
Abstract
Background:
Workplace violence remains a persistent health and occupational issue, but stakeholders often lack sufficient evidence to guide effective mitigation strategies. This review aims to ascertain the prevalence and determinants of workplace violence among healthcare providers in Ethiopia, where the issue is under-researched.
Methods:
The search included studies conducted in Ethiopia, regardless of publication year, that reported workplace violence among healthcare providers using PubMed, SCOPUS, Web of Sciences, EMBASE, CINHAL, Google Scholar, university repositories, and reference. After each author independently evaluated a study for inclusion, data was extracted, and disagreements were discussed and settled. A random-effects meta-analysis approach was used to evaluate the pooled prevalence, patterns, and determinants of workplace violence at 95% confidence intervals. Additionally, the I2 and P-value were used to evaluate the heterogeneity. Meta-regression and subgroup analysis were used to assess the difference by study-level characteristics. Additionally, to evaluate the stability of pooled values to outliers and publication bias, sensitivity analysis and funnel plots were performed.
Results:
A total of 6986 participants from 17 eligible studies were included in this study. Of the participants, 56% (95% CI: 48%-63%) reported having experienced any form of workplace violence. Verbal abuse accounted for 57% (95% CI: 49-65%), sexual harassment for 56% (95% CI: 48-65%), physical violence for 55% (95% CI: 46-63%), and bullying/mobbing for 51% (95% CI: 40-62%), according to the participants’ reports of workplace violence. Working night hours (AOR: 1.57; 95% CI: 1.20-1.93), being female (AOR: 2.24; 95% CI: 1.07-3.41), being single (AOR: 4.58; 95% CI: 2.44-6.73), working in an emergency department (AOR: 3.87; 95% CI: 2.33-5.41), and consuming alcohol (AOR: 2.69; 95% CI: 1.10-4.28) were all associated with a higher risk of workplace violence. Egger’s test and the funnel plot revealed no publication bias, and sensitivity analysis demonstrated that the pooled odds ratios were stable.
Conclusion:
Given the comparatively high prevalence of workplace violence and its various types among healthcare providers, a multilevel intervention strategy was necessary to address and lessen its effects. In order to make the workplace safer and avoid negative consequences for health care providers as well as the larger healthcare system, this strategy should incorporate both individual-level strategies and targeted policies.
Keywords
Introduction
Workplace violence, as defined by the National Institute for Occupational Safety and Health Administration (OSHA), is when employees are subjected to physical or psychological harm as a result of harassment, intimidation, or assault at work or during their way to and from work. 1 Workplace violence (WPV) significantly impacts healthcare providers, affecting their physical health, mental well-being, job satisfaction, and overall ability to provide quality care. All medical personnel, particularly nurses, are susceptible to WPV since they provide direct patient care and interact closely with patients and attendants. 2
There are 4 categories of workplace violence in the health sector, according to OSHA: type 1 involves a perpetrator who is unrelated to the company or its employees; type 2 involves violent client or patient behavior; type 3 involves violence between coworkers; and type 4 involves violence in personal relationships. 3 By decreasing the usual quality of healthcare systems, the WPV impacts both healthcare facilities and the people who surround healthcare providers (HCPs) by posing explicit or implicit threats to their health, safety, or well-being. Additionally, it causes health care providers to experience burnout syndrome and occupational stress. 4
Workplace violence has been a global public health concern and affects around 75% of health sector performance. 5 According to World Health Organization (WHO) data, over 63% of health care providers report they have experienced violence at work. Additionally, healthcare providers are 5 times more likely to experience it than people in other occupations. In Ethiopia, the prevalence of WPV ranges from 26.7% to 80.7%.6,7
Risk factors are sex of clients, 8 long waiting hours, sex of health professionals, 9 dissatisfaction with care, marital status of health professionals, 10 increased workload, aggressor psychiatric status, 11 and age.6,8,10,12,13 Moreover, working units,6,11,12 being a substance user,8,13 nurses ever stressed by job, 13 work experience,8,12,13 working between 6:30 and 7:30 PM o’clock, 13 availability of reporting system, 13 and number of staff are identified as its contributors.8,10,12,13 Moreover, the WHO reports that the occurrence of pandemics, including Ebola and COVID-19, increases the rate of WPV.
Even though WPV is very common in the healthcare sector especially in Ethiopia, many healthcare facilities lack established reporting systems or policies to address WPV. 11 This issue is often underreported and overlooked. Researchers and administrators have not given it enough attention, especially when it comes to management and prevention. Furthermore, prior primary research in Ethiopia has mostly concentrated on particular health occupations and geographical regions, with mixed results about the issue. Furthermore, in order to avoid WPV and enable the provision of high-quality healthcare to customers, this study is crucial in addressing these issues and producing aggregate data for health planners. Therefore, the purpose of this systematic review and meta-analysis was to evaluate the pooled prevalence, patterns, and determinants of WPV among HCPs in Ethiopia.
Methods
Study Protocol and Registration
Records of studies were identified, titles and abstracts were screened, and the eligibility of full texts for final inclusion was assessed using the Preferred Reporting Items for Systematic Review and Meta analysis (PRISMA). 14 Moreover, the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines were used to report the finding of this meta-analysis. 15 This systematic review was registered on the PROSPERO (CRD42024618978).
Eligibility Criteria
We included all observational studies (both published and unpublished) written in English that reported the prevalence and determinants of WPV among HCPs in Ethiopia and published before December 01, 2024. Nevertheless, we eliminated papers that did not report our main outcome of interest, studies that did not meet the Newcastle-Ottawa Scale (NOS) quality standards, 16 reviews, commentaries, and editorials were excluded.
Data Sources and Search Strategy
A comprehensive search was conducted across multiple databases, including PubMed, SCOPUS, Web of Sciences, EMBASE, CINHAL, Google Scholar, university repositories, and reference lists, without imposing any restrictions on publication year. This approach was chosen to ensure the inclusion of all relevant studies on workplace violence among healthcare providers in Ethiopia. A search approach was employed that combined mesh terms, keywords, and word variations for the frequency and determinants of WPV among HCPs with Boolean logic operators (AND, OR, NOT). We have selected MeSH terms and key words depending on relevancy and search optimization to increase the visibility of pertinent literature. Additionally, search strings were modified based on the databases’ particular needs. For instance, PubMed search: (((((work place violence) OR (“sexual harassment”)) OR (“physical abuse”)) OR (“verbal abuse”)) AND (“Healthcare workers”)) AND (Ethiopia). The search strategy is outlined in Supplemental Additional File 1.
Study Selection
After exporting all of the articles found through search techniques to EndNote X6, exact duplicates were eliminated. The reviewers (BB, UJ, NA, ELC, DF, and ML) then shared the EndNote library and used the title and abstract to separately conduct the first screening of the studies. The complete text was evaluated once the reviewers had reached a consensus after discussing and resolving any differences. The PRISMA statement flow diagram is used to display the entire research selection procedure (Figure 1).

PRISMA statement presentation for systematic review and meta-analysis of WPV among HCPs in Ethiopia, 2024.
Data Extraction
The data was individually extracted from the full text of the retained articles by each of the reviewers (BB, UJ, NA, ELC, DF, and ML). Data was extracted using a pre-defined Microsoft Excel 2013 template under the following headings: author, publication year, setting, region, study design, study subject, and primary outcomes of interest (Table 1). The accuracy of the data extraction was verified by comparing the results of the independently extracted data.
General characteristics of articles included in the systematic reviews and meta-analysis in Ethiopia, 2024.

Abbreviations: AA, Addis Ababa; DD, Dire Dawa; HCPs, healthcare providers; SNNPR, Southern Nation, Nationality and People Region.
Quality and Risk of Bias Assessment
The quality of the articles was appraised independently by all authors (BB, UJ, ELC, NA, DF, and ML) using Newcastle-Ottawa Scale (NOS) I2. The mean score of the author’s assessment was taken for a final decision, and any difference was solved by consensus. The included studies were evaluated against each indicator of the tools and categorized as high quality (> 80%), moderate quality (60-80%), and low quality (< 60%). Articles with moderate to high quality were included in the review. The purpose of this critical appraisal was to lower the possibility of bias and evaluate the studies’ external validity (generalizability) and internal validity (systematic error). To minimize the risk of bias extensive searches were used and also included published and unpublished studies. The role of the investigators was critical in reducing bias, during the selection of articles based on the clear objectives, eligibility criteria, quality of the article, and data extraction. Quality scores for each article were presented in Supplemental Additional File 2.
Outcome Measures and Statistical Analysis
The outcome variable was measured based on the primary article that reported by HCPs from the following any type of WPV; physical violence is the use of physical force against another person or group that results in physical, sexual or psychological harm, and it includes beating, kicking, slapping, stabbing, shooting, pushing, biting, and pinching, among others, 17 sexual harassment/violence is any unwanted, unreciprocated, and unwelcome behavior of a sexual nature that is offensive to the person involved, and causes that person to be threatened, humiliated or embarrassed, 17 verbal violence is using inappropriate language, insults and condescending expressions at a workplace 18 while bullying/mobbing is repeated and over time offensive behavior through vindictive, cruel, or malicious attempts to humiliate or undermine an individual or groups of employees.17 -19
STATA version 17 and Microsoft Excel 2013 were used for data analysis. The random-effect model was used for the meta-analysis. Forest plots were used to show the pooled prevalence and patterns of WPV among HCPs in Ethiopia. Also, subgroup-analyses were conducted using the regions and publication year of the studies. Moreover, sensitivity analyses were computed to assess the stability of pooled values to outliers.
Publication bias was assessed using visual inspection of a funnel plot and Egger test. In addition, a P-value <.05 for I2 statistics was used to determine the presence of heterogeneity. The results of the review were reported according to the PRISMA guidelines and presented using a narrative synthesis.
Results
Description of the Studies
A total of 893 papers were found using electronic databases, Google search, Google Scholar, lists of references, and repository of universities. All papers were exported to the endnote library, and 269 duplicated papers were removed. Also, a total of 567 unrelated papers were excluded after titles and abstracts were reviewed. Then, 57 papers were retrieved for detailed examination, and 40 papers were excluded due to different populations and outcomes of interest not being reported. Finally, full texts of 17 papers were selected for the methodological quality assessment using 2020 JBI (Joanna Briggs Institute) critical appraisal tools. 20 All appraised papers met the inclusion criteria and were included in the final review (Figure 1).
Characteristics of Included Studies
Seventeen cross-sectional studies with a sample size of 6831 were used to determine the pooled prevalence of WPV in Ethiopia. The prevalence of WPV included in the reviews ranged from 26.7% to 80.7%.6,7 Of those included studies, 5 were conducted in the Amhara region,6,8,10,21,22 4 in the Oromia region,13,23 -25 3 in the SNNPR,12,26,27 3 in Addis Ababa,7,9,28 and 2 in the Dire Dawa and Harari region11,29 respectively (Table 1).
Pooled Prevalence of Workplace Violence Among Health Care Providers in Ethiopia
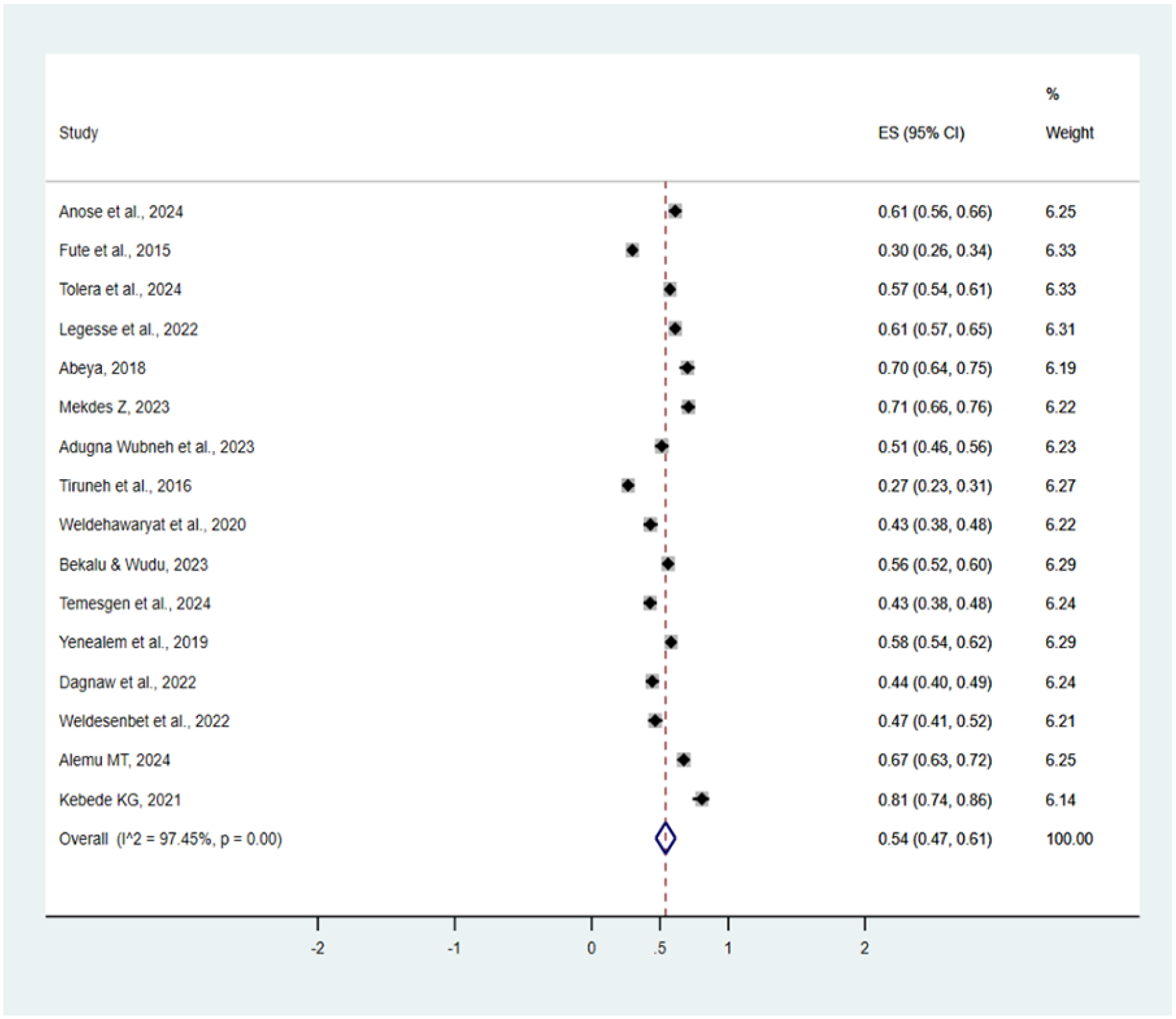
The overall prevalence of WPV was 56% (95% CI: 48%-63%), I2 = 97.75, P < .001. From a total of 6986 healthcare professionals included, 3736 had faced workplace violence which made out of 10 healthcare professionals, above 5 of them had faced workplace violence based on the pooled prevalence rate (Figure 2).

Forest plot for pooled prevalence of workplace violence among healthcare professionals in Ethiopia, 2024.
Subgroup Analysis
A subgroup analysis was performed to decrease heterogeneity in the national pooled prevalence of workplace violence. The subgroup analysis by publication year was performed and showed that the pooled prevalence of workplace violence among healthcare professionals before 2020 was 53% (95% CI: 32-75), whereas from 2020 to 2024 it was 57% (95% CI: 51-63). Moreover, subgroup analysis was performed by region, and the highest burden was found in Addis Ababa (72%; 95% CI: 69-76), followed by a study in Oromia (67%; 95% CI: 50-87), Harari (59%; 95% CI: 56-62), and Amhara (47%; 95% CI: 38-57) while the lowest pooled prevalence was found in SNNPR (45%; 95% CI: 26-64) (Figures 3 and 4).

Forest plot for workplace violence among healthcare professionals by year of publication in Ethiopia, 2024.

Forest plot for workplace violence among healthcare professionals by Region in Ethiopia, 2024.
Publication Bias
To observe publication bias, the Egger regression test revealed no evidence of publication bias among the included studies (P = .905). In addition, a visual inspection of the funnel plot was done and presented in the figure below (Figure 5).

Funnel plot that shows publication bias among included study in Ethiopia, 2024.
Multivariate Meta-Regression
Both univariate and multivariate meta-regression analyses were conducted to identify the sources of heterogeneity, as significant variability among the studies was observed. However, we found no significant variables that could explain this heterogeneity. Specifically, neither sample size nor publication year of the included studies emerged as statistically significant covariates. Consequently, the observed heterogeneity may be attributed to other factors not included in this review (Figure 6).

Heterogeneity test of workplace violence among healthcare professionals in Ethiopia, 2024.
Sensitivity Analysis
Sensitivity was done using leave one out analysis. There was no significant difference when the outliers and inliers were removed (Figure 7).
Sensitivity analysis of workplace violence among healthcare professionals in Ethiopia, 2024.
Patterns of Workplace Violence
This systematic review and meta-analysis showed patterns of WPV that pooled prevalence of verbal violence: 57% (95% CI: 49-65, I2 = 97.75, P < .001, sexual harassment: 56% (95% CI: 48%-65%), I2 = 97.75, P < .001, physical violence: 55% (95% CI: 46%-63%), I2 = 97.75, P < .001, and bullying/mobbing: 51% (95% CI: 40%-62%), I2 = 97.75, P < .001 respectively (Figure 8).

Pooled prevalence of patterns of workplace violence against healthcare professionals in Ethiopia, 2024.
Determinants of Workplace Violence
In this meta-analysis, we found 5 determinants of workplace violence among health care providers. The odds of workplace violence were 4 times higher among single than married healthcare providers (AOR: 4.58; 95% CI: 2.44-6.73). Healthcare providers working in an emergency department were 3.87 times more likely to experience workplace violence than those who were working in other departments (AOR: 3.87; 95% CI: 2.33-5.41). Being female healthcare providers increases the likelihood of developing workplace violence compared to their counterparts (AOR: 2.24; 95% CI: 1.07-3.41). In addition, health care providers who work night shift were 1.57 times more likely to experience workplace violence than those who work daytime (AOR: 1.57; 95% CI: 1.20-1.93). Moreover, healthcare providers who drink alcohol were 2.69 times more likely to have workplace violence than their counterparts (AOR: 2.69; 95% CI: 1.10-4.28). However, we found chewing chat, working in inpatient departments, work experience less than 5 years, and less than the number of staff were not significantly associated with workplace violence among healthcare providers (Figure 9).

Forest plot for determinants of workplace violence among health care providers in Ethiopia, 2024.
Discussion
This systematic review and meta-analysis aimed to assess the pooled prevalence, patterns, and determinants of WPV among HCPs in Ethiopia. Accordingly, a pooled prevalence of workplace violence among HCPs in Ethiopia was 56% (95% CI: 48%-63%). In this review, marital status, working in emergency department, being female, working night shift, and drinking alcohol were the identified determinants of workplace violence among health care providers in Ethiopia.
The finding of this review showed that a pooled prevalence of workplace violence among HCPs in Ethiopia was 56% (95% CI: 48%-63%) which was in line with the reports of Ajuwa et al (45.0%), 30 Berger et al (51%), 31 Liu et al (61.9%). 32 Moreover, it in line with systematic review and meta-analyses in the Asian (58%), 33 India (63%), 34 China (62.4%) 35 respectively.
However, it is relatively lower than the findings of systematic review and meta-analyses in China (71%), 36 Iran (66%), 37 and in Canada (69%). 38 The possible explanation for the observed discrepancy was study population; our study included all HCPs while the previous studies focus specified healthcare professionals who are more vulnerable for workplace violence such as Nurses 36 and Paramedics. 37 Nurses are more susceptible to any form of WPV because they are frontline healthcare providers and have frequent contact with patients and attendants while, Paramedics give services in a place where WPV is high such as emergency department, lack of privacy, and stressful environment for 24 hours. 39 In addition, the discrepancy might be related to differences in research design, sample size, and data collection methods in reporting outcomes.
Our study finding was higher than pooled prevalence reported by Ajuwa et al (45%), 30 Zhang et al (43%), 40 and Aljohani et al (24%). 41 Possible explanations for the variation might be related to contextual factors such as socio-political environments, economic conditions, and cultural attitudes towards healthcare can influence the prevalence of violence. There might be also variations in how workplace violence is reported and documented across different regions may lead to discrepancies in prevalence rates. Additionally, level of provision of Compassionate, Respectful, and Care (CRC) in Ethiopia was low which may harsh the relationships of client and healthcare professionals which may predispose them to WPV. 42
Furthermore, the differences might be in related to healthcare system strain: in Ethiopia, ongoing challenges such as both man-made and natural like disease outbreaks, floods, armed conflicts, limited resources, overcrowding, and inadequate infrastructure may exacerbate tensions between healthcare workers and patients or their families. 43 Many individuals cannot afford healthcare services that push them to use community based health insurance 44 which increase overcrowding of patients with low health professionals to clients ratio within the country, leading to delayed treatment and increased reliance on already overstretched public facilities. 45 When healthcare systems are strained and unable to meet the needs of the population, frustration can escalate, resulting in increased hostility towards medical staff. Addressing these infrastructural challenges is essential to improve both the safety of healthcare workers and the overall quality of care provided to patients.
A systematic review and meta-analysis conducted in Ethiopia revealed alarming patterns of workplace violence among healthcare professionals, with a pooled prevalence of verbal violence at 57% (95% CI: 49%-66%; I² = 97.46%, P = .001), physical violence at 55% (95% CI: 46%-63%; I² = 97.94%, P = .001), and sexual violence at 56% (95% CI: 48%-65%; I² = 97.65%, P = .001). These findings implies that workplace violence is a pervasive and serious issue within the healthcare sector in Ethiopia, significantly impacting the safety and well-being of healthcare professionals. The high prevalence rates highlight an urgent need for comprehensive strategies to address and mitigate violence in healthcare settings.
Addressing workplace violence is critical not only for protecting healthcare workers but also for ensuring the quality of care provided to patients. Implementing effective training programs, establishing clear reporting mechanisms, and fostering a culture of zero tolerance towards violence will be essential steps in creating a safer work environment. Ultimately, prioritizing the safety of healthcare professionals will contribute to improved job satisfaction, retention, and overall healthcare outcomes in the community.
The current review identified determinants of WPV among healthcare workers in Ethiopia. Thus, workplace violence was increased by 4 times among healthcare providers who were single than those who married. This finding was similar to a systematic review and meta-analysis.30,32 This could be due to single healthcare workers lacking the same level of social support that married individuals typically have, which makes them more vulnerable to aggressive behaviors from patients and their families. 46 Additionally, single healthcare workers might be more likely to work longer hours which increases their exposure to violent situations. 47 This finding provides new insights into the social and psychological factors influencing workplace dynamics in healthcare settings. This finding also calls for improving workplace policies and the need for robust support systems in healthcare institutions.
In this current review female healthcare providers were 2 times more likely to have workplace violence than male healthcare providers. The finding was in line with a review from 20 countries 30 and a gender-based review of workplace violence in the global health workforce reported women experienced more WPV than male. 48 Females in healthcare frequently occupy roles involving direct patient care and are perceived as easier targets due to societal norms that view them as less authoritative than males, increasing their exposure to aggressive behavior. Systematic reviews have also shown that female healthcare workers may underreport incidents due to fear of retaliation or stigma, compounded by insufficient support systems. 30 The psychological impact on female workers is significantly affecting job satisfaction and leading to long-term effects such as anxiety, depression, and burnout which also results in changes in their career aspirations and affect job satisfaction, further exacerbating workforce challenges.49,50 To address these issues, healthcare institutions should implement robust and confidential reporting mechanisms, gender-sensitive training, and support networks.
Healthcare providers who work in emergency departments are more likely to have workplace violence than healthcare providers who work in other departments. This was also reported in a systematic review and meta-analysis,30,32 which implicate these settings as risky for violence. The emergency department is characterized by a high-stress atmosphere, where patients often arrive in crises, leading to increased anxiety and aggression among patients and their families. 51 The 24-hour accessibility of the emergency department further compounds the issue, as it creates an environment where aggressive behaviors can escalate without adequate security measures in place. 52 Moreover, the culture within emergency departments often leads staff to perceive violence as an unavoidable aspect of their job, resulting in underreporting of incidents and a lack of institutional response. 53 Addressing workplace violence in emergency departments needs the implementation of comprehensive strategies that include adequate staffing, restricting public access, improved reporting mechanisms, adequate working & visitor spacing, and stronger institutional policies aimed at creating a safer work environment.
In addition, healthcare providers who work the night shift are more likely to have workplace violence than their counterparts. This is also reported review from Europe. 54 A rise in the acuity of patient conditions and reduced staffing levels during night hours can heighten tension and limit the ability to manage violent situations effectively. 55 Additionally, night shift workers are more prone to fatigue, which can impair judgment and the capacity to de-escalate conflicts.56,57 Increased workloads and longer wait times for patients can exacerbate frustration among patients and their families, leading to a greater likelihood of confrontations. 58 Moreover, security measures might be less robust during night shifts, making it easier for violent incidents to occur. 59 Addressing these challenges requires enhanced staffing, comprehensive training, improved security measures, robust support systems, and advocacy for policies that recognize and address the unique challenges of night shifts.
Healthcare providers who drink alcohol were 2.69 times more likely to have workplace violence than their counterparts. This might be the fact that those who use substances remark themselves as being at risk for violence due to the nature of the substance they use. Alcohol consumption can impair cognitive functions and decision-making abilities, reducing patience, increased irritability, and heightened emotional responses and making healthcare providers more vulnerable in high-stress and potentially violent situations. 60 To address these challenges, healthcare institutions can implement Employee Assistance Programs that create a supportive work environment emphasizing mental health and well-being, provide confidential counseling and support, promote awareness about the risks of alcohol use, enforce strict policies regarding alcohol use, and conduct ongoing research to understand the relationship between alcohol use and WPV.
The study provides a strong, more representative finding regarding the overall prevalence of workplace violence and its determinants among healthcare providers in Ethiopia. The limitation of this systematic review was not addressed perpetrators of workplace violence. In addition, there is significant heterogeneity across included studies, which may affect the results.
Conclusion
The prevalence of workplace violence and its types among healthcare providers was relatively high, warranting a multilevel intervention approach to address and mitigate the impacts. This approach should include targeted policies and individual-level strategies to create a safer work environment and prevent adverse effects on both healthcare providers and the broader healthcare system.
Supplemental Material
sj-docx-1-his-10.1177_11786329251325405 – Supplemental material for Prevalence, Patterns, and Determinants of Workplace Violence Among Healthcare Providers in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-his-10.1177_11786329251325405 for Prevalence, Patterns, and Determinants of Workplace Violence Among Healthcare Providers in Ethiopia: A Systematic Review and Meta-Analysis by Bikila Balis, Usmael Jibro, Nesredin Ahmed, Efrem Lelisa, Dawit Firdisa and Magarsa Lami in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251325405 – Supplemental material for Prevalence, Patterns, and Determinants of Workplace Violence Among Healthcare Providers in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-his-10.1177_11786329251325405 for Prevalence, Patterns, and Determinants of Workplace Violence Among Healthcare Providers in Ethiopia: A Systematic Review and Meta-Analysis by Bikila Balis, Usmael Jibro, Nesredin Ahmed, Efrem Lelisa, Dawit Firdisa and Magarsa Lami in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329251325405 – Supplemental material for Prevalence, Patterns, and Determinants of Workplace Violence Among Healthcare Providers in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-his-10.1177_11786329251325405 for Prevalence, Patterns, and Determinants of Workplace Violence Among Healthcare Providers in Ethiopia: A Systematic Review and Meta-Analysis by Bikila Balis, Usmael Jibro, Nesredin Ahmed, Efrem Lelisa, Dawit Firdisa and Magarsa Lami in Health Services Insights
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.