
Abstract
Objectives:
The primary purpose of this study was to assess the knowledge and prevalence of cervical cancer screening (CCS) among women attending prenatal care clinics in the Okaikwei North Municipal Assembly (ONMA) in the Greater Accra region, Ghana. The study also aimed to examine whether there were differences in CCS knowledge between the women attending the prenatal care clinics.
Design:
This study utilized a cross-sectional, quantitative approach and a two-stage cluster sampling method.
Setting:
The study involved 393 women receiving prenatal care at three health facilities in the district, namely NK Salem Medical Centre Hospital (NMCH), Achimota Hospital (AH), and Lapaz Community Hospital (LCH).
Primary outcome:
Level of Knowledge and Prevalence of CCS.
Results:
The sampled participants from the three hospitals were Achimota (36.6%), Lapaz Community (32.1%), and NK Salem (31.3%). The mean age (SD) was 29.7 (±3.8) years. The age group 21 to 30 years formed the majority (57.8%). The prevalence of CCS among women receiving prenatal care was 7.4%; although most of them had heard about CCS, a proportion (46.5%) of them did not know CCS was, and only 33.9% knew Pap Smear as the test for detecting cervical cancer. A very small proportion (19.8%) of the women receiving prenatal care had CCS knowledge. There was a statistically significant difference in mean knowledge by 1.47 between women receiving prenatal care at AH and LCH, as well as by 1.82 between NMCH and LCH.
Conclusion:
There was a very low knowledge and prevalence of CCS in the district. Knowledge of CCS differed significantly between the health facilities in the district.
Strengths and Limitations of the Study
The study was a cross-sectional study involving only women receiving prenatal care above 18 years.
The study had a good response rate of 92.9%, that is, with 393 out of 423 selected respondents.
The study focused on assessing the Knowledge and Prevalence of CCS among three health facilities having a high prenatal care attendance rate in the district.
The study was carried out among three prenatal care facilities using a two-stage sampling to avoid selection bias in the Okaikwei North District.
The study was comprised of women receiving prenatal care who may have different socio-demographic characteristics compared with the general population, and this raised limitations.
Study results may not be generalizable to the larger population, for example, among older age groups due to the contextual or demographic background of the participants and the study setting. Further research can be done nationwide to accurately ascertain a proper representation of knowledge and prevalence of CCS in Ghana.
Introduction
Cancer, characterized by the uncontrollable growth of cells in the body, is a disease with nomenclature derived from the initial site of manifestation, regardless of subsequent spreading.1,2 Cervical cancer (CC) develops in the cervix, the lower part of the uterus connecting to the vagina. Described as a slow-growing cancer, CC may lack symptoms but can be detected through regular Pap tests, involving the microscopic examination of cells scraped from the cervix. The World Health Organization (WHO) estimates that 99% of CC cases are linked to human papillomavirus (HPV), a sexually transmitted infection. The American College of Obstetricians and Gynecologists (ACOG) recommends CCS to identify precancerous changes using Pap smears and HPV testing. 3
Cervical cancer is a major public health issue and a leading cause of mortality and morbidity among women globally. 4 Annually, CC incidence of 528 000 and 266 000 deaths occur, with over 85% of cases concentrated in low-middle-income countries (LMICs), particularly sub-Saharan Africa (SSA). 5 Compared to incidence rates below 2 per 100 000 in Western countries, Ghana has a high incidence of CC, with estimates ranging from 18.3 to 29.3 per 100 000 women per year reflecting the disproportionate CC burden in African nations.5,6 The high prevalence of human papillomavirus (HPV) infections combined with limited screening contribute to Africa’s high CC rates. 7 Estimates indicate over 3000 new cases are diagnosed yearly in Ghana, making CC the second most common female cancer after breast cancer.8,9 The incidence and mortality continue to rise in sub-Saharan Africa, especially in lower-middle-income countries like Ghana, largely due to the absence of nationwide screening policies and programs.10,11
Ghana has worryingly low CCS rates of 2% to 3%. 12 Lack of public knowledge and awareness pose barriers to screening in Ghana.11,13 Less than half of African women correctly identify CC risk factors, signs, prevention approaches, and treatment options. 14 Screening allows early detection and treatment of precancerous lesions before progression to invasive cancer. 15 Ghana endorses CCS with visual inspection with acetic acid for women between the ages of 25 to 45 years.16,17
Without systematic national prevention, screening, and treatment initiatives, reproductive-aged women in Ghana remain at high risk of developing and dying from CC. 18 Pregnant women face a heightened risk of CC due to hormonal changes and their frequent contact with healthcare systems during prenatal care. Integrating CCS into prenatal visits offers a crucial opportunity for education and screening, enhancing early detection and reducing mortality. Prenatal care offers a structured and routine setting to address CC risks, improving early detection rates and potentially decreasing mortality. Moreover, prenatal care facilities can serve as effective platforms for public health interventions, including education on CC prevention. Currently, most CCS occurs via opportunistic physician referrals during unrelated consultations or episodic outreaches by NGOs yielding poor uptake. 19 Establishing regular evidence-based screening for women aged 25 to 49 years could decrease advanced cancer rates by 90%. 20
Some studies in Ghana have examined CCS knowledge and prevalence but none have focused on high-risk groups such as pregnant women and further existing research does not explore differences in CCS knowledge among women receiving care at various health facilities, 21 and determine the difference in knowledge among groups.9,22 This study aims to assess CCS knowledge and prevalence among women attending prenatal care in the Okaikwei North Municipal District and identify disparities in knowledge across health facilities. Understanding these differences is critical for developing targeted educational interventions. The research questions are (1) What is the Level of knowledge of CCS among women receiving prenatal care? (2) What is the prevalence of CCS among women receiving prenatal care? and (3) Is there a difference in knowledge of CCS among women receiving prenatal care attending the different health facilities?
Methodology
Study Area
The study investigated women receiving prenatal care attending selected hospitals under the Okaikwei North District. “The Okaikwei North Municipal Assembly (ONMA) or District is one of the thirty-eight newly created District/Municipal Assemblies inaugurated on Thursday, 15th March 2018 across the country under the President of Ghana, His Excellency Nana Addo Dankwa Akuffo – Addo. The population of the Okaikwei North Municipal Assembly (ONMA) is currently 160 446 according to the 2021 population and housing census. This figure includes 78 421 males and 82 025 females. 23 The capital of the Municipal Assembly is Abeka. It is currently among one of the Two Hundred and Sixty (260) Metropolitan, Municipal, and District Assemblies (MMDAs) in Ghana and one of the Twenty-Nine (29) MMDAs in the Greater Accra Region. It was carved from the Accra Metropolitan Assembly on 14th November 2017.” 24 The average number of pregnant women attending the various facilities may however signify that many others do not reach out to the prenatal clinic services.
Profile of Achimota Hospital (AH)
The hospital, inaugurated in 1927, was large enough to service the healthcare needs of the Achimota School and its sister schools until it was taken over by the Ministry of Health in 1973. It has now expanded its services beyond its immediate surroundings, including comprehensive obstetric care, family health, and, most recently, orthopedic and accident and trauma care. It is a public district hospital now offering comprehensive services including obstetric care. It has an average prenatal care attendance of 78.2 women per clinic day. 25
Profile of Lapaz Community Hospital (LCH)
The Lapaz Community Hospital Limited, a private clinic, was established in September 2003 per the Companies Act of 1963 (Act 179). Uncompromised prenatal care is provided to expectant mothers at Lapaz Community Hospital. Pregnant women receive support, reassurance, and information about pregnancy and birth, as well as tests and examinations to determine the health of both the mother and the unborn child, during prenatal care appointments. They have an average prenatal care attendance of 71 women per prenatal care clinic day. 26
Profile of Nk-Salem Medical Centre Hospital (NSH)
Modern medical technology is used throughout Nk Salem Medical Center. To help the people of Achimota and beyond, this was founded in March 2020. They provide services to a variety of people with insurance, including those with private insurance. The Hospital runs the following clinics: prenatal care clinic, general care, eye clinic, and dietician clinic. There is an average of 51 women receiving prenatal care per prenatal care clinic day. 27
Study Design
A quantitative methodology and cross-sectional design were used to undertake the study. The study was conducted in three health facilities within the Okaikwei North District in the Greater Accra region to ascertain the level of knowledge and prevalence of CCS among women receiving prenatal care who attended the facilities for maternal care. A two-stage cluster sampling method was used; thus, the district was divided into clusters, and hospitals were selected at random from each stratum. The two-stage cluster sampling method was chosen to enhance representativeness and logistical feasibility. In the first stage, as mentioned, the district was divided into clusters based on geographical boundaries and healthcare facilities. From these clusters, three health facilities were selected at random. In the second stage, eligible participants were randomly sampled from the attendance lists of these facilities. This method was preferred over simple random sampling to account for the heterogeneity of the population across different locations. Randomization was performed using Microsoft Excel to ensure unbiased selection and reduce selection bias. This type of sampling is a kind of probability sampling procedure used to select samples from clusters such as cities, countries, and other geographical areas. 28 The list of women receiving prenatal care booked for appointment was obtained and randomized in Microsoft Excel to allow a simple random sampling. The participants who consented to the study were recruited. The inclusion criteria for the study comprised all pregnant women above 18 years of age who were seeking antenatal care and were in a good frame of mind. The exclusion criteria included pregnant women on admission, those visiting for purposes unrelated to prenatal care, and post-natal women seeking care. The sampling frame consisted of all women receiving prenatal care who were above 18 years old, excluding health professionals, post-natal women, and pregnant women admitted for other medical reasons.
Sampling Procedure
Data collection for the study was conducted using an in-person questionnaire administered on the Research Electronic Data Capture (REDCap). The primary language used for the data collection instrument was English; however, for a few participants who did not understand English, Asante Twi was utilized. The research assistant facilitated the administration of the questionnaires at the health facilities after receiving the necessary approval from the authorities. Recruitment of participants involved following a randomized list of attendees. Women who consented to participate in the study were subsequently recruited during their visits to the clinics (Supplemental Material).
Quantitative Sample Size
The sample size calculation below was adopted to determine the sample size for the study.
The sample size is as below.

Where:
Z = “level of confidence (CI)” – This gives the level of uncertainty in the sample mean or prevalence as an estimate of the population mean or prevalence. The probability value for the confidence interval was set to 1.96 (95% CI)
P = Proportion – is the knowledge level of CCS in the population
e = margin of error, which also influences the power of the study (1 − β).
Therefore, with the estimated level of knowledge in the population set to P = 50.0%, and CI of 95% using a 1.96 probability value (Z) and 5% margin of allowable error, the minimum sample size required for the study is 385 women receiving prenatal care. The sample size was scaled up to 423 to make room for a 10% non-response rate. Table 1 specifies the proportion of women expected from each based on the attendance figures per facility per clinic day.
Sampling Proportion.

Data Collection Instrument and Analysis
The data collection instrument from literature was developed by authors, it was piloted and after collective reviews utilized for the study. The data collection tool contained binary and multiple-choice closed-ended questions, there were no Likert scale questions. The target participants were women receiving prenatal care and they were chosen because they were one of the risk groups for CC owing to their sexual activities,29,30 the prevalence of STD among them, 31 accessibility for efficient data collection, they represent reproductive women, may have future screening opportunities. Face and content validities were conducted to authenticate the knowledge instrument. The content validity index (CVI) score of 0.79 was determined through a panel of five experts. They rated each survey item on a scale from “1” (not relevant) to “4” (highly relevant). The Item-Level CVI (I-CVI) was calculated as the proportion of experts who rated the item as 3 or 4. The Scale-Level CVI (S-CVI) was then determined by averaging the I-CVIs across all items.
The Independent variables were sociodemographic variables such as age, marital status level of education, etc. The dependent variables were knowledge (level of knowledge) and the Prevalence of CCS. Data cleaning was performed and expectation maximization an iterative algorithm for finding maximum likelihood estimates of model parameters in the presence of missing data 32 was applied to handle missing data. This approach was specifically chosen because missing data constituted approximately 5% of the dataset, making EM an appropriate method to ensure robust parameter estimation without significant data loss.
Descriptive statistics was done making use of frequency tables and graphs. Knowledge was measured using 12 questions. All correct answers were assigned a value of “1,” and wrong answers a value of “0.” Total composite scores knowledge was graded as poor or low or 0 to 4 marks, moderate for 6 to 8 marks, and high for 9 to 12 marks. The knowledge cutoff points or grading were classified using quartiles/percentiles to account for skewness (right skewness), ensuring low, medium, and high categories reflect the knowledge scores distribution.33,34 The descriptive section reported the knowledge and prevalence of CCS.
Data analysis was conducted using analysis of covariance (ANCOVA). Preliminary analyses revealed significant demographic differences between the healthcare facilities in terms of age, marital status, income level, employment status, and pregnancy status of the participants. Given these baseline differences, data analysis was conducted using ANCOVA with Type III sum of squares to compare CCS knowledge scores across the three healthcare facilities. This model was chosen because the Type III sum of squares is appropriate for unbalanced designs and provides tests for main effects that control for all other effects in the model. The ANCOVA model included healthcare facility type as the fixed factor, with age, marital status, income level, employment status, and pregnancy status as covariates to control for these identified demographic variations between facilities that could potentially influence CCS knowledge independent of the facility type.
The dependent variable was the knowledge score, with the healthcare facility as the independent variable. Covariates included age, pregnancy status, marital status, employment status, and income level. Estimated marginal means were calculated, and pairwise comparisons were performed using the Least Significant Difference method. Statistical significance was set at P < .05. The analysis aimed to identify differences in CCS knowledge levels between facilities while controlling for demographic and socioeconomic factors.
Study Hypothesis
Ho: There is no difference in the level of CCS knowledge among the women receiving prenatal care at the health facilities
H1: There is a difference in the level of CCS knowledge among the women receiving prenatal care at health facilities
The primary outcomes of the study were Knowledge and Prevalence of CCS.
Patient Involvement
Patients and the public were not involved at the initial stages of the study but strategically integrated during the data collection piloting phase to ensure their perspectives were accurately captured. Their input played a vital role in refining the data collection process, enhancing participant comfort, and optimizing the validity of the study outcomes.
Ethical Clearance
This study involved human participants and was approved by GIMPA IRB with reference GM/IRB/2023/12. Lastly, the proposal was reviewed and approved by the management boards of the three facilities before the commencement of data collection at each site. Written informed consent was obtained from all respondents before administering the questionnaires, ensuring that participants were fully informed about the study’s purpose, procedures, potential risks and benefits, and their right to withdraw at any time without penalty. For non-English speaking participants, the trained research assistants provided oral translations to ensure comprehension. To support this process, the questionnaire was largely transcribed into local languages to guide the research assistants during questionnaire administration. This approach ensured accuracy and consistency in delivering the questions while maintaining the integrity of the informed consent process.
Results
Demographic Data/Characteristics of Respondents
Of the 423 women targeted for the prenatal care study, 7% did not respond, resulting in a final sample size of 393 respondents. These respondents were recruited from three facilities: Achimota Hospital (36.6%, n = 144), Lapaz Community Hospital (32.1%, n = 126), and NK-Salem Medical Centre (31.3%, n = 123). Overall, the respondent’s ages ranged from 18 to 41 years, with a mean age of 29.7 years (SD ± 3.8). The specific mean ages across the facilities were similar (29-30 years), yet the difference was statistically significant (P < .001). This is further supported by the differences observed in the age group distribution (P = .03). Marital status, pregnancy status, education level, employment status, and income range (P < .001) all exhibited statistically significant differences among the hospitals. Lapaz Community Hospital had the largest proportion of women with higher incomes (above GHC 1000). Religious affiliation did not differ significantly among the hospitals (P = .33) (Table 2).
Respondents’ Basic Characteristics.
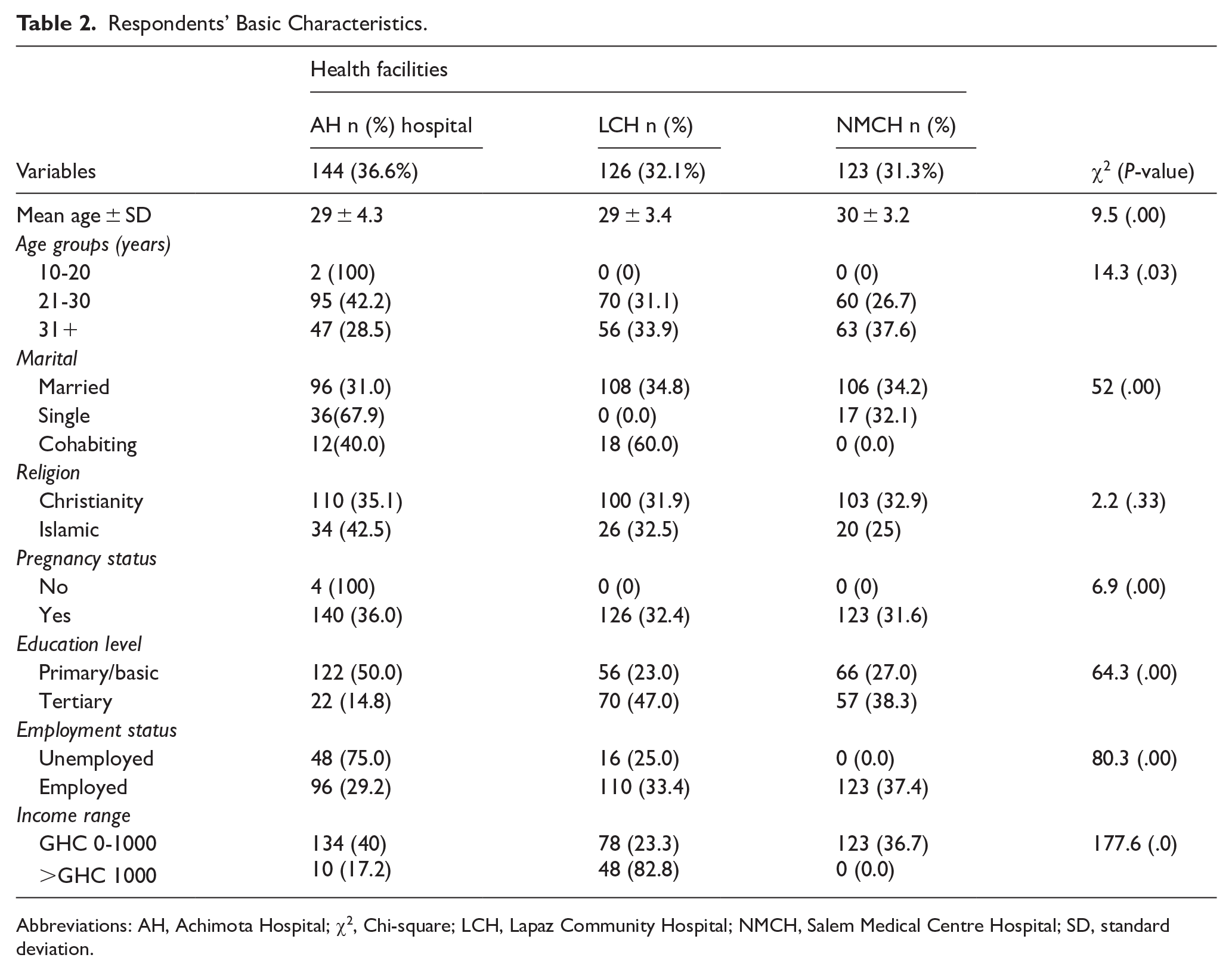
Abbreviations: AH, Achimota Hospital; χ2, Chi-square; LCH, Lapaz Community Hospital; NMCH, Salem Medical Centre Hospital; SD, standard deviation.
Knowledge and Prevalence of Respondents on CCS
In Table 3, a greater proportion of the respondents had heard about CC (75.6%) and CCS (68.4%). Although a majority of them had heard about CCS, a proportion of them had no idea or did not know what CCS was (46.5%), at what intervals screening should be done (71.7%), or the age recommended for screening (62.0%), 24% of them didn’t know which people are to be screened (Figure 1) and 64.5% didn’t know what type of test checks for CC. Further, only 33.9% of the respondents mentioned Pap Smear was the test done to check for the CC. Regarding sources of CCS information (Figure 2), the majority mentioned Social Media (YouTube/ Facebook, etc.) (31.0%).
Knowledge of Respondents on CCS.

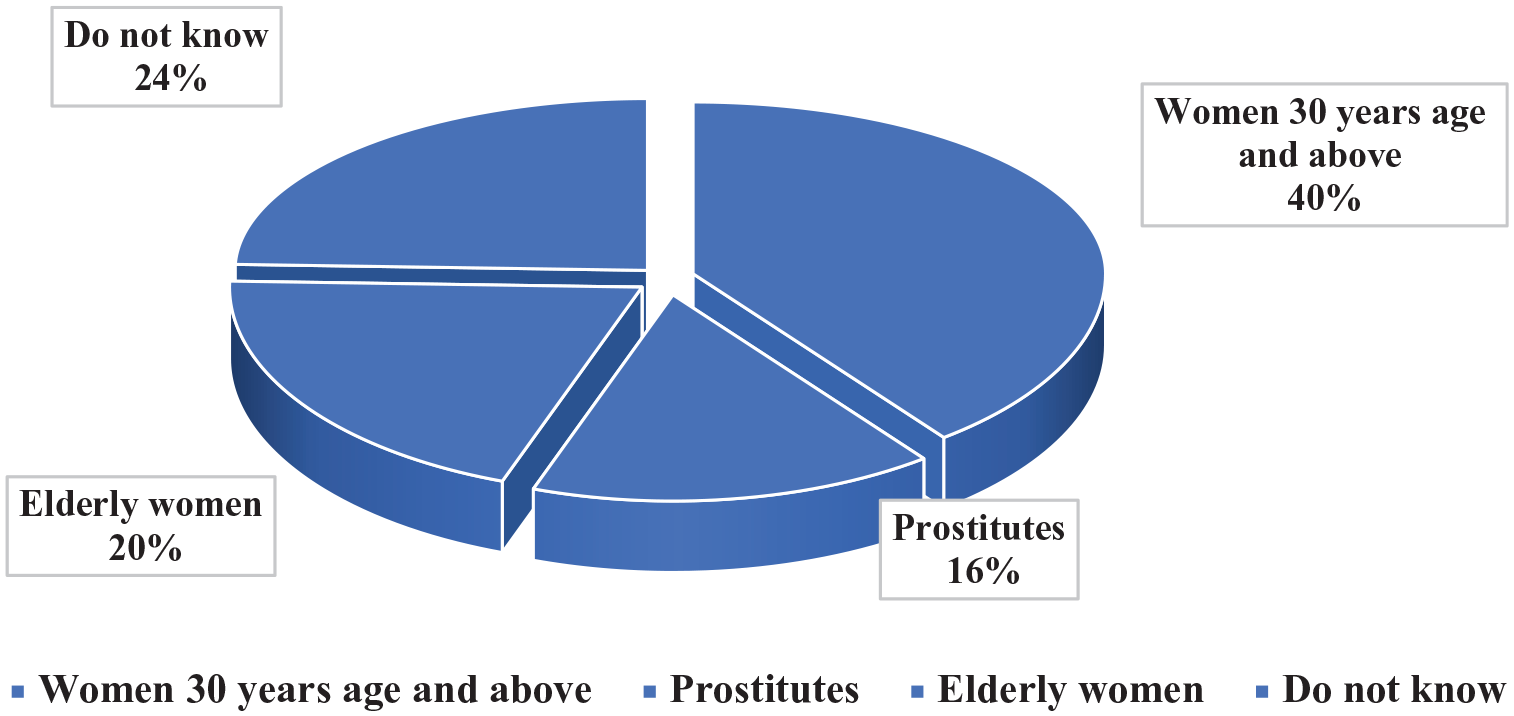
Which people are to be screened?

Sources of information on cervical cancer screening.
Concerning CCS Knowledge risk factors, the respondents indicated having many sex partners (23.3%), having STI infections (18.0%), and having early onset of sex (13.1%) were the top risk factors for CC. The majority reported all forms of STI were risk factors for CC. A greater proportion (60%) of the respondents had screened for STIs before. Almost all of the respondents had not been screened to test for CC before, they formed 90% of the entire women. The prevalence of CCS was very low (7.4%) (Table 3).
Knowledge Score on CCS
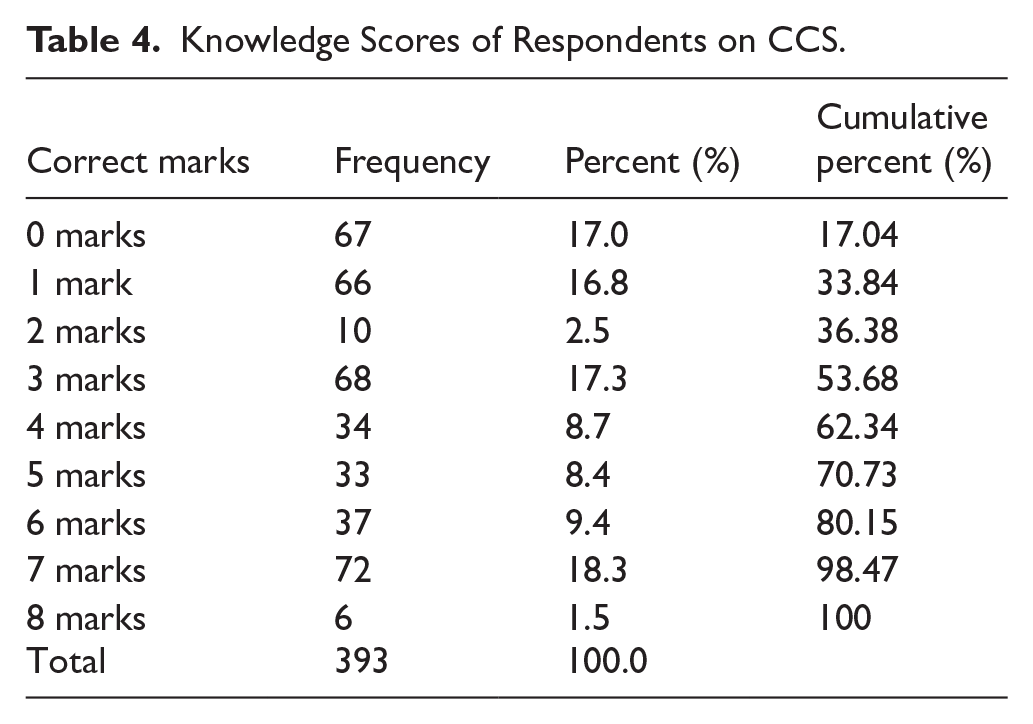
The mean and standard deviation of the CCS knowledge score among respondents were 3.0 ± 2.57, respectively. Respondents’ knowledge of CCS was assessed out of a total of 12 based on correct responses, with only a few (1.5%, n = 6) achieving a maximum score of 8, indicating an overall low level of knowledge. The majority (98.47%) scored below 8, demonstrating poor knowledge of CCS. Knowledge scores were categorized using percentile-based classification as follows: low knowledge (<1 mark, 17.0% of respondents), medium knowledge (scores between 1 and 6 marks, 63.1% of respondents), and high knowledge (>6 marks, 19.8% of respondents). In summary, only a small percentage (19.8%) of respondents had high CCS knowledge (Table 4).
Knowledge Scores of Respondents on CCS.
Assessment of CCS Knowledge Scores Across the Healthcare Facilities
Figure 3 illustrates the differences in CCS knowledge levels among respondents at the three health facilities. Notably, knowledge levels were higher among women receiving prenatal care at Achimota Hospital compared to the other two facilities. To statistically test these differences, a one-way ANCOVA was conducted to evaluate the effect of the hospital (Achimota Hospital, Nk-Salem Medical Centre, and Lapaz Community Hospital) on CCS knowledge scores while controlling for demographic covariates (age, education, marital status, pregnancy status, employment status, and income). The following hypotheses were tested:
Ho: There is no difference in the level of CCS knowledge among women receiving prenatal care at the health facilities.
H1: There is a difference in the level of CCS knowledge among women receiving prenatal care at health facilities.

CCS knowledge scores among women receiving prenatal care at the health facilities.
Table 5 presents the results of the one-way ANCOVA. After adjusting for the covariates, there was a statistically significant effect of the hospital on CCS knowledge scores, F (2, 384) = 75.03, P < .001, ηp2 = .281, thus the hospital facility accounted for approximately 28.1% of the variance in CCS knowledge scores, beyond the effects of demographic factors. This suggests that inter-hospital differences in CCS knowledge may be influenced by facility-specific factors such as variations in patient education programs, access to health information, or differences in healthcare provider engagement. Among the covariates, age (F (1, 384) = 13.76, P < .001, ηp2 = .035), education (F (1, 384) = 9.91, P = .002, ηp2 = .025), marital status (F (1, 384) = 64.44, P < .001, ηp2 = .144), and income (F (1, 384) = 88.45, P < .001, ηp2 = .187) significantly contributed to the model. However, pregnancy status (F (1, 384) = 2.14, P = .145, ηp2 = .006) and employment status (F (1, 384) = 6.48, P = .011, ηp2 = .017) had limited influence.
Analysis of Covariance Results for Knowledge Scores by Hospital with Demographic Covariates.

Abbreviations: df, degrees of freedom; ηp2, partial eta squared (effect size); F, F-ratio; MS, mean square; SS, sum of squares.
R2 = .369 (adjusted R2 = .356).
Comparison of CCS Knowledge Scores Among Respondents at the Facilities
Pairwise comparisons revealed that women receiving prenatal care at Achimota Hospital (M = 4.33, adjusted) and Nk-Salem Medical Centre (M = 4.74, adjusted) had significantly higher CCS knowledge scores compared to those at Lapaz Community Hospital (M = 1.25, adjusted). Further, Achimota General Hospital’s CCS Knowledge score was significantly higher than Lapaz Community Hospital’s (mean difference = 3.08, P < .001), and Nk-Salem Medical Centre’s score was also significantly higher than Lapaz Community Hospital’s (mean difference = 3.49, P < .001). However, no significant difference was found between Nk-Salem Medical Centre and Achimota General Hospital (P = .078). The univariate test confirmed a significant overall effect of hospital/clinic on Knowledge scores (F (2, 385) = 54.63, P < .001) (Table 6).
Comparison of Knowledge Scores Among Respondents at the Facilities.

Abbreviation: CL, confidence interval.
Significant = “*”.
Key Results
The key results are outlined according to the study objectives as seen below.
(1) The level of CCS knowledge among the women receiving prenatal care was low (19.8%).
(2) The level of CCS knowledge was significantly higher among women receiving prenatal care at Achimota Hospital and Nk-Salem Medical Centre compared to Lapaz Comm. Hosp.
(3) The prevalence of CCS among women receiving prenatal care was very low (7.4%).
Discussion
Knowledge and Prevalence Cervical Cancer Screening
The study focused on assessing the knowledge and prevalence of CCS among women attending prenatal care clinics in the Okaikwei North district in the Greater Accra region, Ghana. The findings of the study revealed that the majority (98.5%) of the participants had low CCS knowledge. The findings were consistent with similar studies conducted in different parts of Ghana; 69.7% by Gyamfua, Nkrumah, Ibitoye, Agyemang, Ofosu, Tsoka-Gwegweni and Cumber, 9 in Kenyase Bosore community, Ashanti Region; 52.7% by Nyaaba and Akurugu 35 among female health workers in the Upper East Region of Ghana; knowledge of CCS was low in a qualitative study conducted by Osei et al 36 in Oyibi Community, the eastern part of Greater Accra Region, etc. Further, beyond Ghana, a study done in Nigeria claimed that there was a lack of CCS knowledge (56.5%) and awareness of CCS and these influenced their hesitancy to uptake screening among other reasons, for example, expensive CCS and scarcity of CCS centers. 37 In three different cities in Adigrat town, Ethiopia, the CCS knowledge ranged from 38.1% to 53.3%. 38
Another finding was that there was a statistically significant difference in CCS knowledge among the women receiving prenatal care attending the health facilities in the district. The practical significance of these differences is essential to consider, as inter-hospital variations in CCS knowledge highlight gaps in awareness that require targeted interventions. Notably, the lowest knowledge levels were observed at Lapaz Community Hospital, which may be attributed to factors such as limited public health education efforts or fewer CCS awareness programs. Addressing these disparities through tailored health education initiatives at specific facilities could improve overall CCS awareness and uptake. The knowledge difference might be a result of unique interventions (ie, public health education) done already at the different health facilities. The difference in knowledge was important to study since lack of knowledge can be a reason for low CCS uptake. 37 A study found that women who received education from health professionals concerning CC and its screening had higher odds of uptake of CCS than those who did not receive the education. In furtherance, having knowledge of another who has CC was associated with good screening perceptions. 39
The study also found that socio-demographic characteristics such as income, marital status, age, and education level played a significant role in CCS knowledge. Among these, income (ηp2 = .187) and marital status (ηp2 = .144) had the strongest influence, suggesting that financial stability and spousal support may positively affect CCS awareness. Additionally, education and age contributed moderately to CCS knowledge, reinforcing the need for targeted health education programs that consider these demographic factors. Future interventions should be tailored to address knowledge gaps among younger, less-educated, and lower-income women.
Across the world, some studies have revealed a low prevalence of CCS which was consistent with this study’s finding. Another study conducted among fifty-five (55) Low- and Middle-Income Countries found that the median lifetime prevalence of CCS was 43.6% (range, 0.3%-97.4%). 40 Similarly, the prevalence of CCS in several regions in Cameroon was shown to be very low at 4%. 41 The reasons accounting for the low uptake of CCS could be a result of low CCS knowledge.
It is however noteworthy to note that, this study was conducted among women receiving prenatal care attending three health facilities in the Okaikwei North Municipal Assembly, located in the Greater Accra Region of Ghana had sampling limitations due to the lack of national representation. 42 Other limitations Included potential recall bias due to reliance on self-reported data, selection bias arising from the two-stage sampling approach, lack of generalizability due to its focus on a single district, and the absence of longitudinal data to assess changes in knowledge over time. 42 Specifically, the two-stage sampling method may introduce selection bias 43 if certain clusters are more likely to be selected, the single district may not represent all Ghanaian women receiving prenatal care, and self-reported data can be subject to recall and social desirability biases. 44 Additionally, pregnancy status was initially included in the model but was found to have a non-significant effect on CCS knowledge (P = .145, ηp2 = .006). Given its minimal impact, it may be excluded in future refined models. However, pregnancy status remains an important factor in maternal health, and further research may explore its potential influence on CCS uptake in different populations.
Synthesis
While this study was conducted among women receiving prenatal care at three health facilities in one district in the Greater Accra Region, the findings nonetheless expose major gaps in CCS knowledge and prevalence among pregnant Ghanaian women. Significant differences in CCS knowledge were observed across the health facilities these may be explained by the facility-specific factors, such as public health education initiatives as this may influence knowledge levels. This highlights the need for tailored interventions rather than a uniform approach. The low levels (knowledge and prevalence of CCS) observed in this population likely reflect broader educational and health system inadequacies nationwide in disseminating preventative information and services to women throughout their reproductive years. As such, the highlighted need for interventions promoting CC literacy, screening counseling, and improved structural support for access generalizes well.
Synthesizing results make clear major deficiencies in both knowledge and screening adherence, suggesting that the availability of information alone remains insufficient to drive utilization without addressing multi-level barriers. In particular, socio-demographic factors, that is, income and marital status had a significant impact on CCS knowledge, underpinning the importance of demographically tailored interventions. As prenatal care groups demonstrate particularly low knowledge-to-action gaps, targeting them early on could provide high-yield opportunities for advancing CC prevention. While further studies should explore specific barriers, the evidence points to an urgent need to implement multi-faceted interventions focused on health literacy, clinical counseling, and accessibility levers to reach the most vulnerable women in Ghana.
Conclusion
The study found a very low level of CCS knowledge and prevalence in the Okaikwei North district, emphasizing the urgent need to integrate cervical cancer education and screening into prenatal care programs. Differences in CCS knowledge across facilities suggest the importance of tailored interventions. Women at Achimota Hospital and Nk-Salem Medical Centre had higher knowledge than those at Lapaz Community Hospital. Strengthening referral pathways within prenatal care and considering socio-economic factors can improve screening uptake and additionally, addressing systemic barriers, such as cost and access, can improve screening uptake ultimately reducing CC incidence and mortality. Policymakers should prioritize targeted training for healthcare providers and community outreach to increase CCS awareness.
Recommendation
Based on the key results from this study indicating low knowledge and screening prevalence of CCS among women receiving prenatal care, the following are recommended.
Hospital Management should integrate structured CC education into routine prenatal care through health talks led by trained midwives and nurses, standardized educational materials, that is, posters, leaflets, digital content with language translations, and pre-and post-natal counseling sessions on CCS. The education should consider the socio-demographic characteristics and could also be extended to other at-risk groups. The content should cover risk factors, symptoms, prevention through HPV vaccination, screening modalities, and follow-up requirements since lack of awareness and knowledge impairs individual perception and influences their willingness to screen. 45 Developing culturally appropriate materials in local languages can improve comprehension and engagement. This is important as implemented in Kenya, where a policy led the government to integrate CC services into reproductive health clinics. 45
Some specific interventions for adoption are establishing mobile CCS screening clinics to enhance accessibility, integrating screening with prenatal care, and leveraging community health workers to conduct outreach and facilitate referrals. Tailoring interventions for different age groups can ensure more effective communication and uptake. Additionally, radio, television, and social media campaigns in local dialects should be utilized to increase CCS awareness. Conduct an assessment to identify facility-specific barriers to CCS knowledge and screening uptake to inform facility-specific policy and practical implications. Lastly, future research should conduct a multi-site study across different regions to examine geographic disparities in CCS knowledge and uptake.
Supplemental Material
sj-doc-1-his-10.1177_11786329251337851 – Supplemental material for Knowledge and Prevalence of Cervical Cancer Screening Among Women Receiving Prenatal Care in Accra, Ghana: A Cross-Sectional Study
Supplemental material, sj-doc-1-his-10.1177_11786329251337851 for Knowledge and Prevalence of Cervical Cancer Screening Among Women Receiving Prenatal Care in Accra, Ghana: A Cross-Sectional Study by Victor Akuoku and Michael Darko Ashaley in Health Services Insights
Footnotes
Acknowledgements
We would give our acknowledgment to the management of the hospitals stated above for allotting us all necessary assistance during the data collection.
Author Contributions
Victor Akuoku was the principal investigator, however, both Victor Akouku and Michael Darko Ashaley (MDA) planned and designed the study. Data collection and analysis was done by MDA and reviewed by VK. Discussion, synthesis, and recommendation of the report writing were completed by both VK and MDA. Submission of the article was done by MDA as the corresponding author. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Dataset available from the Zenodo repository, DOI: 10.5281/zenodo.8186699
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.