
Abstract
Background:
Stroke is a leading cause of long-term disability, significantly impacting health-related quality of life (HRQoL). However, evidence from Nepal remains limited.
Objective:
This study aimed to assess HRQoL and identify its associated factors among stroke patients in a tertiary care hospital in Nepal.
Design:
Cross-sectional study
Methods:
This study was conducted at the Annapurna Neurological Institute and Allied Sciences (ANIAS) between November 2023 and April 2024 among 120 stroke patients aged ⩾18 years. Baseline data were collected using a semi-structured questionnaire, and HRQoL was assessed using the EuroQol 5-Dimension 5-Level (EQ-5D-5L) scale. Statistical analyses included descriptive statistics, bivariate analyses, and multiple linear regression to identify factors associated with HRQoL. A p-value < .05 was considered statistically significant.
Results:
The mean HRQoL score was 21.13 ± 6.62, indicating substantial impairment, particularly in usual activities (Mean ± SD: 4.32 ± 1.32), self-care (4.26 ± 1.34), and mobility (4.22 ± 1.32). Lower HRQoL was significantly associated with older age, unemployment, lower educational attainment, and moderate to severe stroke-related disability (p< .001). Strong positive correlations were observed among all five HRQoL domains.
Conclusion:
HRQoL is significantly impacted by stroke, with major impairments in usual activities, self-care, and mobility, influenced by both socio-demographic and clinical factors. Implementing targeted, multidimensional rehabilitation strategies such as structured physiotherapy is essential to enhance recovery and improve the quality of life in this population.
Introduction
Stroke is a major global health challenge and remains one of the leading causes of death and long-term disability worldwide.1,2 According to the Global Burden of Disease (GBD) Report 2019, stroke ranks as the second leading cause of mortality and the third leading contributor to disability globally. That year, approximately 12.2 million new stroke cases, 101 million prevalent cases, 143 million disability-adjusted life years (DALYs), and 6.55 million stroke-related deaths were reported. 3 Alarmingly, the global prevalence of stroke is projected to increase significantly, reaching an estimated 21.9% by 2030. 4 Among its types, ischemic stroke is the most commonly observed. Lacunar stroke is the predominant subtype, accounting for 58.6% of cases, followed by large artery atherosclerotic (LAA) stroke and cardioembolic stroke, each comprising 20.7% of cases. 5
Approximately 80% of stroke-related deaths occur in low- and middle-income countries (LMICs), where limited healthcare infrastructure and resources create substantial barriers to effective stroke management and rehabilitation. 6 In Nepal, the estimated annual prevalence is 117 stroke cases per 100,000 population, translating to approximately 33,000 new cases each year. 7 Contributing factors, including a lack of comprehensive epidemiological data, low public awareness, and limited access to specialized care and rehabilitation services account for 13% to 29% of the country’s stroke-related mortality.8,9
While the majority of strokes in Nepal are ischemic, caused by blockage of cerebral blood vessels, nearly one-third are hemorrhagic, resulting from intracranial bleeding. 3 Stroke, as one of the most disabling chronic conditions, impairs not only physical health but also has profound psychological, social, and economic consequences. These impacts significantly reduce the health-related quality of life (HRQoL) among survivors. 10 Physical and cognitive impairments, such as limited mobility and post-stroke depression, along with increased prevalence of anxiety, emotional distress, and social withdrawal, further exacerbate the decline in HRQoL.11,12
Despite the rising burden of stroke in Nepal, there is a dearth of studies on HRQoL among stroke patients. Previous studies have identified a range of factors associated with HRQoL, including demographic variables such as age, gender, education, and income, clinical characteristics like stroke severity, side of lesion, degree of disability, comorbidities such as diabetes, hypertension, dyslipidemia, and psychosocial determinants like social support and depression.13 -15 However, findings from international studies may not be directly generalizable to the Nepali context due to differences in cultural, socioeconomic conditions, and the healthcare system.
Therefore, this study aims to assess HRQoL and its associated factors among stroke patients receiving care at a tertiary care hospital in Nepal. By addressing this critical gap in the literature, the study seeks to support the development of policy recommendations and provides actionable insights for clinicians and healthcare policymakers. Ultimately, these efforts are vital for strengthening stroke care and rehabilitation services in resource-limited settings, thereby reducing the national burden of stroke and improving patient outcomes.
Methods
Study Design and Setting
A hospital-based cross-sectional study was conducted among stroke patients at the Annapurna Neurological Institute and Allied Sciences (ANIAS), 16 Maitighar, Kathmandu, Nepal, from November 2023 to April 2024. ANIAS is a 100-bed tertiary care hospital that provides regular neurology outpatient and inpatient services, emergency care, and various super-specialization programs, ensuring health and well-being through evidence-based healthcare services.
Selection Criteria
All patients of either gender aged ⩾18 years with a confirmed diagnosis of stroke (radiological evidence from a CT scan and/or MRI), and an identified primary caregiver aged above 18 years, were included during their inpatient stay. Patients who were unable to communicate directly (such as those with dementia or aphasia), unwilling to participate, uncooperative, or diagnosed with terminal illnesses such as end-stage cancer or renal failure were excluded from the study.
Sample Size and Sampling Procedure
According to the hospital administration, an average of 50 stroke patients is admitted monthly. With a data collection period of 3 months, a total of 150 stroke patients were included in the study population. Using Yamane’s formula for sample size calculation with a finite population, the sample size was determined as follows: n = N/(1 + N × e²), where N represents the total population (150), and e is the margin of error (0.05). The calculation yielded n = 150/(1 + 150 × (0.05) 2 ) = 150/(1 + 150 × 0.0025) = 150/1.375 ≈ 109.09. To account for a 10% non-response rate, the final required sample size for the study was adjusted to 120 patients. A convenience sampling technique was used to select the participants for the study.
Data Collection
A semi-structured questionnaire was used for data collection. Patients were identified by reviewing the Kardex, and their inclusion was verified through communication with nurses and doctors. The Kardex is a tool that provides concise access to patient information, including demographic details, diagnosis, medications, health status, treatment schedules, activities, and care plans. 17
Data on sociodemographic characteristics, disability, and health-related quality of life were collected through face-to-face interviews conducted during the hospital stay, lasting 10-15 minutes in a comfortable setting. Clinical information was collected by reviewing the Kardex and consulting with healthcare providers. All collected data were stored securely to maintain patient privacy and confidentiality. The questionnaires used in the interviews were initially translated from English to Nepali and then verified via back-translation to ensure accuracy. All interviews were conducted in the Nepali language. Pretesting of the questionnaire was conducted with 10% of the intended sample (ie, 12 participants) in a similar setting. The internal consistency of the questionnaire, assessed using Cronbach’s alpha, was 0.87.
Outcome Measurement
The primary measure was HRQoL, assessed using the EuroQol 5-Dimension 5-Level (EQ-5D-5L) scale. 18 The EQ-5D-5L consists of 25 items (rated from 1 = best condition to 5 = worst condition) across five domains: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression. In this study, a cumulative score ranging from 5 to 25 was calculated. Higher EQ-5D-5L scores indicate poorer health status, reflecting greater difficulty in daily activities, higher levels of pain, or emotional distress. Conversely, lower scores indicate better health with fewer or no problems.
Explanatory Variables
The degree of disability was assessed using the Modified Rankin Scale (mRS), which was developed and validated by John van Swieten. The mRS scores range from 0 to 6 and are categorized as follows: 0 (no symptoms), 1 (no significant disability), 2 (slight disability), 3 (moderate disability), 4 (moderately severe disability), 5 (severe disability), and 6 (death). Higher scores indicate greater neurological impairment or a higher degree of physical disability. 19 For analysis purposes, a score of ⩽2 was categorized as mild disability, while a score of ⩾3 was considered moderate to severe disability. Additional variables included age, gender, marital status, (ever married/never married), occupation, education level, religion, ethnicity, family type, family history of stroke, smoking and alcohol consumption, type of stroke, infarcted area, and the presence of co-morbidities.
Statistical Analysis
Data were entered into EpiData version 3.1 and exported to SAS version 9.4 for analysis. Descriptive statistics, including means with standard deviations for continuous variables and frequencies with percentages for categorical variables, were calculated based on the level of measurement. The normality of the data was assessed using the Kolmogorov-Smirnov test.
For bivariate analysis, independent sample t-tests and one-way ANOVA tests were performed to evaluate the association between categorical variables and HRQoL. Independent sample t-tests were used for dichotomous variables such as gender, marital status, family type, co-morbidities, type of stroke, and stroke-related disability. One-way ANOVA tests were applied to multi-category variables including age, education level, occupation, ethnicity, religion, smoking and alcohol consumption, and infarcted areas.
Multiple linear regression analyses were conducted using both unadjusted and adjusted models to identify factors associated with HRQoL. The assumptions of linearity, normality, and homoscedasticity were evaluated using residual scatterplots. The normal probability plot of standardized residuals indicated an approximately normal distribution, and the scatterplot of residuals versus predicted values showed no evident pattern, supporting the assumptions of linearity and equal variance. Additionally, the Variance Inflation Factor (VIF) values for all predictors were below 10, indicating no significant multicollinearity. 20 A Pearson correlation matrix was computed to assess the relationships between the overall HRQoL score and its five domains (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). Statistical significance was determined at a p-value of <.05.
Ethical Approval
The study was approved by the Institutional Review Committee of Annapurna Neurological Institute & Allied Sciences (IRC-ANIAS, Ref No.: 115-2023/24). Participant privacy was protected through data coding, and names were not disclosed to third parties. Confidentiality was maintained throughout the study, and the collected data were used solely for research purposes. Participation was voluntary, and participants could withdraw at any time without consequence. They were informed of the study objectives and had access to their information after data collection.
Results
The characteristics of the participants and the bivariate analyses by HRQoL scores are presented in Table 1. Of the 120 stroke patients, most were aged between 61 and 80 years (47.5%), male (65.0%), and employed (30.0%). Ethnically, Janajati constituted the largest group (45.0%). Nearly half of the patients were illiterate (44.2%), and the majority were Hindu (83.3%). The vast majority were married (98.3%) and belonged to a joint family (55.0%).
Socio-Clinical Characteristics and Bivariate Analyses by HRQoL Score.

Abbreviations: COPD, chronic obstructive pulmonary disease; Ever married: married, divorced, separated; mRS, Modified Rankin Scale.
One way ANOVA.
Kolmogorov-Smirnov test.
Independent t-test.
P-value < .05.
Assessment of co-morbid conditions showed that hypertension was highly prevalent, affecting more than three-fourths of the patients (78.3%), while diabetes mellitus was present in (23.3%). Regarding social history, nearly half of the patients had never smoked (48.3%) or consumed alcohol (45.0%), while a small proportion were former smokers and alcohol users (6.7%).
Bivariate analyses revealed several significant associations between various factors and HRQoL among stroke patients. HRQoL scores varied notably across age groups, educational levels, occupational status, family type, and the presence of specific comorbidities such as hypertension, dyslipidemia, and COPD. Additionally, stroke-related disability and infarcted brain areas were significantly associated with HRQoL. Conversely, no statistically significant associations were observed between HRQoL and gender, ethnicity, marital status, smoking history, alcohol consumption, or the type of stroke.
Table 2 presents the distribution of responses across the five domains of the EQ-5D-5L among stroke patients. The highest level of impairment was observed in the domain of usual activities (mean ± SD: 4.32 ± 1.32), followed closely by self-care (4.26 ± 1.34), and mobility (4.22 ± 1.32). Comparable levels of impairment were reported in the pain/discomfort and anxiety/depression domains, with mean scores of 4.17 ± 1.51 and 4.17 ± 1.53, respectively. The overall EQ-5D-5L summary score had a mean ± SD of 21.13 ± 6.62, indicating a substantial impact on patients HRQoL.
Distribution of EQ-5D-5L Dimension Responses Among Stroke Patients (n = 120).

Abbreviation: SD, standard deviation.
Table 3 illustrates the association between socio-clinical factors and HRQoL among stroke patients, based on both unadjusted and adjusted analyses. The adjusted analysis revealed that the HRQoL scores were significantly higher among patients aged 41 to 60 years (β = 7.202; 95% CI: 3.623 to 10.781; P < .001), 61 to 80 years (β = 6.954; 95% CI: 3.470 to 10.439; P < .001), and over 80 years (β = 10.360; 95% CI: 2.714 to 18.006; P < .001), compared to those aged 20 to 40 years. Similarly, being unemployed (β = 3.136; 95% CI: 0.085 to 6.188; P = .004), retired (β = 4.348; 95% CI: −0.131 to 8.27; P = .005), or involved in agriculture (β = 5.100; 95% CI: 1.330 to 8.887; P = .008) was linked with higher HRQoL scores than being employed. Interestingly, educational level exhibited inverse association with HRQoL. Participants with higher secondary (β = −3.391; 95% CI: −7.023 to −0.240; P = .006), graduate (β = −4.852; 95% CI: −8.561 to −1.143; P = .001), and postgraduate education (β = −11.983; 95% CI: −18.221 to −5.744; P = .001) showed significantly lower HRQoL scores compared to illiterate individuals.
Socio-Clinical Factors Associated with HRQoL Among Stroke Patients (n = 120).
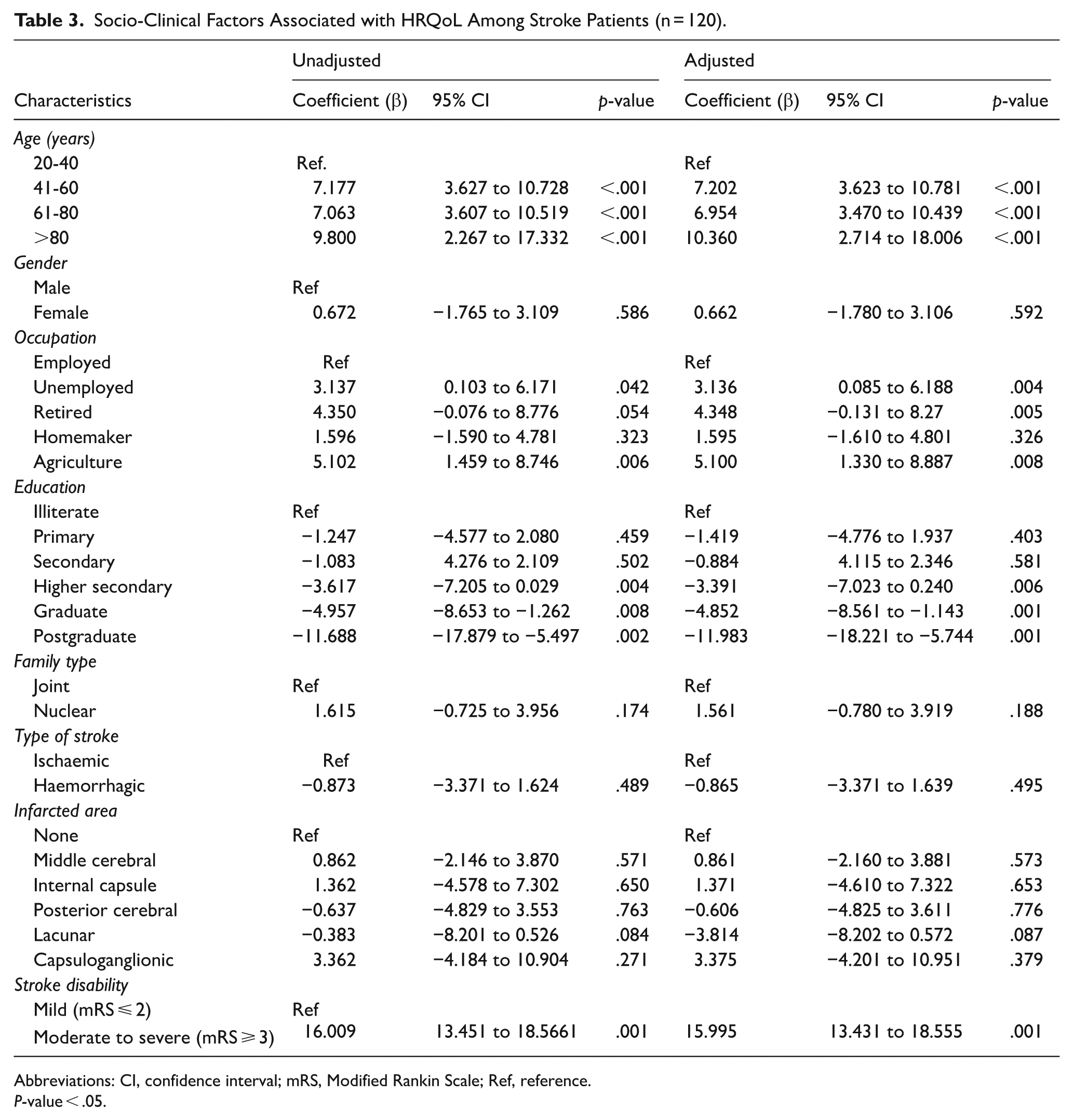
Abbreviations: CI, confidence interval; mRS, Modified Rankin Scale; Ref, reference.
P-value < .05.
Furthermore, patients with moderate to severe stroke-related disability (mRS ⩾ 3) had substantially higher HRQoL scores compared to those with mild disability (β = 15.995, 95% CI: 13.431-18.555, P < .001). In contrast, other factors, including gender, family type, type of stroke, and infarcted area, were not significantly associated with HRQoL after adjustment in the multivariable model
Pearson’s correlation analysis was conducted to assess the relationships between the HRQoL domains, as presented in Table 4. The correlation analysis indicated statistically significant and strong positive correlations between all HRQoL domains. Notably, the overall quality-of-life domain exhibited a strong positive correlation with mobility (r = 0.933), selfcare (r = 0.951), usual activities (r = 0.940), pain/discomfort (r = 0.949), and anxiety/depression (r = 0.956), all significant at P < .01 level. These suggest that overall quality of life is closely linked to all other HRQoL domains.
Correlation Matrix Between HRQoL and Its Domain.
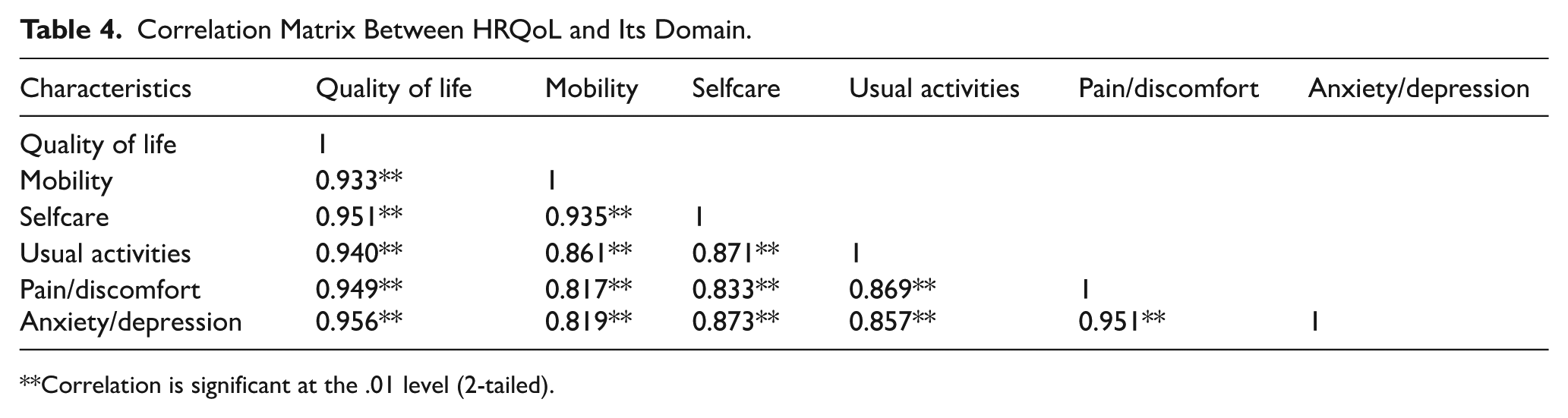
Correlation is significant at the .01 level (2-tailed).
Similarly, the self-care domain was significantly associated with mobility (r = 0.935), pain/discomfort (r = 0.833), and anxiety/depression (r = 0.873), suggesting that individuals with better self-care abilities also tend to report better physical and psychological well-being. Likewise, the usual activities domain demonstrated strong correlations with overall HRQoL, pain/discomfort, and anxiety/depression (r = 0.857, P < .01), suggesting that limitations in daily activities may detrimentally impact both physical and emotional health. Furthermore, the strong positive associations between pain/discomfort and anxiety/depression with other domains highlight the significant role that physical discomfort and psychological distress play in framing overall health-related quality of life.
Discussion
This study assessed HRQoL among stroke patients at a tertiary care hospital in Nepal and identified key sociodemographic and clinical factors associated with it. The findings revealed a substantial impact of stroke on all domains of HRQoL, with the most significant impairments observed in usual activities, self-care, and mobility. Factors such as age, educational level, occupational status, and stroke-related disability emerged as significant determinants influencing overall HRQoL.
The mean EQ-5D-5L score of 21.13 ± 6.62 demonstrates a moderate to severe impact of stroke on the HRQoL of Nepali patients. This is consistent with previous studies that consistently reported diminished quality of life among stroke survivors, particularly in resource-limited settings where structured rehabilitation services are often lacking.3,14,21,22 Among the assessed HRQoL domains, usual activities, self-care, and mobility had the highest impairment scores, underscoring the debilitating consequences of stroke on a patient’s functional independence. These findings align with existing literature, which frequently identifies physical functioning as the most affected area of HRQoL following stroke.2,13,14,23 -25 Additionally, high scores in the pain/discomfort and anxiety/depression domains highlight the psychological burden of stroke. Individuals experiencing these symptoms post-stroke are known to have poorer HRQoL.26,27
In this study, age was a significant determinant of HRQoL, with older adults reporting lower scores, reflecting poorer perceived health. This finding is consistent with previous research demonstrating that advancing age is associated with lower HRQoL, likely due to age-related functional decline, increased comorbidities, and reduced physiological resilience, all of which hinder recovery and exacerbate disability.10,11,21,23
Notably, higher educational attainment was associated positively with HRQoL. Participants with postgraduate, graduate, and higher secondary education reported significantly better HRQoL compared to those who were illiterate. Similar associations have been reported in international studies, where lower education levels have consistently predicted lower quality of life among stroke patients.10,13,28 Educated Individuals are generally more informed about their disease condition, treatment options, and rehabilitation strategies, leading to better adherence to medical recommendations and improved outcomes. Moreover, higher education is often linked with greater economic resources and access to specialized care, both of which contribute to enhanced recovery and quality of life.14,29
Occupational status also influenced HRQoL. Retired individuals, the unemployed, and those engaged in agriculture reported significantly poorer HRQoL, likely due to economic insecurity and reduced social engagement, factors similarly identified in studies conducted in Southeast Asia. 28 However, studies from Ethiopia and Iran reported no significant association between occupational status and HRQoL, suggesting that this relationship may vary by socioeconomic and cultural context.13,14
Stroke-related disability, as measured by the Modified Rankin Scale, emerged as the most significant predictor of poor HRQoL. Patients with moderate to severe disability (mRS ⩾ 3) were significantly more likely to report lower HRQoL, reinforcing the well-established link between functional limitations and reduced quality of life. 21 the dependency resulting from such disabilities places considerable physical and emotional strain on both patients and caregivers.
Furthermore, the study revealed strong, statistically significant positive correlations among all HRQoL domains. Overall quality of life was highly associated with mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Notably, self-care was strongly associated with improved physical and psychological health. Similarly, impairments in usual activities were closely tied to pain and emotional distress, underscoring the broad impact of functional limitations on overall well-being. The strong interrelationships between pain/discomfort and anxiety/depression with other domains further highlight their central role in shaping HRQoL in stroke survivors.
This study is among the few in Nepal to use the EQ-5D-5L scale to assess HRQoL in stroke patients and provides a comprehensive analysis of associated socio-clinical factors. The use of a validated tool and face-to-face interviews enhances the data reliability. However, several limitations should be acknowledged. First, the cross-sectional study design limits the ability to establish causal relationships or assess changes in HRQoL over time. Second, the use of convenience sampling and self-reported responses may introduce selection and social desirability biases, potentially limiting the generalizability. Third, the exclusion of patients with aphasia or cognitive impairments might have led to an underestimation of HRQoL impairment. Lastly, despite multivariable analysis, residual confounding from unmeasured variables such as income and access to rehabilitation services may persist.
Conclusion
The study highlights the profound effect of stroke on patients HRQoL, with significant impairment in usual activities, self-care and mobility. Key factors including age, educational level and occupational status were the crucial determinants of HRQoL, with stroke-related disability, the strongest predictor of diminished HRQoL. These findings emphasized the need for personalized rehabilitation strategies to optimize HRQoL outcomes addressing the physical, psychological, and social aspects of stroke recovery.
Footnotes
Acknowledgements
We sincerely thank the Annapurna Neurological Institute and Allied Sciences Hospital and the patients who participated in this study for generously sharing their time and valuable information. This study would not have been possible without their contributions.
Ethical Considerations
The study was approved by the Institutional Review Committee of Annapurna Neurological Institute & Allied Sciences (IRC-ANIAS, Ref No.: 115-2023/24) and was conducted in accordance with the Helsinki Declaration of Ethical Principles.
Consent to Participate
Written informed consent was obtained from the patients.
Author Contributions
NRM: Conceptualization, methodology, validation, formal analysis, supervision, visualization, project administration, resources, writing – original draft, Writing – review and editing SP: Conceptualization, methodology, data curation, project administration, resources, Writing – review and editing; SS: methodology, data curation, validation, formal analysis, writing – original draft, Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data used to support the findings of this study are available from the corresponding author upon reasonable request.