
Abstract
Introduction:
The long-term impact of COVID-19 on Quality of Life (QoL) is a growing concern, particularly in low- and middle-income countries (LMICs) like Nepal. However, there is limited evidence on how post-COVID-19 health conditions affect daily life in Nepalese communities. This study assesses the QoL among COVID-19 survivors in Pokhara Metropolitan City, Nepal.
Methods:
A community-based cross-sectional study was conducted among 271 post-COVID-19 patients discharged from hospitals in Pokhara Metropolitan City. Participants were selected using systematic random sampling, and data were collected through face-to-face interviews using the WHOQOL-BREF questionnaire. Multivariable logistic regression was applied to determine factors associated with QoL.
Results:
The mean HRQoL score was 61.29 ± 12.54, with the physical health domain scoring the highest (65.58 ± 21.53) and the environment domain the lowest (57.50 ±11.52). Among participants, 82.3% had good QoL, while 17.7% had poor QoL. Living in a nuclear family (aOR = 2.61, 95% CI: 2.14–6.00), being employed (aOR = 4.10, 95% CI: 1.87–9.21), and engaging in regular exercise (aOR = 3.32, 95% CI: 1.36–8.06) were significant positive factors for good QoL among post-COVID-19 patients. Conversely, chronic disease was the strongest negative predictor of QoL, with those without chronic conditions being 6.15 times more likely to report good QoL (aOR = 6.15, 95% CI: 2.65–14.24).
Conclusion:
COVID-19 survivors in Nepal experience varying degrees of QoL impairment, particularly in the environmental and psychological domains. Employment status, exercise, and family structure play crucial roles in post-COVID well-being, while chronic illness remains a significant barrier.
Introduction
The COVID-19 pandemic, caused by the novel coronavirus SARS-CoV-2, rapidly emerged as a global health crisis, affecting millions across all age groups and genders. Since its onset, the pandemic has resulted in a staggering global death toll of approximately 6 million, disrupting healthcare systems, economies, and everyday life throughout the world.1 –4 In Nepal, although the initial rate of infection was relatively slow, a surge in cases occurred from June 2020, leading to the first and second waves between June 2020 and August 2021.4,5 By June 2023, over 1 million Nepali citizens were estimated to have been affected, with an official death toll of 12,031. 6 These figures reflect the extensive spread of the virus across the nation.
Global and national efforts to combat the COVID-19 pandemic included rapid mass vaccination, social distancing, lockdowns, surveillance, and other public health measures, which significantly contributed to the containment and management of the disease.5,7 Despite these advancements, a new set of challenges has emerged for many individuals who have recovered from COVID-19. Persistent, often debilitating symptoms, collectively known as “long COVID,” have been reported, affecting a considerable number of survivors. These symptoms range from physical ailments like fatigue, muscle pain, and respiratory issues to cognitive impairments and mental health conditions such as anxiety, depression, and mood disorders.8,9 The impact of long COVID extends beyond physical health, placing a substantial burden on individuals, families, and healthcare systems globally.
Quality of Life (QoL) is a comprehensive measure of an individual’s physical, psychological, and social well-being. It captures aspects of their overall health status, relationships, and environment, offering insights into their ability to perform daily activities and fulfill social roles.10,11 In context of post-COVID-19 recovery, QoL has become increasingly important in understanding the broader impact of chronic conditions, including long-COVID as survivors are often reported experiencing disruptions in their ability to work, maintain social connections, and engage in regular activities due to persistent symptoms. This condition has underscored the need for holistic approaches in care and rehabilitation, focusing on restoring not just physical health but also mental and social well-being.10,11 While studies from high-income countries have begun to explore these issues, research from low- and middle-income countries (LMICs), including Nepal, remains limited.12 –14
Nepal, like many LMICs, faced significant strain on its healthcare system during the peak first and second waves. 4 The country's limited resources were directed toward managing acute cases, leaving long-term impacts, including QoL, largely unaddressed.15 –17 Given Nepal’s unique socio-economic and healthcare challenges, it is critical to understand how COVID-19 survivors are faring in the long term. Without empirical evidence, it is difficult to design targeted interventions or inform policies that support post-COVID recovery. Despite some small-scale reports, there has been no comprehensive assessment of QoL among COVID-19 survivors in Nepal, especially in diverse urban areas.
Therefore, this study aims to assess the quality of life among discharged COVID-19 patients residing in Pokhara Metropolitan City. Pokhara, the largest metropolitan area in Nepal, represents a diverse population in terms of demographics, ethnicity, culture, and socio-economic status. By focusing on this setting, the study seeks to provide evidence that can inform public health strategies and rehabilitation services for post-COVID-19 care in similar LMIC contexts.
Methods
Study design and setting
This was a community-based cross-sectional study conducted among post-COVID-19 patients discharged from hospitals in Pokhara Metropolitan City, Gandaki Province, Nepal, between March and July 2022.. Pokhara Metropolitan is the largest metropolitan city in Nepal and serves as the capital of Gandaki Province, accommodating a total of 149,459 households and 513,504 residents. 18 With a population density of approximately 1300 persons per square kilometer and rapid urban expansion, Pokhara represents a demographically diverse and socioeconomically dynamic area. It also served as a regional hotspot during the COVID-19 pandemic, with Gandaki Province reporting 745 confirmed cases during the first wave and 2172 during the second wave. The impact extended beyond the general population to frontline health service providers, further straining the healthcare system during peak transmission periods. 5 These factors made Pokhara a strategically important setting for assessing the long-term impacts of COVID-19 on health-related quality of life.
Study participants
During the study period, hospitalization in Nepal was guided by national protocols, which aligned with the World Health Organization (WHO) classification of COVID-19 severity. Only patients with moderate symptoms or severe symptoms or signs of severe respiratory distress while mild cases were managed through quarantine centers or home isolation. The study included all post-COVID-19 patients who had been discharged from five selected hospitals in Pokhara Metropolitan City at least 6 months before the start of data collection. Patients who were not residents of Pokhara Metropolitan were excluded to ensure the study population was representative of this specific region.
Sample size
The sample size was calculated by using Cochran’s formula for the estimation of proportion = z2pq/d2. Since there were prior studies assessing the QoL among post-COVID patients a prevalence of 50% was assumed to maximize sample size. Adjusting this prevalence at a 5% allowable error and 95% Confidence interval, and a finite number of patients discharged from the selected hospital (N = 917), the sample size was estimated at 271.
Sampling technique
Systematic random sampling was employed to select the participants. A comprehensive list of COVID-19 patients discharged from the four selected hospitals that granted permission for the study was compiled in an Excel sheet, along with the registered contact details of the patients. The sampling interval (k) was calculated based on the total number of discharged patients and the required sample size: (k = 917/217 = 3.4 ≈ 3rd) (Figure 1). A random starting point was generated using Excel, and every third patient on the list was chosen. The selected participants were contacted by phone and informed about the study, and also asked to provide a convenient date and time for a face-to-face interview at their household/ residence. If a selected participant could not be reached or declined to participate, the next eligible patient on the list, following the sampling interval, was chosen as a replacement.

Sampling technique.
Data collection
A face-to-face interview technique was used to collect data from the participants at the participants’ households. Informed consent was obtained from each participant before initiating the interviews. The interview schedule consisted of four sections, where first section included questions regarding sociodemographic characteristics including participants' age, gender, ethnicity, religion, family type, educational status, marital status, and occupation. The second section covered lifestyle factors such as smoking habits, alcohol consumption, daily exercise, and chronic disease. The third section included COVID and other health-related information such as the availability of bed in health facilities, satisfaction with services, problems faced during COVID-19, and experiences of discrimination due to COVID-19 positive. Finally, the fourth section consisted of 26 original items World Health Organization Quality of Life Brief Version (WHOQOL-BREF) was used to assess the quality of life. 19
Statistical analysis
Outcome variable
The quality of life was the outcome variable assessed through WHOQOL-BREF. The WHOQOL-BREF comprises four domains: (i) physical health, (ii) psychological health, (iii) social relationships, and (iv) environment, along with two general questions on overall health and perception of quality of life. The WHOQOL-BREF scores range from 0 to 100, where higher scores indicate better quality of life, and lower scores reflect poorer quality of life. 19 In this study, scores equal to or greater than 50 were considered indicative of “good QoL,” while scores below 50 were categorized as “poor QoL”.20,21 The Nepali version of the WHOQOL-BREF was utilized in this study to ensure cultural and linguistic appropriateness. 22 This version has been previously validated, demonstrating good psychometric properties in assessing quality of life among the Nepali population. The interview tool, which included the WHOQOL-BREF and additional sections on sociodemographic and health-related factors, was pretested on a small sample of 30 participants to assess clarity, comprehension, and cultural relevance. Based on pretest feedback, minor adjustments were made only to the additional, non-WHOQOL-BREF items. The WHOQOL-BREF section itself was used in its original validated Nepali version without any modifications. The reliability of the overall tool was assessed using Cronbach's alpha, with a value of 0.88, indicating good internal consistency. The operational definition of each variable is provided as a supplemental file (supplemental 1)
Data processing, management, and analysis
The participants’ responses were thoroughly reviewed for completeness before concluding each interview. The collected data were entered into EpiData V.3.1 and subsequently exported to the Statistical Package for Social Sciences (SPSS) V.16 for further analysis. Data were summarized using frequencies and proportions. Associations between variables were analyzed through unadjusted and adjusted odds ratios at a 5% level of significance to identify the factors associated with QoL. Before going into the multivariable analysis, the multi-collinearity among independent variables was tested using the Variance Inflation Factor (VIF), where the highest VIF observed was 1.86 indicating no issue of multi-collinearity. The Hosmer and Lemeshow test was applied in each adjusted model to assess the goodness of fit of the model where all the models reflected p > 0.05
Ethical considerations
Ethical approval for the study was obtained from the Institutional Review Committee of Pokhara University (Ref. 05/078/079). Approval was also secured from the administration departments of the selected COVID-19-dedicated hospitals. Participants were fully informed about the study objectives before the interviews, and written informed consent was obtained. Confidentiality and privacy of the participants were strictly maintained throughout the study.
Results
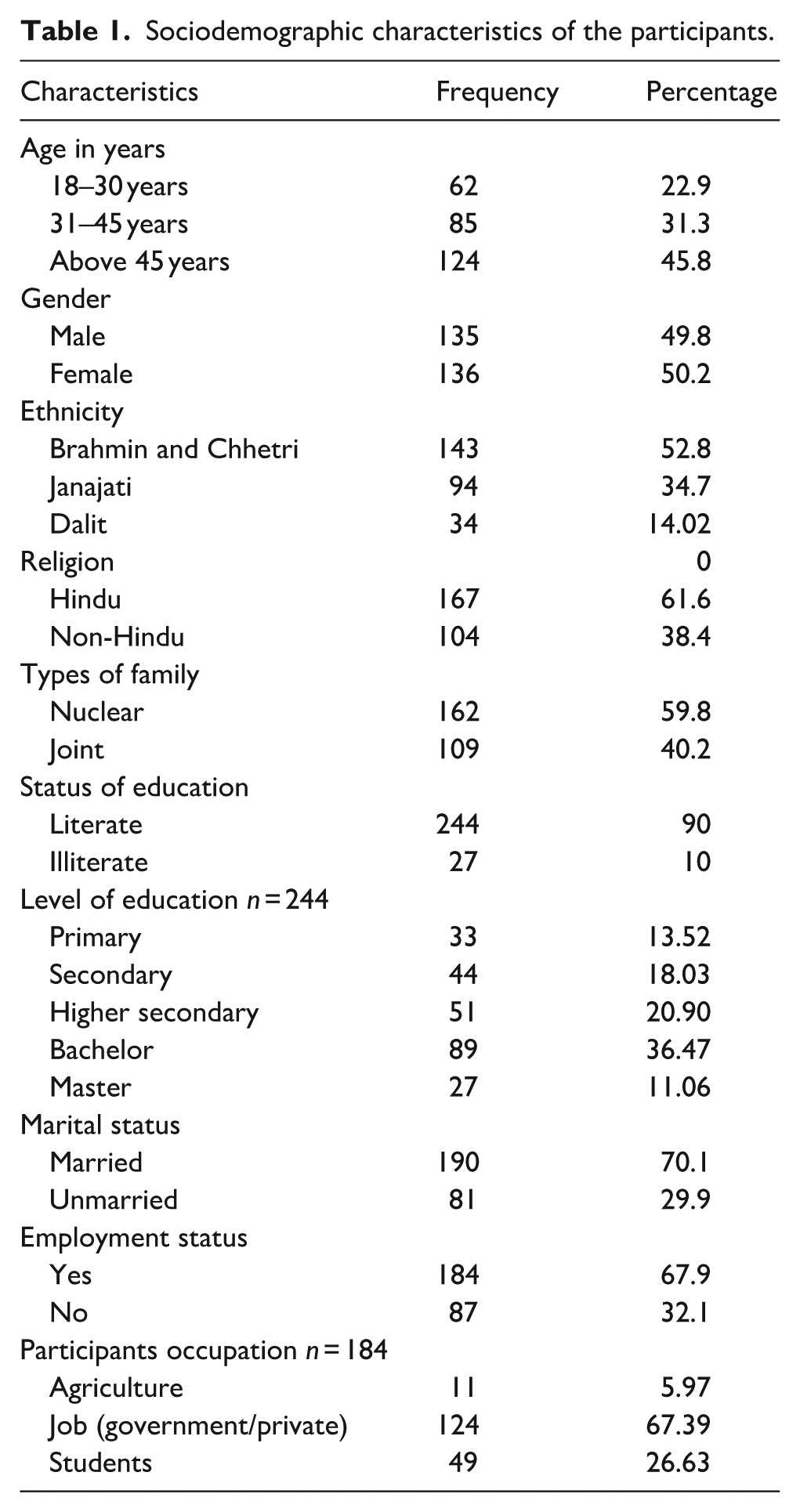
The participants’ mean age was 45.44 years (SD = 16.81), with most (45.8%) being above 45 years. Gender distribution was almost equal, with 49.8% males and 50.2% females. Brahmin and Chhetri (52.8%) were the largest ethnic group, followed by Janajati (34.7%). Most participants identified as Hindu (61.6%). Nuclear families were more common (59.8%). Education levels were generally high, with 90% being literate and 36.47% attaining at least a bachelor’s degree. The majority (70.1%) were married, and 45.8% were employed, with unemployment at 32.1% (Table 1).
Sociodemographic characteristics of the participants.
Around 35.8% of participants smoked, and 36.9% consumed alcohol. However, only 32.5% reported daily physical exercise. Chronic diseases were prevalent in 37.6% of participants, with hypertension (43.1%) and diabetes (41.2%) being the most common. During COVID-19, 72% experienced breathing problems, and 58.7% reported loss of smell or taste. About half (50.2%) faced discrimination due to their COVID-positive status. Despite challenges, 91.9% had access to hospital beds, and 93.4% were satisfied with healthcare services (Table 2).
Lifestyle and health-related characteristics of the participants.

The physical domain had a minimum score of 13 and a maximum score of 100, with a mean of 65.58 ± 21.53. The psychological domain scores ranged from 19 to 94, with a mean of 60.97 ± 16.33. The social relations domain had scores between 25 and 94, with a mean of 61.09 ± 14.27. The environment domain scores ranged from 25 to 94, with a mean of 57.50 ± 11.52. The overall QoL scores ranged from 28 to 86, with a mean of 61.29 ± 12.54 (Table 3).
Data distribution of QOL response.

In regards to HQoL, poor HQoL was reported by 19.2% in the physical domain, 20.3% in psychological, 11.8% in social relations, 14.4% in environment, and 17.7% overall. Good HQoL was highest in social relations (88.2%) and lowest in the psychological domain (79.7%). Most participants had good HQoL across all domains (Figure 2).

Distribution of poor and good HQOL across different domains.
In the multivariable analysis, several key factors were significantly associated with good quality of life (QoL) among post-COVID-19 patients. Participants living in nuclear families had 2.61 times higher odds of reporting good QoL compared to those in joint families (aOR = 2.61, 95% CI: 2.14–6.00). Employment played a crucial role, with individuals engaged in jobs being four-fold increase in odds of experiencing better QoL than housewives (aOR = 4.10, 95% CI: 1.87–9.21), whereas those in agriculture had significantly lower odds of QoL (aOR = 0.13, 95% CI: 0.024–0.81. Regular physical exercise was another strong predictor, as participants who exercised daily had thrice the odds of good QoL than those who did not (aOR = 3.32, 95% CI: 1.36–8.06. Conversely, the presence of chronic disease was the strongest negative predictor of QoL, with those free of chronic illness being 6.15 times more likely to report good QoL (aOR = 6.15, 95% CI: 2.65–14.24). Other demographic factors such as age, gender, ethnicity, and religion did not show significant associations in the adjusted analysis(Table 4).
Factors associated with QOL.

Statistical significance at p<0.05.
Discussion
This study evaluated the quality of life among post-COVID-19 patients in Pokhara Metropolitan, Kaski, using the WHOQOL-BREF scale. The findings revealed that 82.3% of participants had a good QoL, while 17.7% experienced poor QoL. Among the domains, the environment domain scored the lowest mean, followed by social relationships, psychological, and physical domains but the overall QoL seems to be good. These findings align with a study from Bangladesh, which similarly reported the physical domain as having the highest average score, followed by social relationships, psychological, and environmental domains, yet reflecting a good overall QoL. 20 It has been also been suggested that ability to perform physical activity could be highly impaired in post COVID patients. 23 Collectively, these studies highlight substantial changes in the QoL of post-COVID-19 patients, emphasizing the need for targeted interventions to address these concerns during any form of public health emergencies.
Several factors, such as age, sex, education, religion, marital status, smoking, and alcohol intake, were not significantly associated with QoL in this study. This contrasts with prior research that linked declining QoL with increasing age, female gender, and lower education levels.24 –26 Interestingly, a study from Bangladesh found that gender only affected the psychological domain. 20 Similarly, past evidence suggest that that increasing level of education could generally increaser the QoL score. 20 Similar observation was made in our bivariate analysis but the association weekend in multivariable analysis suggesting that other factors could be considered. Contrary to evidence that smoking and alcohol use can negatively impact health-related QoL during and after COVID-19, 27 but our study found no such association. The lack of association in our study could reflect regional differences in lifestyle habits or cultural norms, which may mitigate the adverse effects typically associated with these behaviors. One possible explanation for the lack of statistical significance could lie in Nepal's sociocultural norms and consumption patterns. In many communities, moderate alcohol use is socially accepted and embedded in cultural events, 28 and therefore may not be associated with reduced QoL unless it becomes excessive or problematic.
Living in a nuclear family was positively associated with good QoL (aOR: 2.61, 95% CI: 2.14–6.00). This might be because the smaller family structures may provide better support or reduced stress during the recovery period, possibly due to fewer caregiving burdens, greater privacy, and more stable household dynamics during lockdowns. In contrast, other studies report mixed results, with some associating better QoL with joint families, others with nuclear families, and some finding no significant association.28 –30 Differences in family dynamics, reduced interpersonal conflicts, and smaller household sizes during lockdowns could explain the findings in our study. The observation suggest that family-centric interventions should consider the dynamics of both nuclear and joint families. Tailored counseling and support mechanisms can mitigate stressors unique to each family type.
Employment was a significant predictor of good QoL (aOR: 4.10, 95% CI: 1.87–9.21). Employed individuals, as compared to housewives, reported better QoL, consistent with studies from Germany and Israel, which highlighted financial security and social interaction as buffers against psychological distress.31,32 It has been reported that monthly family income could have a significant positive association with physical, social and environmental domains of QoL of the participants. 20 These findings highlight the importance of lifestyle behaviors, access to economic resources, and effective chronic disease management in supporting the long-term well-being of COVID-19 survivors. Conversely, unemployment or limited roles such as caregiving may exacerbate stress and reduce perceived life satisfaction during recovery. Policymakers should prioritize economic recovery programs, including job placement services and skill-building initiatives, to support unemployed individuals post-COVID-19.
Regular exercise was positively associated with QoL (aOR: 3.32, 95% CI: 1.36–8.06), consistent with Italian studies where physical activity was linked to better physical and mental recovery from COVID-19.33,34 Exercise may improve physical endurance, reduce symptoms of fatigue, and alleviate psychological stress. 35 Awareness campaigns promoting daily physical activity, even at home, should be integrated into post-COVID-19 recovery programs. Community fitness initiatives could further encourage participation.
The absence of chronic diseases was the strongest predictor of good QoL (aOR: 6.15, 95% CI: 2.65–14.24). Similar findings have been reported globally, as chronic illnesses often require prolonged medication and healthcare access, imposing financial and psychological burdens. Study based on Bangladesh reported that presence of any of the major six non-communicable comorbid condition such as HTN, DM, IHD, BA/COPD, CKD, and cancer could significantly lower the Qol scores. 36 Furthermore, another study from Bangladesh suggested that new onset of chronic diseases after recovery from COVID-19 can also have a significant negative determinant of QoL among the sufferers. 25 These findings suggest the need to prioritize comprehensive care for chronic disease patients by the healthcare systems at the time of these forms of public health emergencies. This could be done by including regular follow-ups, affordable medication, and psychological counseling. Preventive health measures such as early screening should also be emphasized.
This study emphasizes the interplay of sociodemographic and behavioral factors in shaping QoL post-COVID-19. This study has several strengths. It captures diverse sample of post-COVID-19 patients from five major hospitals in Pokhara, enhancing the representativeness of the urban population in Nepal. By focusing on the post-discharge period, it provides timely insights into long-term recovery that are often underexplored in low- and middle-income countries. The low environmental domain score (mean 57.5 ± 11.5) may reflect urban challenges in Pokhara. The environmental domain assesses factors like financial resources, safety, and access to a healthy physical environment. Issues such as air pollution, limited green spaces, or crowded living conditions, common in urban LMIC settings, may contribute to lower scores. However, as these factors were not directly measured, this interpretation is speculative and warrants further investigation. The findings underscore the need for a multidisciplinary approach to patient recovery, incorporating physical, psychological, and social health dimensions. Policies should target vulnerable groups, including those with chronic diseases, and promote employment, exercise, and family support to enhance overall well-being.
Despite these implications, several limitations should be considered when interpreting its findings. The timing of data collection may have introduced contextual influences on QoL. Interviews were conducted between March and July 2022, several months after Nepal's second major COVID-19 wave, during a relatively stable period without lockdowns. While this stability may have positively influenced perceived quality of life, variability in time since discharge (ranging from 6 to 18 months) may have affected recall and recovery experiences differently. As the study was conducted exclusively within Pokhara Metropolitan, its findings may not be reflective of the culturally diverse populations in Nepal, particularly those in rural areas with varying socio-economic and cultural contexts. The study included only adults aged 18 years and above, which may limit the generalizability of findings to younger populations. Furthermore, data on the frequency of follow-up care after hospital discharge or the duration between discharge and the time of interview were not captured and the absence of these variables may limit the comprehensiveness of our findings and should be considered when interpreting the results. Lastly, some important factors that could significantly influence QoL, such as levels of social support, experiences in social relationships before and after the pandemic, participants’ psychological well-being and other contextual variables, were not explored due to time constraints and the need to minimize respondent burden. Future research could incorporate validated tools to assess these factors and provide a more comprehensive understanding of the determinants of QoL. These unexamined aspects highlight the need for further research to deepen our understanding of the relationship between public health emergencies, such as COVID-19, and QoL. Future studies could explore these gaps to provide a more comprehensive perspective on post-pandemic recovery strategies.
Conclusion
This study provides valuable insights into the QoL of COVID-19 survivors in Nepal, revealing significant disparities based on socioeconomic and health-related factors. While most participants reported good overall QoL, challenges remain in the psychological and environmental domains, suggesting the need for targeted interventions. Employment, exercise, and family structure were key determinants of better QoL. These findings emphasize the importance of comprehensive post-pandemic rehabilitation programs focusing on both physical and mental health support. Policymakers should consider implementing community-based follow-up services and targeted support for patients with such conditions that might have long-term impact.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251390940 – Supplemental material for Health-related quality of life among COVID-19 survivors in Pokhara Metropolitan, Nepal: A cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036251390940 for Health-related quality of life among COVID-19 survivors in Pokhara Metropolitan, Nepal: A cross-sectional study by Bhawana Dhakal, Dhurba Khatri, Shishir Paudel, Dipendra Kumar Yadav, Yamuna Chhetri, Shushil Tripathee and Bhakta Bahadur KC in Journal of Public Health Research
Footnotes
Acknowledgements
We sincerely thank all the participants for their valuable time and information; their contributions were essential to the success of this study.
Ethical considerations
Ethical approval for the study was granted by the Pokhara University Institutional Review Committee (Ref. No. 05/078/079).
Consent to participate
Prior to data collection, written informed consent was obtained from all participants, ensuring their right to withdraw at any time and their voluntary participation.
Author contributions
Conceptualization: BD, DK, DKY; Data curation: BD, ST, YC; Formal Analysis: BD, DK, SP; Methodology: BD, DK, SP, DKY; Project administration: BD, DK; Supervision: DKY; Validation: BD, DK, SP; Visualization: DK, SP; Writing original draft: BD, DK, SP; Writing review & editing: YC, BBK, ST, DKY
Funding
The authors disclosed receipt of the following financial support for the research: This study was funded by the Nepal Health Research Council, Nepal, to Bhawana Dhakal as part of the 2021 Post-Graduation Health Research Grant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data generated during the study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.