetable intake (more than 5 units/wk) was significantly associated with good asthma control. The results of our study support these findings. Moreover, an association between dietary patterns and newly diagnosed chronic obstructive pulmonary disease was reported in a large cohort of men and women in the United States. 15 A Prudent dietary pattern characterized by a high intake of fruits, vegetables, fish, and whole grain products was associated with a decreased risk, whereas a Western pattern characterized by a high intake of refined grains, cured and red meats, desserts, and French fries was associated with an increased risk. 15 The results of our study support these findings. The previous dietary patterns are different from those obtained in our study. This can be explained by demographic, cultural, and ethnic differences, varying between countries, influencing behavior and attitudes regarding food choices.
In our study, the inverse association between Prudent dietary pattern with poorly controlled asthma could be attributed to pattern’s healthy ingredients including vitamins, dietary fibers, potassium, magnesium, and antioxidants. These nutrients have been independently associated with reduced risks of asthma exacerbation. 34 In addition, anti-inflammatory and antioxidant effects in these foods may have beneficial effects in alleviating inflammation and oxidative stress, which are pathogenic factors in asthma exacerbation. 35 Furthermore, vegetables, legumes, and fruits contain minerals, polyphenols, and other phytochemicals that combat oxidative stress and inflammation.36,37 In our study, the Prudent dietary pattern has been shown to be the healthiest dietary pattern and is quite close to that diet, which is generally recommended as a healthy dietary pattern with low animal foods, saturated fat, trans fat, cholesterol, and simple sugar, which may be associated with a higher risks of asthma exacerbation. 38 Our study is not adjusted for other confounding variables such as genetics factors, types of asthma drugs, adherence, intrinsic factors, psychological factors, and environmental exposures, which could contribute to these results. Actually, the relationship between dietary patterns with the level of asthma control needs more studies in the future.
The main limitation of this study is its cross-sectional design; the causal relationship could not be determined. Moreover, the possibility of recall bias and misreporting by using FFQ assessment of dietary patterns are other limitations. The main strength of our study was its being the first study, which identified the major dietary patterns and their association with the level of asthma control among patients with asthma in Gaza Strip, Palestine.
Conclusion
In conclusion, a Prudent dietary pattern may be associated with a lower prevalence of poorly controlled asthma, whereas a Western dietary pattern may be associated with a higher prevalence of poorly controlled asthma among patients with asthma in Gaza Strip, Palestine. Further future studies with large sample size are required to confirm these findings.
Footnotes
Acknowledgements
The authors wish to thank and appreciate the staff and participants in the chest department at Al-Shifa Medical Complex in Gaza Strip, Palestine, for their important participation in the study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AHB (Principal Investigator) collected, analyzed, and interpreted the data and wrote the first draft of the manuscript. AHB, AB, SH, and KD significantly contributed in the study design and the critical review of the manuscript. AHB and AB remarkably contributed in the analysis and interpretation of data and the critical review of the manuscript. All authors approved the final manuscript.
Ethical Approval
The study protocol was approved by the Ethics Committee of Al-Azhar University of Gaza and by the Palestinian Health Research Council (Helsinki Ethical Committee). Moreover, written informed consent was also obtained from each participant.