
Abstract
Introduction:
Clinical pathways (CPWs) are evidence-based, standardised, clinical management plans that are designed to deliver a sequence of clinical interventions to improve the efficiency and effectiveness of healthcare. The aim of this study was to identify and summarise the current available evidence on the use of CPWs in emergency departments (EDs).
Study design:
A literature search was conducted in Scopus, Embase, Emcare, and PubMed academic databases. The search strategy was guided by Arksey and O’Malley’s framework and results reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis Extension for Scoping Reviews Checklist. Studies were included if they reported empirical data either qualitatively or quantitatively, studied the use of CPW practices, and reported on the use of at least one CPW activity.
Results:
Sixty-four articles were eligible for the scoping review. Variation and quality of treatment, resource utilisation and time to treatment were identified as the three main patient and organisational outcomes from the use of CPWs. Three main categories of barriers to use were identified: Organisational environment factors, Healthcare professional-related factors, and CPW operational issues.
Conclusions:
CPW implementation has wide positive patient and organisational outcomes in the ED. Whilst no single strategy would result in implementing CPWs in the ED settings successfully, broad engagement with clinicians of all disciplines who use the pathways and involvement of multidisciplinary teams in implementation is vital to increase visibility of the CPW.
Keywords
CPWs are increasingly being utilised in the healthcare sector to align practice with evidence-based guidelines. Although the use of CPWs has increased, their use in complex settings like the ED is poorly understood.
This review reported on a range of CPW clinical conditions, their use and impact on patient and organisational outcomes. A range of factors influencing the successful implementation of CPWs in the ED setting are discussed and contribute to future CPW implementation and research efforts.
Our review informs current and future research efforts on the implementation and evaluation of CPW use in the ED. Outcomes for future research studies on the impact of CPWs should be more patient-focused and include treatment quality satisfaction from the patient’s perspective. Future research should explore collaboration between researchers and clinicians to enhance the use of CPW.
Introduction
Clinical Pathways (CPWs) are increasingly being utilised in the healthcare sector to align practice with evidence-based guidelines. 1 They aim to identify an appropriate sequence of clinical interventions, timeframes, milestones, and decision points for specific patient cohorts making them useful for quality assurance and process improvement. 2 The operational definition of CPWs includes structured multidisciplinary plans of care, guidelines or evidence translated into specific steps within the pathway along with a timeframe in a course of treatment, and standardised care for a specific patient cohort. 3 Therefore, CPWs are designed to enhance clinical processes by lowering risk, eliminating duplication, and reducing variation in the provision of healthcare. 2 They differ from general treatment guidelines which offer a range of reasonable treatment options without a specific sequence of steps. 3
Hospital systems are complex and evolving. Research suggests that 60% of current care is evidence-based, 30% contributes to waste or low-value care, and 10% is harmful. 4 Consequently, it is fundamental to ensure that quality and standardisation of care delivery is maintained. 5 Literature identifying best practices for addressing Emergency Department (ED) service delivery and quality issues, to promote safety, and positive patient experiences is rapidly evolving . Increasing coordinated, evidence-based patient care and efficiency is vital in complex systems, such as the ED, which are made up of numerous interdependent, fragmented components that produce varying levels of quality and safety. 6 ED presentations are increasing globally, creating challenges for quality, safety, and timeliness of care.7,8 Patients are having to wait longer to be seen impacting on service delivery outcomes. 9 Delays in the assessment, diagnosis, and treatment of time-sensitive diseases as well as in the delivery of necessary medications like antibiotics and analgesics are among the adverse effects of increased ED presentations and resultant overcrowding. 10 The increased interest in addressing these issues is evidenced by the growing body of work focusing on improving patient outcomes. 11 This includes the use of CPWs to address known ED challenges like reducing length of stay (LOS) and improving patient quality of care. 12
There is extensive literature demonstrating the value of CPWs. Beginning in the UK in the 1990s, the use of CPWs has been growing throughout Europe, and there is increased focus on the further development and implementation of CPWs globally. 13 Although the use of CPWs in the health sector has increased, their use in complex settings like the ED is generally poor and the reasons for this are not well understood. 14 Evidence for effective implementation strategies of CPWs in ED remains variable. 15 Therefore, it is critical to get a thorough understanding of the available evidence on the use of CPWs in the ED context. The objective of this review was to identify and summarise the current available evidence on how CPWs are implemented and used in the ED. This includes reported barriers and enablers for CPW implementation and outcomes reported with the use of CPWs in the ED setting.
Methods
Study Design
This scoping review followed the methodological recommendations described in Arksey and O’Malley’s 16 framework. This methodological approach was deemed appropriate to map important concepts, and communicate the scope and depth of research about the use of CPWs in the ED setting.17-19 The framework steps provided guidance for identifying the research question, identifying relevant studies, study selection, charting and collating the data, summarising, and reporting the results. Findings of the review were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension protocol for scoping reviews (Supplementary file 1 PRISMA – ScR). 20 A protocol for this study was registered prospectively with Open Science Framework. 21
Search Strategy
Stage One: Identifying the Research Question
The objective of this review was to identify and summarise the current available evidence on the implementation and use of CPWs in the ED. The research questions were left broad to allow rigorous searches for all sources of evidence simultaneously with one search strategy and to provide a greater sensitivity in the search. 22 The CPW needed to meet the construct requirements of a CPW definition of either structured multidisciplinary plan of care, guidelines or evidence translated into specific steps within the pathway along with a timeframe in a course of treatment, or standardised care for a specific patient cohort. 3 Our review sought to answer three research questions:
Research Question 1 (RQ1): What original research evidence is available on the use of CPWs in the ED setting?
Research Question 2 (RQ2): What are the reported outcomes with the use of CPWs in the ED setting?
Research Question 3 (RQ3): What are the reported barriers and enablers for CPW implementation in the ED setting?
Stage Two: Identifying Relevant Articles
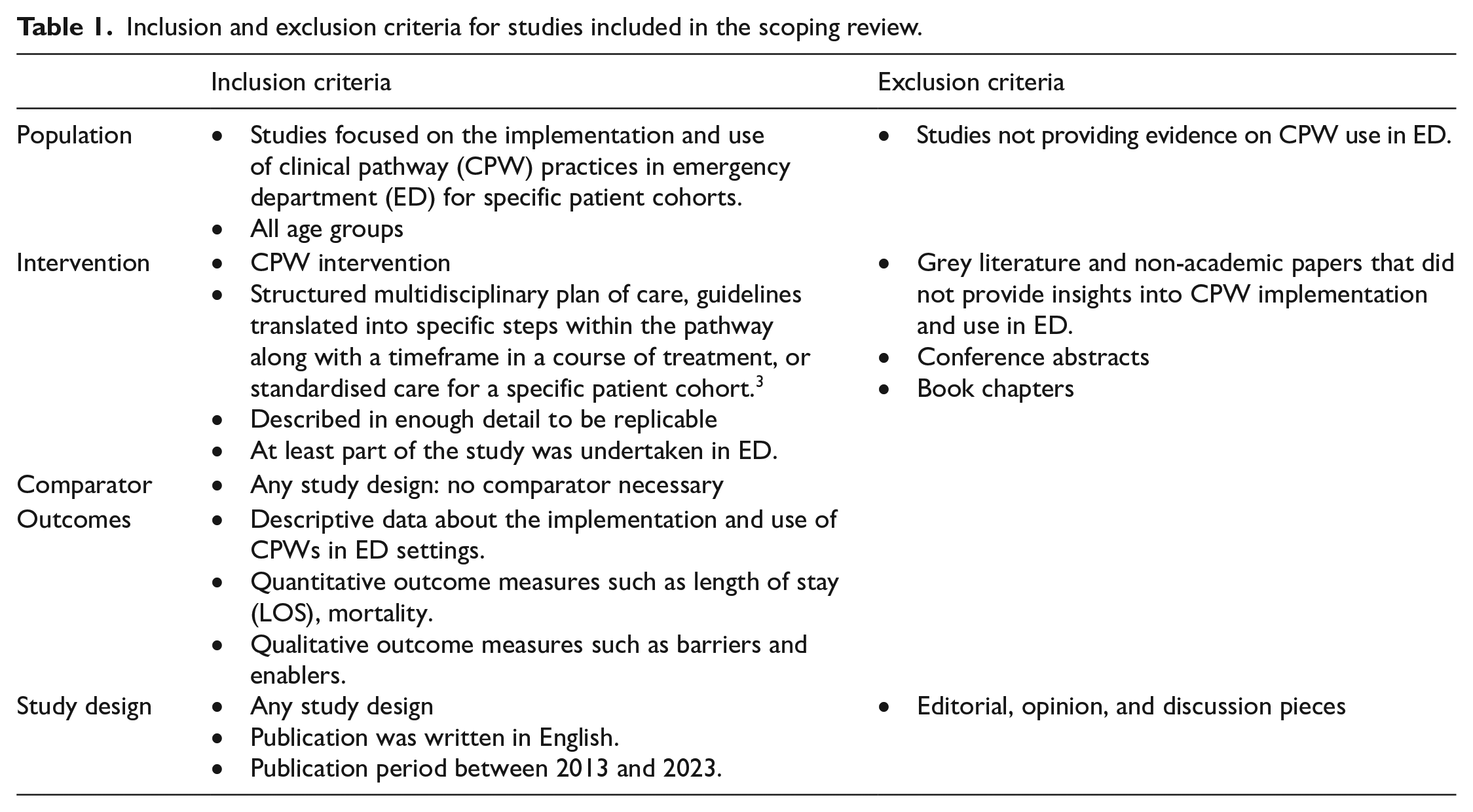
Inclusion and exclusion criteria: The authors (ITM, SJP, PG, and ET) included studies focused on the implementation and use of CPW in the ED setting for all age groups. Studies were included if they reported descriptive data about the implementation and use of CPWs in ED settings including empirical data either qualitatively or quantitatively, or if they were systematic literature reviews. The authors excluded studies that were conference abstracts, grey literature or did not provide insights into how CPWs were implemented or used in the ED setting. The authors also excluded editorials and discussion papers, and research protocols. The full inclusion and exclusion criteria are shown in Table 1.
Inclusion and exclusion criteria for studies included in the scoping review.
To ensure the identification of relevant studies, the authors critically reviewed the search strategies, search terms, inclusion and exclusion criteria. A preliminary search was developed by identifying and then searching one database relevant to the topic. The purpose of the preliminary search was to assist in refining search terms. A preliminary search from Scopus database was completed on the 6th of December 2023 (Supplementary file 1_preliminary search). This search was followed by analysis of the text words in the abstracts, titles, and MeSH terms of retrieved papers to inform terms for CPW use. The search terms and combinations related to CPWs was built on Boolean operators “AND” “OR” and “NOT” to facilitate custom combinations of search terms.
Table 2 summarises the final search terms used for the scoping review. The following databases were searched in December 2023: Scopus, Embase, Emcare, and PubMed academic databases. The authors reviewed the reference lists of studies identified and included relevant studies in the scoping exercise. A review strategy was developed and approved by the first four review authors prior to searching the database.
Database search terms.

Stage Three: Selecting the Articles for Full Text Review
The study selection process is illustrated in the PRISMA flow diagram (Figure 1). Search results from each of the databases was aggregated and imported into an Endnote library and duplicate entries were removed. The authors met regularly to discuss their assessments of the abstracts and full-text articles and the inclusion and exclusion criteria to reach agreement on the studies to be included. Two authors undertook a two-stage screening process against inclusion criteria for selection of studies using Covidence systematic review software. Reasons for exclusion of sources of evidence included screening by title and abstract to identify potentially eligible studies. Reasons for exclusion of sources of evidence at the full text that did not meet the inclusion criteria were recorded and reported (see Figure 1 – studies excluded n = 294). Any disagreements that arose between the authors was resolved through discussion (see Supplementary form 3_example of conflict resolution discussion).
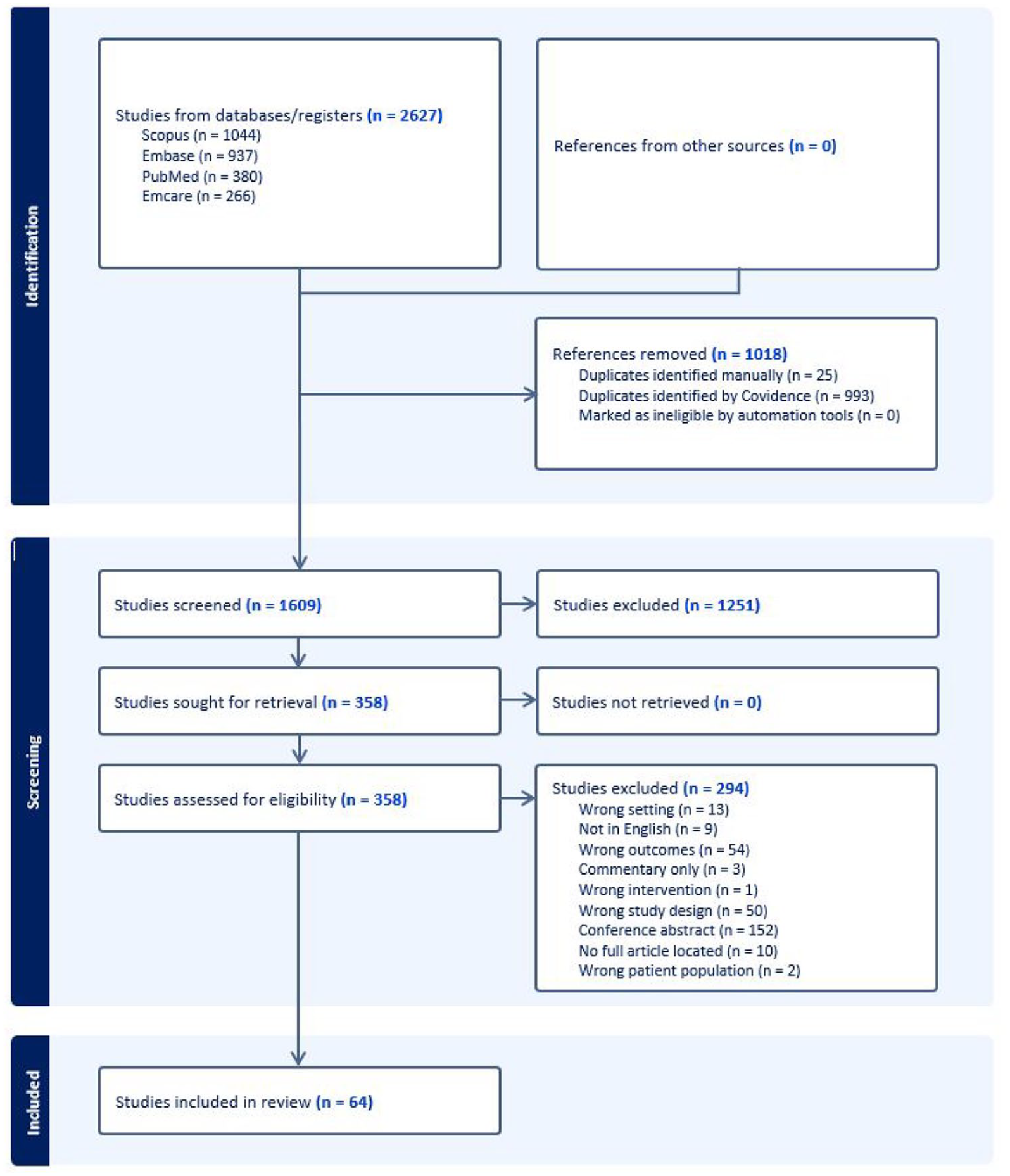
Identification and selection of studies for inclusion in our review (PRISMA flowchart).
Stage Four: Charting the Data
Data were extracted from each included article according to a data extraction template which was developed and agreed by the authors. The template was piloted by the authors using a random selection of ten eligible articles. Authors clarified ambiguous items through discussion, and this process was repeated several times to improve agreement before the template was finalised (Supplementary file 2 – Data extraction form). For each article, two authors independently extracted the required information. Additional authors provided consensus. The extracted key data items were organised in Covidence using checkboxes or free text boxes. These identified study details (author(s), location, study sample, setting), the CPW intervention/characteristic details (format, content, implementation, and evaluation), and reported outcomes (positive, negative or no change; Tables 3-5). The free text boxes captured the study reference, title, year of publication, aim of study, and the number of participants. The checkboxes included the rest of the information (see Supplementary file 2).
Stage 5: Collating, Summarising, Reporting Results
The data were analysed and summarised according to categories consistent with the research questions. Using a flow chart, table, and narrative summaries to track significant elements of information, we presented results in accordance with PRISMA guidelines. The authors did not evaluate the quality of evidence presented in the included studies as it was not a part of the scoping review methodical recommendation. 16 Reported outcomes were described and included reporting on variation, resource utilisation, time to treatment and length of stay. Barriers and enablers were categorised according to organisational environment factors, healthcare professional-related factors, and CPW operational issues. 37
Results
Covidence systematic review software was utilised to itemise stages of data analysis. Records for 2627 publications were initially identified through database searches. After duplicates were removed, 1609 studies were identified for title and abstract review. Of these, 1251 were excluded based on eligibility criteria and marked as ineligible by covidence software at this abstract and title screening stage. 358 articles were retrieved for full text review, of which 292 were excluded for not meeting the eligibility criteria. Full list of reasons is highlighted in Figure 1. Sixty-four (N = 64) publications were deemed eligible for inclusion in our review (Figure 1). Tables 3 and 4 describe the characteristics of included articles and summary of the peer reviewed publications.
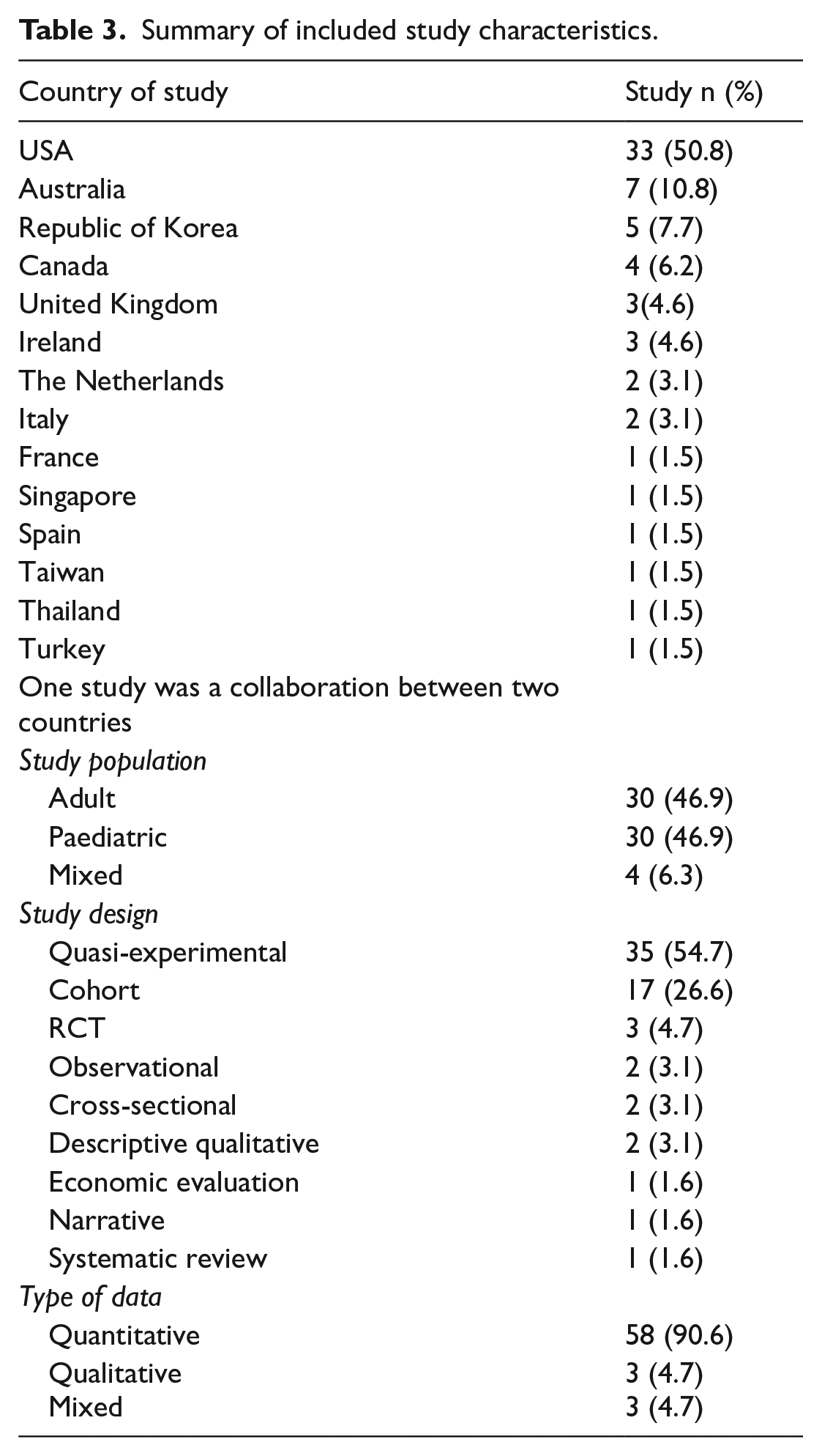
Summary of included study characteristics.
Summary of peer reviewed included publications.

Characteristics of Included Studies
Most included studies were conducted in the United States of America (USA; n = 33), Australia (n = 7) and the Republic of Korea (n = 5). Studies from eleven other countries were included with between one to four studies from each. Thirty-four studies were published within the last 5 years. Fifty-eight studies utilised quantitative methods whilst three studies each focused on qualitative and mixed data collection methods. An equal number of studies reported on the adult and paediatric population (n = 30), with four (n = 4) studies accounting for mixed populations. Quasi-experimental design was the most utilised study design (n = 35), followed by cohort design (n = 17), and randomised controlled trials (RCT; n = 3). Observational, cross-sectional and descriptive qualitative designs reported two studies each whilst economic evaluation, systematic review and narrative design, reported one study each.
RQ1. What Original Research Evidence Is Available on the Use of CPWs in the ED Setting?
Thirty-five different CPW conditions were identified from the included studies (Table 4). Seven studies focused on asthma.25,29,36,37,39,41,52 Of these, six focused on the paediatric population and one focused on mixed adult and paediatric populations. 37 Chest pain accounted for five adult population studies12,31,48,59,65 and one paediatric population study. 53 Sepsis accounted for two adult population studies62,77 and three paediatric population studies.67,76,81 Atrial fibrillation (AF),51,60,71 acute appendicitis,34,64,68 and concussion23,42,84 were the focus in three studies each. Other notable CPW conditions, fractured neck of femur (#NOF) and stroke, had two35,55 and one studies respectively. 82
RQ2. What Are the Reported Outcomes with the Use of CPWs in the ED Setting?
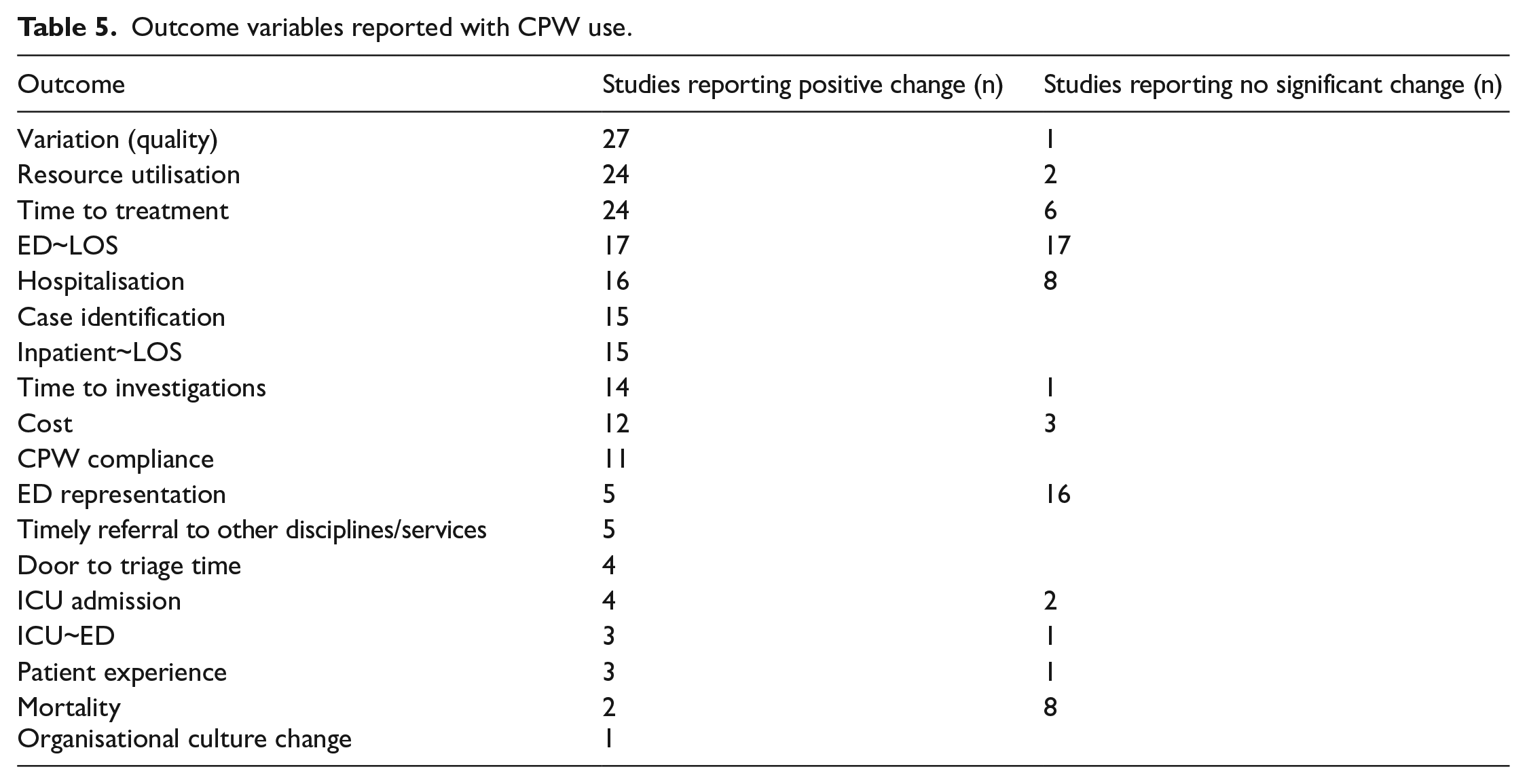
Fifty-nine studies reported on patient and organisational outcomes of CPW use in the ED. Eighteen variables were identified (Table 5).
Outcome variables reported with CPW use.
Variation and Quality of Treatment
Twenty-eight studies reported on variation and quality of treatment. Of these, 27 reported improved quality and reduced variation of treatment with implementation of CPWs. Asthma CPW implementation was associated with improved adherence to National Institute of Health (NIH) Guidelines, fewer hospital admissions, and reduced length of hospital stay.25,29,36 CPW allowed clinical diagnostic clearance of more cervical spine patients without compromising patient care. 45 Implementation of a seizure CPW led to more neurological examination and improved documentation around driving safety and legal guidelines. 80 Introduction of vestibular physiotherapy for vertigo/dizziness CPW in ED was associated with greater diagnostic specificity and efficiency of care. 72 Following the implementation of an ED skin and soft tissue infections (SSTI) CPW, hospitalisation rates dropped considerably. 73 Implementing CPWs was associated with improved outpatient follow-up. 84 The adoption and increased awareness of sepsis CPW was linked to an immediate rise in the rate of lactate testing. 62 Disparities in door to balloon times decreased, independent of arrival times with the adoption of chest pain CPW. 65 The door to balloon time is recommended to be less than 90 minutes and is at EDs with percutaneous coronary intervention (PCI) facility. 65
Resource Utilisation
Twenty-four studies reported on resource utilisation with CPW implementation in ED. Chest pain CPW implementation resulted in an increase in the administration of recommended medications and reduction of stress testing. 31 Utilisation of imaging and associated costs of care decreased with adoption of CPW.23,30,43 Antibiotic prescription changed with introduction of CPW with reduction in inappropriate antibiotic use and broad-spectrum antibiotic prescriptions.32,47
Time to Treatment
Of the 30 studies that reported on waiting time to treatment, 24 studies reported improvement with the use of CPWs. The improved waiting time to treatment ranged from time to administration of pain control medications,28,33,58 antibiotics,49,56 corticosteroids,36,76 and early access to operation room.55,85 Median door-to-balloon time improved with chest pain CPW use. 65
Other Variables
Seventeen studies reported reduced ED LOS, although an equal number of studies also reported no change in ED LOS after CPW implementation. The heart pathway study demonstrated an increase in early discharge rate which was defined as the proportion of patients discharged directly from the ED, a decrease in hospitalisation rate at 30 days which included inpatient admission, transfer, or observation. 48 Out of twenty-one studies reporting on ED representations, only five reported reductions with CPW use. Six studies reported on mortality with five reporting no improvement in mortality rate with CPW use.
RQ3. What Are the Reported Barriers and Enablers for CPW Implementation in the ED Setting?
Twenty-six (n = 26) studies reported on these enablers and barriers.23 -26,31,35-37,39-41,45-47,51,52,54-56,69,72,76,79-81,85 A range of specific enablers and barriers for the successful implementation and use of CPW in the ED setting were described. Three main categories of barriers emerged in our review namely: (i) Organisational environment factors, (ii) healthcare professional-related factors, and (iii) CPW operational issues.
Organisational Environment Factors
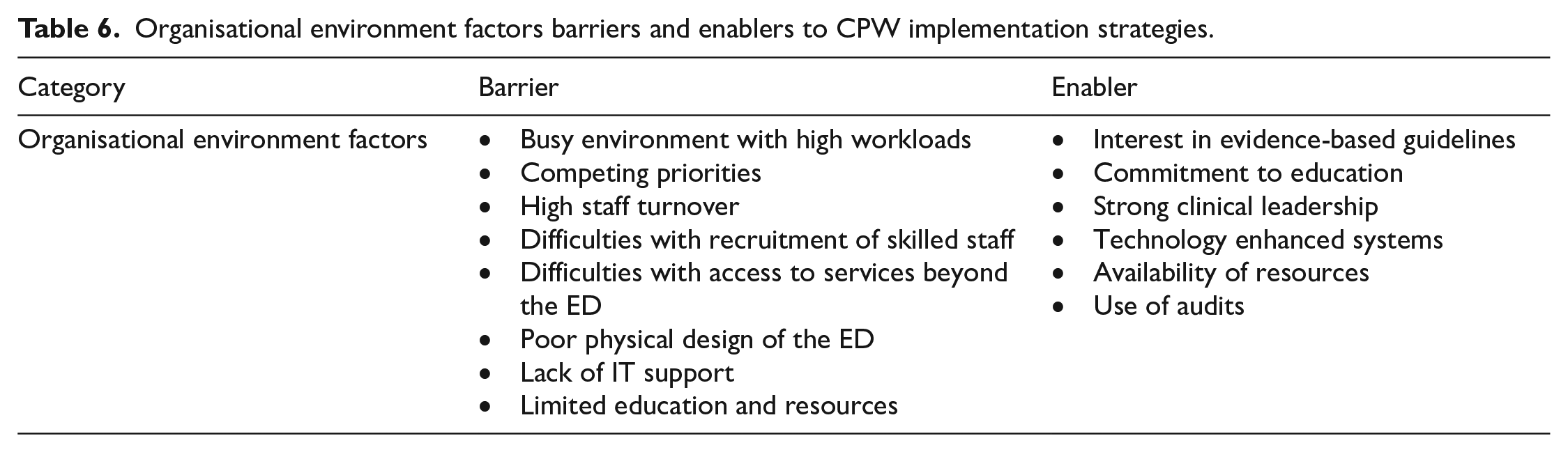
The overarching organisational environment includes external and internal factors (summarised in Table 6). External factors are those that the organisation cannot control, such as economic issues, societal trends, availability of skilled professionals and services available outside the individual organisation. 86 The infrastructure, characteristics of the healthcare delivery system and management and organisational culture are categories of internal factors.
Organisational environment factors barriers and enablers to CPW implementation strategies.
Barriers
The ED was reported to be a busy environment with high workloads where staff were constantly under work pressure and had limited time for new initiatives like CPWs. 35 Many existing organisational initiatives were reported to create competing priorities with CPW implementation.35,40,52,56,72,80,81 Recruitment difficulties and high staff turnover associated with ED departments were reported as barriers to the use of CPWs and inexperienced staff, part time staff, and/or locum/agency staff who may not be familiar with the CPW processes were also reported as contributing to poor uptake of CPWs.37,40,72 Furthermore, varying levels of staff clinical skill set were shown to affect readiness to care for critically ill patients including the implementation of CPWs. 81 When CPWs were used, access to services beyond the ED, including downstream obstructions to discharge and availability of rehabilitation beds was reported as a barrier to continued and consistent CPW use.35,36,46,51,72 Limitations around access to services beyond the ED also included waiting for other departments like Pharmacy, limited availability of inpatient beds, and unavailability of community-based services. 36 The physical design and space within the ED were reported as barriers for successful implementation of CPWs. 37 Non-optimised computer decision support and an incompatible electronic record system to support the CPW was reported by one study as impacting significantly on implementation. 41 Limited education and resources on CPWs and processes were also viewed as barriers in two studies.46,85
Enablers
Organisational interest in evidence-based guidelines and commitment to staff education were viewed as major facilitators for successful CPW implementation. This included development and testing of guidelines, performance feedback, and audits.23,25,27,32,35,37,40,41,45,49,51,52,54 -57,59,68,72,79,81,83,85 Strong clinical leadership was viewed positively as it allowed accountability, sense of responsibility, and flexibility when faced with work pressures.40,81 Access and availability of resources was also reported as contributing to CPW uptake success.35,51,71,72 Technology enhanced systems like electronically enhanced CPW use, SMS alert system, and QR code scanning were reported to contribute to the successful implementation and use of CPWs.26,45,49,52,57 Clinical decision tools like prompts were also reported enablers to promote use and uptake of CPWs.42,72 The use of periodic, retrospective or prospective audits was reported as a justification for the successful introduction and implementation of CPWs.24 -26.49 Incremental dissemination of CPW information and integration with existing systems was reported as an enabling strategy.23,24 Extensive broad marketing prior to implementation of CPWs was reported in one study as being an enabler for successful implementation.24 -27,49 This broad marketing approach ranged from utilisation of print material, notice boards, educational campaigns, case study presentations, email feedback, information on both internal and external facing organisational websites, and electronic newsletters.24 -27,49 To enhance sustainability and long-lasting improvements, several strategies were highlighted by some studies. One study incorporated experiences of both families and professionals in the development of CPW whereby families highlighted the decision points that they considered most important in the pathway 54 and another recommended utilisation of clinician-led redesign efforts. 26
Healthcare Professional-Related Factors
Healthcare professional-related factors include professional competency, motivation and attitudes. 86 These are summarised in Table 7 below.
Healthcare professional-related factors barriers and enablers to CPW implementation strategies.

Barriers
Lack of staff clinical knowledge and skill is a perceived conflicting issue affecting individual staff confidence in interdisciplinary capabilities to use the CPW. 37 This was reported as affecting patient flow, timely room placement for patients, and administration of medication. 25 Lack of clear delineation about individual professional roles and responsibilities within the CPW were frequently reported barriers.35,37,40,56 CPWs were also perceived in one study to cause threats to individual professional scope of practice and autonomy. 37 Clinician lack of motivation and poor attitude towards use of CPWs were reported barriers. This was evident with some clinical professionals with more experience for example consultants opting to disregard the CPW document in favour of their own clinical expertise and knowledge.40,56 Poor team communication about the CPW process was reported as a significant barrier impacting CPW implementation. 35 This was reported as creating poor awareness of the CPW which resulted in the CPW not being utilised, especially during busy periods in the ED.37,69,79 In one study, staff reported that they were unfamiliar with scoring tools associated with the CPW. 72 Competing organisational initiatives at the same time were reported to result in change fatigue where staff were not able to prioritise new processes. 37
Enablers
A number of included studies suggested that the most successful approaches to improving health professional behaviour were built on good communication and broad engagement from multiple parties.24 -27,35,40,45,49,55 This ranged from working across departments, having engagement champions, to support of the multidisciplinary team (MDT) during development and implementation of the CPW.44,51,76 Adopting MDT focus was reported to lead to mutual ownership, respect, and adoption of the CPWs. 76 In addressing CPW implementation, targeted individual education modules for new staff at each changeover time was suggested. 79 One study suggested a review of team skills and roles at the beginning of each shift and use of low-cost, low-resource tools like dry-erase boards or paper-based visual prompts to lessen the cognitive load on staff as a strategy for successful implementation and use of CPWs. 81
CPW Operational Issues
CPW Operational issues were categorised as the design of the CPW document and accessibility issues like its location and stocking.87,88 Table 8 summarises the operational issues.
CPW operational related factors barriers and enablers to CPW implementation strategies.

Barriers
CPW document design was flagged frequently as a reason for not using the CPW.31,37,39,40,45,69,80,81 The CPW document design was perceived to be lengthy and created double documentation. 35 It was also perceived to cause inconsistency, variation in practice, and general non- adherence with the use of the CPW.39,40,45 The physical location of the CPW document within ED was reported as a barrier with some staff reporting uncertainty on its location. 79 Logistical issues were also flagged such as staff unsure of the restocking process for the CPW paper documents. 79
Enablers
One study proposed simplification of instructions and shortening the CPW order sets. 35 The simplicity of the CPW in its design and documentation with single-page CPW were preferred.41,53 Electronic CPW would simplify the process and reduce inconsistency and variation in practice. 41
Discussion
This scoping review reports on the approaches to implementation and use of CPWs in the ED as well as patient and organisational outcomes associated with the use of CPWs in the ED setting. The range of specific clinical conditions targeted in the ED suggest that the CPWs target medical conditions that are prevalent, costly to the healthcare system, and require extensive communication to prevent catastrophic effects on patient, carers and the healthcare organisation. 89 CPWs are context specific compared to clinical practice guidelines and therefore are inherently difficult to compare between health services as most will have different targeted pathways.
Many positive impacts of CPW use were noted, consistent with other studies reporting on CPW outcomes in departments outside the ED.89 -98 Our review suggests that CPW can reduce variation and improve quality of treatment in the ED setting, an important component of improving the safety, efficiency and effectiveness of healthcare for patients. Improvements in documentation quality, reduced clinical complications and decreased LOS were also apparent following the implementation of CPWs, factors which have been associated with better patient experience and improved staff satisfaction. 79 Whilst a reduction in LOS has many positive flow on effects in the ED, CPW implementation can also improve micro-level performance indicators like diagnostics which includes ordering tests and the provision of prescriptions,95,97,99 further contributing to improved outcomes for patients and for organisations. The micro-level performance indicators were reported in our study as evidenced by reduction in inappropriate imaging, prescriptions and antibiotic use.97,99 Further, the implications of a reduction in hospital complications include improved safety, efficiency and timeliness of care. 94 Whilst broadly suggesting positive outcomes with CPW implementation, our review also highlighted some mixed outcomes. These include an increased (or no change in) LOS, mortality and representation to the ED. This is also demonstrated in previous studies where there is inconclusive evidence around the impact of CPWs on mortality, 89 and on reducing hospital LOS. 95 Inconsistent findings across studies suggests that CPW use is different across settings and may be dependent on a range of barriers and enablers.
The three main categories of barriers that emerged in our review are consistent with other studies86 -88,96,97,100,101 and they incorporate issues like time constraints, workload, poor communication, limited availability of resources, lack of clarity with the CPW, lack of knowledge and skills, unclear individual professional role, motivation and attitude. These variables are common constraints in healthcare and worse in complex settings like the ED where staff are constantly working at high levels of pressure. There is no single strategy that is likely to result in successful implementation of CPW into the ED setting 79 as contextual factors will play a role in their development and use. Therefore, a thorough understanding of current and potential barriers and enablers for implementation is necessary to understand the individual components that will influence success and also the barriers that include organisational environment factors such as economic issues and availability of skilled professionals and external services to support ED discharge.37,79
Our review demonstrates that wide engagement with clinicians of all disciplines who use the pathways and involvement of multidisciplinary teams in implementation is vital to increase visibility of the CPW. This type of engagement allows gap analysis and involvement of multidisciplinary improvement teams resulting in increased adoption of CPWs. 100 The benefits of engagement and integration with existing systems, building intrinsic capacity and capability to create new innovations have been broadly reported enablers and are essential for the success of CPW use.97,102 Education strategies that ensure that healthcare staff are aware of the rationale behind CPW implementation have been suggested in other studies to bring successful CPW implementation. 97 CPW adherence can be increased through incorporating relevant education and training materials to already-existing education programs. 101 Barriers like low motivation, inadequate knowledge and skills could be overcome through timely and appropriate education. 101 Unclear guidance about each individual’s professional role in CPW implementation can result in poor engagement with the pathway and affects CPW implementation.97,102 One study argues that poor engagement is linked to historical fragmentation at organisational environment level and lack of strong leadership in the health sector. 103 CPW will bring organisational culture change which includes the process of modifying values, beliefs, and behaviours within an organisation. 103 However, this can be overcome through strategic alignment, improved information systems, feedback, and audits in organisations to enhance uptake and use of CPWs. 103
Positive benefits of CPWs are not only restricted patients but include benefits to the greater health care industry including staff.90,98 A previous study highlights the importance of promoting positive patient outcomes through a combination of professional and patient perspectives. 96 There were no patient perspective studies identified in our review. More meaningful decisions are made for a responsive health care service when a patient is asked about their values in addition to their wants or needs.89,104,105 Patient perspective in the frame of CPWs is of importance and the adoption of CPWs will not only give patients a good experience but assist in proactively addressing potential misunderstandings. 106
Limitations
Due to the wide range of CPW conditions covered by the included studies, subgroup analysis was not conducted, making it difficult to generalise findings to any one specific CPW condition. It is also critical to understand the constraints of the scoping review approach. In general, scoping reviews lack the empirical rigor of more quantitative literature studies like meta-analyses. There may be some reporting bias in our results as people who investigate the use of CPWs are usually engaged in the ED setting potentially resulting in positive reporting. Some useful publications may have been excluded as our review was only limited to English publications. Excluding conference abstracts may have impacted on identifying relevant evaluations including those with no impact or a negative outcome.
Future Research
Most of the studies in our review were conducted in the USA and studies in other countries with different funding models will be valuable. This will allow comparisons to be made on reported outcomes and different implementation approaches based upon healthcare funding models. 107 Future studies could further explore successful implementation strategies to assist with reliability and replicability. Evidence suggests that CPWs have a place in the ED, but developing, implementing, and evaluating them will require worldwide benchmarking and knowledge exchange. 14 Future research should explore collaboration between researchers, patients and their families, and clinicians to enhance sustainability. 106 To support iterative cycles of knowledge generation and improvement in healthcare, learning health systems have recently gained popularity. 108 The predominancy of quasi-experimental designs in our review demonstrates real-world practical solutions and a quality improvement approach in the ED setting. However, further research is required to investigate the effects of CPWs when drawing conclusions about causality. 89 Further research could also involve conducting meta-analyses and systematic review, and built standards based on the barriers and enablers to provide better generalisable real-world solutions
Conclusion
CPW implementation has wide positive patient and organisational outcomes in the ED. Whilst no single strategy would result in implementing CPWs in the ED settings successfully, broad engagement with clinicians of all disciplines who use the pathways and involvement of multidisciplinary teams in implementation is vital to increase visibility of the CPW. Key factors influencing the successful implementation of CPWs include organisational environment factors, healthcare professional factors and clinical pathway operational issues and should inform future implementation efforts in the ED setting.
Supplemental Material
sj-docx-1-his-10.1177_11786329251328527 – Supplemental material for The Use of Clinical Pathways in Emergency Departments: A Scoping Review
Supplemental material, sj-docx-1-his-10.1177_11786329251328527 for The Use of Clinical Pathways in Emergency Departments: A Scoping Review by Innocent Tawanda Mudzingwa, Sarah Jane Prior, Phoebe Griffin, Emma Tavender and Viet Tran in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251328527 – Supplemental material for The Use of Clinical Pathways in Emergency Departments: A Scoping Review
Supplemental material, sj-docx-2-his-10.1177_11786329251328527 for The Use of Clinical Pathways in Emergency Departments: A Scoping Review by Innocent Tawanda Mudzingwa, Sarah Jane Prior, Phoebe Griffin, Emma Tavender and Viet Tran in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329251328527 – Supplemental material for The Use of Clinical Pathways in Emergency Departments: A Scoping Review
Supplemental material, sj-docx-3-his-10.1177_11786329251328527 for The Use of Clinical Pathways in Emergency Departments: A Scoping Review by Innocent Tawanda Mudzingwa, Sarah Jane Prior, Phoebe Griffin, Emma Tavender and Viet Tran in Health Services Insights
Supplemental Material
sj-docx-4-his-10.1177_11786329251328527 – Supplemental material for The Use of Clinical Pathways in Emergency Departments: A Scoping Review
Supplemental material, sj-docx-4-his-10.1177_11786329251328527 for The Use of Clinical Pathways in Emergency Departments: A Scoping Review by Innocent Tawanda Mudzingwa, Sarah Jane Prior, Phoebe Griffin, Emma Tavender and Viet Tran in Health Services Insights
Footnotes
Acknowledgements
The project is part of the IMplementing CPWs for Acute Care in Tasmania (IMPACT) initiative which aims to promote adherence of CPWs into current patient-centred models of care across Tasmanian EDs.
Ethics and Dissemination
This study did not require ethical approval. The results of this research will be published in a relevant journal and will be presented at relevant international scientific events in emergency medicine and implementation science.
Author Contributions
The authors confirm contribution to the paper as follows: study conception and design: ITM, SJP, PG, ET; data collection: ITM, SJP, PG, ET; analysis and interpretation of results: ITM, SJP, PG, ET, VT; draft manuscript preparation: ITM, SJP, PG, ET, VT. All authors reviewed the results and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by a National Health and Medical Research Council (NHMRC) Medical Research Future Fund (MRFF) grant (No. GNT2018041).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.