
Abstract
Insomnia is a sleep disorder that affects significant portion of the population. It can result in adverse health outcomes and increased healthcare utilization. The purpose of this review was to identify existing research on the association between insomnia and healthcare utilization. A five-stage scoping review process was conducted guided by the Joanna Briggs Institute process. Data sources searched through 2022 were PubMed, HINARI, Google Scholar and Cochrane, with additional studies identified through hand searching. Descriptive and exploratory analyses were conducted from the findings of the selected studies. After reviewing 124 references, 23 studies were selected. A strong and positive association between insomnia and healthcare utilization and healthcare costs was identified. We also found that insomnia was associated with absenteeism from work, lower work performance ratings, disability, difficulties in daily activities, and life dissatisfaction. An unexpected theme that emerged from the included studies is that there is a large population with persistent insomnia who do not seek help that could benefit from improved management. Findings suggest that identifying and managing insomnia could result in a decrease in healthcare utilization and costs. Further research is needed to determine the most effective methods of identifying and managing insomnia.
“The association between insomnia and healthcare utilization was strong and positive with the rate highest for inpatient care and lowest for prescription refill.”
Introduction
Insomnia is one of the most common sleep disorders. It is defined as complaints of difficulty falling asleep and maintaining sleep accompanied by daytime sleepiness and fatigue or functional impairment. According to the fifth edition of the Diagnostic and Statistical Manual for Mental Disorders a diagnosis of insomnia requires that symptoms occur for at least three nights a week for a duration of at least three months.1,50 The American Academy of Sleep Medicine and the Sleep Research Society recommend 7 hours of sleep by night for healthy adults. 2 Healthy People 2030 has set an objective to increase the proportion of adults who get enough sleep. 3 It is reported that 10–30% of adults and up to 75% of older adults experience insomnia. 4 Direct and indirect costs related to insomnia exceed $100 billion USD per year because of drug prescriptions, absenteeism, poor workplace performance, increased accident risk, and healthcare utilization. 5 Insomnia is reported to have increased during the COVID-19 pandemic across the globe and that nearly 40% of healthcare workers experienced insomnia during the pandemic. 6
Risk factors associated with insomnia include female sex, older age group, low socio-economic status, presence of some mental health conditions, stress, and absence of a regular sleep schedule or pattern. Insomnia is associated with conditions related to aging such as osteoarthritis and other degenerative diseases, hypertension, and diabetes. 7 Chronic insomnia can occur sometimes because of traumatic life events such as catastrophic occurrence, illness, or death of loved ones. In addition, consumption of substances that affect sleep, medical disorders like Alzheimer’s and gastro-esophageal disease have been found to be associated with chronic insomnia. Women are reported to be more at risk of developing insomnia because of hormonal shifts that occur during menstrual cycle, pregnancy, and menopause. Menopause often presents with hot flushes, night sweats and other symptoms which can interrupt sleep.7,8 Some studies reported veterans to be a vulnerable group for developing insomnia with an estimated 90% diagnosed with sleep disturbance and about 50% diagnosed with insomnia.9-11 Sleep disorders may occur in children and teenagers due to consumption of stimulants such as nicotine and irregular sleep schedules. 7
Research indicates that prolonged insomnia can lead to adverse outcomes such as reduced performance at school or low productivity at work, risk of road traffic accident, and diseases such as heart disease, diabetes, metabolic syndrome, and depression.2,12 Sleep problems are associated with falls among the elderly, 13 mental health problems, 14 and obesity. 15 Also, higher pain intensity was reported by patients who had difficulty falling and staying asleep.16,17 Although insomnia and its association with poor health outcomes is reported in the literature, the evidence linking insomnia and healthcare utilization is not as abundant. Therefore, the purpose of this scoping review was to investigate available evidence about the association between insomnia and healthcare utilization, to identify gaps in the research and make recommendations for future research, practice, and policy.
Methods
A scoping review of the literature was conducted. According to the Joanna Briggs Institute (JBI), Methodology for Scoping Reviews, 18 Arksey and O’Malley (2005), and Cochrane Institute guidelines, there are 5 steps for conducting scoping reviews: developing a protocol with a clear research question and eligibility criteria, searching the literature, study selection, charting characteristics of studies, and reporting results, implications, and recommendations.
JBI recommends the PCC mnemonic as a guide to construct a review. “P” stands for population or participants, “C” concept, and the last “C” context. We identified population [P] as patients diagnosed with insomnia or those who functional impairment. According to the fifth edition of the Diagnostic and Statistical Manual for Mental Disorders a diagnosis of insomnia requires that symptoms occur for at least three nights a week for a duration of at least three months.1,50 The American Academy of Sleep Medicine and the Sleep Research Society recommend 7 hours of sleep by night for healthy adults. 2 Healthy People 2030 has set an objective to increase the proportion of adults who get enough sleep. 3 It is reported that 10‐30% of adults and up to 75% of older adults experience insomnia. 4 Direct and indirect costs related to insomnia exceed $100 billion USD per year because of drug prescriptions, absenteeism, poor workplace performance, increased accident risk, and healthcare utilization. 5 Insomnia is reported to have increased during the COVID-19 pandemic across the globe and that nearly 40% of healthcare workers experienced insomnia during the pandemic. 6
Risk factors associated with insomnia include female sex, older age group, low socio-economic status, presence of some mental health conditions, stress, and absence of a regular sleep schedule or pattern. Insomnia is associated with conditions related to aging such as osteoarthritis and other degenerative diseases, hypertension, and diabetes. 7 Chronic insomnia can occur sometimes because of traumatic life events such as catastrophic occurrence, illness, or death of loved ones. In addition, consumption of substances that affect sleep, medical disorders like Alzheimer’s and gastro-esophageal disease have been found to be associated with chronic insomnia. Women are reported to be more at risk of developing insomnia because of hormonal shifts that occur during menstrual cycle, pregnancy, and menopause. Menopause often presents with hot flushes, night sweats and other symptoms which can interrupt sleep.7,8 Some studies reported veterans to be a vulnerable group for developing insomnia with an estimated 90% diagnosed with sleep disturbance and about 50% diagnosed with insomnia.9‐11 Sleep disorders may occur in children and teenagers due to consumption of stimulants such as nicotine and irregular sleep schedules. 7
Research indicates that prolonged insomnia can lead to adverse outcomes such as reduced performance at school or low productivity at work, risk of road traffic accident, and diseases such as heart disease, diabetes, metabolic syndrome, and depression.2,12 Sleep problems are associated with falls among the elderly, 13 mental health problems, 14 and obesity. 15 Also, higher pain intensity was reported by patients who had difficulty falling and staying asleep.16,17 Although insomnia and its association with poor health outcomes is reported in the literature, the evidence linking insomnia and healthcare utilization is not as abundant. Therefore, the purpose of this scoping review was to investigate available evidence about the association between insomnia and healthcare utilization, to identify gaps in the research and make recommendations for future research, practice, and policy.
Methods
A scoping review of the literature was conducted. According to the Joanna Briggs Institute (JBI), Methodology for Scoping Reviews, 18 Arksey and O’Malley (2005), and Cochrane Institute guidelines, there are 5 steps for conducting scoping reviews: developing a protocol with a clear research question and eligibility criteria, searching the literature, study selection, charting characteristics of studies, and reporting results, implications, and recommendations.
JBI recommends the PCC mnemonic as a guide to construct a review. “P” stands for population or participants, “C⃜ concept, and the last “C” context. We identified population [P] as patients diagnosed with insomnia or those who self-report symptoms of insomnia; concept [C] as healthcare utilization and context [C] as prevalence, associated factors, and international scope.
To address the research question, a systematic search was performed on the following databases: PubMed, HINARI, Google Scholar, and Cochrane. Four search terms were used: “association,” “insomnia,” “healthcare,” and “utilization.” During the search process, Boolean operators “AND” and “OR” were used to extend the search for different forms of the title. The search terms used included association*[relationship], insomnia*[sleeplessness], healthcare*[health service], and utilization*[use]. This scoping review included peer reviewed primary research studies using quantitative and qualitative designs that have been published in English Language between 2011 and 2022. The selection of studies within 10 years timeframe is recommended by JBI.
A total of 124 articles were retrieved from the selected databases. The literature search included analysis of the reference lists of the identified studies. Titles and abstracts were screened for eligibility against the inclusion criteria. Twenty-three articles met the criteria for the full text review. The Preferred Reporting Items for Systematic Reviews and Meta – Analysis (PRISMA) flowchart in Figure 1. Illustrates the search process and results. To present the data, a table was created with column headings denoting author, date, location, population, and study design. PRISMA [Preferred reporting items for the systematic reviews and meta-analysis]. Prisma 2020 flow disgram for new systematic review which included searches of data bases, registers, and other sources.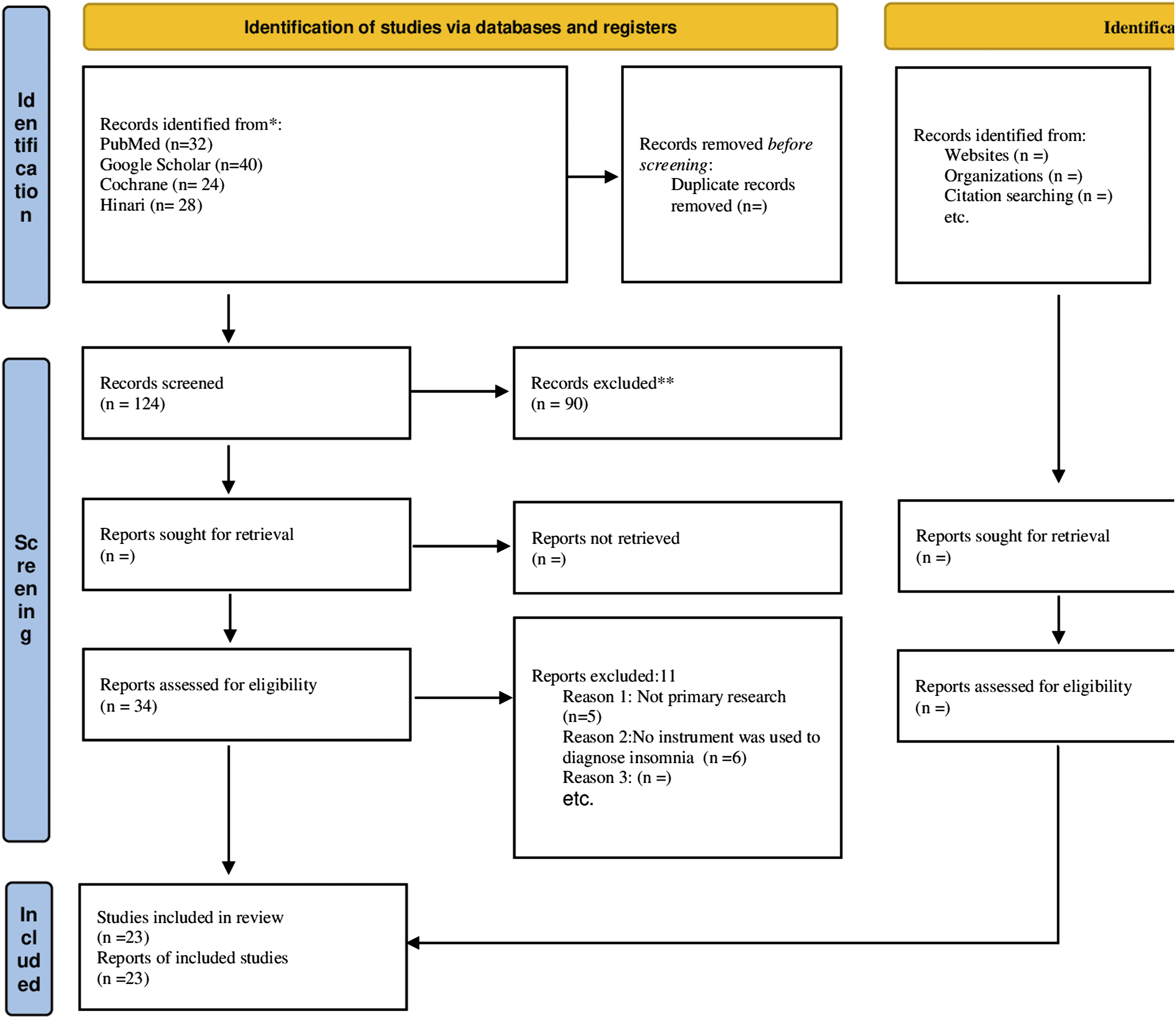
Table 1 lists the characteristics of the studies (see Appendix A).
Results
After analyzing the 23 studies based on the inclusion criteria, the following themes were identified: healthcare utilization, confounding comorbidities, other outcomes, barriers to identification, and treatment of insomnia.
Characteristics of Included Studies
Twenty-three studies were selected for the scoping review based on the inclusion criteria. Most of the studies were from the United States (52%), 2 were from the United Kingdom (9%), 2 from Australia (9%), three from Sweden (13%), one from the US and European Union (4%), one from Taiwan (4%), one from Finland (4%), and one from Hong Kong (4%).
Concerning the study design, 22 were case control, cohort, or cross sectional in design and one employed 1 mixed method study design [descriptive cross sectional and semi structured interview]. Many of the studies used large surveys such as the National Health and Wellness Survey 19 or the Women’s Health Initiative. 20 Others obtained data from claims records.21,22,24,25 Survey instruments used included the Insomnia Severity Index,17,26 the Pittsburgh Sleep Quality Index,13,27,28 the Epsworth Sleepiness Scale,26,28 Health Risk Assessment, Work Limitations Questionnaire, 30 and Health Related Quality of Life19 (HRQoL).
The Relationship Between Insomnia and Healthcare Utilization
A strong and positive association between insomnia and healthcare utilization and healthcare costs was identified.24,25,31-39 A trend analysis looking at data from the National Ambulatory Medical Care Survey (NHAMCS) found that office visits with insomnia as the stated reason for the visit increased from 4.9 million visits in 1999 to 5.5 million visits in 2010, a 29% increase. 40 Interestingly, data from the 2018 NHAMCS reports 10.7 million visits for disturbances of sleep, another 29% increase since 2010. The number and percentage of office visits accompanied by a prescription for a sleep medication also increased dramatically. 40 Anderson and colleagues (2014) found an insomnia diagnosis was associated with 26% higher healthcare costs at baseline and 46% higher in the 12 months after diagnosis compared to a matched cohort without a diagnosis of insomnia. 21 In addition, Wickwire and colleagues (2020) found that Medicare recipients with insomnia had higher rates of healthcare utilization across all points of service. Rates of healthcare utilization were highest for inpatient care and lowest for prescription costs. Emergency department and prescription costs were elevated among patients with insomnia relative to the control group. 25
Furthermore, a study of 1,459 community women found that healthcare costs increased in a graded manner across a sleep health score that included 5 dimensions: timing, latency, duration, satisfaction, and daytime sleepiness. 31 Also, Bin, Marshall, and Glazier (2012) reported a higher number of visits to general practitioners among respondents to the 2007 National Mental Health and Wellbeing Survey 41 (Australia). Sandlund, Westman, and Hetta (2016) investigated factors associated with the self-reported need for treatment of sleeping difficulties. Significantly more women than men reported such a need. 36 Older age (60-69 years), sick leave, retirement, and unemployment were associated with a self-reported need for treatment. Difficulty initiating sleep was most strongly associated with a self-reported need for treatment. Burton and colleagues (2017) surveyed employees of a multisite financial services corporation in the U.S. and reported that almost half (45.0%) of employees getting less than or equal to 5 hours of sleep reported feeling tired during waking hours and are unlikely to be productive. 42 Choi et al. (2017) also reported that sleep less than 6 hours was associated with greater odds of emergency department visits whereas sleep over 10 hours was associated with greater odds of an overnight hospital stay. 43 A meta-analysis of 74 studies representing over 3 million participants found a J-shaped relationship between sleep duration and mortality and cardiovascular disease 44 supporting findings of these studies that insomnia is associated with increased healthcare utilization.
Comorbidities Confound the Relationship
Studies that examined comorbidities reported higher healthcare costs among participants with medical and psychiatric comorbidities and those that controlled for clinical covariates found weaker associations between insomnia and healthcare utilization.31,33 In a population of young adults, Bramoweth and Taylor (2012) reported a significant difference in healthcare utilization when medical or mental health problems were present, but healthcare utilization did not differ significantly when comorbid disorders were not present. 26 Another study that explored the link between insomnia, future primary care, and psychological distress in self-reported insomnia observed that future healthcare use and the relationship was stronger in those participants scoring higher on the Hospital Anxiety and Depression Scale. 45 In a case control study that investigated the relationship between insomnia and use of health resources in people diagnosed with fibromyalgia, insomnia was associated with increased likelihood of use of antidepressants and opioids and a diagnosis of insomnia was associated with an increased frequency of visits to ambulatory care services for fibromyalgia and other conditions. 22 Kaufman and colleagues investigated a prospective association between insomnia and healthcare utilization in 14,355 adults over the age of 55 and found that participants reporting 2 or more insomnia symptoms had a greater odd of hospitalization, use of home care, and nursing home utilization. Findings suggest that preventing insomnia in this population could reduce health service use 6 to 14%. However, after controlling for clinical covariates, associations weakened and in some cases were no longer statistically significant. 33
A cohort study of 6700 community dwellers aged 65 years and over in Sweden found an association between geriatric syndromes, including insomnia, and healthcare utilization that remained significant after adjusting for multimorbidity. 35 Schousboe and colleagues (2020) also found that self-reported poor sleep and excessive daytime sleepiness were associated with higher subsequent healthcare costs even after full multivariable adjustment. 38
Other Outcomes Related to Insomnia
A finding of this scoping review is that insomnia affects work productivity and health related quality of life. Di Bonaventura and colleagues (2015) found that people with insomnia who did not receive treatment had worse health related quality of life, greater overall work impairment, more physician visits in the past 6 months. 19 Morin and colleagues (2016) reported that study participants with insomnia had a higher probability of being absent at work, reduced productivity, and non-motor-vehicle accidents when compared to participants who were not reporting insomnia. 46 Chen and colleagues (2018) examined employees based on changes in self-reported hours of sleep from 2012 to 2013. They observed that consistently poor sleepers and down graders had significantly more lost productivity compared to sleep improvers and consistently optimal sleepers. 30 Hui and colleagues (2015) found that participants in the Kansas State Wellness Program who had higher levels of sleep disturbance were more likely to be absent from work, have lower work performance ratings, and have higher healthcare costs. 32
Barriers to Identification and Evidence-based Treatment of insomnia
Although most of the studies focused on the characteristics of people who are in contact with healthcare services for insomnia, a few of the studies addressed people with sleeping difficulties who do not seek help and the barriers to identification and treatment of insomnia. The prevalence of self-rated sleeping difficulties varies according to population sub-group. Barros et al., (2019) observed the prevalence of poor self-rated sleep was 29.1% and significantly higher in women, individuals aged from 40 to 50 years, migrants, and in those who were without occupation, physically inactive in leisure context, with common mental disorder, with greater number of health problems, poor self-rated health, and/or life dissatisfaction. 49 Sandlund, Westman, and Hetta (2016) found that 30% of all participants who reported a need for treatment of sleeping difficulties had not sought treatment for their sleeping difficulties at some point. 36 In a cohort study using data from the Australian Longitudinal Study on Women’s health, Meredith (2018) found a substantial percentage of women aged 62 to 67 years who reported sleeping problems utilized herbal medicines to self-treat their insomnia. 34
Non-pharmacological and pharmacological treatments are employed to manage insomnia in clinical practice. Non-pharmacological therapies, such as multi-component cognitive behavior therapy for insomnia (CBT-I) are recommended as first-line treatments for insomnia especially in the context of significant comorbidities such as post-traumatic stress disorder, depression, sleep apnea, and chronic pain11. Sow and colleagues (2020) identified barriers to diagnosis and treatment which include perception of insomnia as mild, trivial, or a problem that one should be able to cope with alone, lack of awareness of treatment options and notion that the available treatment options as unsafe and unattractive. 47 Among Veterans, Bramoweth and colleagues (2012) identified barriers such as poor knowledge about treatment and lack of options that fit Veterans’ preference. 26 Ogeil and colleagues (2020) observed that Physicians’ knowledge, skills, available treatment options, and place of practice determine the kind of treatment that can be offered to patients. 48 Also, patients’ beliefs about insomnia, social influences, and severity of symptoms have been identified as barriers to treatment uptake.
Discussion
Most of the studies were cohort and case control studies relying on self-reports of sleep duration and quality although correlation with objective measures such as actigraphy is poor. Many mined established cohort studies that asked a question(s) regarding sleep. Most of the studies employed mailed or online surveys where representativeness is more difficult to obtain than with face-to-face interviews. Poor sleepers may be more inclined to reply thereby overestimating the prevalence of insomnia. Much of the research was conducted in the USA. To obtain more comprehensive results, future research is needed to explore factors influencing the relationship between insomnia and healthcare utilization in a variety of locations and with participants of diverse ethnic backgrounds. A limitation of the scoping review methodology is the lack of quality assessment of the included articles. While the authors attempted to include all relevant articles in the review, it is possible that some were missed due to databases used or search terms.
Conclusion
This scoping review was conducted to ascertain the association between insomnia and healthcare utilization. The association between insomnia and healthcare utilization was strong and positive with the rate highest for inpatient care and lowest for prescription refill. The healthcare utilization rate was also highest when compared with medical conditions such as chronic fatigue or pain. Important consideration is the cost of insomnia treatment which often entails consultation, inpatient care, nursing care, ambulance use, cognitive therapy procedure bill, emergency use, and cost of medications. Finding showed that the cost of healthcare utilization is an inhibiting and deterring factor among those with insomnia and this is even higher in those with co morbidities.
Valuable insights into barriers to the uptake of treatment were noted. Some patients decline treatment based on religious beliefs, perception that treatment is unsafe, lack of awareness of potential therapies and cost implications. The knowledge of the Physician on management and effective referral system can be a barrier if they are not up to date. Also, non-availability of prompt and effective service at the healthcare facility can discourage patients seeking treatments.
Recommendations
1) Health education and awareness program should be targeted at those who are at risk. 2) The cost of insomnia treatment, both pharmacologic and non-pharmacologic, should be made accessible and affordable. 3) There should be training and re training of healthcare professionals on current guidelines and management options. This may also entail encouraging healthcare workers and providing necessary incentives to sub specialize in sleep medicine. 4) It is important for employers to incorporate sleep improvement intervention as one of the essential lifestyles change interventions offered in employment work profile EWP to promote health and productivity. 5) Interventions improving sleep quality may enhance quality of life for older adults and reduce healthcare utilization and costs. 6) Studies of Medicare beneficiaries with insomnia indicate that rates of HCU were highest for inpatient care. Further analyses of insomnia and HCU are required to understand if insomnia results from or exacerbates comorbid medical conditions or accidents leading to hospital stay. 7) Within cohorts diagnosed with insomnia, there are differences in HCU and costs between treated and untreated. Future studies are needed to explain why some individuals diagnosed with insomnia receive treatment but others do not. 8) An increasing number of older adults remain in the workforce, and understanding the impact of insomnia on workplace productivity and/or early retirement is an important research priority
Implications of the findings for Education, Practice, and Future research
Education
Discussion on insomnia, diagnosis, and treatment must be regularly placed at the front burner of discourse. Physicians and all health workers must be trained and retrained on diagnostic criteria and treatment options that are available.
Practice
Clinicians should evaluate the (non)effectiveness of sleep medications, both prescription and over the counter, and adjust/remove them as required. Second, clinicians should evaluate those who sleep too little or too much for psychological distress and refer them to mental health treatment as required. Fourth, special attention should be paid to preventive care for short and long sleepers to reduce their need for healthcare use.
Future Research
First, previous studies of the association of sleep with healthcare costs have not focused on the older population, among whom sleep complaints are most common and healthcare costs high in most of these studies.
Second, more research is needed to assess the potential benefit of lifestyle modifications (dietary patterns, exercise, etc.) in the prevention and management of insomnia.
Further research is also needed to determine if the association is causal or attributable to confounding variables that also predict mortality.
Assessment of sleep health is not usually included in geriatric assessment or case management programs for older patients with multimorbidity.
Thus, future randomized trials may be warranted to determine whether sleep health assessment and incorporation of sleep interventions (e.g., cognitive behavioral therapy for insomnia symptoms) into chronic disease management programs in high risk older adults reduces subsequent healthcare utilization and costs
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Appendix
Summary of the Included Articles in the Review.
Author, year of publication, country
Aims
Population/sample size
Methodology
Measures
Key Outcomes
1. Anderson et al., 2014, USA
To compare healthcare costs and utilization of patients diagnosed with insomnia who received care in a managed care organization with a set of matched controls
7647 adults with an insomnia diagnosis with an equally sized matched cohort of health plan members without an insomnia diagnosis between 2003 and 2006.
Observational, retrospective cohort study
Diagnosis of insomnia
Healthcare utilization and costs from claims dataInsomnia diagnosis was associated with 26% higher costs in the baseline and 46% in the 12 months after diagnosis. When comorbidities were recognized, the insomnia cohort had 80% higher costs, on average, than the matched control cohort.
2. Bin, Marshall & Glozier, 2012, Australia
To determine the extent to which insomnia poses an independent burden on individual function and healthcare use
8,841 respondents, representative of the Australian population aged 16 to 85 in the 2007 National Mental Health and Wellbeing Survey
Cross sectional
Insomnia questions
Medications for mental health
General practice visits, hospital admission, use of complimentary alternative medicine (CAM)Controlling for a priori confounders, insomnia was associated with greater odds of disability days (1.62; 1.20-2.18), difficulties in daily activities (1.60; 1.10-2.31), life dissatisfaction (2.34; 1.11-4.93), use of sleep medication (1.78; 1.12-2.82) and a higher number of visits to general practitioners (1.57; 1.06-2.33). Insomnia not significantly associated with medications for mental health (1.17; 0.82-1.67), hospital admissions (1.31; 0.82-1.67), CAM (1.10; 0.73-1.67) or unmet need for healthcare (1.22; 0.84-1.77).
3. Bramoweth & Taylor, 2012, USA
To investigate the relationship between chronic insomnia and HCU in a population with fewer medical/mental health problems.
Young adults (18–35 years of age) from a large, public university. Of the total sample (N = 1,010), 72.0% were women, 24.5% were men, and 3.5% did not specify gender
M age 20Cross sectional
Insomnia Severity Index
weeklong sleep diary
Quick Inventory of Depressive Symptomatology
State-Trait Anxiety Inventory
Epsworth Sleepiness Scale
Multidimensional Fatigue InventoryWith no medical/mental health problem, no HCU differences occurred; a significant difference in HCU between groups when a medical/mental health problem was present. These results suggest that, although chronic insomnia may be related to increased distress and reduced quality of life, if no comorbid disorder is present, HCU does not differ in a young adult sample
4. DiBonaventura et al. 2015, USA & EU
(1) to compare health outcomes between those with insomnia and non-insomnia controls, (2) to compare health outcomes between those treated for insomnia and non-insomnia controls, and (3) to assess the prevalence of side effects of insomnia medications and their relationship with health outcomes.
2013 US (N = 75,000) and 5EU (N = 62,000)
Cross sectional study using data from National Health and Wellness Survey (NHWS)
health-related quality of life [HRQoL], productivity at work, and healthcare resource use visits
Patients with insomnia (n = 4147) and treated insomnia (n = 2860) in the 5EU reported significantly worse HRQoL than controls, greater overall work impairment, and more physician visits in the past 6 months
Similar findings were observed in the US. Among those treated
13.56% and 24.55% in the US and 5EU, respectively, were non-adherent due to side effects. In the US, non-adherence was associated with significantly worse HRQoL and greater overall work impairment. Relationship not significant in EU.
5. Dragioti, 2018, Sweden
To investigate the association of insomnia severity with general well-being, health-related quality of life and health care costs
10,000 randomly selected older adults (65 years and older) in south-eastern Sweden.
2790 valid responsesCross-sectional study is a part of a larger project that used data from a sampling frame based on the Swedish Total Population Register (TPR)
Insomnia severity index (ISI
Pain
BMI
Comorbidities
General Well Being Schedule
European QoL
Costs: outpatient care, inpatient care, pain drug costs, total drug costs and total health care costs.An association between severe insomnia, well-being, quality of life, outpatient care, total drugs costs and total health care costs remained after controlling for age, sex, pain intensity, frequency, body mass index and comorbidities using linear regression models
Persons who reported clinical insomnia were more likely to experience pain more frequently with higher pain intensity.
6. Fielding & Wong, 2012, Hong Kong
To: (1) determine the prevalence and severity of chronic pain, fatigue, and insomnia in the general adult population of Hong Kong; (2) identify associated factors; and (3) quantify the health care utilization associated with these conditions over the preceding 3 months
A random sample of 5001 Chinese adults aged ≥18 years was recruited to complete a structured telephone interview 2007-2008.
Cross-sectional observation
The Pittsburgh Sleep Quality Index
Chronic Pain Grade questionnaire
Chalder Fatigue Scale
Hospital Anxiety and Depression
Scale
QoL
HCUAfter controlling for gender, age, and chronic health problems, more severity in chronic pain, insomnia, and fatigue was associated with greater use of health care services
7. Ford, et al., 2014, USA
To examine recent national trends in outpatient visits for sleep related difficulties in the United States and prescriptions for sleep medications.
Sample sizes for adults aged 20 y or older ranged from 17,223 in 1999 to 26,647 in 2007. During the study period, mean age ranged from 53.2 y in 2000 to 55.4 y in 2009 (P linear trend < 0.001),
Trend analysis
Data from the National Ambulatory Medical Care Survey from 1999 to 2010.Office visits with diagnosis of insomnia
Office visits with Rx for sleep medicationsThe number of office visits with insomnia as the stated reason for visit increased from 4.9 million visits in 1999 to 5.5 million visits in 2010 (13% increase), whereas the number with any sleep disturbance ranged from 6,394,000 visits in 1999 to 8,237,000 visits in 2010 (29% increase). Striking increases in the number and percentage of office visits for sleep related problems and in the number and percentage of office visits accompanied by a prescription for a sleep medication occurred from 1999-2010.
8. Haaramo et al., 2014, Finland
To examine the associations of insomnia symptoms with subsequent psychotropic medication, reflecting mental health
40- to 60-year-old employees of the city of Helsinki, Finland, surveys collected in 2000–2002 (N= 6,227, response rate 67 %, 78 % women
Prospective cohort
Insomnia symptoms using the Jenkins Sleep Questionnaire
Purchase of psychotropic medications
Mental and physical strenuousness of work questions
Self-reported physician diagnosed mental disordersInsomnia symptoms were associated with higher frequency of subsequent psychotropic medication prescriptions. The associations were strongest for frequent insomnia symptoms (women OR 3.55, 95 % CI 2.64–4.77; men OR 4.64, 95 % CI 2.49–8.66, adjusted for age and prior medication)
9. Hayward, Jordan, & Croft, 2010, UK
To determine the association of insomnia with future primary care for sleep and mood problems, and explore the link with psychological distress
A total of 2662 (56%) responded and 2192 (82%) consented to record review
Mean age 51.3 yearsCohort study using mailed survey linked to health care records
Self-reported insomnia
Hospital Anxiety and Depression scale
Relevant healthcare use defined as a consultation or Rx for insomnia or mood problem in the 12 months following the baseline
surveySelf-reported insomnia was related to future relevant healthcare use (odds ratio = 1.77; 95% CI = 1.35 to 2.33). This relationship was stronger in those with psychological distress. 63% of those with baseline insomnia and psychological distress had no relevant healthcare use
10. Hayward, Jordan, & Croft, 2012, UK
To determine the association of persistence and remission of insomnia with primary health care using a longitudinal study
474 participants reporting insomnia symptoms at baseline were followed up at 12 months.
Prospective cohort study using postal survey of registered adult (over 18 years) populations of five UK general practices, repeated after 1 year, linked to primary care records.
4 questions related to insomnia
Medical records131(28%) consulted for mood problem(s) or received a relevant prescription. Of these 100 (76%) still had insomnia symptoms at one year, compared with 227 (66%) of those with no contact with primary care for this condition (OR 1.37; 95% CI 0.83, 2.27). Prescription of hypnotics showed some evidence of association with persistence of insomnia at follow-up (OR 3.18; 95% CI 0.93, 10.92)
Those with insomnia symptoms continue to have problems regardless of whether they receive primary care management or not. Hypnotic use appears to be related to persistence of insomnia. Further research is needed to determine the most effective methods of identifying and managing insomnia in primary care. There is also a large group of people with persistent insomnia who do not seek primary health care.
11. Huang et al., 2019, Taiwan
To determine whether comorbid insomnia is associated with increased use of fibromyalgia-related medications and health resources in fibromyalgia (FM) patients
17,920 patients with FM divided into 2 groups: with (n=5466) and without comorbid insomnia (n= 12,454).
Cohort data retrieved from the Longitudinal Health Insurance Database 2010 (LHID2010) released by Taiwan’s National Health Research Institutes
Fibromyalgia and insomnia ICD9 codes
Insomnia associated with increased likelihood of future use of antidepressants OR=3.84, P < 0.001, gabapentin OR=1.67, P < 0.001), pregabalin OR=1.79, P = 0.046), muscle relaxants OR=3.05, P < 0.001), and opioids and tramadol OR=1.59, P < 0.001) a diagnosis of insomnia was associated with an increased frequency of visits to ambulatory care services for both FM (β=1.79; 95% CI, 1.57-2.02; P < 0.001) and other conditions (β=108.51; 95% CI 103.14-113.89; P < 0.001).
12. Kaufman et al. 2013, USA
To investigate the prospective association between insomnia symptoms in 2006 and healthcare utilization in 2008
14,355 adults aged 55 and older
Prospective Cohort enrolled in the 2006 and 2008 waves of the health and Retirement Study
Respondents were asked questions about their use of health services, including hospital, home health care, or nursing home within the prior 2 years; insomnia symptoms; health conditions
those reporting one symptom had a greater odds of hospitalization (AOR= 1.28, 95% [CI] = 1.15–1.43, P < .001), use of home health care services (AOR = 1.29, 95% CI = 1.09–1.52, P = .004), and any health service use (AOR = 1.28, 95% CI = 1.15–1.41, P < .001). Those reporting greater than or equal to two insomnia symptoms had a greater odds of hospitalization (AOR = 1.71, 95% CI = 1.50–1.96, P < .001), use of home health care services (AOR = 1.64, 95% CI = 1.32–2.04, p < .001), nursing home use (AOR = 1.45, 95% CI = 1.10–1.90, p = .009), and any health service use (AOR = 1.72, 95% CI = 1.51–1.95, P < .001) after controlling for demographics. These associations weakened, and in some cases were no longer statistically significant, after adjustment for clinical covariates.
Findings suggest that by preventing insomnia in this population could result in a 6%–14% decrease in health service use.
13. Leggett et al., 2016, USA
To examine rates and predictors of new prescription sleep medications and sleep treatments, and sleep treatments without a doctor’s recommendation
8,417 adults aged 50 and older
Cohort from two waves of the nationally representative Health and Retirement Study (HRS) not using a sleep medication or treatment at baseline (2006).
Insomnia symptoms, prescription med use (“Do you regularly take prescription medications to help you sleep?”), current sleep treatment use (“In the past two weeks, have you taken any medications or used other treatment to help you sleep?”), and for those who responded yes to the latter question, a follow-up question asked “Were these medications or other treatments recommended to you by a doctor?”
New sleep prescriptions started by 7.68%, 12.62% started using a new sleep treatment, and 31.93% were using the treatment outside of doctor’s recommendation. Common predictors included greater severity of insomnia, worsening insomnia, older age, and use of psychiatric medications. New prescription medication use was also associated with poorer mental and physical health, whereas new sleep treatment was associated with being white, higher educated, and drinking less alcohol
14. Meredith, 2018, Australia
To investigate the health service use—including complementary and alternative medicine (CAM)—and self-care by women aged 62 to 67 with sleeping problems.
9,110 participants (99.6%) responded to questions about sleeping problems, health service utilization and self-care
Part of the Australian Longitudinal Study on Women’s Health (ALSWH): a prospective, population-based survey
Asked: lying awake for most of the night, taking a long time to get to sleep, or sleeping badly at night. If they indicated that they had one or more of these problems, they were classified as having a sleeping problem
Asked about health service useWomen with sleeping problems consulted a general practitioner (GP) more frequently (odds ratio [OR] = 1.72; 95% confidence interval [CI] = [1.36, 2.17]; P < .005) and were more likely to be using herbal medicines (OR = 1.24; 95% CI = [1.13, 1.36]; p < .005) than women without sleeping problems
A substantial percentage of women aged 62 to 67 with sleeping problems utilize herbal medicines and it is important for all health professionals to actively inquire with patients about such use to ensure safe patient outcomes and avoid potentially dangerous drug–herb interactions.
15. Möller et al., 2021, Sweden
To determine the association between geriatric syndromes, including insomnia, and health-care utilization
Based on the Stockholm Public Health Cohort study, a total number of 6700 community dwellers aged ≥65 years were included
Sub-Cohort post-based questionnaires linked to information from Swedish health registers,
Insomnia was defined as having light to heavy sleeping problems.
Health-care utilization was assessed according to number of hospital visits, hospitalized days, outpatient visits and medications annually during follow-upThe prevalence of specific geriatric syndrome items was 59.9% for insomnia, 37.2% for functional dependence, 28.1% for urinary incontinence, 11.1% for depressive symptom and 4.7% for vision impairment. The association between geriatric syndromes and health-care utilization was still significant after adjusting for multimorbidity
16. Rissling et al., 2016, USA
To compare the prevalence and cardiometabolic health impact of sleep disturbance among postmenopausal Veteran and non-Veteran participants in the Women’s Health Initiative (WHI).
3,707 postmenopausal women Veteran and 141,354 non-Veteran participants from the WHI
Case-control using a subset of the 161,808 Veteran and non-Veteran participants from the Clinical Trial (CT) and Observational Study of the WHI, a longitudinal study of postmenopausal health and mortality risks in women aged 50–79 years at enrollment
five categories of sleep disturbance—medication/alcohol use for sleep; risk for insomnia; risk for sleep disordered breathing [SDB]; risk for comorbid insomnia and SDB (insomnia + SDB); and aberrant sleep duration [SLD]
CVD
Type II diabetesWomen Veterans were more likely to have high risk for insomnia + SDB relative to non-Veteran participants.
Risks for SDB and insomnia + SDB were both linked to heightened risk of CVD and diabetes; SLD was consistently linked with greater risk of CVD and diabetes in non-Veterans but less strongly and consistently in Veterans. there were no differences between the 3,462 (24.6%) WVs and 132,812 (24.7%) non-Veterans in baseline use of medication or alcohol for sleep
17. Sandlund, Westman, & Hetta, 2016, Sweden
To investigate factors associated with the self-reported need for treatment of sleeping difficulties in the general population
A telephone survey of 1550 people randomly selected from the total population of Sweden was completed by 1115 people aged 18–85 years.
Cross sectional
Outcome question: “Do you think you need treatment of some kind for sleeping difficulties? insomnia disorder was defined as having major difficulty initiating sleep during the past month and/or maintaining sleep (score between four and five) and having moderate to severe sleeping difficulties that interfered with daily life (score 2–4) during the past month. This variable was dichotomized into no insomnia and insomnia
12.5% reported a need for treatment because of sleeping difficulties. Significantly more women than men reported such a need (OR 1.46, 95% CI 1.02–2.10). Older age (age 60–69), sick leave, retirement, and unemployment were associated with a self-reported need for treatment. A logistic regression model showed that difficulty initiating sleep (OR 6.29, 95% CI 3.67–10.78) was most strongly associated with a self-reported need for treatment for sleeping difficulties. Other important factors were nonrestorative sleep (OR 3.70, 95% CI 2.05–6.69), mental health disorders (OR 3.01, 95% CI 1.59–5.67), and fatigue (OR 2.95, 95% CI 1.53–5.68).
70% of all participants who reported a need for treatment of sleeping difficulties had consulted a physician for their sleeping difficulties at some point.
Previous studies have focused on the characteristics of people with sleeping difficulties who are in contact with healthcare services, but many people with sleeping difficulties never seek help
18. Sands-Lincoln et al., 2013, USA
To identify whether self-reported sleep duration and insomnia, based on a validated questionnaire, are associated with increased incident CHD and CVD among postmenopausal women
Women's Health Initiative Observational Study Participants (N=86,329; 50–79 years) who reported on sleep at baseline
Cohort followed prospectively for incident CVD events for 10.3 years
Sleep duration
WHI Insomnia Rating Scale
Incident CVD or ischemic stroke
Incident CHD, MI, death, hospitalized angina, coronary revascularizationWomen with high insomnia scores had elevated risk of CHD (38%) and CVD (27%) after adjustment for age and race, and in fully adjusted models (hazard ratio [HR]=1.19, 95% CI] 1.09–1.30; 1.11 95% CI 1.03–2.00). Women with high insomnia scores and long sleep demonstrated the greatest risk of incident CHD compared to midrange sleep duration (HR=1.93, 95% CI 1.06—3.51) in fully adjusted models.
19. Sarsour et al., 2011, USA
To examine the association between insomnia severity and productivity, healthcare utilization and costs.
2086 health plan members
Cohort design linking claims data with telephone survey
Insomnia severity and comorbidities
Health care costs
ProductivityCompared with the no insomnia group, healthcare costs were 75% larger in the group with moderate and severe insomnia [$1323 vs. $757, P < 0.05], mean lost productivity costs were 72% larger in the moderate and severe insomnia group [$1739 vs. $1013, P < 0.001]. Chronic medical co morbidities and psychiatric co morbidities were positively associated with health care cost. Psychiatric co morbidities were associated with lost productivity while medical co morbidities were not
20. Schousboe, et al., 2020, USA
To estimate the association of self-reported poor sleep-in multiple dimensions with health care costs in older men.
1,413 men (mean [SD] age 76.5 [5.7] years) enrolled in both the Outcomes of Sleep Disorders in Older Men (MrOS Sleep) study and Medicare Fee-for-Service
Longitudinal cohort
Poor sleep was characterized at the baseline MrOS Sleep visit on five dimensions (satisfaction, daytime sleepiness, timing, latency, and duration). Health care costs and utilization were ascertained over 3 years of follow-up using Medicare Claims.
All sleep health dimensions except for poor sleep timing were associated with higher subsequent health care costs even after full multivariable adjustment. Self-reported poor sleep satisfaction (CR 1.38, 95% CI 1.16 to 1.63) and excessive daytime sleepiness (CR 1.38, 95% CI 1.13 to 1.67) had the strongest associations, followed by short or long sleep duration (CR 1.19, 95% CI 1.04 to 1.37), and longer sleep latency (CR 1.19, 95% CI 1.02 to 1.3
21. Tzuang, 2021, USA
To determine the association of insomnia symptoms with subsequent health services use,
4,289 community-dwelling Medicare beneficiaries who had continuous fee-for-service Medicare coverage 30 days before, and 1 year after the National Health and Aging Trends Study (NHATS) Round 1 interview
Prospective cohort study
health services use within 1 year of interviews from linked Medicare claims: emergency department (ED) visits, hospitalizations, 30-day readmissions, home health care (all measured as yes/no), and number of hospitalizations and ED visits
Compared to participants with no insomnia symptoms, those with two insomnia symptoms had a higher odds of ED visits (odds ratio [OR) = 1.60, 95% confidence interval [CI] = 1.24-2.07, P < 0.001), hospitalizations (OR = 1.29, 95% CI = 1.01-1.65, P < 0.05), and 30-day readmissions (OR = 1.88, 95% CI = 1.88-3.29, P < 0.05). Reporting 2 insomnia symptoms, versus no insomnia symptoms, was associated with a greater number of ED visits and hospitalizations (incidence rate ratio (IRR) = 1.52, 95% CI = 1.23-1.87, P < 0.001; IRR = 1.21, 95% CI = 1.02-1.44, P < 0.05, respectively) after adjusting for demographic and health characteristics
22. Wickmire et al., 2019, USA
To examine the impact of untreated insomnia on health care utilization (HCU
total sample size of 484 707
151,668 beneficiaries were found to have insomnia. Compared to controls (n = 333 038)cohort design
Random 5% sample of Medicare administrative data 2006-2013International Classification of Disease, Version 9, Clinical Modification (ICD-9-CM)
Insomnia related medications
HC claims 1 year prior to month of index dateHCU highest for inpatient care (rate ratio [RR] 1.61; 95% [CI] 1.59, 1.64) and lowest for prescription fills (RR 1.17; 95% CI 1.16, 1.17). Those with insomnia demonstrated $63,607 (95% CI $60,532, $66,685) higher all-cause costs, driven primarily by inpatient care ($60,900; 95% CI $56,609, $65,191). Emergency department ($1,492; 95% CI $1,387, $1,596) and prescription costs ($486; 95% CI $454, $518) were also elevated
23. Wickmire et al., 2020, USA
To evaluate the impact of insomnia treatment on HCU and costs among patients diagnosed with insomnia
23,079 beneficiaries with insomnia
M age 71.7
22% received one or more insomnia medicationsNested cohort design
Random 5% sample of Medicare administrative data 2006-2013Insomnia ICD9 codes
Treatment operationalized as
HCUFor treated and untreated individuals, HCU and costs increased in 12 months prior to diagnosis. Insomnia treatment was associated with significantly increased ED visits and Rx fills in the year following insomnia diagnosis. After accounting for pre-diagnosis differences between groups, no significant differences in pre- to post-diagnosis costs were observed between treated and untreated individuals. Higher costs were driven by inpatient care, ED, and prescription costs.