
Abstract
Background:
The utilisation of healthcare services is critical to maintaining and improving the health status of communities, however, numerous barriers and enablers can either hinder or facilitate an individual’s ability to access and benefit from these services, and this is the case in South Africa.
Objective:
This study aimed to identify and describe barriers to and enablers of healthcare service utilisation in a rural village of Mpumalanga province, South Africa.
Methods:
A quantitative descriptive survey design was conducted with 415 adults who met the inclusion criteria, selected using a systematic sampling technique. Data were gathered through a researcher-administered questionnaire. Descriptive statistics were conducted, using the IBM SPSS version 29 software, to explain and summarise the data. The study was guided by Andersen and Newman’s Behavioural Model, focusing on barriers and enabling factors to Health services utilisation.
Results:
Key barriers identified in this study included cultural beliefs (58.7%), treatment shortages (54.4%), staff shortages (45.6%), negative staff attitudes (88%), long wait times (84.1%), lack of grievance mechanisms (77.8%), and poor interpersonal skills from nurses (88.5%), leading to low patient satisfaction. Men showed disengagement from chronic care (13%) compared to women (2.9%). A significant portion (20%) had no education, impacting health literacy. Enabling factors included a preference for the local clinic (98.8%) due to its proximity (69.3%) and confidence in nurses’ abilities (88.7%).
Conclusion:
The study highlighted that healthcare access is hindered by resource limitations, staff issues, attitude and communication problems, and cultural factors. Women, young adults, and less educated individuals underutilise services. This necessitates age and gender targeted programs, culturally sensitive strategies, and improved service delivery and quality assurance policies. Counselling for healthcare workers and accessible feedback mechanisms can enhance patient interactions and satisfaction. Further research is recommended to comprehensively address these barriers to healthcare access and utilisation.
Introduction
South Africa is regarded as one of the economic powerhouses of Africa and the state spends about 8.6% of its gross domestic product (GDP) on health services; 1 however, like most sub-Saharan African countries, it continues to experience challenges in healthcare utilisation and access, as well as delivery of healthcare services. Despite strategies employed by the country to improve the healthcare services access and utilisation, barriers still exist, especially in the rural and most disadvantaged parts of South Africa, such as in the Nkomazi sub-district, in the Ehlanzeni district of the province of Mpumalanga. Among the strategies employed by the country was the development of a 10-point plan to improve the health system and central to this initiative was the prioritisation of primary healthcare (PHC), as the backbone of healthcare services delivery. 1 In South Africa, access to healthcare is especially limited in underprivileged rural communities and among vulnerable groups such as young people, senior citizens, those with less education, children, and people with disabilities. 2 Structural factors, related to policies, the health system and resources; socio-cultural factors, including language and cultural barriers; organisational factors, such as lack of healthcare provider training and preparation, and overburdened clinics; and individual and provider factors, such as stigma, were identified as barriers to perinatal mental health in South Africa. 3 Lack of parents/caregivers’ support, as well as the support of sexual partners, and healthcare providers’ negative attitudes, arose as barriers to contraception use by adolescent girls and young women. 4 Another study conducted in the Eastern Cape, South Africa, found that physical inaccessibility and shortage of resources, long travel distances, lack of transportation, including ambulances, and the shortage of healthcare workers and unavailability of health facilities were among the barriers to accessing healthcare services. 5 Moreover, a study conducted in South Africa, on HIV management services, revealed denial and lack of readiness, side effects, perceived stigma, fear of non-adherence, dislike of pills and preferences of alternative medication, and progression of HIV, as barriers to access HIV treatment; while accepting status, fear of HIV progression, disclosure and exposure to people living with HIV emerged as enablers for HIV treatment. 6
Mpumalanga Province is ranked as the third most rural province in South Africa and has historically lagged in the development and delivery of basic services such as education and healthcare services. 7 A study conducted in rural north-eastern Mpumalanga found that the utilisation of pregnancy-related healthcare services and the presence of skilled birth attendants at delivery have steadily increased since 1993. However, the study also revealed that mothers of Mozambican descent are still less likely to use free healthcare services. 8 Another study revealed that the non-use of sexual and reproductive health services in the province was due to a lack of awareness about these services, varying levels of knowledge about the services, poor quality of services in public hospitals and clinics, negative attitudes of nurses, and a lack of services specifically designed for males. 9 Various measures and strategies have been introduced by governments and health agencies such as the WHO to improve the quality of healthcare services. These measures aim to ensure that healthcare services are effective, safe, people-centred, integrated, and efficient services. 10
Despite these efforts, significant gaps still exist in healthcare service delivery. Several identified improvement tools and resources made little or no mention of measurement considerations and there is currently no mechanism to track the application of Service Delivery Standards (SDS) and tools and resources within countries. 10 Additionally, issues such as inappropriate awarding and management of tenders for healthcare service delivery persist. 11
A study conducted at Ehlanzeni District revealed that health care services utilisation (HCSU) is also a challenge in this area, particularly for young adolescents living with HIV resulting in low retention into care, a situation consistent with other services. 12 The situational analysis indicators for district health services, showed that the primary healthcare services utilisation rate for Ehlanzeni District was at 2.8% for the 2016/2017. 7 Similarly, in the Enkomazi sub-district the residents have repeatedly expressed their dissatisfaction with the poor quality of healthcare services delivery during community meetings. They have called on the government to improve healthcare service quality and enhance existing healthcare facilities to ensure the provision of efficient and quality services. However, despite these appeals, little progress has been made, and the utilisation rate of healthcare services remains low. 13
The Nkomazi sub-district of Ehlanzeni, in Mpumalanga, faced comparable difficulties, where residents were not utilising health services, as shown by the discrepancies in the headcount statistics and the actual population in the area. Community members often postpone seeking medical attention, sometimes only going to the clinic when pressured by family or friends or when their health has significantly worsened. When questioned about these delays, patients often do not provide clear reasons for not using available healthcare. Consequently, the health facility’s monthly patient numbers have remained consistently low, averaging around 1868 patients per month from January to July 2022, which is only about 25% of the total population of 7396. In addition, about 20 patients per month are lost to follow-up (defined as missing appointments for three consecutive months), with many admitting to using herbal remedies instead of prescribed medications. The reasons behind this low healthcare usage are not well understood. Moreover, there’s a noticeable lack of outreach programs, visits from doctors and other healthcare professionals, and school health services in some communities, including the area where this research took place. This study seeks to identify and describe the factors contributing to the low utilisation of healthcare services in order to improve individual and community health outcomes in the village as well as providing evidence-based recommendations to policymakers and relevant stakeholders, to enhance the utilisation of healthcare facilities.
Methods
Study Design, Setting and Participants
A quantitative descriptive survey design was followed in this study, where face-to-face, individual questioning, using a structured questionnaire, were conducted by the researcher to identify and describe factors that impede or facilitate the use of the available healthcare services by the residents of Nkomazi.
The study was conducted in a rural village of Nkomazi sub-district, in the Ehlanzeni district of Mpumalanga, which is approximately 55 km from the nearest town. The village follows a traditional lifestyle and is led by a chief, supported by four advisors known as indunas. The village’s primary economic activities are agriculture and livestock farming, with an employment rate of 57.9% among residents aged 15 to 64. Education levels are generally low: nearly 30% of residents over 20 have no formal education, around 27% have completed high school, and only 6.5% have a higher education. The community relies on a single public clinic for basic healthcare, which operates for 8 hours a day, 5 days a week, and is located within 5 to 10 km of the village. There are no private healthcare options.
The village has a strong presence of traditional healers, with 57 practitioners (23 men and 34 women) serving an adult population of approximately 7396 (53% women, 47% men) spread across 1518 households, averaging about five people per household. The district experiences a high disease burden, with non-communicable diseases causing 39% of deaths and HIV/tuberculosis contributing to 30% of mortality. In 2022, the HIV prevalence rate in the district was 17.5%. 14
All adult residents, aged 18 years and older, who willingly agreed to participate in the research, from the entire target population, were included in the study. Individuals with mental health conditions that impaired their ability to give informed consent, those who were not willing to participate, and people who were not residents of the village were excluded from the study.
Sampling and Sample Size
In this research, a probability systematic sampling technique was employed across all eight sections of the village. This method was chosen to ensure a representative sample of community members meeting the inclusion criteria, as it gives every individual an equal chance of being selected. From the 1518 households with approximately three adults each, 138 households were chosen by starting at a random household and then selecting every 11th household until the target of 415 adults was reached out of a total of 4154. A larger sample size was necessary to ensure the generalizability and reliability of the study’s findings. 15 Sampling was conducted concurrently with data collection, as the number of adults present in each household on the day of data collection was unknown. The village was divided into eight sections to ensure representativeness, accuracy, and reliability. Data collectors made one visit to each household, except for two households where no adults were present on the initial visit. The response rate was 100%, with no respondents refusing to answer questions or showing disinterest during the process.
Data Collection
After obtaining approval from the University of South Africa Research Ethics Committee and Mpumalanga Provincial Department of Health, including all necessary permissions from the local traditional and political leadership, the researcher commenced with home visits and attending traditional lekgotlas (meetings), where respondents were provided with participant information sheets, containing details of the project. Those who understood and agreed to participate signed consent forms, written in English. For non-English speakers, the information was interpreted and explained to them by the researcher, using the local language, to ensure informed consent was given voluntarily. Data were collected by the researcher and two trained data collectors, who signed a declaration of confidentiality agreement. The questioning process was primarily conducted in Siswati, as it is the predominant language in the community; however, respondents could choose between Siswati and English. The questioning, held at the respondents’ homes, lasted approximately 25 to 30 minutes, and consisted of close-ended questions related to HCSU including, among others, beliefs and myths related to disease causation and cure, staff attitudes, Health care workers (HCWs)’ interpersonal skills, and wait times, as well as demographic information see Supplemental Appendix A. To ensure privacy during the questioning process, a private space, away from other family members, was requested, preferably outside, under shade, or in a living room, during bad weather. If the initially scheduled time was inconvenient for the respondents, interviews were rescheduled accordingly.
Before the main study, the data collection tool was pre-tested with five systematically selected households to identify any potential issues. This pre-testing assisted in estimating the time needed to complete the questionnaire and allowed data collectors to become familiar with the data collection process. Participants were also asked about any difficulties or discomfort experienced while answering the questions. No issues were found with the questionnaire, so no changes were made. The pre-testing study respondents and the results were not included in the main study. To ensure face validity, the questionnaire was reviewed by the researcher’s supervisor, a statistician, and the scientific review committee to assess its appropriateness for measuring the intended variables. Furthermore, data collectors checked the questionnaires daily for completeness during the data collection process.
Data Analysis
Descriptive data analysis was employed to provide an explanation and summary of the data, thereby illustrating the characteristics of the dataset, 15 as well as the organisation of the data in a way that facilitates meaning and insight. The data was captured in Microsoft Excel and was cleaned and verified before it was imported into IBM SPSS software. Categorical variables were presented, using frequency tables and graphs, and compared, using percentages, to determine the relationship between the dependent and independent variables. 16 Cross-tabulation statistical analysis was used to quantitatively assess the relationships between multiple variables and to understand the correlation among different variables, by using the IBM SPSS 29 software. The following statistical measures were used: frequency 17 distribution, showing the number of times a result occurs, and the measure of central tendency, which includes the mean, median, and mode. The mean shows the arithmetic average of all the scores in a distribution, the median shows the midpoint score when data is ranked from lowest to highest, and the mode shows the value or score which occurs most frequently in a distribution. 16
Frequency distributions and proportions were used to describe beliefs and myths about disease causes and cures, resource shortages, negative staff attitudes, lack of avenues for complaints, poor nurse interpersonal skills, health facility choices, healthcare service patterns, perceptions of nurses’ skills and knowledge, and the number of respondents taking chronic medication. Frequency distributions, proportions, measures of central tendency (mean, median, mode), and measures of variability (standard deviation and range) describe waiting times. Cross-tabulation was used to analyse the relationship between gender, age, and education level, and the use of health facilities for minor ailments; gender and the use of health facilities for contraceptives and gender and engagement in and dissemination of care.
Ethical Considerations
The data were collected in October 2023, after obtaining approval from the College of Human Sciences Research Ethics Review Committee (CREC Reference: 42966272_CREC_CHS_2023), and further approval was also obtained from the Mpumalanga Provincial Health Research Ethics (Reference Number: MP_202309_003). Respondents were provided with participant information sheets, with details of the project, and those who understood and agreed to participate signed consent forms. To ensure privacy during the interviews, a private space, away from other family members, was requested. To ensure confidentiality, the data collectors signed confidentiality agreements, used numbers instead of the respondents’ real names, and kept data collection tools separate from consent forms to prevent linkage. The study did not receive any specific funding from any organisation.
Results
A total of 415 adults from 138 households, aged 18 to 60 years and above, who reside in the rural village of Nkomazi, in Ehlanzeni, a district in Mpumalanga, participated in the study. This study identified the demographic characteristics of respondents, as summarised in Table 1. Barriers and enabling factors related to healthcare access and utilization were identified, including healthcare facility usage by gender, age, and education level, the number of respondents on chronic medication, accessing minor ailments and contraceptives and gender-based patient engagement in care. The results are presented as follows.
Demographic characteristics of respondents.

Source: Researchers’ own work.
Demographic Characteristics
Table 1 presents a summary of the respondents’ demographic characteristics. A larger percentage of participants were female (66%) compared to male (43%). The majority of respondents (40.7%) were in the 30 to 39 age group. Christianity was the predominant religion (87.2%), while 5.8% practiced ancestral worship. 26.3% of respondents were married, and 45.5% were in a relationship. Although the majority (95%) had some form of education (formal or informal), 4.8% had no education. Understanding the community’s demographics provides healthcare workers with valuable insights to develop tailored and effective health programs that align with the community’s specific characteristics.
Enabling Factors to Access and Utilisation of Healthcare Services
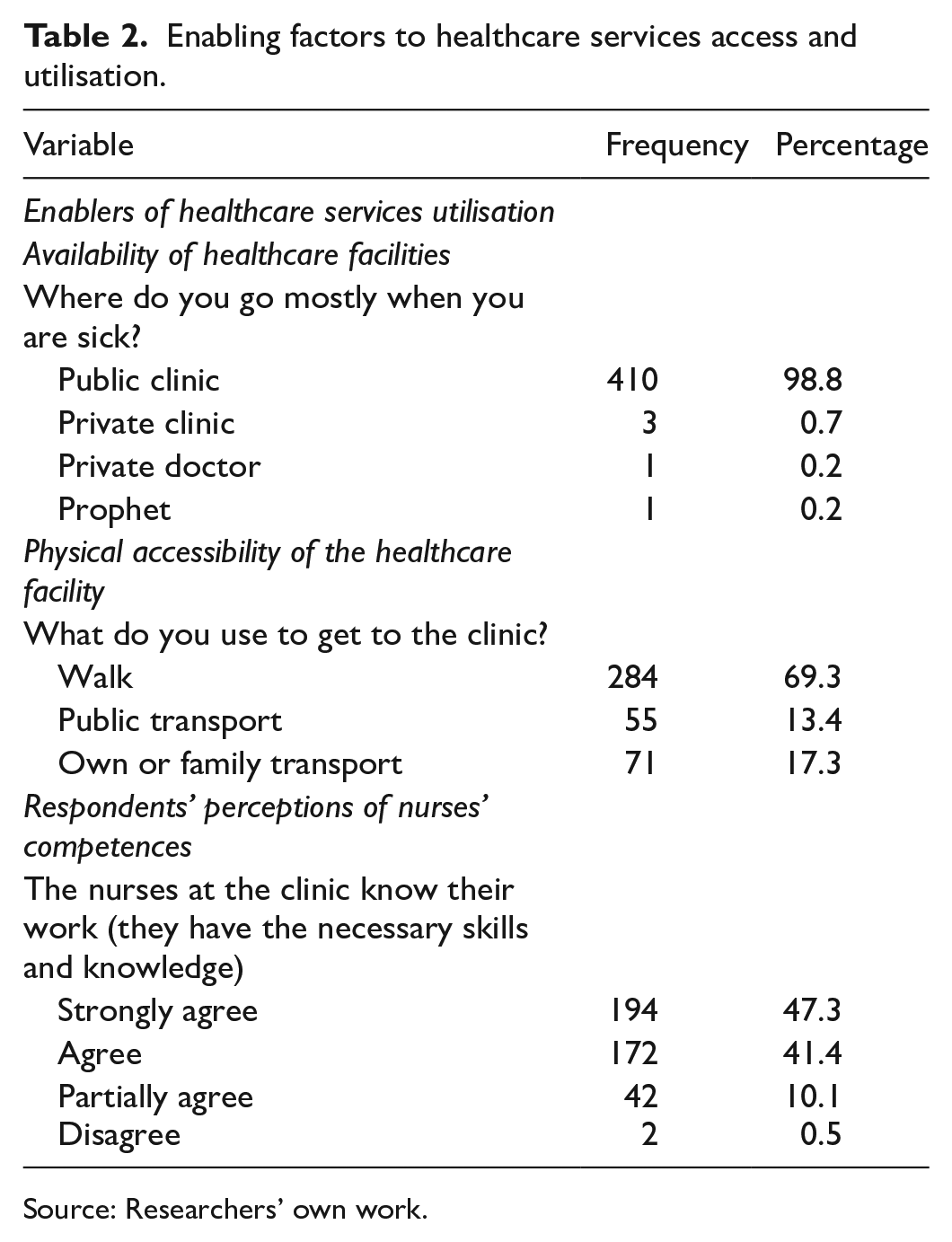
Table 2 outlines the factors enabling community members to access healthcare services. The local public clinic was the preferred choice for most (98.8%) when they were sick due to its convenient location within the village, allowing them to walk there without needing transportation (69.3%), however, 30% still required a form of transport to reach the clinic. Furthermore, a notable proportion (47.3%) expressed confidence in the skills and knowledge of nurses to deliver quality healthcare. This motivates them to seek medical care at a health facility even when they face challenges.
Enabling factors to healthcare services access and utilisation.
Source: Researchers’ own work.
Barriers to Health Care Services
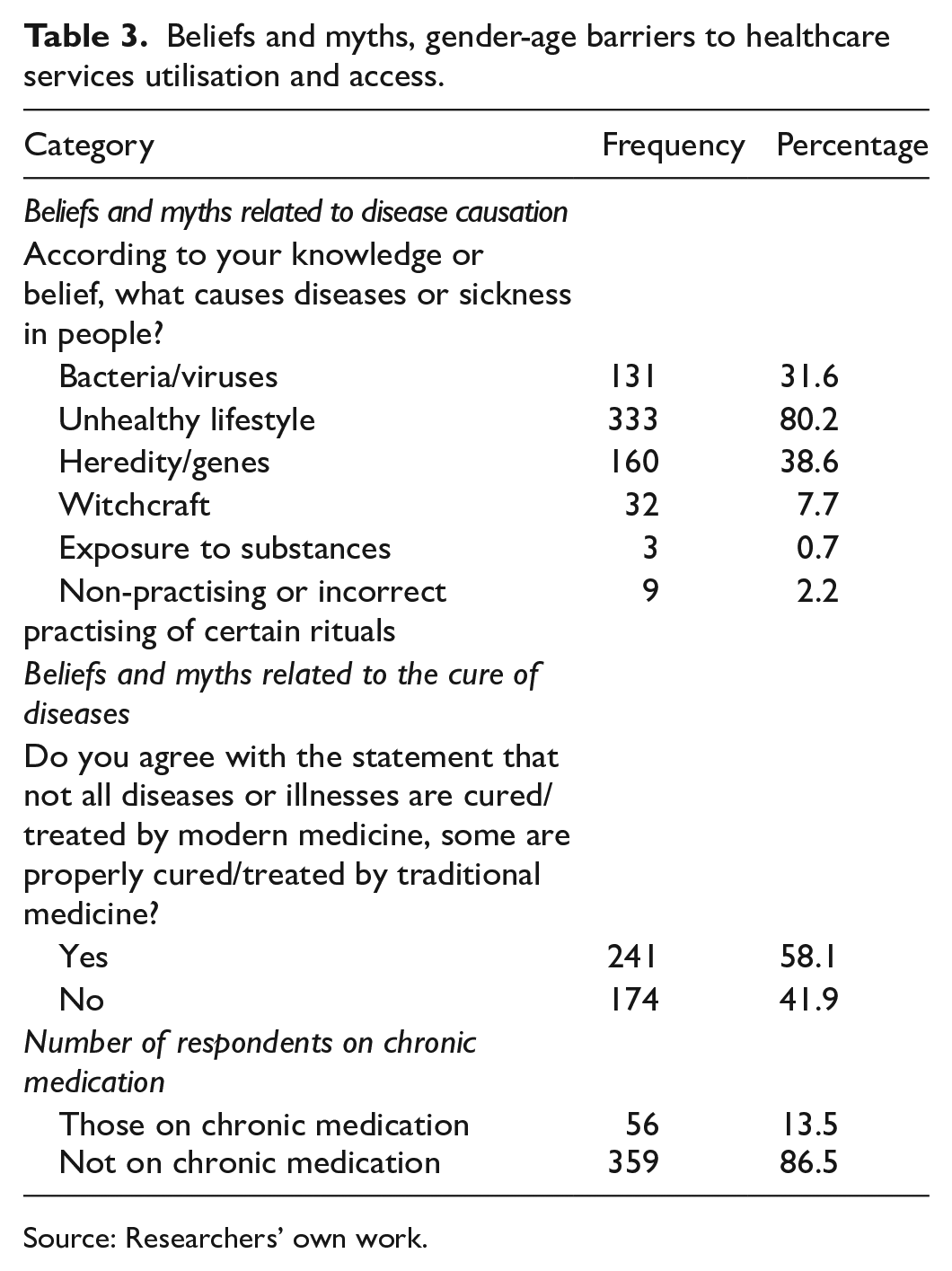
Table 3 outlines several significant barriers to accessing health services identified in this study, including cultural beliefs and misconceptions about the causes and treatments of diseases (58.7%), with 2.2% attributing illness to witchcraft, and that some diseases can be cured by traditional medicine (58.1%). Conversely, respondents also believe that diseases are linked to unhealthy lifestyles (80.2%), genetics (38.6%), and bacteria (31.6%). The majority of the participants (86.5%) were not on chronic medication.
Beliefs and myths, gender-age barriers to healthcare services utilisation and access.
Source: Researchers’ own work.
Table 4 illustrates the utilisation of health facilities for minor ailments and contraceptives. Males utilise (91.5%) healthcare services for minor ailments than women (65.3%. Among age groups, older adults aged 60 and above had the highest usage for minor ailments (96.2%), than young adults aged 25 to 39. Young adults aged 18 to 24 more commonly accessed services for contraceptives (88.0%). Other significant barriers were that disengagement from chronic care was more prevalent among men (13%) than women (2.9%).
Utilisation of Health Facilities for Minor Ailments and Contraceptives.

Source: Researchers’ own work.
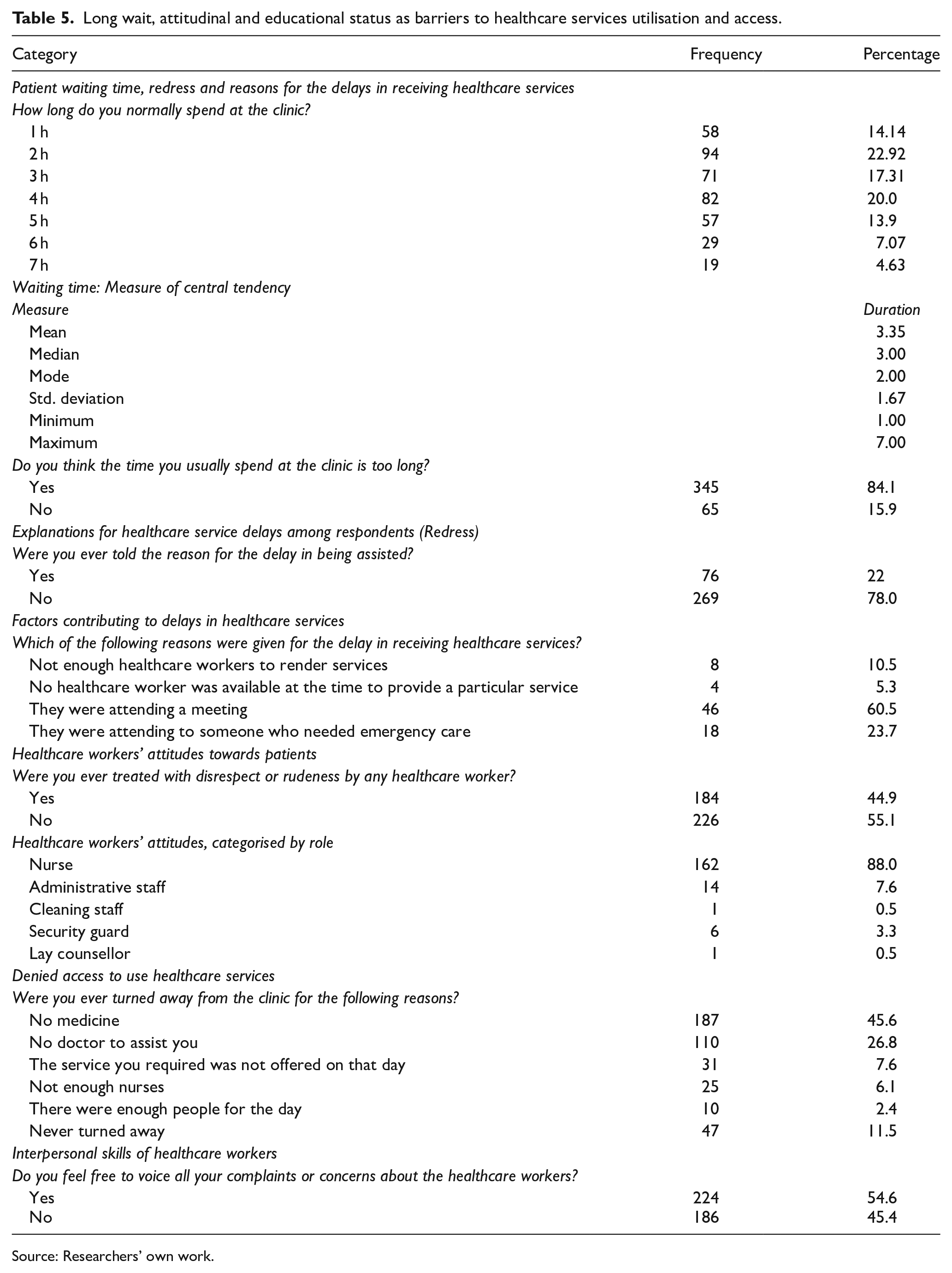
Table 5 highlights several factors that hinder the utilization and access to healthcare services, including long waiting times, healthcare workers’ attitudes, and respondents’ educational backgrounds. Participants reported average waiting times of 3 hours, with some experiencing waits of up to 7 hours, exceeding the quality assurance policy’s average of 4 hours. Contributing factors included staff meetings (60.5%), attending to emergencies (23.7%), and insufficient staffing (10.5%). Additionally, the absence of grievance mechanisms (77.8%) posed a challenge, leaving patients uninformed about delays. Attitudinal issues, such as disrespectful treatment (55.1%), particularly from nurses (88.5%), and poor interpersonal skills among healthcare workers (54.6%), were noted as barriers to accessing and using health services, resulting in low patient satisfaction. Some individuals were also denied access due to a lack of medication (45%) or the unavailability of a doctor (26.8%).
Long wait, attitudinal and educational status as barriers to healthcare services utilisation and access.
Source: Researchers’ own work.
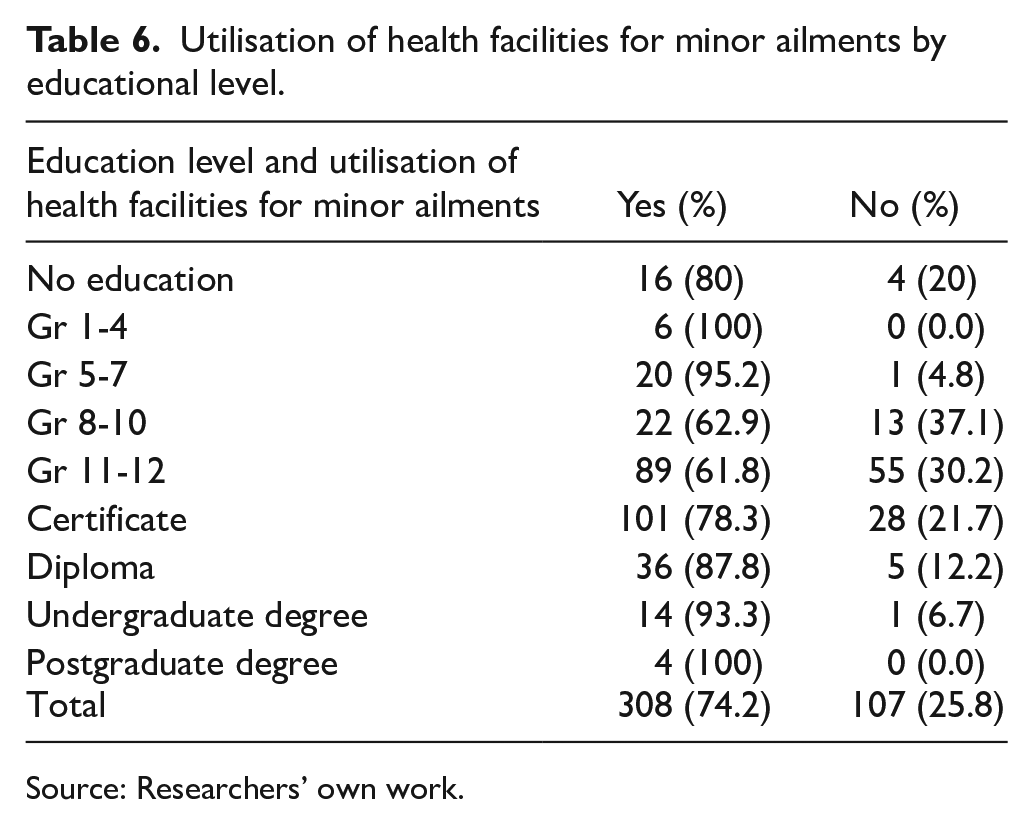
Table 6 shows the utilization rates of health facilities for treating minor ailments based on educational levels. It notes that 20% of respondents lacked formal education, which impacts their health literacy.
Utilisation of health facilities for minor ailments by educational level.
Source: Researchers’ own work.
Discussion of Findings
This quantitative, community-based survey investigated factors influencing access to and utilization of healthcare services among residents of Nkomazi, a rural village in South Africa. The study identified a complex interplay of barriers and enabling factors, highlighting the need for evidence-based strategies to address identified gaps.
Enablers of Healthcare Services Access and Utilisation
The choice of health facility and patterns of healthcare service use, perceptions regarding the skills and knowledge of nurses, and physical accessibility of healthcare services were perceived as factors enabling the use of healthcare services in this study.
The majority of respondents preferred and used the local public clinic as their primary healthcare facility. This indicates a strong value placed on health by the respondents, who actively seek and use available healthcare services. These findings contrast with a study on barriers to primary care, where 77% of participants reported no knowledge of or use of their nearest health facility, despite some expressing satisfaction with the primary health facilities. 17 Only 18.8% would always visit the PHC facility for medical help. 17 Similar findings established that public health facilities are the most widely used choice among households, followed by private facilities, with traditional health facilities being the least preferred option. 18
Another significant enabling factor was the easy accessibility of the healthcare facility, as it is situated within a 5 to 10 km radius of the community, aligning with the WHO’s recommendation that everyone should live within 5 km radius of health facilities. 19 A large proportion of the respondents reported being able to reach the facility on foot, without needing alternative transportation. These findings contrast with the results of a study, which identified a lack of transportation and high service costs as significant barriers for young people to access sexual reproductive health services. 20 Similarly, another study, conducted in Nigeria, established that distance and transportation costs posed barriers to healthcare access for rural residents. 21
Over 80% of the respondents perceived nurses as healthcare workers possessing the necessary knowledge and skills to deliver healthcare services effectively. This perception is crucial, as it enhances patients’ confidence in seeking healthcare services and adhering to treatment recommendations. Trust in nurses’ competence and expertise plays a vital role in fostering patient satisfaction and compliance. Similarly, research on patient trust has shown that trusting in nurses’ knowledge provides patients with a feeling of safety and empowerment. 22 However, contrasting findings established that 61.2% of the participants perceived nurses as lacking understanding of their conditions and 51.0% lacked confidence in nurses. 23
Barriers to Healthcare Services Access and Utilisation
The study findings revealed that, while the majority of respondents demonstrated awareness of the scientific causes of diseases, 2.2% believed in witchcraft as a cause of disease, 0.7% believed in cultural practices, and 58.1% of the respondents believed that some diseases are not cured by modern medicine. 23 These beliefs suggest a need for further education and awareness regarding the scientific understanding of disease causation. Similarly, findings of a study in Kenya established that late medical-seeking behaviour was associated with beliefs in witchcraft among certain cultural and religious groups. 24 These findings are further supported by a study conducted in Ethiopia that revealed that many people use traditional and religious treatments for mental health problems, often attributing illness to evil spirit possession or divine punishment, leading them to keep their relatives at home, instead of seeking medical help. 25
The study established that resource shortages and challenges in the integration of healthcare service delivery are major barriers to the accessibility of healthcare services. A significant proportion of respondents (88.5%, n = 363), reported being turned away or denied services, highlighting an urgent need to improved resource management and healthcare delivery strategies. The unavailability of medicine, doctors and nurses, along with the limited capacity of the clinic, contributes to the challenges respondents face in accessing necessary healthcare. Findings from a study on the amenability of adolescents and young people to utilise health services revealed that specialised surgical, clinical, counselling, therapeutic and other services were not always readily available or were limited to certain days, often necessitating referrals to the district hospital. 26 The results further revealed that healthcare workers, when faced with shortages and an overflow of clients, tend to pragmatically adopt coping mechanisms focused on attending as many clients as possible, a practice referred to as ‘pushing the line’. 26 Similarly, a study in Nigeria identified the main reasons for respondents avoiding the utilisation of primary healthcare services as the poor quality of health services, unavailability of doctors, unavailability of nurses, unavailability of drugs, and high costs of services at primary healthcare facilities. 21
A substantial number of respondents (44.9%) reported being treated poorly at the healthcare facility. It was established that nurses exhibited negative attitudes towards respondents at a higher rate (88%), compared to other staff members, affecting the entire community’s perception of care. Therefore, it is crucial to implement interventions aimed at improving nurses’ attitudes, as they are the primary point of contact for clients at the clinic. Without such improvements, such negative interactions can significantly impact the utilisation of healthcare services, as individuals may choose to avoid the clinic altogether, to avoid disrespectful treatment. These findings align with the results of a study where 59.4% of participants reported that nurses’ attitudes were a primary barrier to accessing healthcare services. 23 Further findings revealed that inadequate knowledge among community members concerning mental illness and negative attitudes of nurses towards mental health patients were significant barriers to accessing mental health services. 25
A significant number of respondents (45.4%) either felt afraid of the staff or were uncertain as to whether their concerns or complaints would be taken seriously. This lack of confidence in voicing opinions or grievances can hinder effective communication and lead to patient dissatisfaction. Improving the interpersonal skills of healthcare workers, when interacting with clients, could reassure individuals that their voices matter, yielding positive results. Studies that confirm this finding show that 61.2% of participants identified the nurses’ lack of desire to communicate with patients as a major barrier to accessing healthcare services.23,27-29 In another study, older individuals feared complaining directly to healthcare workers, as this could result in punitive reactions, such as having their files placed at the end of the pile – an experience some had witnessed or endured. The results further revealed that a lack of patient-centredness, prompt attention and communication led to a lack of trust in the healthcare system and health professionals.30,31
The study findings revealed that almost half (45.6%) of the respondents typically spend more than 3 hours at the clinic. This extended waiting time is considered excessive for outpatient health facilities and can act as a barrier to the utilisation of healthcare services. According to the ‘National Policy on Management of Patient Waiting Time in Outpatient Departments’, the acceptable waiting time, including the time of receiving service, is 3 hours.32-34 Although more than one-third (n = 152, 37%) of the respondents spent less than 3 hours at the clinic, over 84.1% (n = 258) felt that the time spent was too long. Of those who felt the waiting time was excessive, only 22% (n = 76) were provided with an explanation for the delay in receiving healthcare services. Redress is an integral aspect of the Batho Pele principles, which emphasise the importance of addressing any shortcomings or failures in service delivery. 35 Therefore, it is essential to prioritise redress, whenever there is a delay in rendering healthcare services. In a study on perceived barriers to primary care services in Saudi Arabia, waiting time was identified as a leading barrier to accessing primary healthcare services, with 83.4% of participants agreeing or strongly agreeing that they had to wait a long time before seeing a primary healthcare physician. 17 In contrast to both the findings in Saudi Arabia and the current study, the majority of participants – 65% females and 72% males – expressed satisfaction with the time spent for both inpatient and outpatient healthcare services. 36 Similarly, a study on the association between wait times and patient satisfaction found that the majority of the patients waited between 31 and 40 minutes to see a doctor, with one-third of the patients overall reporting satisfaction with the waiting time. 37
The study results revealed that males sought treatment for minor ailments at the health facility more frequently than females. This underutilisation of healthcare services by women may lead to delayed diagnosis and treatment of health conditions, leading to poorer health outcomes and increased mortality rate. Similarly, a study conducted in Pakistan revealed that low healthcare services utilisation is higher in women (37.8%) than in men (33.8%). 38 This contradicts the common assumption that females tend to use healthcare facilities more often than males. Contrary to these findings, another study revealed that females used healthcare services more (61%) than men (38.4%). 39 It was revealed that women aged 25 to 50 had an 8.244 times higher probability of being high users of healthcare services compared to those under 25 years of age. In contrast, for men, the odds in the 50+ years age group were 0.734, indicating that older men were 27% less likely to utilise primary healthcare services compared to those aged 25 to 50 years. 40
The study findings indicated that the elderly population utilised the health facility for minor ailments more frequently compared to their younger counterparts. This is expected as the immune system of older individuals tends to be weaker, making them more susceptible to minor ailments. Additionally, the aging process often brings about health challenges that may require medical attention. In contrast with these findings, a study on age, sex and primary healthcare setting differences in patients’ perception of community healthcare-seeking behaviour revealed that participants under 50 years sought healthcare services more frequently (67.2%) compared to those aged 50 years and above (32.8%). 39 These findings align with fundings of a study on healthcare services utilisation which showed that older individuals used healthcare services more frequently: 40 to 64 years (34.3%), 65 to 84 years (27.4%), compared to the younger people aged 0 to 19 years (11.3%), and 20 to 39 years (20.8%). 41
The research findings revealed that overall, there is not a significant difference in the utilisation of the health facility for minor ailments across most educational groups, with utilisation rates ranging from 78.3% to 100%. However, two exceptions were noted: the grade 8 to 10 group with a utilisation rate of 62.9% and the grade 11 to 12 group with a utilisation rate of 61.8%. These two educational groups demonstrate lower utilisation rates compared to the others. A study conducted in Brazil contradicts these findings, as their findings revealed a strong positive association between the use of public healthcare services and the level of education. In 2003, the use of healthcare services was higher among individuals with lower education levels, whereas in 2015, the analysis found that the use of public healthcare services was 44% higher among individuals with a lower level of education compared to those with higher education levels. 42 Similarly, results of another study revealed that education has a positive influence on the utilisation of maternal healthcare services. Compared with uneducated women, higher educated women were almost 2 times, 3.6 times and 1.6 times more likely to have ⩾ ante-natal visits, institutional delivery and post-natal check-ups, respectively. 43
The study findings established that the younger generation (18-24) had the highest utilisation rate of contraceptives, which is a positive outcome. It shows that young women are actively seeking and utilising family planning services to prevent unintended pregnancies. Conversely, utilisation rates gradually decreased among older age groups, with the lowest utilisation rate observed among women aged 40 to 49. This is expected as some women in this age group may have reached menopause or are no longer fertile, leading to a lower need for family planning services. In line with these findings, a study conducted in Saudi Arabia revealed that 68.9% of women who used contraceptives were very educated (P = .031), not working (P = .000) and within the age of 26 to 35 years. 44 These findings differ from those of a study on contraceptive use, where 63.6% of the respondents used contraception, with the majority being from the age group 35 to 49 (54.77%), followed by the age group 25 to 34 (33.97%), and the least users being from the age group 15 to 24 (11.26%). 43
A very low percentage_13.5% of the total sample, took chronic medication at the local clinic, indicating a potential gap in the management of chronic conditions within the population. The findings further indicated that a greater proportion of males missed their appointments and disengaged from their treatment compared to females. This observation reinforces the notion that females tend to exhibit higher treatment adherence compared to males. Findings of a study discovered that young women demonstrated much better adherence than young men. Additionally, the findings suggested that the side effects of anti-hypertensive pills on the sexual function of older men may contribute to their low or non-adherence compared to older women. 45 A study on adherence to treatment and related factors among patients with chronic conditions in primary care found that 24% of participants stopped taking their treatment because it made them feel bad. 46
Conclusion and Recommendations
The study aimed to identify and describe factors influencing healthcare utilisation of services among residents of a rural village in the Ehlanzeni district. Findings revealed that barriers, such as beliefs and myths about disease causation and treatment, resource shortages such as lack of nurses, doctors, medicine, and limited facility capacity, negative staff attitudes, lack of interpersonal skills among nurses, and long wait times, were identified as negatively impacting healthcare service utilisation and access leading to low patient satisfaction. Conversely, enabling factors that positively influence healthcare service utilisation include the ability to choose the local healthcare facilities, and perceptions of nurses’ competence, as well as the physical accessibility of facilities. The research findings on barriers to healthcare services access and utilisation, such as shortage of resources, long waiting times and poor engagement in care, are particularly relevant to the local rural context, where limited healthcare resources and suboptimal engagement in care are common challenges.
The research emphasised the necessity to enhance patient treatment engagement in care to enhance adherence with chronic conditions, education and collaboration with traditional healers and community to dispel myths and beliefs surrounding disease causation, review policy regarding meetings to reduce extended waiting times, bolster staffing levels, and foster positive attitudes among healthcare providers towards patients, redress concerns with the community to improve healthcare service utilisation and access in rural areas. Conversely, it is essential to maintain the existing enabling factors. These recommendations could be accomplished by developing strategies to enhance reviewing existing healthcare policies regarding quality in healthcare for South Africa based on community and patient concerns including: equitable funding distribution- ensuring fair allocation of resources between public and private sectors such as National Health insurance to improved access to healthcare services for all with patient centred care and -increasing patient participation and treating them with respect and dignity; evidence-based practice-expanding research on effective interventions and promoting appropriate use of healthcare services; and error reduction-implementing measures to minimise healthcare errors.
Study Limitations and Strengths
Quantitative studies have limited depth; therefore, it is possible for this study not to capture contextual information, but superficial or unrelated information. The study was conducted in one village only, where the health facility under study is situated; consequently, individuals who do not reside in this village but use the health facility as their primary healthcare provider were excluded. Young people, under the age of 18, who are capable of making decisions regarding their health, for example, high school learners, who often use the health facility for contraception services, and those in child-headed families, were excluded from the study. The sampling may be prone to periodic bias, as a significant portion of data was collected during the week when many working individuals were absent from their homes due to work commitments. This timing may have led to the exclusion of their perspectives. The use of a structured questionnaire with pre-determined questions and responses limited the opportunity for respondents to elaborate on their answers, and maybe potential for response bias as respondents may not answer truthfully or accurately. Therefore, this cannot be generalised to the whole sub district or other areas in the province; however, utilising the random sampling method, ensured that every individual in the population had an equal opportunity for selection, leading to reduced bias and enhancing the representativeness and generalisability of the study findings to the whole community. On the other hand, the study provided a basis that can guide policymakers and local healthcare facility managers to develop evidence-based strategies that can improve healthcare utilisation and access in the rural areas, based on the responses of community members who participated in the study. Future research would be beneficial to conduct the study in the whole district, possibly through qualitative studies, to explore the experiences and perspectives of community members. This approach would provide a deeper understanding of the subject matter and offer valuable insights for further research or policymaking.
Supplemental Material
sj-doc-1-his-10.1177_11786329251356931 – Supplemental material for Barriers and Enablers of Health Services Utilisation in Rural Communities of Nkomazi Sub-District in Mpumalanga Province, South Africa: A Quantitative Community Survey
Supplemental material, sj-doc-1-his-10.1177_11786329251356931 for Barriers and Enablers of Health Services Utilisation in Rural Communities of Nkomazi Sub-District in Mpumalanga Province, South Africa: A Quantitative Community Survey by Nonhlanhla Fortunate Metiso and Sheillah Hlamalani Mboweni in Health Services Insights
Footnotes
Acknowledgements
We sincerely thank the Department of Health and traditional and political leadership for granting permission to conduct our study in the community. We are grateful to the community members for their valuable participation, which has greatly contributed to this study’s findings.
Author Contributions
NF originated the study, formulated the protocol, and conducted data collection and analysis, while SH evaluated the data analysis process, reviewed the writing, and endorsed the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.