
Abstract
Background:
Unsafe abortion is a major contributor to maternal mortality in low- and middle-income countries. Despite the legalization of abortion and expanded access to services in Nepal, data on abortion practices and patient satisfaction remain limited.
Objective:
This study aimed to assess abortion methods, their management, and patient satisfaction among women seeking safe abortion services at a tertiary care hospital in Kathmandu, Nepal.
Design:
A hospital-based cross-sectional study.
Methods:
The study was conducted from December 2023 to May 2024 among 285 women aged ⩾18 years with gestational age of up to 12 weeks. Data were collected through face-to-face interviews and clinical records, followed by 7-day post-abortion assessment via in-person visits or phone calls. Pearson’s chi-square test and binary logistic regression were performed at a 5% level of significance to identify factor associated with patient satisfaction.
Result:
Among 285 women, 76.8% underwent medical abortion with oral mifepristone followed by misoprostol via sublingual, buccal, or vaginal routes, while 23.2% received surgical abortion through vacuum aspiration after misoprostol pre-treatment and local anesthesia. Discharge medications commonly included analgesics (paracetamol and ibuprofen) and antibiotics (ciprofloxacin, and metronidazole). Post-abortion contraceptive uptake was 79.3%, with implants (28.8%) and condoms (28.4%) being the most chosen methods. Overall, 50.2% of women reported satisfaction with the abortion services received. Logistic regression analysis showed that higher education (AOR: 5.63; 95% CI: 2.40-13.16), extended family structure (AOR: 7.25; 95% CI: 3.11-16.91), and no history of live birth (AOR: 4.20; 95% CI: 1.48-11.93) were significantly associated with higher satisfaction, while age ⩾35 years was negatively associated (AOR: 0.52; 95% CI: 0.28-0.95).
Conclusion:
Medical abortion was the preferred method, and overall management was aligned with WHO guidelines. However, patient satisfaction was moderate. Improving infrastructure, ensuring privacy, reducing waiting times, enhancing post-abortion counseling, and providing tailored health education with regular service evaluations are needed to improve the quality of abortion care and patient satisfaction.
Introduction
Each year, nearly 500 000 maternal deaths occur globally due to complications related to pregnancy and childbirth, with 95% of these deaths taking place in low- and middle-income countries (LMICs).1,2 Among various contributing factors such as hypertension, sepsis, unsafe abortion, postpartum hemorrhage, and other obstetric complications, the most significant in LMICs is unsafe abortion. 3 The World Health Organization (WHO) estimates that approximately 22 million unsafe abortions occur worldwide each year, accounting for 13% of maternal deaths in LMICs. 4
Abortion may be spontaneous or induced; the latter can be performed using medications such as mifepristone and misoprostol, or through surgical procedures like manual vacuum aspiration (MVA) and dilation and curettage (D&C). The method chosen depends on a woman’s health and preferences, gestational age, and clinical guidelines.5,6 Unsafe abortion can lead to severe complications, including hemorrhage, infection, ongoing pregnancy, uterine perforation, hysterectomy, and even death. 5
Access to high-quality abortion care is a fundamental reproductive right that supports women’s autonomy over their bodies and health, while also promoting patient satisfaction. Women’s satisfaction with abortion services is crucial, as it influences their willingness to seek timely care, adhere to treatment, and attend post-abortion follow-up appointments ultimately improving health outcomes for those experiencing abortion-related complications. 2 Satisfied women are more likely to comply with medical advice, return for future services, and recommend them to others. In contrast, low-quality services may lead women to seek unsafe abortions from unqualified providers, thereby increasing the risk of abortion-related morbidity and mortality. 6 Research indicates that multiple factors influence patient satisfaction, including the skill and expertise of healthcare providers, the quality of counseling and information provided, prior experiences, awareness of reproductive health, cultural and social context, emotional support, the legal environment, waiting times, and the assurance of privacy and confidentiality.7,8
In Nepal, abortion is reported to be the third most common cause of maternal death, accounting for approximately 7% of cases. 9 To ensure safe abortion and reduce maternal morbidity and mortality, abortion services were legalized in Nepal in 2002. By 2004, both public and private healthcare facilities across the country had begun providing surgical and medical abortion services. 10 Subsequently, free abortion services were introduced in government health facilities. Provisions such as the Public Health Service Act (2018), the Safe Motherhood and Reproductive Health Rights (SMRHR) Act (2018), and its corresponding regulation (2020) further established abortion as a fundamental right of women.11-13 Since legalization, Nepal has seen a substantial decline in maternal mortality, from 539 deaths per 100 000 live births in 1996 to 151 in 2021. 14 While this progress reflects the positive impact of policy advancements and improved access to reproductive healthcare, the current prevalence of maternal deaths directly attributable to abortion remains inadequately documented. Moreover, real-time data on abortion practices, including the methods used, their management, and patient satisfaction remain limited.
To enhance the quality of abortion care and address existing service delivery gaps, this study aimed to assess the methods used for abortion, their management, and patient satisfaction among women seeking safe abortion services at a tertiary care hospital in Nepal. Such an assessment not only helps identify areas for improvement but also contributes to the development of evidence-based clinical guidelines, informs health policy decisions, and promotes high-quality, patient-centered abortion services. This, in turn, contributes to the broader global objective of advancing reproductive health and reducing maternal mortality rates.
Methodology
Study Design, Setting, and Population
A hospital-based cross-sectional analytical study was conducted from December 2023 to May 2024 at the Safe Abortion Service Clinic of Paropakar Maternity and Women’s Hospital, Thapathali, Kathmandu. 15 This tertiary central government hospital is the largest maternity hospital in Kathmandu in terms of the number of deliveries and abortions. It is one of the pioneers and continues to be the leading provider of safe abortion services in Nepal.
Participant recruitment took place during the clients’ routine visit to the Safe Abortion Service Clinic. After the women completed their registration and clinical screening, the counseling nurse provided standard pre-abortion counseling as part of routine care. Following the counseling session, eligible women were informed about the study by the same counseling nurse and invited to participate. Those who expressed interest were referred to a researcher, who explained the study’s purpose, procedures, risks, and benefits in detail and obtained written informed consent. Recruitment was conducted prior to the abortion procedure to ensure that participation did not interfere with clinical care. Participation was voluntary, and refusal to participate did not affect the services received. The study was conducted independently of the hospital’s routine abortion process, with coordination from clinical staff to maintain privacy and minimize disruption to patient flow.
Women’s aged ⩾18 years old and with gestational age up to 12 weeks (1st trimester) were included in the study, as shown in Figure 1.
Sample Enrollment Process

Sample enrollment.
Sample Size and Sampling Technique
The sample size for the study was determined using the Cochrane formula (Cochran, 1963), based on the prevalence of abortion among women of reproductive age in Nepal, which is 21.1%. 9 The formula used was n = z2 × p × q/d2, where n is the desired sample size, z is the standard normal deviate (1.96 for a 95% confidence level), p is 0.21 (prevalence rate), q is 0.79 (1 − p), and d is 0.05 (desired accuracy). Substituting these values, the calculated sample size was 255. To account for a 10% non-response rate, the total adjusted sample size was 280.4~285. Convenience sampling technique was used for the study.
Data Collection and Measurements
A face-to-face interview was conducted in the counseling room using a semi-structured questionnaire, while clinical information was retrieved from the Kardex. A follow-up was carried out 7 days of post-abortion, with in-person (65%) assessments for participants who returned to the hospital. Those who did not return were contacted via telephone (35%) to identify any complications they may have experienced (Supplemental Material).
The data collection tool was developed by reviewing similar previously published articles2,16-18 and consists of four sections. Section 1 covers baseline characteristics, including age, marital status, religion, ethnicity, education, occupation, monthly family income, type of family, one-way travel time from residence to hospital, and clinical details such as the number of live births, previous abortion history, gestational age (in weeks), cesarean section history, ectopic pregnancy history, underlying medical conditions. Section 2 includes details related to abortion, such as the type of abortion, reasons for abortion, methods used, and associated side effects. Section 3 focuses on abortion-related complications, including the prevalence of complications, types of complications observed, and their management. Section 4 assesses patient satisfaction with service providers based on factors such as greeting, cooperation, adequacy of information provided, discrimination, confidentiality, privacy, respect, information about the procedure, pain management, necessary advice, waiting room conditions, cleanliness of the service area, opportunity to ask questions, provider’s experience, and waiting time. Responses were coded 1 for yes and 0 for no. To obtain a total score, the individual item scores were summed, resulting in a cumulative score ranging from 0 to 15. The score was then categorized as “Satisfied” (scores of 10 and above) and “Dissatisfied” (scores below 10). This dichotomized patient satisfaction variable was used in a binary logistic regression model. A pretest of the tool was conducted among 10% of the total sample population (n = 28) in a hospital with a similar setting. The questionnaire demonstrated strong internal consistency, with a Cronbach’s alpha of .89.
Statistical Analysis
The collected data was entered into Epi-Data 3.1 and exported to SAS version 9.4 for statistical analysis. 19 Descriptive statistics, such as frequencies and percentages were computed. Bivariate analyses were conducted for categorical variables. Variables found to be significant in the bivariate analysis were included in the binary logistic regression model to determine the measures of association, expressed as odds ratios (ORs) with 95% confidence intervals (CIs). The variance inflation factor (VIF) test was performed among selected independent variables to be subjective to the regression model to manage the issue of multicollinearity. Statistical significance was determined using a P-value threshold of <.05.
Ethical Approval
Ethical approval was obtained from the Institutional Review Committee of the Paropakar Maternity and Women’s Hospital (Ref No: 64/762). Data privacy was ensured through coding, keeping participants’ names confidential. Their information remained secure and was used solely for research. Participation was voluntary, with the option to withdraw at any time without risk.
Results
Baseline Characteristics
Table 1 presents an overview of the study participants and factors associated with method of abortion and patient satisfaction. Out of 285 participants, the majority were aged 18 to 35 years (80.4%) and married (94%). Most identified as Hindu (89.1%), had attained higher education (40.7%), and were homemakers (67.4%). Nuclear families were predominant (84.2%). Approximately half of the participants (49.1%) had a monthly family income below NPR 25 000, and 88.4% reached the hospital within an hour. Most (95.4%) reported having family support.
Baseline Characteristics and Bivariate Analyses by Abortion Method and Patients’ Satisfaction (n = 285).

Regarding clinical characteristics, 73.3% sought abortion between 7 and 9 weeks of gestation, and 69.8% had at least one child. The majority had no prior abortion history (66.3%), had not used contraceptive methods (90.9%), and had no comorbidities (89.8%). Most abortions were induced (92.6%), and medical abortion was the predominant method (76.8%). Unwanted pregnancy (52.2%) was the leading reason for seeking abortion.
Bivariate Analysis of Baseline Characteristics Associated with Abortion Method and Patient Satisfaction
Medical abortion was significantly more frequent among those with gestational age between 7 and 9 weeks (P < .01), and less frequent among those with prior cesarean history (P < .01). Patient satisfaction, reported by 50.2%, was significantly associated with age (P < .05), educational level (P < .01), occupation (P < .01), type of family (P < .01), monthly income (P < .05), parity (P < .01), CS history (P < .05), and reason for abortion (P < .01).
Self-Medication Practices
Table 2 shows that only 5.3% of participants had self-administered the MTP Kit prior to seeking medical care. Among these individuals, the primary reason reported was concern for privacy (80.0%), followed by financial constraints (20.0%).
Self-Medication Practice Prior to Abortion (n = 285).

Abbreviation: MTP, mifepristone and misoprostol.
Abortion Medication Regimens
Table 3 presents the pattern of medication regimen for abortion. For medical abortion, mifepristone 200 mg was administered orally, followed by misoprostol 800 mcg via sublingual, buccal, or vaginal route after 24 hours. For surgical abortion, patients received pre-procedural medications including metronidazole to prevent infection, PCM + Ibuprofen for pain relief, and misoprostol for cervical ripening prior to manual vacuum aspiration. Discharge medications for surgical abortion included a 5-day course of ciprofloxacin, metronidazole, PCM and pantoprazole.
Medication Regimens for Abortion.
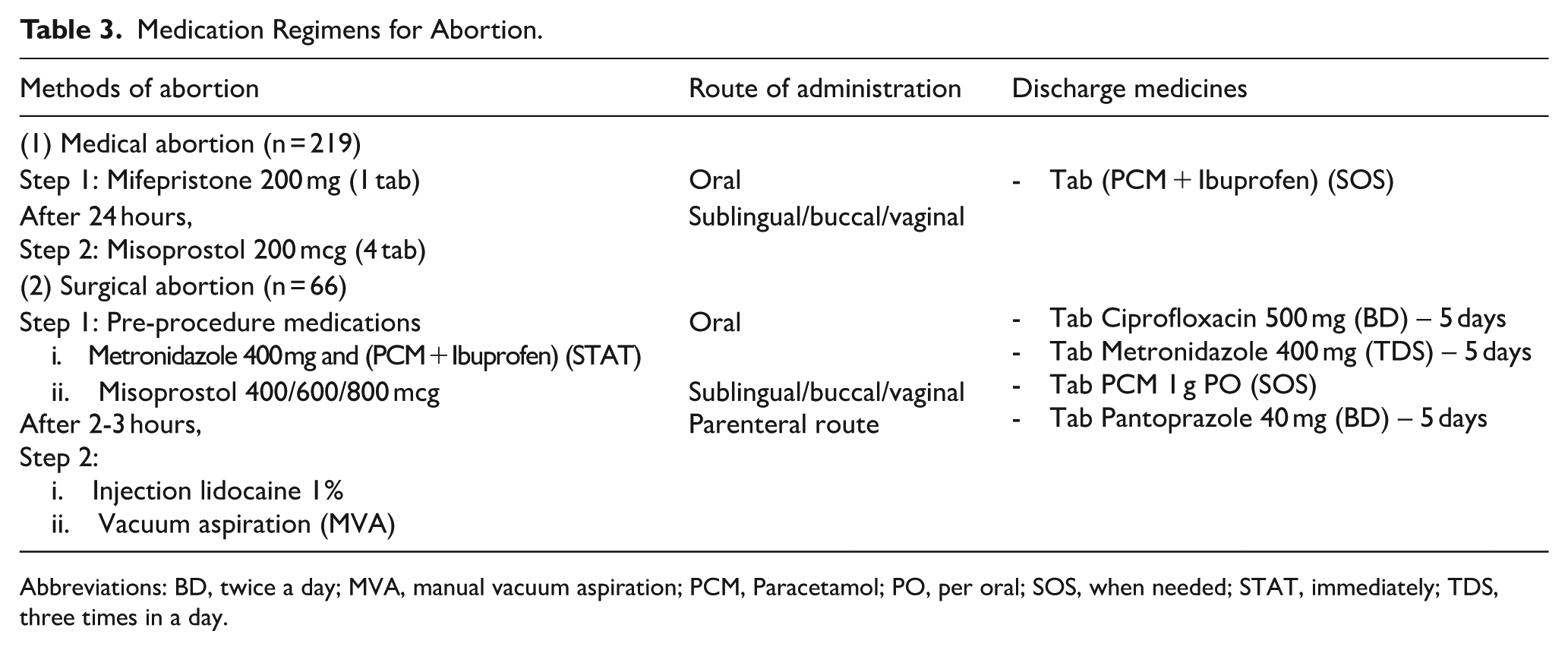
Abbreviations: BD, twice a day; MVA, manual vacuum aspiration; PCM, Paracetamol; PO, per oral; SOS, when needed; STAT, immediately; TDS, three times in a day.
Side Effects and Complications Following Abortion Procedures
Table 4 presents the incidence of side effects and abortion-related complications among women undergoing medical or surgical abortion. A total of 61.75% of women experienced side effects with vomiting being the most reported one (43.1%), followed by headache (30.1%), diarrhea (19.8%), and fever (18.1%). Vomiting and diarrhea were predominantly associated with medical abortion. Complications were reported in 15.4% of cases, with incomplete abortion being the most common (86.3%). This occurred more frequently among medical abortion users (68.18%). Bleeding (11.36%) and infections (2.27%) were less common, with bleeding more common in surgical procedures (80.0%).
Incidence of Side Effects and Complications in Medical and Surgical Abortion (n = 176).

Multiple response.
Management of Complications
Table 5 presents the management of abortion-related complications. Incomplete abortions were primarily managed using ciprofloxacin (60.5%) and metronidazole (39.4%). Infections were treated with a combination of clotrimazole and metronidazole. Bleeding was managed using tranexamic acid (40.0%), IV fluids (40.0%), and in one case, blood transfusion (20.0%). Pain relief was managed through injectable and oral analgesics such as lidocaine (7.8%), fentanyl (2.6%), ketorolac (20.0%), and PCM + Ibuprofen (35.21%).
Management of Abortion-Related Complications (n = 44).

Post-Abortion Contraceptive Choices
Table 6 presents the contraceptive choices of women after abortion. Most participants (79.3%) opted for post-abortion contraception. Implants (28.8%) and condoms (28.4%) were the most chosen methods. Younger women (<35 years) preferred implants (29.7%), while condoms were more common among those ⩾35 years (26.8%). Married women primarily selected implants (30.6%), whereas most unmarried participants did not choose any contraception (88.2%). Higher educated (37.1%) and employed (34.7%) women showed a preference for condoms (37.1%), while homemakers favored implants (28%). Women with Furthermore, participants with more than two children favored implants (39.5%), while those with no children often chose not to use any contraceptive method (48.8%).
Post-Abortion Contraceptive Choices (n = 285).

Patient Satisfaction with Abortion Services
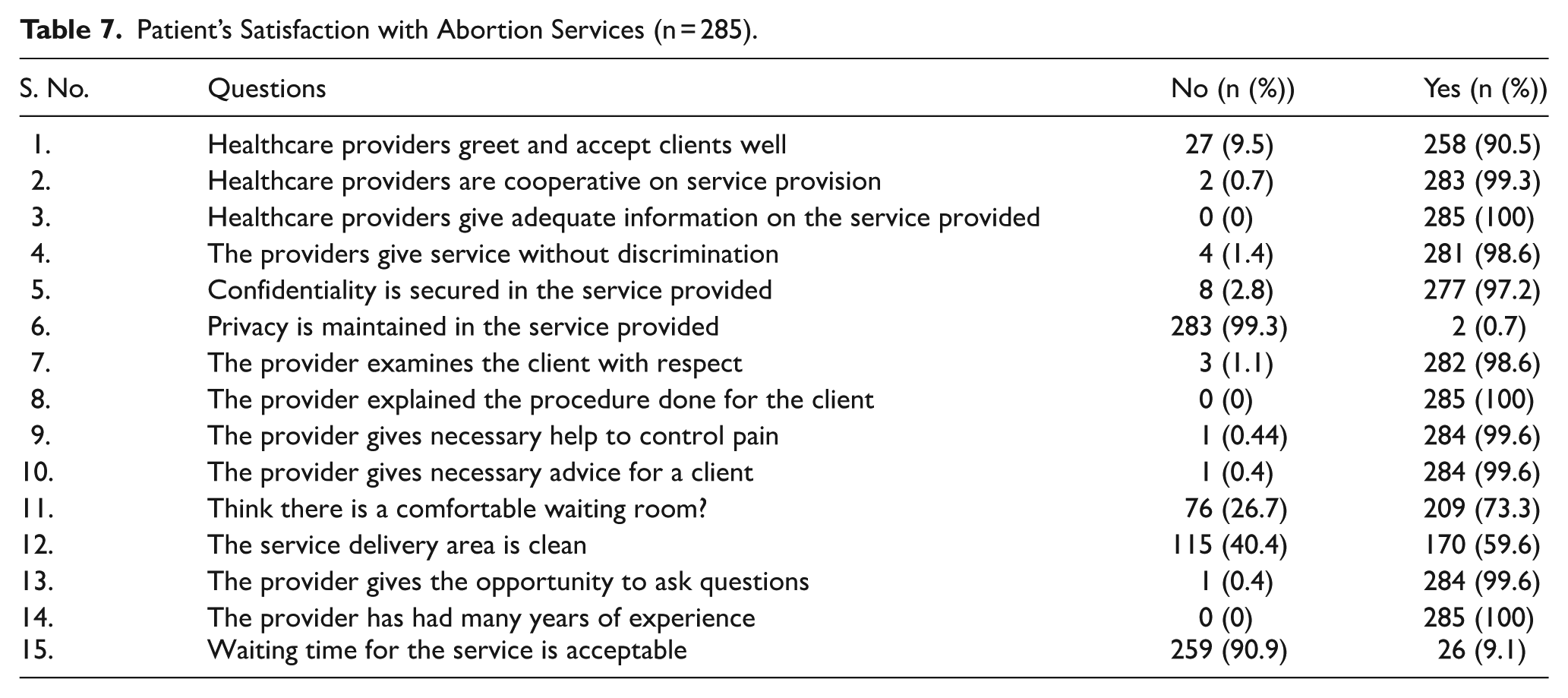
Table 7 summarizes patients’ satisfaction with the healthcare services received during abortion care. Most participants (90.5%) reported being greeted by healthcare providers, 99.3% felt that the providers were cooperative, and 100% confirmed receiving adequate information about the procedure. A similarly high proportion reported receiving services without discrimination (98.6%) and with confidentiality maintained (97.2%). However, 99.3% of participants reported lack of privacy, 40.4% perceived the service area as unclean, and 90.9% indicated that the waiting time was long. Despite these concerns, 98.6% stated they were examined with respect, and nearly all participants were satisfied with pain management and communication with their providers. Around three-quarters (73.3%) found the waiting area comfortable, and all respondents (100%) believed their provider possessed many years of experience.
Patient’s Satisfaction with Abortion Services (n = 285).
Factor Associated with Patients Satisfaction
Table 8 presents the results of the binary logistic regression analysis identifying factors associated with patient satisfaction with abortion care services. Variables included in the final model were assessed for multicollinearity, with all Variance Inflation Factor (VIF) values falling within acceptable limits, the highest being 2.41, indicating no significant multicollinearity concerns.
Adjusted Odds Ratio of Factors Associated with Patients Satisfaction (n = 285).

P-value < .05; Ref.: Reference; AOR: Adjusted odd ratio..
The analysis revealed that women aged ⩾35 years had significantly lower odds of being satisfied with the services compared to those under 35, with a 48% reduction in the likelihood of satisfaction (AOR: 0.52; 95% CI: 0.28-0.95; P < .05). Conversely, participants with higher secondary education or above were over five times more likely to report satisfaction than those who were illiterate (AOR: 5.63; 95% CI: 2.40-13.16; P < .01). Similarly, women from extended families were seven times more likely to be satisfied compared to those from nuclear families (AOR: 7.25; 95% CI: 3.11-16.91; P < .01). Participants with no live births had significantly higher odds of satisfaction compared to those with more than two births (AOR: 4.20; 95% CI: 1.48-11.93; P < .01).
Discussion
Abortion remains a crucial component of reproductive healthcare, with safe abortion services significantly reducing maternal morbidity and mortality worldwide. 20 This study assessed the abortion methods employed, their management, and patient satisfaction among women seeking safe abortion services at a specific hospital in Nepal over a 6-month period. Induced medical abortion was the most common method used by participants to terminate their unwanted pregnancies. This finding aligns with previous studies that reported a high preference for medical abortion, primarily due to its noninvasive nature and the desire to avoid the pain and discomfort associated with surgical procedures.2,6,21 Increased awareness and education about medical abortion, along with fewer physical complications and a lower risk of infection, may also contribute to its growing preference and utilization. Similarly, a study conducted in another region of Nepal found that 46% of women sought abortion services primarily to avoid having an unwanted child. 9
The management approach for abortion and its complications followed the World Health Organization (WHO) abortion care guidelines, where mifepristone followed by misoprostol is the primary regimen recommended for induced abortion. Misoprostol is also recommended for managing incomplete abortion. In addition, antibiotics are recommended as prophylactic agents for both medical and surgical abortions, and NSAIDs (paracetamol, ibuprofen) are used for pain management, including as pre-procedure medications. The guidelines also suggest offering contraceptive methods immediately after medical or surgical abortion, including combined hormonal contraceptives (oral contraceptives, contraceptive patch, vaginal ring, and injectable contraceptives), progesterone-only contraceptives (progesterone-only pills, levonorgestrel or etonogestrel implants, depot medroxyprogesterone acetate injectables), barrier methods (condoms, spermicide, diaphragm), and copper-bearing intrauterine devices (Cu-IUDs). 20 In this study, the choice of post-abortion contraception was influenced by factors such as age, marital status, education, occupation, and number of live births.
Half of the women using abortion services reported satisfaction with the care provided. This finding is consistent with a study in Ethiopia, where 56% of women were satisfied. 3 However, the level of satisfaction observed here is lower than that reported in India (90.0%) and Guinea (92.6%),22,23 but higher than in northwest Ethiopia (25.1%) 18 and Tigray (40.6%). 24 These variations may be explained by differences in study duration, population characteristics, geographical location, healthcare providers’ attitudes and skills, sociocultural context, adherence to clinical protocols, and availability of appropriate equipment.3,6
Women aged ⩾35 years, those with higher secondary education or above, those belonging to extended families, and those with no live births were more likely to be satisfied with abortion care services. In contrast, a previous study found that women aged 20 to 24 years had 2.94 times higher odds (AOR: 2.94; 95% CI: 1.02-8.48) of being satisfied. 6 Older women may have greater exposure to healthcare services, enhancing their understanding of medical procedures and increasing satisfaction. Younger women, on the other hand, may focus more on avoiding social stigma and on pregnancy termination itself rather than on the quality of care. Another study showed that women with a college education or above were 73% (AOR: 0.27; 95% CI: 0.14, 0.95) less likely to be satisfied compared to those who were illiterate. 2 Highly educated women may be better able to articulate their needs, expect more individualized care, and have higher standards regarding quality. They are also better informed about their health and can communicate more effectively with their providers. 17 Similarly, another study from Ethiopia reported that women living in smaller households (alone or with 2-3 members) were 53% to 89% less likely to be satisfied compared to those living with more than five family members. 17
This suggests that women from smaller families may have limited access to information on healthcare services, including the safety of abortion. Furthermore, women with prior live births may have higher expectations regarding the quality of abortion services, potentially leading to lower satisfaction. However, this contradicts a study which found that women who wanted to have a baby were 56% less likely to be satisfied with abortion services compared to their counterparts. 17
Strength and Limitations
This study is likely the first of its kind to provide valuable insights into abortion methods, their management, and women’s satisfaction with abortion care services in a tertiary care setting. However, several limitations should be acknowledged. First, as a single-center study, the findings may not be generalizable to other healthcare settings. Second, the use of convenience sampling may not fully represent the broader population of women seeking abortion services in Nepal. Third, the 7-day post-abortion follow-up may not capture long-term satisfaction or complications. Additionally, self-reported responses may be influenced by recall or social desirability bias. Finally, the focus on first-trimester abortions limits the applicability of the findings to women undergoing second-trimester procedures.
Conclusion
The study highlighted medical abortion as the preferred method, with its management aligning with WHO guidelines. Satisfaction with abortion care services was reported by half of the participants and was influenced by factors such as age, education level, family type, and number of live births. The findings underscore the need to strengthen infrastructure, ensure privacy, reduce waiting times, and enhance post-abortion counseling. Furthermore, tailored educational initiatives and regular service evaluations are essential to improve patient-centered abortion care and overall satisfaction.
Supplemental Material
sj-docx-1-his-10.1177_11786329251406022 – Supplemental material for Assessment of Abortion Methods, Management, and Patient Satisfaction Among Women Seeking Safe Abortion Services in a Tertiary Care Hospital, Nepal
Supplemental material, sj-docx-1-his-10.1177_11786329251406022 for Assessment of Abortion Methods, Management, and Patient Satisfaction Among Women Seeking Safe Abortion Services in a Tertiary Care Hospital, Nepal by Sonika Thapa, Nirmal Raj Marasine, Shishir Paudel, Sagun Thapa, Sabina Sankhi and Prayas Ghimire in Health Services Insights
Footnotes
Acknowledgements
The authors would like to acknowledge the CiST College for providing opportunities to conduct this study, and nursing staff of the comprehensive care center (CAC) of Paropakar Maternity and Women’s Hospital who helped me immensely during the collection of data required for this study and participants for participating in this study
Abbreviations
ANM: Auxiliary nurse and midwife
BMI: Body mass index
CS: Cesarean section
IRC: Institutional Review Committee
IUCD: Intrauterine contraceptive device
MA: Medicinal abortion
MVA: Manual vacuum aspiration
OCP: Oral contraceptives pills
PMWH: Paropakar Maternity and Women’s Hospital
RPOC: Retained product of conception
SBA: Skilled birth attendant
WHO: World Health Organization
Ethical Considerations
Ethical approval was obtained from the Institutional Review Committee (IRC) of the Paropakar Maternity and Women’s Hospital (Ref No: 64/762), the study followed the Helsinki Ethical Guidelines.
Consent to Participate
Written informed consent was obtained from the patients.
Author Contributions
SoT: Conceptualization, methodology, data curation, project administration, resources, writing – review and editing; NRM: Conceptualization, methodology, validation, formal analysis, visualization, validation, project administration, resources, writing – original draft, writing – review and editing; ST and SP: Writing – review and editing; PG: supervision; SS: methodology, formal analysis, validation, writing – original draft, writing – review and editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data used to support the findings of this study are made available from the corresponding author upon reasonable request
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.