
Abstract
Background:
Palliative care units and specialised palliative home care teams are well established in many countries. Palliative day-care clinics, however, are not. Studies assessing which patients benefit from this setting of care are rare.
Aim:
This is the first routine data analysis of patients treated in three settings of specialised palliative care within a single geographical region. Our aim was to gain understanding of how patients in this region, where specialised palliative care structures are well-established, differ in their characteristics and treatments, and to explore the potential role of a palliative day-care clinic.
Design:
Retrospective data were extracted from medical records and analysed using SPSS® and R®. Data were analysed using the Shapiro-Wilk, Chi-Square, and Kruskal-Wallis tests. Setting/Participants: Patients (n = 603) were included if they received treatment at either a palliative day-care clinic, a palliative care unit, or a specialised palliative home care service. To cover the “normal” pre-pandemic period, the analysis was conducted retrospectively from 31 December 2019.
Results:
Patients attending the palliative day-care clinic were more likely to have cancer (90%, P < .001), were younger than those receiving specialised palliative home care (66.1, P < .001), had a better ECOG performance status (2, P < .001) and fewer high-complexity symptom domains (3.4, P < .001). Patients in the palliative day-care clinic and the palliative care unit underwent similar numbers of medical procedures and interventions. The majority of patients were admitted to the palliative day-care clinic from home (76%, P < .001) and discharged to the palliative care unit (41.5%, P < .001).
Conclusions:
The three care models differ in their patient populations, time-based criteria and symptom burden—with the palliative day-care clinic treating younger patients at earlier stages of the disease, with a lower ECOG score and a less complex symptom burden. These variations emphasise the importance of tailoring palliative care to the needs of patients and the progression of their disease. Recognising these differences can enhance integrated care pathways and patient-centred outcomes in various settings.
Keywords
Key Statements
What Is Already Known About the Topic?
Palliative care should be provided early in the course of the disease and in structures that allow patients to remain at home for as long as possible.
Early palliative care significantly improves quality of life, symptoms and satisfaction with care.
Palliative care day services provide a safe and secure environment for people with complex palliative care needs, enabling them to access a range of services, while also acting as a respite service for family carers.
What This Paper Adds
The palliative day-care clinic provides a low-threshold, specialised palliative care service within the framework of early integration and addresses gaps in care for patients with complex needs.
Less invasive procedures as provided by the palliative day-care clinic can minimise the need for hospitalisation and/or longer hospital stays.
Hospitalisation during treatment can be delayed by the palliative day-care clinic, which can lead to savings in healthcare costs. By sharing diagnostic and therapeutic resources within a clinic, costs can be reduced.
The palliative day-care clinic allows patients to stay at home longer, providing a more familiar and supportive environment in which to recover.
Implications for Practice, Theory, or Policy
Palliative day care has a clear added value in the (palliative) care landscape and should be part of standard health care.
A full economic evaluation is needed, not only to demonstrate the benefit to patients and families, but also to quantify the impact on the health care system.
Introduction
According to international guidelines, palliative care should be provided early in the course of the disease and in structures that allow patients to remain at home for as long as possible.1,2
Access to home care is dependent on meeting certain criteria, and the necessary support and solutions will vary from person to person. A systematic review by Filiciano et al 3 found that home-based palliative care interventions can significantly improve quality of life and increase the likelihood of patients dying at home. These interventions also reduce the use of healthcare services, particularly hospital admissions and visits to the emergency department, emphasising a patient-centred approach and supporting the sustainability of the healthcare system. 4 A study in Belgium has shown that palliative home care reduces total costs of care at the end of life. 5
Ribeiro et al 6 evaluated transitions to home care, concluding that the majority of complex patients could be effectively monitored and die at home. Hospital deaths would be reserved for exceptional cases requiring interventions that could not be carried out at home or for those where there would be a significant burden on caregivers. An own study 7 found that, in the last 3 months of life, caregivers needed support in managing out-of-hours care, financing home care, and preparing for it, as well as in communicating with medical staff and managing pain.
Relatives whose next of kin did not die at home—although this was the preferred option—had greater support needs. This suggests that these factors are key to providing home care for dying patients.
Palliative day-care clinics can support home care by providing a structured, accessible, interdisciplinary environment in which ongoing symptom management, psychosocial support, and advance care planning are actively coordinated and aligned with care goals at home. These clinics address complex symptom burdens such as pain, dyspnoea, fatigue and delirium, and optimise pharmacotherapy, while offering non-pharmacological interventions such as rehabilitation, counselling and spiritual care. This is achieved through regular daytime assessments by an interprofessional team comprising nurses, physicians, social workers, pharmacists, rehabilitation therapists, and chaplains. By providing education and training for caregivers, as well as respite and instruction in recognising deterioration and managing crises, day-care clinics reduce caregiver strain and empower families to sustain home-based care. 8
A study by Ancuta et al 9 has shown that palliative day- care programmes address physical, psychosocial and spiritual needs, fostering a sense of connectedness and meaning for patients. The results show that it is necessary to increase coverage of the complex needs of patients and families by offering a variety of individually tailored services. This is confirmed by van Hyde et al, 10 who showed that patients using specialist palliative care services should have the opportunity to have their condition assessed and reviewed appropriately, with a wide range of supportive interventions provided.
Palliative day-care clinics enhance continuity of care by generating a shared, up-to-date care plan and ensuring timely communication, also with GPs. 11 This allows for earlier escalation when necessary and facilitates smoother transitions between different care settings. Evidence suggests that palliative day services can help more patients to remain at home, reduce unnecessary emergency visits and hospitalisations, and improve patient and carer satisfaction and perceived quality of life. 8 This is particularly beneficial for individuals with complex symptom clusters or non-cancer illnesses. However, successful implementation hinges on appropriate patient selection and timing, geographical accessibility, adequate staffing and funding, and integration with telehealth and community resources, in order to maintain seamless continuity of care.
While palliative care units and specialised palliative home care teams are well established in many countries, palliative day-care clinics are not as readily available. 12 In Germany, a recent study identified only five palliative day-care clinics. 13
The United Kingdom, Ireland and the United States are proving to be pioneers of palliative day-care.14,15 In the United Kingdom, for example, there were already over 220 day-hospices by the turn of the century. 16 In France and Belgium, palliative day-care services have existed since the 2000s.17,18 In Germany, the national guideline recommends palliative day-care clinics, but only a few have been established to date.13,19,20
Although palliative day-care is offered internationally, only a few studies have been performed on palliative day-care clinics. 21 A recent systematic review has shown that most of the studies were qualitative in nature and demonstrated high patient satisfaction but did not provide sufficient evidence of improved symptom control or quality of life. 18 A quantitative study showed improvements in symptoms, general functionality and quality of life occurring within 1 week in all three settings, with the biggest improvements shown in the palliative day-care clinic. 22 Other studies did not show a benefit by a palliative day-care clinic. 23
This manuscript describes the first study to compare three specialised palliative care settings in a given geographical region of Germany where all three settings have been fully established for years. Palliative day-care clinics, palliative care units and specialised palliative home care are offered to patients; the latter started operating in 2013 under the sponsorship of the local hospice association. The objective of the study was to conduct an external evaluation of the palliative day-care clinic at the Aschaffenburg-Alzenau Clinic and gather data on integrating this model into routine care. We wanted to compare the characteristics and treatments of patients in this geographical region with well-established specialised palliative care structures, and to understand what role a palliative day-care clinic can play.
Materials and Methods
The collected data was used to examine the extent to which there is a gap in care between palliative care units and outpatient care provided by specialised palliative home care teams, as well as how this gap could be closed by a palliative day-care clinic.
The following research questions were posed:
How do the characteristics and treatments of patients in these three care settings compare?
How were the patients previously treated?
Who initiated the further care?
Where does further patient care take place?
This analysis was part of a wider mixed methods evaluation of the palliative day-care clinic Aschaffenburg-Alzenau (Müller et al 8 ).
The evaluation consisted of three work packages. The first work package comprised a quantitative, retrospective analysis of data from 603 patients. SK, an MD student, collected and analysed the retrospective data alongside KL (psychology student) and AF (physician).
In the second work package, qualitative data were collected and 69 interviews were conducted by AD and JS with patients and relatives. 8 In the third work package, questionnaires were sent to referring physicians and 76 questionnaires were analysed by AD (research associate and health services researcher) and JS (principal investigator and health services researcher). 24 The data presented here cover the analysis of work package one. The results of the research questions regarding sociodemographic and medical characteristics, as well as comparisons, are reported in Table 1. The results of medical procedure intensity are reported in Tables 2 and 3, while admission and discharge results are reported in Table 3.
Sociodemographic and Medical Characteristics.
Abbreviations: ECOG, Eastern Cooperative Oncology Group; KW, Kruskal-Wallis test result; χ2, chi-square-independence test result.
Only the 3 most frequent ones are included.
Multiple answers were possible.
Symptom area of high complexity, such as pain, gastrointestinal, urogenital, respiratory, cardiological, neurological, psychiatric, psychological and exulcerative wounds, per German Federal regulations.
Chemotherapy, radiotherapy, cardiological, neurological therapy, or other.
Medical Procedure Intensity.

Abbreviations: KW, Kruskal-Wallis test; PC, palliative care; W, Wilcoxon-rank sum test; χ2, chi-square-independence test.
Diagnostic procedures = number of radiological, physical, sonography, laboratory, pathology diagnostics.
Maximum of four pain medication classes possible: opiates World Health Organization (WHO) level 1, 2, 3 and coanalgetics.
Human albumin and erythrocyte concentrate transfusions.
Admission and Discharge.

Abbreviations: n.s, no statistical significance in the pairwise post hoc comparison; palliative care unit, palliative care unit; palliative day-care clinic, palliative day-care clinic; specialised palliative home care, specialised palliative home care; χ2, chi-square-independence test.
Ethical Approval
This study used aggregated and fully anonymised data, which was collected as part of the routine diagnosis and treatment process prior to our access to it. The study was approved by the Ethics Committee of the Medical Faculty of the University of Cologne (IRB # 25-01-27). As it was a retrospective analysis, informed consent was waived for Work Package 1; therefore, patient or family consent was not required. According to § 15 (1) of the Medical Association’s professional code of conduct for physicians in North Rhine (Germany), there was no obligation to provide retrospective advice. In addition, s. 6 para. 1 sentence 1 of the GDSG NRW also applies, which allows scientific staff to use data to which they already have access in the course of their work for research purposes without requiring the consent of the persons concerned. Personal rights must still be respected. The letter from the ethics committee has been uploaded and can be viewed upon request. This work package was part of a larger study that also received ethical approval (IRB # 20-1377).
Data Sources and Data Management
For this study (work package 1), a retrospective data analysis of 200 (203 in the palliative care unit) consecutive patients treated in the palliative day-care clinic, palliative care unit and specialised palliative home care (inclusion criteria), respectively, backward from December 31, 2019 was carried out, to cover “normal” pre-pandemic times. Pre-pandemic data provide a stable baseline allowing us to distinguish short-term fluctuations. Thus, pre-pandemic data can inform policy by highlighting persistent gaps, even as norms evolve.
This work package was part of an evaluation study that started on June 1, 2020, and ended on August 31, 2021.
The Study Is Presented Using the RECORD Statement
Prior to data collection, parameters were defined based on the core dataset for palliative care patients of the German Society for Palliative Medicine. Sociodemographic parameters (type of care, age at admission, living situation, level of care), diagnosis (brain tumours, oral/jaw/facial NPL (neoplasia), lung/bronchial NPL, breast NPL, ovarian/uterine/cervical NPL, oesophageal/gastric/pancreatic/liver/gallbladder NPL) were pseudonymised, colon/sigmoid/rectum NPL, renal cell/urothelial/prostate NPL, haematological/lymphatic disease, other NPL, underlying neurological disease, underlying medical disease, COPD, heart failure, cirrhosis, other disease).
In addition, metastases, previous care, total number of personal (for specialised palliative care home visits) contacts in the respective care structure, average length of stay per treatment day, total treatment time and days, concomitant treatment of underlying disease, referring physician/initiator, and discharge after/further treatment were recorded. Complex symptoms at the start of treatment (pain symptoms, gastrointestinal symptoms, genitourinary symptoms, ulcerating/healing wounds/tumours, respiratory/cardiological symptoms, neurological/psychiatric/psychological symptoms, other prominent symptoms) were then documented.
The following parameters were documented both on admission and on discharge from each type of care in the minimal documentation system MIDOS (pain, shortness of breath, nausea, vomiting, other nutritional problems/ loss of appetite, weakness/ weight loss/cachexia, depression, anxiety/confusion, excessive demands on family, sleep disturbance, fatigue, lymphoedema, constipation, wounds/ulcerations/decubitus, need for assistance with daily activities, nursing problems, condition on day of admission, pleural effusion/ascites, dysphagia/mucositis/dry mouth, neurological problems/spasticity/other, anemia, ileus/subileus); anaemia, ileus/subileus; diarrhoea).
ECOG (Eastern Cooperative Oncology Group) was also documented at both time points as well as Medication. ECOG which is used to assess the health status of patients and ranges from a score of 0 (complete health) to a score of 5 (death). It assesses the patient’s ability to perform their usual daily activities independently or with ambulatory support, their ability to work and the extent to which they need care
Measures and support during treatment days such as medication request form, sedation, nutrition, nutritional advice, transfusion therapy, continuous infusion by pump, pleural drainage, ascites drainage, catheter care, radiotherapy, tumour-specific therapy, nursing care, special positioning, wound care and rectal laxative measures were documented for each type of care.
The total time spent on treatment days was documented for the following types of contact: Physiotherapy; creative therapy (art and music); psycho-oncology; medical; and nursing. Invasive diagnostics/surgical intervention, diagnostics (radiology/CT/MRI, anamnesis/examination, sonography, laboratory, pathology), contact with non-specialist medical disciplines, patient education/decision making/relative education, pastoral care, care transfer/social counselling, hospice support, and place of death were also recorded.
Data on inpatients were obtained from the Orbis hospital information system used at the Aschaffenburg-Alzenau hospital; non-digitised data were taken from the analogue medical records that were kept in parallel.
For palliative day-care clinic patients, the analogue documentation of symptoms and services was used. This was kept for each patient in the form of a re-assessment/performance recording sheet and updated at each visit to the palliative day-care clinic. In addition, the analogue medical records kept in parallel were also used for day clinic patients.
The clinical routine data of palliative day-care clinic and palliative care unit patients were extracted into a Microsoft Excel® table from the digital hospital information system, Orbis®, or from medical paper records. The clinical routine data of specialised palliative home care patients were documented in the digital recording system ISPC®. For the purpose of data extraction, the head physician of specialised palliative home care accessed the clinical system and data were entered in an anonymised form.
Data Analysis
Data analysis was conducted using the statistical programmes SPSS® and R®. The distribution of the ratio-scaled variables was checked graphically with a Q-Q diagram and inferentially with the Shapiro-Wilk test. Since a normal distribution could not be found for most of the variables, non-parametric procedures were used in the inferential statistical analysis. In order to compare the three forms of care with regard to the nominally scaled variables, chi-square independence tests were carried out. This involved checking the preconditions. 25 After a significant chi-square independence test, pairwise Bonferroni-corrected Fisher exact tests were performed as post hoc tests. 26 The Kruskal-Wallis test was used to compare the three types of care in terms of at least ordinal scaled variables. Pairwise Bonferroni-corrected Wilcoxon rank sum tests were conducted as post hoc tests. The significance level was set at .05 to suggest statistical significance.
Results
Sociodemographic and Medical Characteristics
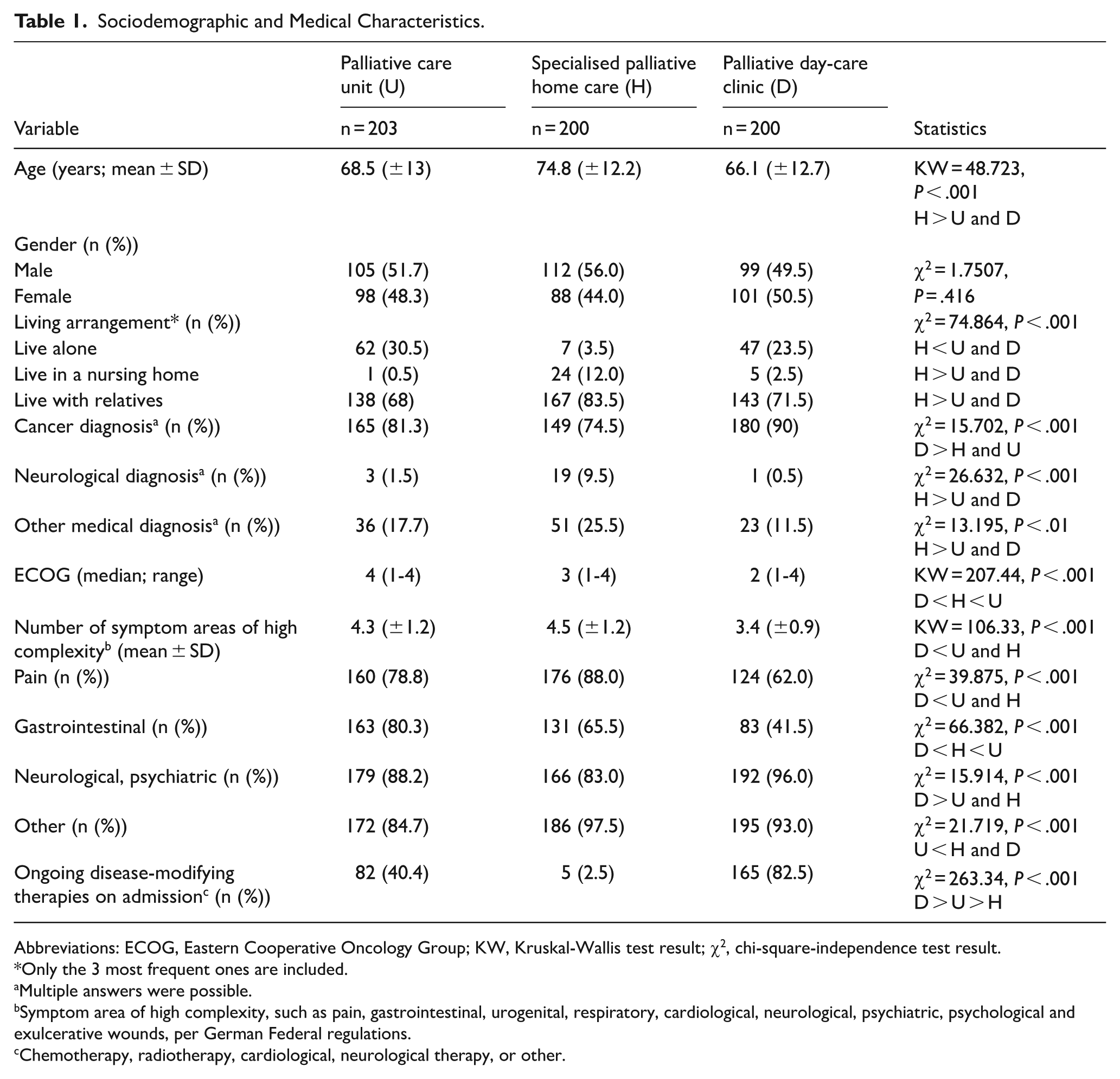
As can be seen from the comparison of sociodemographic and medical characteristics (Table 1), the palliative day-care clinic mainly sees cancer patients (90%) as does the palliative care unit (81.2%). By contrast, the specialised palliative home care team cares not only for cancer patients (74.5 %) but also for neurological (9.5 %) and other patients (25,5%, multiple diagnoses possible) mostly with internal diseases, all of whom are significantly older (average age 74.8 years compared to 66.1 years in the palliative day-care clinic and 68.5 years in the palliative care unit). The specialised palliative home care team also sees residents in nursing homes more frequently (12%) than the palliative day-care clinic and palliative care unit teams.
Patients treated in the day-care clinic had a significantly better ECOG status (with a median of 2 compared to 3 at home and 4 in the palliative care unit. Those in the day-care clinic were also more likely (90%) to have received concomitant treatment for the underlying disease, primarily tumour therapies (P < .001).
All patients in all three settings fulfil the German Palliative Care Association’s (DGP) official criteria 27 for needing specialised (vs general) palliative care, that is, showing at least one symptom area of high complexity. The day-care patients showed 3.4 different symptom areas of high complexity, which is significantly lower by one symptom area than the average in both the palliative care unit (4.3) and specialised palliative home care (4.5; P < .001). Interestingly, neuropsychiatric symptoms were significantly more frequent (96%) in palliative day-care than in the other settings.
Medical Procedure Intensity
On average, patients attended the palliative day-care clinic six times over a period of approximately 4 months (Table 2). This is significantly different from the palliative care unit, where patients stayed for an average of 13 days, and from the specialised palliative home care, where patients were seen for about 14 out of 28 days during the duration of care.
Medical diagnostics and interventions, such as radiological, physical, and sonographic examinations, laboratory and pathological diagnostics, and infusion, substitution and drainage procedures, were significantly more frequent among day-care patients than among home care patients (P < .001). In the palliative care unit, these were slightly lower than in the palliative day-care clinic, but not significantly so. Important symptom control, as indicated by the number of pain medication classes, was consistent across all three settings, with an average of approximately 1.6.
Admission and Discharge
Depending on the three settings, patients were admitted from different structures (Table 3): day-care patients were admitted most frequently from home through an oncologist (76%) or GP (15%), whereas palliative care unit patients were admitted by the general hospital (63.6%) or the palliative day-care clinic (16.8%). Specialised palliative home care patients originated from either a GP (91.5%) or an oncologist (7%).
Ninety-two per cent of patients died in specialised palliative home care, 61% in the palliative care unit and only 8% during the treatment period in the palliative day-care clinic. Most patients from day-care were admitted to the palliative care unit (35.5%) or specialised palliative home care (16.5%). In the case of 53 palliative day-care clinic patients, it was not possible to determine which form of care they switched to on the basis of the available documentation. For these patients, there was no further personal contact or information from relatives about the further course of treatment.
Discussion
This study compared three specialised palliative care structures within the same geographical region of Germany, analysing patient characteristics, treatments, and the role of a palliative day-care clinic. Our results show that the three care models differ in terms of their patient populations, time-based criteria and symptom burden—with the palliative day-care clinic treating younger patients in earlier stages of the disease, with a lower ECOG score and a less complex symptom burden.
Palliative care has traditionally focused on the end of life rather than on earlier phases of serious and incurable diseases. Modern palliative care aims to improve quality of life by preventing and alleviating physical, psychological, and spiritual suffering through early identification, comprehensive evaluation, and treatment targeting specific symptoms. For cancer patients, receiving early specialist palliative care has been shown to improve health-related quality of life, reduce depressive symptoms, and decrease the use of aggressive end-of-life care. It may also extend survival, as demonstrated by the landmark Temel et al 28 trial.
Other studies have shown improvements in health-related quality of life, 29 mood, symptom management, and end-of-life care outcomes.30,31
A randomised trial found that integrating palliative care with oncology care early on led to a better quality of life, mood, and coping skills, as well as more frequent end-of-life discussions for patients with newly diagnosed lung and gastrointestinal cancers. 32
Studies have shown that early integration can prevent and relieve suffering through the appropriate assessment and treatment of pain and other issues, such as psychological, social, and spiritual concerns. The World Health Organization (WHO) affirms that patients with chronic conditions may benefit from palliative care interventions in the early phases of their condition, alongside specific life-prolonging treatments. 33
However, systematic reviews, such as those by Haun et al 34 show that, while early palliative care improves quality of life, its effects on mood and symptoms are inconsistent, and there is no clear survival benefit. This is likely due to varying definitions and implementations. There is limited evidence for early palliative care in non-cancer illnesses, partly due to variable illness trajectories and a lack of standardised approaches. 35
A recent systematic review by Haroen et al 36 has shown that early palliative care reduces long-term psychological distress and improves health-related quality of life and satisfaction with care among patients. Therefore, early palliative care should be more broadly integrated into care at earlier stages to address patients’ psychological burdens.
Various methods for the early identification of patients who might benefit from palliative care have been proposed. These methods include disease-specific and general approaches based on clinical judgment, prognostic factors, and care needs. 35
The palliative day-care clinic Aschaffenburg-Alzenau, according to our results, offers specialised palliative care services with an emphasis on early integration. These services address gaps in care for patients with complex needs. The clinic offers less invasive procedures to minimise the need for hospitalisation and reduce the length of stays.
The palliative day-care clinic has the potential to delay hospitalisation during treatment, as demonstrated in our previous publication, 8 which may contribute to savings in healthcare costs. By sharing diagnostic and therapeutic resources within a single clinic, there is also the possibility of further cost reductions.
Although our data suggest a reduction in hospitalisations associated with palliative day-care clinics, we did not conduct a formal economic analysis. Consequently, any conclusions regarding potential cost savings should be considered tentative and are primarily based on observed trends and existing literature, rather than definitive evidence.
Additionally, the palliative day-care clinic enables patients to stay at home longer, 8 providing a more familiar and supportive environment in which to recover.
These results validate those by Cheung et al 37 who demonstrated that cancer patients receiving aggressive end-of-life care incurred costs that were 43% higher than those managed non-aggressively through palliative care integration. This approach may partially offset these costs and generate savings.
Our data lead to the hypothesis that more palliative day-care clinics are needed to provide GPs with the option of early integration and access to an array of services while also acting as a respite service for family carers. 8 Day clinics (hospice or palliative) have been described as a “transformative bridge to inpatient care, providing a connection, capable of allaying fears about inpatient palliative care and enabling earlier access to resources for care and support”, 27 which was also shown in our results where patients from the palliative day-care clinic were admitted to the palliative care unit or specialised palliative home care at a later point in time.
Patients with neuropsychiatric symptoms, were frequently seen by the palliative day-care clinic in Aschaffenburg-Alzenau. Maybe day clinics may stabilise home care especially in this patient group. For patients with non-malignant diseases, palliative care services can be utilised at any point along the disease trajectory and studies have shown a benefit for patients with, for example, non-malignant diseases such as MS or Parkinson’s disease.29,38,39 However, despite a very high symptom burden, many non-tumour patients do not receive the same level of palliative care as cancer populations. 40
Our results showed that patients in the palliative day-care clinic are, on average, almost 10 years younger than those in specialised palliative home care (SAPV). They enter the program earlier in the course of their illness with a lower symptom burden than patients in SAPV or hospital. Early integrative care is a priority at the palliative day-care clinic Aschaffenburg-Alzenau but is almost nonexistent at SAPV. Patients in the palliative day-care clinic have a better performance status and live more independently in their homes than SAPV patients. In the palliative day-care clinic, patients progress through the ECOG scale until further outpatient and day clinic care is no longer feasible, typically reaching ECOG 3 or 4. This is often followed by inpatient admission. While palliative tumour-specific therapy is being carried out, discussions about therapy goals, including information about prognosis and treatment options, as well as end-of-life decision-making, take place. The aim is to improve quality of life and avoid medically inappropriate aggressive therapies.
In palliative care, changes to analgesic therapy and the discontinuation of co-analgesics are common. Co-analgesics are often associated with anticholinergic side effects. The dose of medication is increased to alleviate symptoms (eg, antiemetics, benzodiazepines) and medication that is no longer necessary is reduced. In SAPV, analgesic therapy is also mainly intensified and unnecessary medication is reduced. Both in the inpatient setting and in the SAPV setting, medication is administered with the aim of controlling symptoms.
In the palliative day-care clinic, analgesic medication is often started first (WHO level 1 and also 3 in cases of severe symptoms) and, if necessary, other drug groups are added to the analgesic therapy depending on the type of pain. Therapy and further treatment are optimised in cases of existing comorbidities in patients in the early stages of the disease with differentiated body/symptom perception. However, symptom-relieving medications such as antiemetics, benzodiazepines, and adjuvants are also established.
In the palliative day-care clinic, invasive procedures such as punctures and drainage systems were most frequently performed as part of the low-threshold therapy offering. All three forms of care offer sonographic diagnostics, which are cost-effective, non-invasive, and readily available.
A systematic review has criticised the fact that the medical benefits of day-care clinics cannot be sufficiently proven. 15
Our retrospective data analysis of the three forms of care—day clinics, outpatient therapy, and SAPV—highlights and adds the medical benefits of day clinics.
Our results show that patients in the palliative day-care clinic can usually receive care at home for longer periods of time and that the palliative day-care clinic provides support in this regard, thereby stabilizing home care structures.
In addition to providing medical care for patients, the palliative day-care clinic also offers respite care for relatives by allowing patients to spend up to 5 days a week at the palliative day-care clinic. The palliative day-care clinic thus creates the possibility for patients who require intensive care in particular to remain in their own homes, possibly also because relatives feel supported and relieved by the structured processes. The aim is therefore not only the medical and psychosocial stabilisation of the patient, but also the relief of the families providing care. 8
Dierickx et al 41 showed that patients and family carers appreciated the social interactions at in the palliative day-care clinic, and that their symptoms were assessed whenever needed. The study also showed that a palliative day-care clinic enabled the patients to live at home for as long as possible, which was also found in our study (see above). By transferring patients from the day-care clinic to specialised palliative home care at a later stage, it was most often possible for patients to die at home if they wished. Therefore, as mentioned above, the palliative day-care clinic can act as an entry point to palliative care structures and a bridge to specialised palliative home care.
Strengths and Limitations
To the best of our knowledge, this is the first study that compares three different settings of specialised palliative care in one given geographical region in Germany where all three settings have been fully established over years. It uses a very comprehensive source of reliable secondary data. A power analysis for sample size calculation was not performed. Our study evaluated patient outcomes and therefore contributed to the rather scarce literature on this topic. In connection with the statistical evaluation and interpretation of the data, several parameters, however, were not evaluated due to a lack of clinical relevance and missing documentation in one or more of the comparison groups. Of course, the use of care settings very much depends on specific regional parameters, from the availability of services to the personal contacts involved. These data from one specific geographical region, therefore, only give a first insight and of course are not representative for the whole of Germany. Another limitation of this study is that we did not evaluate organisational factors or interventions nor any potential cost reductions. These are speculative until an economic evaluation is performed. However, our qualitative data, published elsewhere8, describe the benefits from the viewpoint of patients, caregivers, and GPs. While referral causes were not examined in this study due to data limitations, several factors may influence referral decisions: disease stage and prognosis, patient and family preferences and goals, the quality and timing of clinician communication, clinicians’ knowledge of and attitudes toward palliative care, the availability and accessibility of services, health system policies and funding, and cultural, religious, psychosocial, and spiritual needs across care settings. Testing these hypotheses requires data on the relevant variables and a design capable of causal inference, which could be the focus of future research.
Conclusions
Our findings reveal significant differences between the three palliative care models. The palliative day-care clinic primarily treats younger patients with fewer symptoms at earlier stages of the disease, as opposed to the specialised home care and inpatient unit. These variations emphasise the importance of tailoring palliative interventions to patient needs and disease progression to facilitate appropriate resource allocation and care planning. Understanding these differences can improve the development of integrated palliative care pathways, ultimately enhancing patient-centred outcomes in various care settings.
Based on the routine data analysis, the findings suggest that the palliative day-care clinic may serve as a valuable setting for the potential implementation of early, integrated, and specialised palliative care.
The palliative day-care clinic’s capacity to perform certain invasive interventions and diagnostics could contribute to delaying or possibly reducing the need for hospital stays, as was shown in Müller et al. 8 Additionally, the clinic might support patients in remaining in their own homes for a longer period, which could be beneficial for both patients and the healthcare system. However, further research would be necessary to more definitively establish these outcomes and the optimal timing of such interventions.
Further Research
Further research is needed to validate these findings and make them more representative, as they are currently based on one specific geographical region in Germany. This must include a full economic evaluation to demonstrate not only that patients and their families benefit, but also quantify the impact on the healthcare system. Future research could examine organisational-level determinants and interventions to establish whether system-level changes improve patient outcomes.
Footnotes
Acknowledgements
The authors would like to thank all the staff members involved in this study from the palliative day-care clinic and the palliative care unit at Klinikum Aschaffenburg-Alzenau, as well as the Hospiz- und Palliativ-Team Bayerischer Untermain. Further thanks go to the Hospizverein Aschaffenburg.
Author Contributions
Stephanie Kunkel: Writing—Review and editing, writing—original draft, data curation, investigation, formal analysis, validation, methodology, conceptualisation. Julia Strupp: Project administration, funding acquisition, supervision, writing—review and editing, writing—original draft, visualisation, resources, formal analysis, methodology, conceptualisation. Kevin Liu: Writing—review and editing, formal analysis, validation, methodology. Alfred Paul: Writing—review and editing, resources, software. Johannes Best: Writing—review and editing, resources. Anne Mueller: Writing—review and editing, resources. Almut Foeller: Data curation, validation, conceptualisation. Raymond Voltz: Project administration, funding acquisition, writing—review and editing, methodology, conceptualisation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from the Aschaffenburg-Alzenau Clinic.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.