
Abstract
Background
The Palliative Care Early and Systematic (PaCES) program implemented an early palliative care pathway for advanced colorectal cancer patients in January 2019, to increase specialist palliative care consultation and palliative homecare referrals more than three months before death. This study aimed to understand the experience of patients with advanced colorectal cancer and family caregivers who received early palliative care supports from a specialist palliative care nurse and compared those experiences with participants who experienced standard oncology care prior to implementation of early palliative care.
Methods
This was a qualitative and patient-oriented study. We conducted semi-structured telephone interviews with two cohorts of patients with advanced colorectal cancer before and after implementation of an early palliative care pathway. We conducted a thematic analysis of the transcripts guided by a Person-Centred Care Framework.
Results
Seven patients living with advanced colorectal cancer and five family caregivers who received early palliative care supports expressed that visits from their early palliative care nurse was helpful, improved their understanding of palliative care, and improved their care. Four main themes shaped their experience of early palliative care: care coordination, perception of palliative care & advance care planning, coping with advanced cancer, and patient and family engagement. These findings were compared with experiences of 15 patients and seven caregivers prior to pathway implementation.
Conclusion
An early palliative care pathway can improve advanced cancer care, and improve understanding and acceptance of early palliative care. This work was conducted in the context of colorectal cancer but may have relevance for the care of other advanced cancers.
Background
Patients with advanced cancers often experience high symptom burden, and trouble coping with their illness (Greer et al., 2013; Kotronoulas et al., 2017). Patients with advanced colorectal cancer specifically experience high symptom burden such as pain, and other challenges such as obstruction and nutrition (Delisle et al., 2019). For patients with advanced cancers, early palliative care involvement has been associated with reduced hospitalizations, lower healthcare utilizations (Delisle et al., 2019), more community-based care consistent with patients preferences (Maltoni et al., 2016; Morrison et al., 2011), higher quality of life (Bakitas et al., 2009; Haun et al., 2017; Temel et al., 2010), and patient and family caregiver satisfaction (Kavalieratos et al., 2016; Prescott et al., 2017; Temel et al., 2010). Palliative care has been defined as patient and family centred care that improves quality of life and addresses physical, emotional, social, and spiritual needs of patients (Arora et al., 2017). A palliative approach to care is recommended to optimize patient outcomes (Canadian Institute for Health Information, 2018; Ferrell et al., 2017; Kaasa et al., 2018; Simon & Sinnarajah, 2018; Ziegler et al., 2018), and organizations recommend early integration eight weeks into diagnosis of advanced cancer (Ferrell et al., 2017). However, access and delivery of palliative care varies across jurisdictions (Canadian Institute for Health Information, 2018) and those with advanced cancers are often referred late to palliative care or not at all (Earp et al., 2021; Simon & Sinnarajah, 2018; Wentlandt et al., 2012). With sufficient palliative care resources, earlier referral to palliative care is possible (Hausner et al., 2021).
The few qualitative studies that explored impact of early palliative care on patients and families, report positive experiences including improved communication, care coordination, patient engagement, and advance care planning discussions (Fliedner et al., 2019; Hannon et al., 2017; Maloney et al., 2013). Only one of these studies compared patients with and without experience of a palliative care intervention, and they found intervention participants’ felt supported, gained self-management skills, and were empowered in participating in their care (Maloney et al., 2013). However, their intervention was conducted primarily over the phone as most patients were unable to travel to the clinics for the in-person consultations. The authors recommended the need for community-based palliative care for patients. Within our cancer center, an early palliative care pathway was implemented in 2019 for advanced colorectal cancer, led by the addition of specialist palliative care nurse consultations in addressing the following components: understanding of illness and coping with advanced cancer, advance care planning and shared decision making, attending to symptoms and functional status, and coordination of care (Figure 1) (Temel et al., 2010). This study was a follow up to our previous publication that informed the development of the early palliative care pathway, through understanding the experiences of advanced colorectal cancer patients as they received standard oncology care (without early palliative care supports) (Ahmed et al., 2020). We identified gaps in their cancer care that included poor communication with patients and among healthcare providers, misunderstanding of palliative care, and lack of advance care planning discussions (Ahmed et al., 2020). The implementation of an early palliative care pathway with the introduction of a specialist palliative care nurse was meant to address these gaps in cancer care. Thus, the present study aimed to understand the experiences of advanced colorectal cancer patients and caregivers after receiving early palliative care support from a specialist palliative care nurse, and then compare their experiences to those patients who previously received standard oncology care prior to implementation of early palliative care.
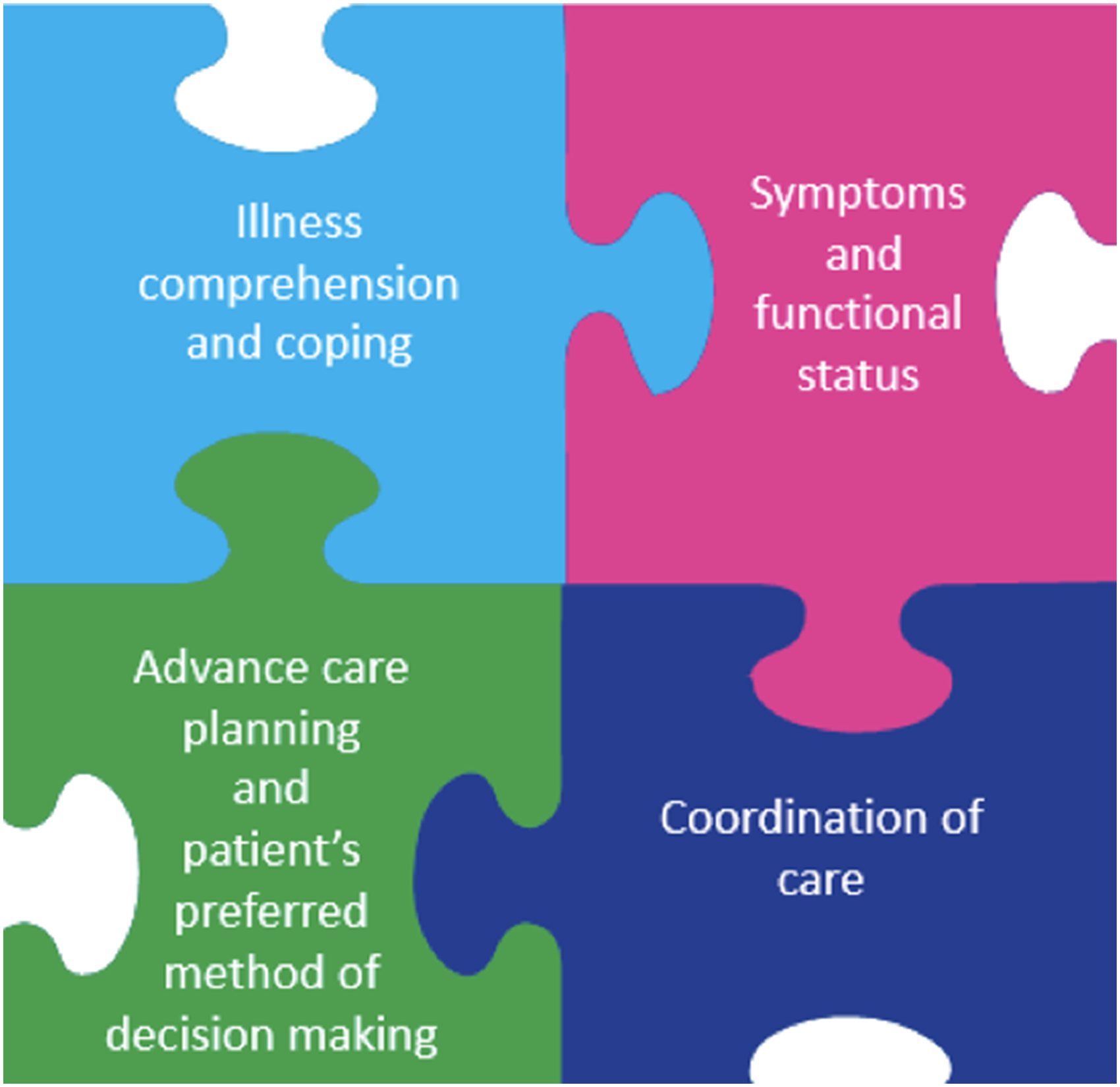
Early palliative approach to care.
Methods
Study design
We conducted a qualitative patient-oriented study, of patients and family caregivers who experienced care after the implementation of an early palliative care pathway (described below) for advanced colorectal cancer. This study was patient-oriented as we engaged patients and families as partners to inform the research project (Canadian Institute for Health Research, 2014). In this case, patient and family advisors were members of the project team, were involved from the start of the project in grant development, they informed the development of interview guides, attended and participated in team meetings.
We employed semi-structured telephone interviews. We chose telephone interviews because they were suggested by patients who found comfort and convenience sharing their experiences over the phone (Ahmed et al., 2020). The interview guide was developed in collaboration with palliative care specialist clinician-researchers and three patient and family advisors on the team. The interview guide consisted of questions on the experience of early palliative care supports received, introduction and timing of palliative care, coping with cancer, discussions about advance care planning and end of life planning (Appendix A). The Health Research Ethics Board of Alberta Cancer Committee provided ethics approval (ID: HREBA.CC-18-001, February 2018).
Description of the palliative care early and systematic (PaCES) care pathway
All patients interviewed in this study had received early palliative care through implementation of the PaCES, an integrated early palliative care pathway for advanced colorectal cancer. The PaCES pathway was a province-wide initiative, that engaged multiple stakeholders (clinicians, knowledge end users, researchers and patient and family advisors). The PaCES pathway followed an integrated model of care, through early referral of advanced cancer patients to specialist palliative care nurse consultative visits and palliative homecare supports more than three months before death. The early palliative care pathway for advanced colorectal cancer (implemented in January 2019) included guidance for clinicians caring for patients and a process for screening of patients likely to benefit from early palliative care (metastatic cancer / starting second line chemotherapy / no systemic therapy options / high symptom distress (Edmonton Symptom Assessment System (ESAS) scoring of >7) / deteriorating function / patient request). The early palliative care pathway also consists of identifying patient needs, primary palliative care management of unmet patient needs and having advance care planning discussions with patients and family caregivers (by family physicians, oncologists, and nurses) (Simon & Sinnarajah, 2018). Care coordination and communication was facilitated by a templated “shared care letter” from the oncologist to the family physician and patient, which outlined the role of each healthcare provider in palliative care (Alberta Health Services, 2019b; Simon & Sinnarajah, 2018). The process encouraged timely referral to a specialist palliative care nurse to provide support and ensure all elements of an early palliative approach to care were addressed (Alberta Health Services, 2019a; Simon & Sinnarajah, 2018). Most of the palliative specialist nurse's visits occurred in the patient's own home, with templated consult notes shared with both the oncologist and family physician and made referrals to homecare as needed. Standard palliative homecare with functional and psychosocial supports remained available to all patients with these needs before and after the pathway implementation (Figure 1).
Recruitment and data collection
Eligible interview participants were adults (>18 years) with advanced colorectal cancer, who had at least one visit with the specialist palliative care nurse. Additionally, caregivers were also invited to participate. A caregiver was defined as an adult relative or friend, whom the patient described as their primary caregiver (someone providing unpaid assistance to the patient). The caregiver did not need to live in the same residence as the patient. Participants were informed about the study by the palliative care nurse during a visit in-person or on the phone. Participants completed a ‘consent to contact’ form if interested in being interviewed. They were followed up by the researcher for more information about the study (include sending the consent form via email) and to schedule an interview time. Both types, dyad participants (patient and their caregiver, but interviewed separately), and non-dyad participants were recruited. Participants were offered a $20 gift card as compensation for their participation. Interviews were conducted with consenting participants from September 2019 to February 2020 by the qualitative researcher (MSc), and were audio recorded and transcribed. Interviews ranged from 20 to 70 min, that included obtaining informed consent as well as demographic information.
Data analysis
We conducted a thematic analysis of the transcripts to allow for the identification of themes and patterns, using the six-step thematic analysis process described by Braun and Clark (Braun & Clarke, 2006). We utilized the qualitative analysis software, NVIVO to aid in data analysis (QSR International, 1999). Coding was performed by two study researchers (with qualitative research background, MSc and BCr), using a mix of deductive, inductive, and iterative coding strategies. The domains from the Person-Centred Care (PCC) Framework (Santana et al., 2018) were used to guide deductive analysis because of the patient and family-centered nature of palliative care. Specific domains from the PCC framework, and codes developed from the previous cohort interviews informed codes for the interviews conducted in this study. Domains of person-centred care include cultivating communication, access to care, and engaging patients in managing their care (Santana et al., 2018). However, coding was also inductive as new codes were identified from the data that were not already included in the coding book. The coding process was iterative because when a new code was identified, the transcripts were read once again to ensure codes were not missed. Transcripts were read multiple times to generate codes and differences in coding were resolved through discussions between the two researchers who coded the data. After organizing codes into themes, they were presented to the research team, including patient and family advisors for feedback. We employed strategies to increase credibility, such as member checking (asking participants to clarify responses during the interviews), and peer debriefing between team members to discuss themes identified. Afterwards, themes identified were compared to the themes from the previous study conducted, including identifying similarities and differences in the findings. Complete records of the start of the research project to the end were kept, with transcripts and notes. This audit trail process was important in providing a transparent research process and increasing dependability.
Findings
A total of 12 participants (seven patients, five caregivers) were interviewed. There were two dyad pairs interviewed (one spouse pair, and one child-parent pair), however each participant was interviewed separately. Participant age ranged from 36 to 86 years. Interviews were conducted eight months after implementation of early palliative care support. At the time of the interview, patients reported having received palliative care support from one month to 12 months.
Patient and family caregiver experiences with early palliative care supports can be summarized into the following main themes: (1) Care Coordination, (2) Perception of Palliative Care & Advance Care Planning, (3) Coping with Advanced Cancer, and (4) Patient and Family Engagement. Associated sub-themes were identified and summarized in Tables 1 and 2 with supportive quotes. Figure 2 presents a visual summary of the findings.
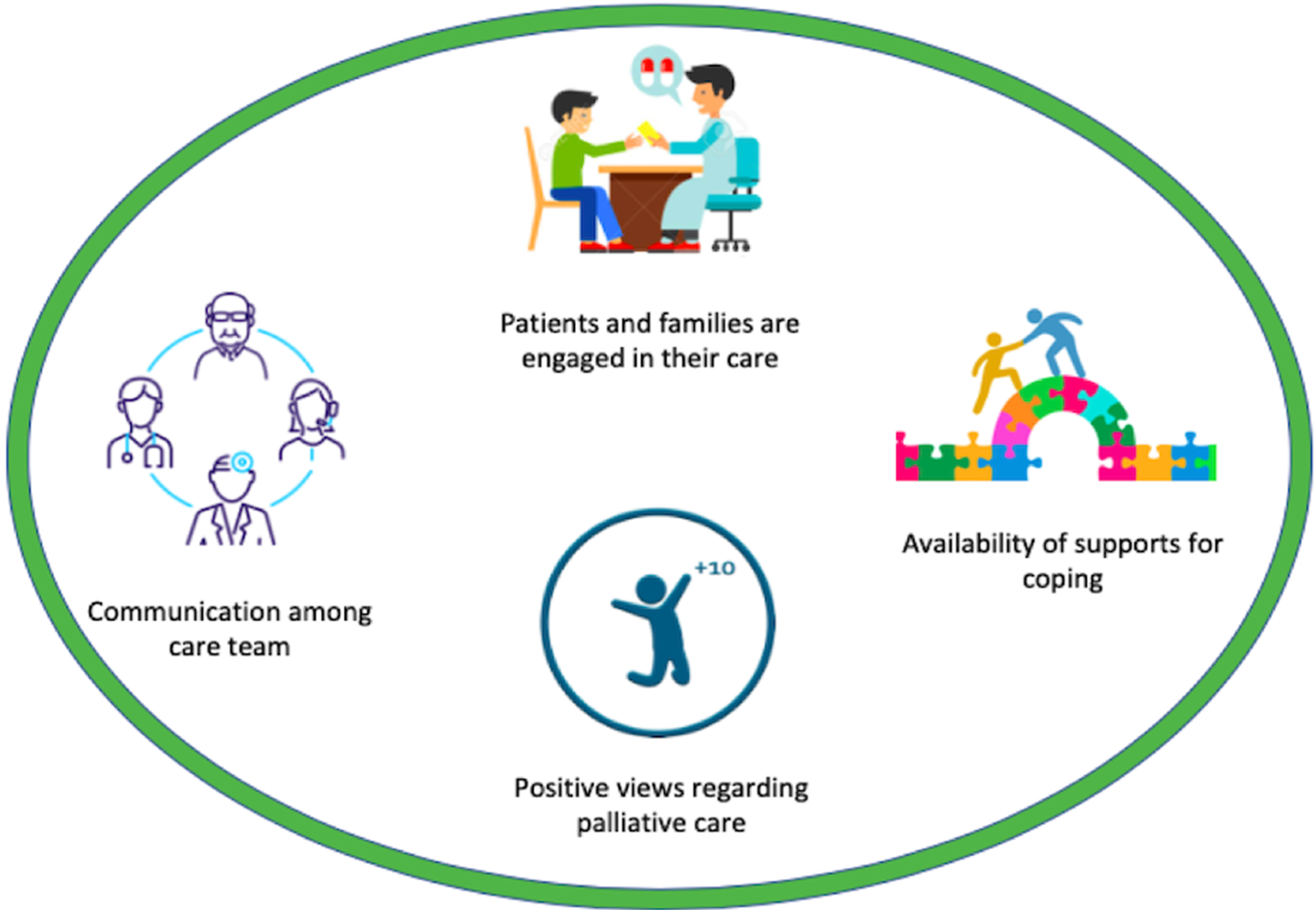
Patient and family caregiver experiences after early palliative care.
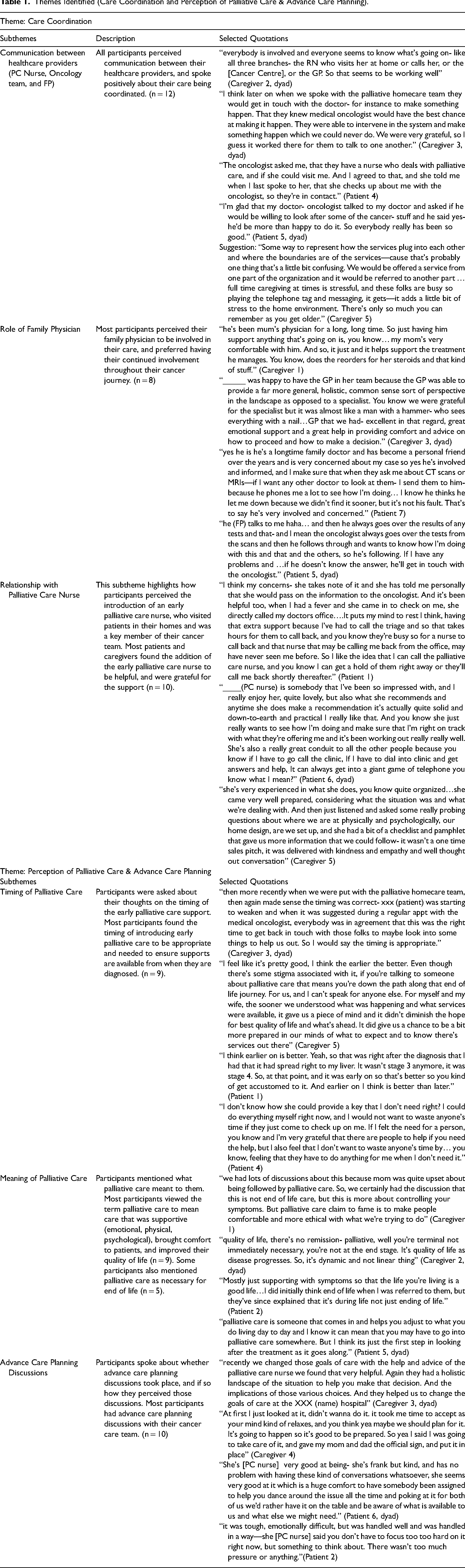
Themes Identified (Care Coordination and Perception of Palliative Care & Advance Care Planning).
Themes Identified (Coping with Advanced Cancer & Patient and Family Engagement).

Care coordination
Within the theme care coordination, we identified the following subthemes: communication between healthcare providers, role of family physician, and relationship with palliative care nurse. Participants mentioned their healthcare providers worked together to provide their care. Most participants mentioned instances where they perceived teamwork and communication between the care team, especially between the oncologist, palliative care nurse, and family physician. Participants referred to the palliative care nurse as someone who aided communication and helped with coordination. One caregiver perceived communication between their palliative care nurse and oncologist as necessary to provide patients with the best quality of life: “We don't always see the direct interaction but we do get the feedback that the care staff (palliative care team) has been in touch with the doctor (oncologist)[…]The doctor (oncologist), will mention—she reviewed the palliative care report and understands the circumstance, a little bit more thorough. I think that's good right now, your primary doctor understands the specialty treatment, the treatment is for the physical too, but if your doctor also understands the mental—how your patient's doing […] better prepared to design the treatment that's going to provide the best quality of life.” [C5]
The family physician was another healthcare provider that most participants mentioned as an important member of their care team. Most participants saw their family physician and wanted their family physician to be informed about their cancer care. The role of the family physician was identified as someone who provided emotional support, managed pain, ordered prescriptions, went over reports during appointments received from other healthcare providers (bloodwork, scans, etc), and managed other healthcare conditions. One patient mentioned her preference for involvement of her family physician: “Yes, he's involved and informed, and I make sure that when they ask me about CT scans or MRIs—if I want any other doctor to look at them, I send them to him. Because he phones me a lot to see how I’m doing.” [P7]
Patients and family caregivers developed a bond with their palliative care nurse and communicated with her about their care. Participants mentioned the palliative nurse was a liaison to other services and helped to coordinate their care. One family caregiver described the care provided by the palliative care nurse as genuine and thorough: “She seems to have a genuine care for her, takes notes and asks a lot of questions. She touches my mom, basically to see how she's doing—her hands, with the numbness and cracks in her fingers, and in her last visit my mom told her she had trouble with bowel movements so and she’ll kind of check on my mom and rub her stomach and refer some meds she should take. She’ll talk to the doctor about having some new meds.” [C4]
There were also opportunities for improvement in care coordination identified by two family caregivers. One family caregiver brought up a recommendation for the care team to outline the specific responsibilities of each service that is introduced to mitigate confusion for patients and families. Another family caregiver described the care as being coordinated, until the last day of the patient who passed away without being able to reach the early palliative care nurse that day, resulting in the patient dying in hospital.
Perception of palliative care and advance care planning
The addition of a palliative care nurse in cancer care impacted participants’ perception of palliative care and advance care planning. Within perception of palliative care & advance care planning, we identified the subthemes: timing of palliative care, meaning of palliative care, and advance care planning discussions. Most participants found the timing and introduction of early palliative care to be appropriate, and participants emphasized early integration of palliative care to be very beneficial for patients and caregivers. One caregiver mentioned early palliative care did not diminish hope for his wife's care, but rather reassured them they were going to receive care to improve quality of life: “For myself and my wife, the sooner we understood what was happening and what services were available, it gave us a piece of mind and it didn't diminish the hope for best quality of life and what's ahead. It did give us a chance to be a bit more prepared in our minds of what to expect and to know there's services out there” [C5]
Most participants viewed the term palliative care to mean care that was broad, supportive, and improved quality of life. For some participants, their view of palliative care changed after speaking to the palliative care nurse. One patient noted the change in perception: “Mostly just supporting with symptoms so that the life you’re living is a good life […] I did initially think end of life when I was referred to them, but they’ve since explained that it's during life, not just ending of life.” [P2]
However, there were still some participants that found the term held stigma and associated it with end of life. One caregiver did not consider the support his mom received as palliative care, but rather as preparation for palliative care.
For most participants, the palliative care nurse facilitated advance care planning discussions. Most participants had discussed their goals of care, wishes and preferences, values, and end of life planning with their care team (including with family members). Participants described discussions with their palliative care nurse were helpful and they did not feel pressured during the process. One caregiver described the process of revisiting their goals of care: “Recently we changed those goals of care with the help and advice of the palliative care nurse we found that very helpful. Again, they had a holistic landscape of the situation to help you make that decision. And the implications of those various choices” [C3, dyad]
However, for two patients, they did not feel they needed to have advance care planning discussions early and had not yet engaged in any discussions. One of the patients associated palliative care and advance care planning with end of life care, which may have impacted his readiness for advance care planning, “It's difficult for me to say where I would end my life. How or where I would like to be or go and so on but none of that, I don't have any interest in that […] To end in a hospital that's okay for me I told that, if it's at home that's okay. I just cannot plan that. It's something I don't believe I have any control over—planning” [P4]
Coping with advanced cancer
We identified the following subthemes within coping with advanced cancer: support from family and friends, support from healthcare system, strength in faith, and value in independence. Some participants mentioned how their palliative care nurse specialist facilitated access to different resources such as a psychologist. Participants appreciated both the informal and formal supports they received throughout their care. One patient described respectful and personalized care from two healthcare providers, the pharmacist and dietician as they helped her with the side effects from chemotherapy: “I wasn't able to eat very well when I was on chemo[…]I contacted the dietitian and she was super helpful[…]She sent me recipes, she talked to me over the phone and the pharmacy—after the chemotherapy which was really powerful, I had neuropathy in my feet[…]she [pharmacist] would call every week to see how I was doing with the neuropathy, what was changing. She was absolutely fantastic.” [P7]
Some participants also talked about valuing their independence and being able to do things on their own. For one patient, this meant he did not feel he needed the support from the palliative care nurse and homecare, due to being able to work on his own and having the support of his wife.
Patient and family engagement in care
We identified the following subthemes within this theme: taking initiative and being informed, and patient advocacy. Most participants described being well informed about their cancer care, and services offered to them, even before seeing the palliative care nurse. This information helped participants to make decisions about their care. Some participants talked about feeling engaged in their care and supported in decision-making. For instance, one patient mentioned the palliative care nurse supported her in the decision-making process: “He's [husband] here pretty much every visit that she comes for so he can be part of the discussion […] She's [palliative care nurse] very good at sharing all kinds of information, very good at giving us space to make decisions. There's never been any question on who's making that decision. We’re given time, we’re given space, and we can ask questions. I’ve stumbled into a team with really good folks” [P6, dyad]
Some participants also mentioned the importance of advocating for their care, and some patients and caregivers recounted past experiences of feeling pressured into decisions on treatments. Some family caregivers brought up the need for a patient advocate/navigator in the healthcare system from the start of the patient journey, especially if patients didn't have a support system: “When I’m dictator, there will actually be a patient navigator who actually acts like that who can navigate the system, and has a holistic view of the landscape and can say this, now we know who you are and what your wishes are” [C3, dyad
Comparison with patient experiences prior to palliative care pathway
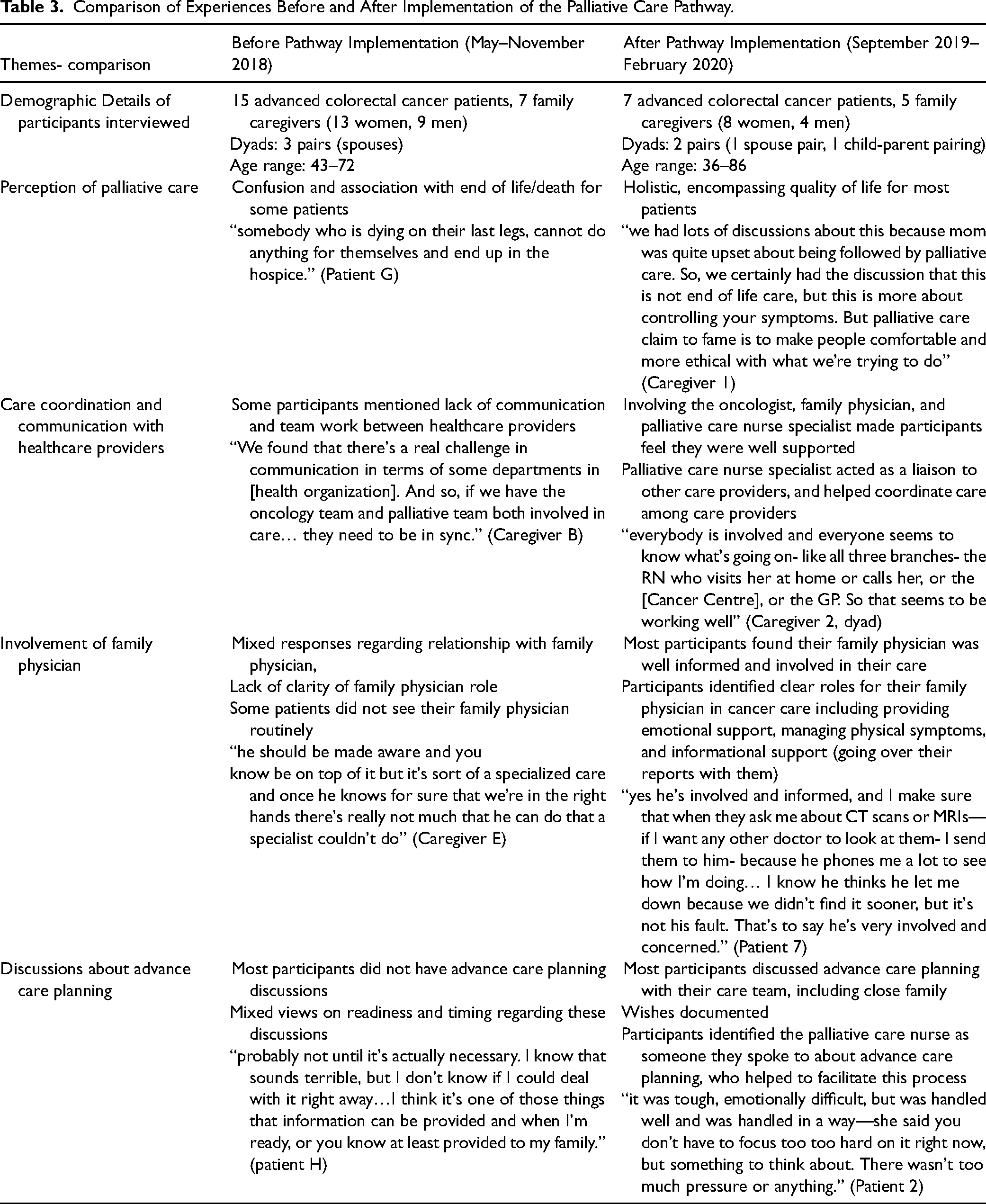
We compared these interviews to those conducted by our team with another cohort of patients living with advanced colorectal cancer receiving care prior to implementation of the early palliative care pathway (Ahmed et al., 2020). Demographic details of both interviews and the comparison of the experiences before and after implementation of the early palliative care pathway are summarized in Table 3. The experiences of participants who received early palliative care support from a specialist palliative care nurse were different than those described by a cohort interviewed prior to pathway implementation. From our interviews, we identified improvements in care coordination. Involving the oncologist, family physician, and palliative care nurse specialist made participants feel they were well supported. The role of their family physician was more readily perceived and valued. Participants interviewed prior to the palliative care pathway expressed frustrations with poor communication among care providers. Whereas, after the implementation, participants perceived the palliative care nurse as a liaison, who facilitated and supported access to care and ensured patients received timely care. Additionally, there were also differences in how participants perceived palliative care and advance care planning between the two participant cohorts, with most participants who received care after implementation, described palliative care as supportive and encompassing quality of life. Participants identified the palliative care nurse as someone they spoke to about advance care planning, who helped to facilitate this process. After implementation, more patients reported discussing advance care planning with their care team. In both cohorts, patients and family caregivers mentioned being engaged in their care, and valuing their independence and autonomy.
Comparison of Experiences Before and After Implementation of the Palliative Care Pathway.
Discussion
This study described the experiences of patients with advanced colorectal cancer and caregivers who received early palliative care and compared those experiences with another cohort of patients and caregivers who received standard oncology care prior to implementation of early palliative care. The four main themes identified in the cohort who received early palliative care (care coordination; perception of palliative care and advance care planning; coping with advanced cancer; and patient and caregiver engagement) aligned with domains included in the Person-Centred Care Framework such as communication, care coordination, and patient engagement in care (Santana et al., 2018). Participants in our study described a positive patient centred relationship with the palliative care nurse, and described the interactions as supportive and caring. Patient contact with early palliative care nurses have been described as supportive and helpful in other studies conducted as well (Fliedner et al., 2019; Maloney et al., 2013). Also, after the implementation of the early palliative care pathway, we identified improvement in care coordination. Similarly, in Hannon et al.(Hannon et al., 2016) early palliative care integrated with oncology care improved the coordination of care. In their study, participants described the relationship with their palliative care physician as comfortable and personal (Hannon et al., 2016). The palliative care nurse fulfilled a key role in care coordination, supporting patients through their cancer trajectory. The role of the nurse was critical in enhancing communication amongst other clinicians, patients and caregivers, and improving patient and caregiver understanding of palliative care. Improved communication between patients and healthcare providers was also found in other studies integrating palliative care (Akyar et al., 2018; Rugno et al., 2014). The integration of early palliative care through specialist palliative care teams (such as nurse specialists) in cancer care was found to be beneficial for patients in our study. Integrated care models have been recommended by Hui & Bruera (Hui & Bruera, 2015) as it ensures standard access to early palliative care concurrent with cancer care.
Most participants had an improved understanding of palliative care after discussions with the palliative care nurse, similar to the study by Fliedner et al. (Fliedner et al., 2019). However, few participants noted that the term palliative care carried stigma, as did Zimmermann et al. (Zimmermann et al., 2016). The study by Hannon et al. (Hannon et al., 2017) also found some participants perceived palliative care negatively, impacting how comfortable they were with palliative care supports. Negative perception of palliative care can be a barrier to effective referral.
The importance of the role of the family physician in their cancer care was clearer to participants interviewed after the early palliative care pathway. This finding was similar to a survey conducted in Germany where 85.5% of patients wanted their family physician to be informed about their cancer therapy on a regular basis, and were supported by their family physician in cancer care (Lang et al., 2017). In Zimmerman et al. (Zimmermann et al., 2014) early palliative care trial, where routine communication with family physician was a component of the intervention, patient satisfaction with care significantly improved as well. In Canada, this shared care model for cancer care is recommended, with some oncology programs involving family physicians in integrated palliative care (Fassbender & Watanabe, 2015).
Engaging patients and families in their care was important to the delivery of early palliative care. Some participants recounted past experiences of feeling pressured in making decisions, and mentioned lack of early support to navigate the cancer care system. Advance care planning discussions were an important component of an early palliative care approach, and most participants interviewed after pathway implementation positively described their experiences with these discussions. Similarly, other studies that delivered early palliative care supports also found advanced cancer patients were able to engage in discussions about advance care planning and found them beneficial (Fliedner et al., 2019; Hannon et al., 2017).
Strengths and limitations
This study provided in-depth understanding of the care experiences of patients and family caregivers, identified aspects of the PaCES early palliative care pathway that were beneficial, and aspects of care that they valued. A strength of this study design was that it allowed for comparison of care experiences before and after implementation of the early palliative care pathway, and identified potential impact of the pathway from the perspective of patients. Another strength was that all patients were similar in their health condition, advanced colorectal cancer, which affects both sex and genders equally. A potential limitation of this study was that a different cohort of participants were interviewed before implementation of the care pathway and after, so we could not observe differences in perceptions and experiences among the same participants. However, our participants had an advanced cancer diagnosis (with a prognosis of 6 to 24 months), therefore it was not possible for the same participants to participate in the time frame of the two studies. Additionally, participating in the first study interview included hearing a definition of palliative care that could be seen as influencing participants’ subsequent perceptions, therefore it was important to interview a different set of participants after implementation of the care pathway to mitigate interview influence on participant views. During recruitment, the specialist palliative care nurse informed potential participants about the study, which may have resulted in those with a positive bias towards their experiences participating. Through our comparison, we identified differences and similarities in the care experiences of the two cohorts of participants, rather than understanding whether care experiences have changed. Qualitative studies do not seek to be generalizable, and the experiences of early palliative care may be different for other cancers and populations.
Conclusions
Early palliative care delivered by a specialist palliative care nurse may improve advanced cancer care, including an improved understanding and acceptance of early palliative care. This study used a patient-oriented approach in the design and in identifying what matters to patients and family caregivers in early palliative care. This study was novel in comparing experiences of patients and family caregivers before and after implementation of an early palliative care pathway for advanced colorectal cancer in a health system. The sustainability of integrating early palliative care in cancer care is currently being studied within our cancer centre. Different cancer centres need to consider various factors when implementing an integrated model including the availability of staff and resources and patient needs. Future studies could use a similar method to examine whether this care pathway can be implemented in other cancers and non-cancer diseases and compare the experiences of patients across different conditions.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621221079534 - Supplemental material for Patient & Caregiver Experiences: Qualitative Study Comparison Before and After Implementation of Early Palliative Care for Advanced Colorectal Cancer
Supplemental material, sj-docx-1-cjn-10.1177_08445621221079534 for Patient & Caregiver Experiences: Qualitative Study Comparison Before and After Implementation of Early Palliative Care for Advanced Colorectal Cancer by Sadia Ahmed, Syeda Farwa Naqvi, Aynharan Sinnarajah, Gwen McGhan, Jessica Simon and Maria J. Santana in Canadian Journal of Nursing Research
Footnotes
Acknowledgments
The authors would like to acknowledge the support of our patient and family advisors: Alice Campbell, Karen Leaman, and Nicole McKenzie. We would like to acknowledge the support of the Patient Partner Lead of the Strategy for Patient Oriented Research (SPOR) Patient Engagement Platform: Sandra Zelinsky, for her advice on interviewing research participants, and feedback on the interview guide. Additionally, the authors would like to acknowledge the support of Janet Vandale and Dr.Patricia Biondo in the recruitment of study participants and feedback on study. This work was presented at the 27th Annual Conference of the International Society for Quality of Life Research in October 2020 (virtually).
Availability of data and material
This study analyzes qualitative data and the participants did not consent to have their full transcripts made publicly available. No additional data.
Author's contributions
AS, JS, and MS conceived and designed study. SA and SFN worked on the analysis and interpretation of findings, with feedback from AS, JS, GM, and MS. SA drafted the article, and all authors (SFN, AS, GM, JS, and MS) provided critical feedback and approved the version to be published.
Compliance with ethical standards/ethics approval
The Health Research Ethics Board of Alberta Cancer Committee gave ethics approval for the proposed study (ID: HREBA.CC-18-0013) on February 2018.
Consent to participate
Interview participants provided informed consent to participate in the study.
Consent for publication
Not applicable
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SA was supported by the Alberta Strategy for Patient Oriented Research (SPOR) Graduate Studentship (co-sponsored by Alberta Innovates and CIHR) & Cumming School of Medicine, University of Calgary. AS and JS are supported by a Canadian Institute of Health Research and Alberta Health grants. MS is supported by a Canadian Institute of Health Research Project grant.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
![]() ) that is aiming to improve patient and health system outcomes through enhancing the timely integration of palliative and cancer care. She also works as a palliative care physician consultant, predominately in acute care, and as a physician consultant for Advance Care Planning and Goals of Care for Alberta Health Services, Calgary Zone.
) that is aiming to improve patient and health system outcomes through enhancing the timely integration of palliative and cancer care. She also works as a palliative care physician consultant, predominately in acute care, and as a physician consultant for Advance Care Planning and Goals of Care for Alberta Health Services, Calgary Zone.
![]() ).
).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.