
Abstract
Background:
When parents or other guardians of children need treatment for a substance use disorder, it presents challenges impacting both them and their children, as a lack of childcare can be a barrier to treatment access. However, some treatment facilities provide childcare services to increase access. Little is known about how local economic factors like childcare costs and income levels are associated with the availability of childcare services in addiction treatment programs in the United States.
Objectives:
This study’s objectives were twofold: (1) assess whether county-level childcare prices are associated with the availability of childcare services in substance use disorder treatment facilities, and (2) assess whether county-level median household income is associated with the availability of childcare services in substance use disorder treatment facilities.
Design:
This is a cross-sectional study.
Methods:
This study examined n = 9003 substance use disorder treatment facilities in the United States. Childcare costs and median income estimates were linked with facilities based on the county in which they were located. Univariable and bivariable statistics were used to examine the facilities. An adjusted logistic regression model was used to evaluate associations between childcare availability and county-level economic indicators, while controlling for facility-level characteristics.
Results:
Approximately 5.7% (n = 514) of the facilities in the sample had childcare services. The multivariable logistic regression model identified factors associated with facilities having childcare including having outpatient and residential treatment (compared to having only outpatient only), accepting females only (compared to accepting males only), having a pregnant or postpartum program/group, accepting Medicaid, slightly higher county-level toddler center prices, and slightly higher county-level preschool center prices.
Conclusion:
Local childcare costs, but not median income appears to be slightly associated with the availability of childcare services in substance use disorder treatment settings. Economic investment in family-friendly services may help reduce access barriers for parents seeking treatment.
Introduction
Estimates suggest that approximately 12% of children in the United States (U.S.) reside in households in which a parent has a substance use disorder (SUD). 1 Along with the impact of SUD on the parent, parental SUD is associated with emotional disturbances, mental health challenges, and substance use among children.2,3 Parents or guardians, especially those with greater socioeconomic challenges,4-6 may encounter barriers to accessing treatment when there is an absence of reliable loved ones or other trusted adults to care for their child. The combined complexity of SUD and parenting is also further complicated by the risk of losing custody of their children and related outcomes.6-10 The absence of childcare during SUD treatment is not only a barrier to treatment access, but it may affect treatment retention, especially for those in high risk populations experiencing structural barriers (lack of housing and lack of supportive social networks). 11 Lack of childcare is problematic as the health and well-being of those in need of SUD treatment and the broader familial unit can be negatively affected if treatment services are not accessed.
Internationally, different countries, such as Australia, England, Northern Ireland, and the U.S., have implemented policies to treat SUD among parents with interventions such as childcare and family drug treatment courts.12-14 Clinicians and researchers have long identified the impacts of parenting among individuals undergoing SUD treatment highlighting the importance of childcare services in these settings.14-16 A review paper examining SUD treatment programs for women in which “child care” was used as a search term identified childcare as an intervention among studies conducted in Australia and U.S. 13 Further, those researchers identified that women focused programs that have prenatal or childcare improve post-treatment outcomes for the children and their mothers. 13 Another review paper examined the needs of mothers with a SUD and identified the importance of comprehensive childcare services in improving outcomes among studies based in various countries including Iran, Portugal, and the United States. 17 Overall, studies indicate that incorporating childcare services in SUD treatment improves both SUD-related and parenting outcomes.18,19 Children are often a motivating factor for parents entering treatment, 20 particularly when caregiving does not present as a barrier to treatment access. 21 Studies have found that the availability of childcare impacts women more than men regarding accessing SUD treatment.22-24 This is important when considering that the majority of women entering treatment (73%), report having dependents under age 18. 25
While levels of parental programming vary among treatment agencies, childcare support can be an integral form of support that is associated with better parenting factors for at-risk families, including promoting parental skills, quality of mother-child interactions, and secure child attachment. 26 Parents can better focus on their treatment when they have reliable childcare. Additionally, the inclusion of caregiver-child relationships in the treatment plan benefits the family unit more than parental treatment alone. 27 Although childcare services in SUD treatment are associated with several beneficial outcomes, childcare is not universally available for parents in treatment facilities. Administrators of SUD treatment facilities may cite a lack of available funding to provide childcare services to their patients in need. 28
In the general population, there is a shortage of childcare options, and there is considerable nationwide variability in the cost and availability of childcare services. For example, families spend between 8.9% and 16.0% of their income on full-day care for one child. 29 Additionally, socioeconomic characteristics of a given area often dictate the availability, type (eg, infant, toddler, preschool, and school-age; center or home-based), quality, and cost of childcare.29-31 On average, underserved areas contain fewer options. 32 Relatedly, although there are more options for childcare in high socioeconomic areas,30,32 the local market rate for childcare is influenced by demand, location, type, and ratio of caregiver-to-child. Identification of contextual socioeconomic factors that affect childcare in the general population suggests there is a need to determine whether similar factors are associated with the availability of childcare in SUD treatment facilities.
As in the general population, there is a shortage of childcare in treatment facilities. Estimates suggest that less than 10% of treatment facilities that serve women in the United States provide childcare services.33-35 Some factors associated with the availability of childcare at SUD treatment facilities have been identified. For instance, one study found that treatment facilities without services for pregnant and postpartum women are less likely to have childcare than facilities with dedicated services for pregnant and postpartum women (3% vs 16% respectively). 35 The variation in availability of childcare services in treatment centers highlights a need to explore interactions between socioeconomic context and facility level characteristics that contribute to childcare availability.
Studies have identified treatment facility characteristics and socioeconomic factors independently associated with SUD facilities providing childcare services. However, we were unable to identify any studies that examined associations between SUD treatment childcare service availability while considering average county-level childcare prices and median income in the U.S. Counties are considered the main subdivision of states in the U.S. 36 Therefore, this study sought to fill this gap in the literature by examining county-level childcare prices and median family income, relevant treatment facility characteristics, and the availability of childcare services in SUD treatment. Findings from this study may point to economic considerations in improving childcare access to parents needing SUD treatment.
Methods
Data
All data used in this study were publicly available which was determined to be non-human subjects research by the University of North Carolina at Chapel Hill Institutional Review Board. Three datasets were used to complete this study: (a) American Community Survey, 37 (b) Childcare Prices by Age of Children and Care Setting, 38 and (c) National Directory of Drug and Alcohol Use Treatment Facilities. 39 Data included in this study were downloaded on January 15, 2025. The American Community Survey dataset contains estimates of demographic, housing, and socioeconomic factors about communities throughout the United States. 37 The Childcare Prices by Age of Children and Care Setting dataset contains data on the average costs for center-based or home-based services throughout the United States. 38
The National Directory of Drug and Alcohol Use Treatment Facilities dataset contains information on all known SUD treatment facilities that responded to the Substance Abuse and Mental Health Services Administration’s 2022 National Substance Use and Mental Health Services Survey and selected yes to being listed on an online treatment locator directory. 39 Essentially, the Substance Abuse and Mental Health Services Administration sends a survey to all known SUD treatment facilities in the United States to capture the services that they provide. Of the 20 898 SUD treatment facilities invited to participate in the 2022 National Substance Use and Mental Health Services Survey, 14 854 were included in that study. 40 The 2023 National Directory of Drug and Alcohol Use Treatment Facilities includes data from 12 744 SUD treatment facilities. 39 The primary unit of analysis for this study was SUD treatment facilities using the 2023 National Directory of Drug and Alcohol Use Treatment Facilities. Using the package ZipcodeR 41 in R, 42 treatment facility zip codes were matched to their corresponding county and state. County-level data from the American Community Survey and Childcare Prices by Age of Children and Care Setting were matched with the treatment facilities. Therefore, county-level variables for each treatment facility were added. The income and price data in this study are presented in United States dollars.
Measures
Childcare Services
This binary Yes/No dependent variable described whether a treatment facility provides childcare services for parents receiving treatment from them. This variable was extracted from the National Directory of Drug and Alcohol Use Treatment Facilities dataset. 39
County Childcare Prices
Eight numeric variables identified the average childcare prices for the county in which a treatment facility was located. Infant, toddler, preschool, and school-age prices were provided for childcare centers and home-based care. These variables were extracted from the Childcare Prices by Age of Children and Care Setting dataset. 38
County Local Percentages of Youth Population
Four numeric variables identified the percentage of minors for the county in which a treatment facility was located. These variables included (a) under 5 years old, (b) 5 to 9 years old, (c) 10 to 14 years old, and (d) under 18 years old. These variables were extracted from the American Community Survey. 37
County Median Family Income
This numeric variable extracted from the American Community Survey 37 identified the median family income for the county in which a treatment facility was located. Median family income was selected instead of the mean to avoid extreme outliers impacting the data. Family income was selected instead of household income as family is defined by the United States Census Bureau as individuals being related by adoption, birth, or marriage, in the same location. However, household is defined as all individuals in that housing unit, which may include individuals living alone or roommates. 43
Gender Accepted
This categorical variable indicated whether a facility admitted men only, women only, or both men and women. This variable was extracted from the National Directory of Drug and Alcohol Use Treatment Facilities dataset. 39
Payment Options Accepted
Four different binary (Yes/No) variables described whether different payment options were accepted by a facility. These variables are (a) Medicare, (b) Medicaid, (c) Private Health Insurance, and (d) Cash or Self-Payment. These variables were extracted from the National Directory of Drug and Alcohol Use Treatment Facilities dataset. 39
Percentage of County SUD Facilities with Childcare
This numeric variable described the percentage of SUD facilities with childcare services in a specific county in which a specific facility was located. Therefore, if a facility was located in a county in which 10.4% of all the treatment facilities had childcare services, that facility would have 10.4 as a value for this variable. This variable was created by using the childcare services variable (Section “Childcare Services”).
Pregnant or Postpartum Program/Group
This binary variable included Yes and No values for whether a treatment facility has a program or group specifically for individuals who are pregnant or postpartum. This variable was extracted from the National Directory of Drug and Alcohol Use Treatment Facilities dataset. 39
Service Setting
This categorical variable described whether a treatment facility has outpatient treatment only, residential treatment only, or outpatient and residential treatment. This variable was extracted from the National Directory of Drug and Alcohol Use Treatment Facilities dataset. 39
Quartiles of Aggregate Childcare Prices
Any of the eight County Childcare Prices listed above (Section “County Childcare Prices”) that were associated with the dependent variable (Section “Childcare Services”) in the bivariable analyses were summed. This summed variable was separated into quartiles based on the county in which a facility was located. This variable was suggested during the peer review process and used in a posteriori logistic regression models.
Sample Selection
The initial National Directory of Drug and Alcohol Use Treatment Facilities dataset contained 12 744 treatment facilities. After applying the sample selection criteria: (a) facilities provide SUD treatment (some facilities may just screen and provide referrals and not necessarily treatment; which resulted in 12 502 facilities), (b) facilities providing outpatient and/or residential treatment (some facilities may only provide telehealth/telemedicine services; which resulted in 12 380 facilities) and, (c) facilities not missing data for the measures listed above, the final sample included 9003 treatment facilities. Therefore, of the 12 744 SUD treatment facilities included in the 2023 National Directory of Drug and Alcohol Use Treatment Facilities, approximately 71% were included in the current study’s final sample after simultaneously applying the sample selection criteria. Facilities in specific states and the District of Columbia were excluded from the analyses due to missing childcare price data, including Colorado, Indiana, and New Mexico. Facilities in Connecticut were excluded from the analyses due to a county-level shift in which the names and geographic regions of the counties were altered in the state, which caused treatment facility data to be discrepant with the County Local Percentages of Youth Population data. Essentially, the state of Connecticut shifted from eight counties to nine different regions, which are not perfectly aligned geographically.44,45
Analysis
Univariable statistics such as means and percentages were examined. The dependent variable in this study was childcare services. This variable was also used to separate the sample into facilities with childcare services (n = 514; 5.7%) and facilities without childcare services (n = 8489; 94.3%). These separate groups were then used as a basis to conduct bivariable analyses using independent samples t-tests for numeric variables and Chi-square for categorical variables. Independent variables identified as significant in the bivariable analyses were included in binary logistic regression models. Using binary logistic regression models, each independent variable was examined separately in unadjusted models and simultaneously in an adjusted model. Logistic regression models were conducted to examine the association between the dependent variable and the independent variables. Geographically, county-level data were examined in this study, such as county childcare prices and median family income. However, to avoid identifying specific treatment facilities, the data were aggregated to describe percentages for specific states instead of specific counties (see Table 1).
State-Level Percentage of Substance Use Disorder Treatment Facilities with Child Care.
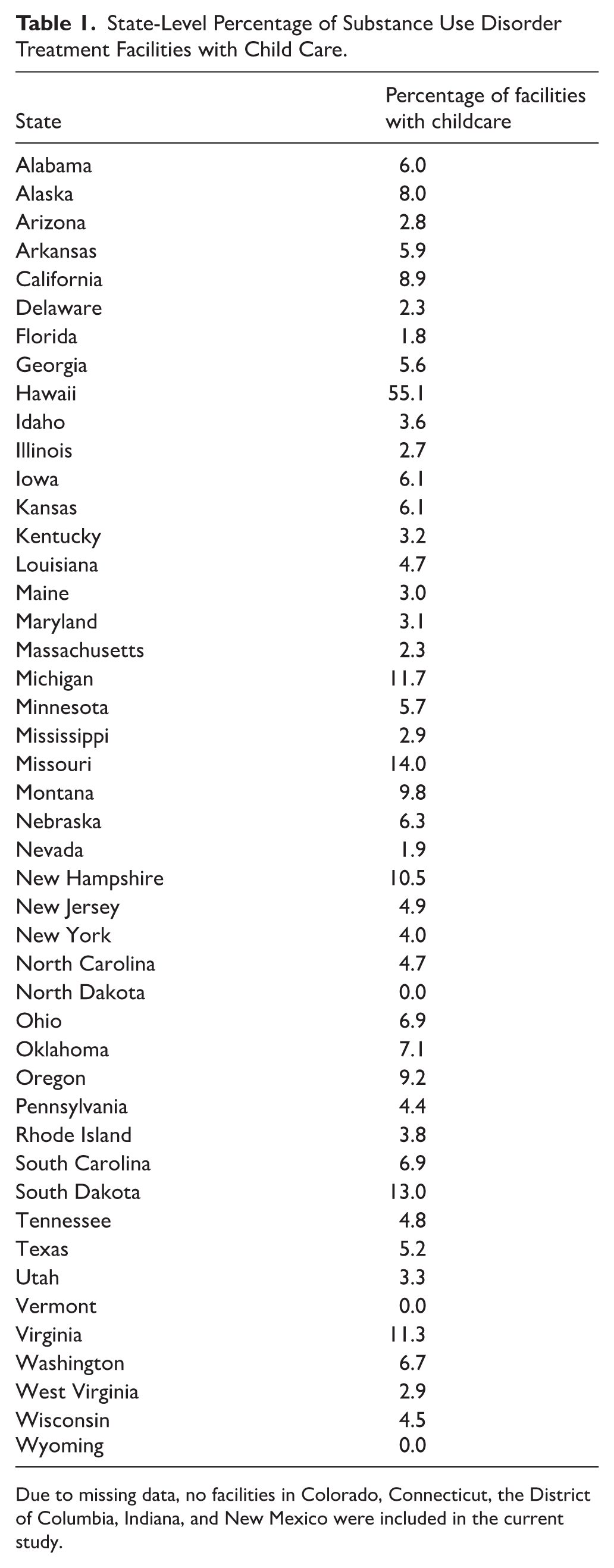
Due to missing data, no facilities in Colorado, Connecticut, the District of Columbia, Indiana, and New Mexico were included in the current study.
Ethical Review
As all study data are publicly available and examined aggregately, the University of North Carolina at Chapel Hill determined that this study was not human subjects research.
Results
Descriptive Characteristics
Table 1 provides state level data identifying the percentage of facilities included in this study with childcare services. The percentage of county SUD facilities with childcare ranges from 0.0% to 100.0%. However, approximately 38% (n = 3396) of facilities were located in a county in which no facilities had childcare services. Facilities were from 743 different counties in 46 different states. Approximately 5.7% (n = 514) of facilities in the sample had childcare services. As seen in Table 2, the presence of childcare services was significantly associated with service setting, gender accepted, pregnant or postpartum program/group, accepting Medicaid, accepting private health insurance, accepting cash or self-payment, percent of county SUD facilities with childcare, infant center price, toddler center price, preschool center price, preschool home price, and school-age home care price. These 12 variables were included in the binary logistic regression models.
Descriptive Characteristics of Substance Use Disorder Treatment Facilities With and Without Child Care Services.

Income and price data are presented in United States dollars.
A posteriori bivariable analyses were conducted examining the associations between childcare service availability with county childcare prices subtracted from the county median family income. These results may be found in Supplemental Table 1.
Factors Associated with Childcare Services
Results from the binary logistic regression models may be seen in Table 3. Factors associated with childcare availability in SUD treatment facilities in the unadjusted and adjusted models were (a) having outpatient and residential treatment, (b) accepting females only, (c) having a pregnant or postpartum program/group, (d) accepting Medicaid, (e) accepting private health insurance, (f) accepting cash or self-payment, (g) percentage of county SUD facilities with childcare, (h) county-level toddler center prices, and (i) county-level preschool center prices.
Binary Logistic Regression Models Examining Childcare Services in Substance Use Disorder Treatment.

The variables in the leftmost column were included in the unadjusted models and the adjusted model.
P < .05. **P < .01. ***P < .001.
In the adjusted model each of these nine variables were associated with facilities having childcare based on the adjusted odds ratios (AOR) such as (a) AOR = 2.390 (95% confidence interval [CI] = 1.709, 3.341; P ⩽ .001) for having outpatient and residential treatment, (b) AOR = 14.169 (95% CI = 6.994, 28.707; P ⩽ .001) for accepting females only, (c) AOR = 3.693 (95% CI = 2.924, 4.665; P ⩽ .001) for having a pregnant or postpartum program/group, (d) AOR = 1.924 (95% CI = 1.444, 2.565; P ⩽ .001) for accepting Medicaid, (e) AOR = 0.710 (95% CI = 0.550, 0.917; P = .009) for accepting private health insurance, (f) AOR = 0.646 (95% CI = 0.468, 0.891; P = .008) for accepting cash or self-payment, (g) AOR = 1.114 (95% CI = 1.104, 1.125; P ⩽ .001) for the percentage of county SUD facilities with childcare, (h) AOR = 1.000 (95% CI = 1.000, 1.000; P ⩽ .001) for county-level toddler center prices, and (i) and AOR = 1.000 (95% CI = 1.000, 1.000; P ⩽ .001) for county-level preschool center prices. For the adjusted model, the Cox & Snell R2 is .134 and the Nagelkerke R2 is .379.
The Quartiles of Aggregate Childcare Prices variable was made by summing five different County Childcare Prices variables: (1) Infant Center, (2) Toddler Center, (3) Preschool Center, (4) Preschool Home Care, and (5) School-Age Home Care. This variable was then separated into quartiles based on the county in which a facility was located, with cutoffs being 45 289.9065 for the 25th quartile, 56 310.1749 for the 50th quartile, 68 777.9821 for the 75th quartile, and the remaining values, which were >68 777.9821, for the 100th quartile. Supplemental Table 2 shows the results of the quartiles variable with other County Childcare variables excluded from the adjusted logistic regression model.
Discussion
Childcare is a prominent consideration for parents needing SUD treatment. SUD treatment facilities that provide childcare services may increase accessibility to and retention in treatment.11,18,20,21 By examining characteristics of treatment facilities and county-level childcare and income data, we identified having outpatient and residential treatment, admitting females only, having a pregnant or postpartum program/group, accepting Medicaid, not accepting private health insurance, not accepting cash or self-payment, being in a county in which there is a higher percentage SUD facilities with childcare, slightly higher county-level toddler center prices, and slightly higher county-level preschool center prices to be associated with treatment facilities having childcare services.
Six percent of treatment facilities in our sample offer childcare services, with state-level variability ranging from 0% to 55%. This finding is troubling because a lack of childcare services is one of the most significant barriers to treatment for parents. Further, women are more likely to act as the primary caregiver while facing a disproportionate number of structural barriers to treatment compared to men (eg, housing instability, legal issues, lack of transportation).21,46 Offering outpatient and residential treatment programs with on-site childcare or child-friendly policies is a vital strategy that acknowledges the challenges of caregiving responsibilities for caregivers seeking treatment for SUD. Outpatient and residential treatment both offer unique logistics for incorporating childcare services. Outpatient treatment would suggest that a patient’s child(ren) would accompany them to the facility, then leave with the patient on the same day on which services were received. However, residential treatment has more unique considerations for childcare services on-site, as the child(ren) would live at the facility with the patient. Both on-site and child friendly policies provide opportunities for individuals to reach their recovery goals. 47 When parents can bring their children with them or are assured that their children are in safe care while they attend treatment, retention in programs increases, and return to use rates decrease.11,18,20,21 Family-focused residential programs provide a powerful model that addresses not only the individual’s recovery but also supports the parent-child relationship and the developmental needs of children impacted by parental substance use. 48
Integrated programs often include parenting support, trauma-informed therapy, and opportunities for bonding, recognizing the intergenerational impact of substance use and recovery.49-52 By investing in such wraparound services, healthcare systems acknowledge the role of social determinants in recovery and offer a compassionate, practical path forward. Furthermore, co-locating childcare with treatment facilities directly challenges stigma by affirming that parents and especially mothers who use substances are not unfit to parent;10,53 rather, caregivers must navigate systems that can fail to support them. Programs that accommodate parenting responsibilities lead to better outcomes for both mother and child, underscoring the importance of reimagining care models that meet people where they are. 54 Future research may examine the role of specific programming components in relation to individual and family level outcomes among mothers in SUD treatment facilities.
Regarding treatment-level characteristics, this study found that treatment facilities that admit only female clients are significantly more likely to offer childcare services. This finding facilitates a deeper understanding of the gendered realities of substance use and recovery. Mothers seeking treatment for SUD face unique challenges, including fear of child welfare involvement, lack of childcare, and stigma related to parenting while using substances. 54 By tailoring services to the needs of women, these facilities acknowledge the complex interplay of substance use, caregiving responsibilities, intimate partner violence, and mental health issues. This gender-responsive approach is backed by evidence showing that women in female-only programs with childcare report higher treatment satisfaction and improved retention. 13 The inclusion of childcare in female-only settings is a foundational aspect of trauma-informed, equitable care that aligns with broader public health goals of reducing intergenerational harm and promoting family stability. 33
Relatedly, another treatment facility level characteristic associated with having childcare is the provision of services for pregnant and postpartum women. This study confirms extant literature as SUD treatment programs in this sample were more likely to provide childcare when they offered services tailored to pregnant or postpartum individuals. 35 Pregnancy and the postpartum period are critical windows for intervention, marked by both heightened vulnerability and increased motivation for change. 55 However, without supportive services like childcare, many individuals are unable to attend treatment consistently, or at all, especially if they are pregnant and are raising another child.6,55-57
Programs that address perinatal needs often include wraparound supports such as prenatal care coordination, parenting groups, mental health services, and child development resources alongside substance use treatment. 58 On-site or affiliated childcare is a central element, reducing logistical barriers and reinforcing a message that parenting and recovery are not mutually exclusive. 59 These programs also serve a protective function for infants and young children, reducing the risk of adverse developmental outcomes associated with maternal substance use and separation. 14 Integrated perinatal substance use programs that include childcare may not only improve treatment retention and birth outcomes but also foster long-term family stability. 14 Expanding the availability of such services is a public health imperative grounded in compassion and evidence.
This study also found that facilities accepting Medicaid are more likely to have childcare services. Alternatively, facilities accepting private health insurance or cash/self-payment were less likely to have childcare services. Considering these findings, with these payment options as potential proxy variables, it seems more likely that facilities for individuals with higher socioeconomic needs are more likely to provide childcare services. Finally, this study examined socioeconomic context surrounding SUD treatment facilities. Infant center, preschool home care, and school-age home care county-level prices were not associated with the availability of childcare services in the multivariable model. This suggests that while the absolute cost of childcare is high in many regions, it may not directly influence whether treatment programs provide childcare services. Furthermore, childcare costs vary based on the costs of different types of childcare services at the county-level.
There are several possible interpretations of this finding. In counties where childcare is more expensive, facilities may lack the resources to provide onsite services or may rely more heavily on external partnerships and referrals, limiting accessibility. Alternatively, the presence of higher childcare costs could reflect broader market dynamics in wealthier counties, where programs are more likely to be better funded and situated in more resource-rich environments. 32 Further, this study did not find median level county income to be associated with childcare service availability in SUD treatment settings. Childcare availability is not merely a function of cost but of institutional prioritization and infrastructure. Economic hardships can significantly limit the childcare options available to parents overall.30,60,61 SUD treatment programs committed to serving parents may absorb the cost of providing childcare as part of a family-centered treatment philosophy. Therefore, policy interventions aimed at expanding childcare in treatment settings should focus not only on reducing childcare costs but also on incentivizing integration within treatment programs, particularly in under-resourced counties. 62
Unlike other economic indicators, county-level toddler center prices and preschool center prices showed a very slight positive association with the availability of childcare services in SUD treatment programs in adjusted models, when controlling for income and other contextual variables. This suggests that higher preschool center care prices and toddler center care prices alone do not independently predict the presence of childcare in treatment facilities. In fact, they may act as a proxy for broader socioeconomic and facility-level conditions rather than directly influencing program decisions. Future studies may examine the contextual socioeconomic factors that affect the cost of childcare and availability of childcare in SUD treatment facilities. Further, future studies focusing on policy-based research are needed to examine the potential impact of state and county-level policies on the availability of childcare services in treatment facilities.
Limitations
The National Directory of Drug and Alcohol Use Treatment Facilities is self-report and only includes facilities that complete the National Substance Use and Mental Health Services Survey and opt in to being included in the directory. While this dataset provides the most detailed description of all known SUD treatment facilities in the United States, it is not the total population of facilities. Further, the National Directory of Drug and Alcohol Use Treatment Facilities dataset is self-report, which may introduce response bias. The American Community Survey and Childcare Prices by Age of Children and Care Setting provide estimates of economic level data. Another limitation is only examining SUD treatment facilities and not mental health treatment facilities. No power analysis was conducted. Although 71% of the 12 744 SUD treatment facilities were retained from the 2023 National Directory of Drug and Alcohol Use Treatment Facilities, missing data excluded facilities from four states and Washington, DC (Colorado, Connecticut, the District of Columbia, Indiana, and New Mexico). Considering these limitations, this study identified pertinent county-level economic factors and treatment facility characteristics associated with facilities having childcare services. This study may prompt local considerations for child-care service availability in SUD treatment facilities.
Conclusion
This study identified that only 6% of SUD treatment facilities provide childcare services. Overall, some parents seeking SUD treatment may face difficulties entering treatment as they consider having to balance childcare. This study highlights the limited availability of childcare in SUD treatment programs across the United States and identifies key facility and county-level characteristics associated with its presence. Childcare was more commonly available in having outpatient and residential treatment, admitting females only, having a pregnant or postpartum program/group, accepting Medicaid, not accepting private health insurance, not accepting cash or self-payment, being in a county in which there is a higher percentage SUD facilities with childcare, slightly higher county-level toddler center prices, and slightly higher county-level preschool center prices – underscoring how structural factors influence access to family-friendly care. Surprisingly, most local childcare costs were not consistently linked to whether treatment facilities offered childcare, suggesting that broader institutional priorities and resource allocation play a more pivotal role than market price alone. As SUD treatment systems strive to become more responsive, integrating childcare must be viewed not as an ancillary service, but as a core component of effective care. Future research and policy efforts should focus on funding mechanisms, regulatory supports, and implementation strategies that expand access to childcare in treatment settings, particularly in underserved areas where the need is greatest.
Supplemental Material
sj-docx-1-his-10.1177_11786329251405979 – Supplemental material for Is Childcare Availability in Addiction Treatment Associated with County-Level Childcare Prices and Median Income in the United States?
Supplemental material, sj-docx-1-his-10.1177_11786329251405979 for Is Childcare Availability in Addiction Treatment Associated with County-Level Childcare Prices and Median Income in the United States? by Orrin D. Ware, G. Rose Geiger, Malina A. Howard, Stefani N. Baca-Atlas and Michael H. Baca-Atlas in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251405979 – Supplemental material for Is Childcare Availability in Addiction Treatment Associated with County-Level Childcare Prices and Median Income in the United States?
Supplemental material, sj-docx-2-his-10.1177_11786329251405979 for Is Childcare Availability in Addiction Treatment Associated with County-Level Childcare Prices and Median Income in the United States? by Orrin D. Ware, G. Rose Geiger, Malina A. Howard, Stefani N. Baca-Atlas and Michael H. Baca-Atlas in Health Services Insights
Footnotes
Author Contributions
Orrin D. Ware, PhD, MPH, MSW: Conceptualization, methodology, validation, formal analysis, investigation, data curation, writing – original draft, writing – review and editing, visualization, supervision, project administration. G. Rose Geiger, BA: Conceptualization, methodology, writing – original draft, writing – review and editing. Malina A. Howard, MD: Conceptualization, writing – original draft, writing – review and editing. Stefani N. Baca-Atlas, PhD, MSW: Conceptualization, writing – original draft, writing – review and editing. Michael H. Baca-Atlas, MD: Conceptualization, writing – original draft, writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stefani N. Baca-Atlas received support from the Population Research Training grant (T32 HD007168) and the Population Research Infrastructure Program (P2C) awarded to the Carolina Population Center at The University of North Carolina at Chapel Hill by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data used in this study are publicly available. Three datasets were used to complete this study: (a) American Community Survey: https://www.census.gov/programs-surveys/acs/data.html; (b) Childcare Prices by Age of Children and Care Setting: https://www.dol.gov/agencies/wb/topics/childcare/price-by-age-care-setting; (c) National Directory of Drug and Alcohol Use Treatment Facilities: ![]()
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.