
Abstract
Addressing the mental healthcare needs of the population at the Primary Health Care (PHC) level has gained global consensus as a key strategy to realising the mental health targets of the United Nations (UN) Sustainable Development Goals (SDGs), especially SDG3. This research explored the question ‘What is the nature and level of community participation and ownership in the development and integration of mental healthcare service provision at the PHC, especially at Community Health Planning and Services Centre (CHPS) level(s) in Ghana?’. A cross-sectional study that adopted concurrent mixed quantitative and qualitative research methods was undertaken to explore and answer the question. The quantitative data of the study was collected through a survey questionnaire. Key informant interviews and focus group discussions were used to collect the qualitative data. Thematic analysis with the use of NVivo 12 was applied for the qualitative field data and Stata SE16 used for quantitative data. Data triangulation strategy was used to report both the qualitative and quantitative data sets. The study findings show that community participation and ownership was low, requiring more concerted efforts to engender that into mental health care policy and services development and implementation to realise the seamless integration of mental healthcare into general healthcare at the PHC level. Community participation and ownership will substantially enhance the (re-)organisation and resourcing of mental health services in Ghana to make them more responsive and inclusive.
Introduction
‘Mental Health’ used as a generic and inclusive term to refer to the concept of ‘mental ill-health’ and as well a positive state of social and emotional wellbeing, is a major public health and development issue globally.1–3 The concerns around mental health have to do with the significant contribution of mental health conditions to the global burden of disease, and the overall negative impact of mental health conditions on wellbeing, human rights and socio-economic development.4–6 Neglect of mental health risks the achievement of the global objectives set in the World Health Organisation (WHO) Comprehensive Mental Health Action Plan (2013-2030) and the United Nations (UN) Sustainable Development Goals (SDGs).7,8 According to the Global Burden of Disease 2019 Mental Disorders Collaborators, 9 mental health conditions accounted for 970.1 million estimated cases of age-standardised disease prevalence, corresponding to an increase of 48.1% of the disease burden between 1990 and 2019. Years Lived with Disability (YLD) was 14.6%, mental health disorders being the significant contributor to the burden. 9 Mental health conditions remain among the top ten leading causes of disease burden worldwide.9,10 Depression and anxiety disorder are the most common, and sub-Saharan Africa (SSA), north-Africa and Middle-East having the highest prevalence. Schizophrenia and eating disorders are the least common. 9
The fact that mental health has been a neglected area mainly due to the engrained social stigma associated with it and inadequate resourcing heighten the urgency to comprehensively address the associated emerging challenges.6,7
Addressing the mental healthcare needs of the population at the PHC level has gained global consensus as a key strategy to realising the mental health targets of the UN SDGs, especially SDG3.8,10–12 Community-based healthcare services can be traced to the Alma Ata Declaration with the PHC policy based on equity and community participation.13,14 Community participation and ownership and for that matter community health policy and service development are key to the realisation of Universal Health Coverage (UHC).15,16
The need to decentralise mental health and make it community-based came along with turning the Lunatic Asylums of the late nineteenth century into psychiatric hospitals and the provision of psychiatric services in general hospitals.17,18 The glaring need for mental healthcare services outside of psychiatric hospitals was acknowledged as necessary to complement the limited access and coverage the psychiatric hospitals provided.2,19,20 In Ghana, by 1972, a cadre of qualified nurses had additional training and christened Community Psychiatric Nurses (CPNs), were deployed into general hospitals to open, and manage Community Psychiatric Units (CPUs) that will provide treatment for mental health conditions to the population.
The Mental Health Act, 2012 (Act 846), abundantly stated the mental health care services in Ghana needed to be community-based. The mental health law emphasises decentralisation of mental healthcare services, and a human-rights centred approach to managing mental illnesses of the population. 21
In Ghana, up to 10% of the estimated 33 million people experience a mental health condition with up to 650,000 people in the country living with severe mental health conditions requiring medical attention.22,23 Undesirably, the country is associated with a high treatment gap of 98%, where less than 2% of the population with mental healthcare needs actually accessing treatment.2,24 Despite Ghana’s growing urbanisation, a significant proportion (41.4%) of Ghana’s population live in rural areas with rural poverty levels as high as 67.7% poverty headcount.25,26 Mental healthcare at the community level will be enhanced through a concerted effort to increase communities’ involvement in the development and structure of mental healthcare services at their level(s) and health system strengthening overall. This is particularly so for preventive and promotive mental healthcare services, as that positively impact treatment and management of mental health conditions, including rehabilitative care. Building a community-based mental healthcare system with active community participation and ownership guarantees an enduring, inclusive and benefiting mental healthcare system. The introduction of the WHO QualityRights which promotes patient/user-centred, recovery-oriented management of mental health conditions that people live with added impetus to the need for user-involvement and participation in the treatment processes.27,28 QualityRights emphasises user wills and preferences in the care and management their ill-health conditions, thus prioritising the participation and ownership in the mental healthcare services and policies.27,29 Similarly, the WHO Comprehensive Mental Health Action Plan 2020-2030 and the WHO Special Initiative for Mental Health provide yet another compelling case for health care systems to garner and maximise participation of mental health service-users and communities to ensure that mental health service provision is people-centred, rights-based and recovery-oriented.8,11,30
Community participation and ownership constitutes one of the health systems building blocks identified as essential to the production of health and whose exclusion from the health system framework could undermine responsiveness of health systems to the rights and needs of the people, for that matter overall health system. The WHO Regional Office for Africa describes community ownership and participation in the context of healthcare development to refer to a representative mechanism that allows communities to influence policy, planning, operation, use and enjoyment of the benefits arising from the delivery of health services. 31 It also refers to the community taking ownership of its health and taking actions and adopting behaviours that promote and preserve health. Community participation and ownership can therefore be understood and described as the collective and active involvement of local people in assessing the health needs, organising strategies and local resources to address those needs, with the firm sense that the service structures and results thereof were as a result of the individual and collective effort.32–35 Community participation and ownership in health encapsulates the principle and practice of bottom-up approach to health development and community health.36–39
Despite these longstanding intentions and pronouncements, in Ghana, community participation and ownership of mental health care policy and services remain barely existent. 40 In Ghana, there is limited evidence of successful and sustainable community involvement in the development of and provision of mental health care services. Mental health care effectively remains isolated and parallel to the rest of the healthcare system of the country, with Ghana’s current mental healthcare system described as being overly centralised, medicalised, and generalised with rare community involvement.
This study is part of a PhD thesis exploring the research question, ‘What is the nature and level of community participation and ownership in the development and integration of mental healthcare service provision at the PHC/CHPS level(s) in Ghana?’ as part of in exploring perspectives of stakeholders in the integration of mental healthcare services at the PHC/CHPS in Ghana utilising the WHO Health System Framework which is enhanced by be the Ouagadougou Declaration on Primary Health Care and Health Systems for Africa. The objective of the study is “to assess the nature and level of community participation and ownership in the integration of mental healthcare at the PHC level.”
Materials and Methods
Study area
The study was conducted in the Republic of Ghana. Ghana is divided into sixteen regions (Figure 1) and three coterminous ecological zones (Northern, Middle, and Southern). In terms of health service delivery, the country operates a five-tiered service system, covering National, Regional, District, Sub-district, and the Community.41,42 The regional, district and community level health facilities are established to provide secondary and primary health care services. 42 In 1999, Ghana adopted the Community-based Health Planning and Services (CHPS) strategy as a primary health care system to bring basic essential healthcare services closure to the people with their active participation.43–46

Map of Ghana.
Study population
The study population were respondents aged 18 years and above who were health policy officials and health service managers, health care service workers, people living with mental health conditions and or primary caregivers of people living with mental health conditions, as well as staff of civil society organisations working in the mental health space, and patient/ human rights advocates. The respondents were categorised into three utilising the Human Rights-Based Approach (HRBA) of ‘rights holders’ and ‘duty bearers’ with a mixed category of both rights-holders and duty-bearers. 47
Study respondent inclusion and exclusion criteria
The inclusion criteria were that the respondent is an adult of legal age 18 years and above, with a role in mental health, located within the target study communities and healthcare facilities, freely and wilfully giving consent to participate in the study. They included persons with mental health conditions receiving medical treatment for their mental illness with significant reduction of the symptoms of their mental ill-health conditions ready to participate of their own freewill. Primary caregivers of persons living with mental health conditions, healthcare service provider(s), healthcare service manager(s) within the study location, as well as health policy official(s) at national and sub-national levels. Patient advocates and officials of known funders of mental health initiatives in Ghana.
Exclusion criteria covered persons below the legal age of an adult, a person with no clinical diagnosis of his/ her mental health condition and not receiving treatment from outside a formally recognised medical facility and is a person not normally residing in the target study locations or stakeholder not willing to give consent.
Study design
This was a cross-sectional study that employed concurrent triangulation mixed methods design.48,49 A mixed methods approach involving the use of both qualitative and quantitative methods was deployed to maximise the effect of both methods in understanding the phenomena being studied. 48 A cross-sectional descriptive study design was used for the quantitative component of the study.48,50,51 The design of the qualitative arm of the study was a critical descriptive ethnography approach.48,52 The study was carried out with the conceptual framework of the WHO Health Systems Framework 53 and the Ouagadougou Declaration on Primary Health Care and Health Systems in Africa 31 in which the health systems building blocks guided the study.
Sampling and sample size determination
Stratified purposive sample was used for the quantitative method. A sample of 1104 potential respondents of the survey was established. This sample size was computed using Epi InfoTM programme developed by the United States of America Centers for Disease Control and Prevention (CDC), (https://www.cdc.gov/epiinfo/index.html). A 75% response rate was achieved in the survey. The final sample was proportionally split among the target districts to reflect the differences in the populations of those locations. Being a cross-sectional descriptive study, the sample of this study did not have to satisfy a statistical power.
For the qualitative arm of this study, purposive sample, ensuring maximum variation, was utilised. Key Informant Interviews (KIIs) and Focus Group Discussion (FGDs) were used to collect the qualitative data. Study respondents selected were stakeholders who play critical roles in mental health care service organisation and delivery and service utilisation. The selected individual stakeholders were based on initial desk review of available policies and laws on mental health in Ghana and available literature within Ghana and other countries.54,55
Data collection tool(s)
A survey instrument (questionnaire), developed by the lead author, which was informed by the WHO ‘Systems Thinking for Health System Strengthening’ framework, 56 was used to collect the quantitative data. The questionnaire was developed using Microsoft 365® Forms. 57 For clarity and relevance of the data collection tools the survey questionnaire and discussion guides were pilot-tested in the LEKMA Municipal area of the Accra Metropolitan Area at the LEKMA hospital and surrounding households. The discussion guides were tested in the Ledzekuku community of LEKMA with two groups, each with nine participants. One being a group of members of a mental health Self-help peer support Group (SHG), and the other, a group of community volunteers.
Data collection procedure
The quantitative data was collected using the survey questionnaire for target study respondents to self-complete or via interviewer assisted face-to-face administration. Data collection assistants were recruited and trained to serve as interviewers to assist the majority of respondents who could not self-complete the questionnaire. Informed consent was obtained for all respondents. Capacity of study respondents to provide consent was by affirmation where the research participants themselves expressed the free and willing participation because of their full understanding and acceptance of the purpose of the research, and the potential risks thereof. Participants signed the consent form and those who self-completed the survey questionnaire, completing the questionnaire was taken as consenting to freely participate in the study.
The survey data was collected from 830 (469 female) available and willing respondents who fully completed the questionnaire giving a 75% response rate. Non-participation was mainly due to timing when after three follow ups a respondent was not available to complete the survey.
The qualitative data was collected through KIIs and FGDs using the interview and discussion guides developed for the study. The Principal Investigator led the KIIs and moderated the FGDs with the assistance of data collection agents who were hired and orientated for the purpose of the field data collection note-taking and related arrangements. A total of 27 KIIs covering 27 (13 female) respondents, and FGDs, (N = 12) involving 75 (40 female) respondents, were conducted (Table 1).
Respondents of qualitative data collection.

Triangulation of information collected from the data was used during analysis to gain richer understanding of complex processes of the multiple data collected enabling constant comparison and synthesis of the data. The qualitative data covered the same topics as the questionnaire which allowed for in-depth exploration of the questions. Saturation58,59 was achieved when no new and additional information could be obtained.
The data collection was over four months between November 2020 and February 2021.
Reflexivity, trustworthiness, and rigour
The authors did recognise and were conscious of their personal beliefs and assumptions, acknowledging their relationship with the research topic and the respondents. This was assured by applying scientific steps and process(es) to generating empirical knowledge, immersing with the data collected from the field rather than emotive firsthand and or previous experience. Field data collected was inputted and analysed by different individuals limiting or eliminating bias altogether.
Analysis
The quantitative data was analysed using StataSE 16 (64 bit) statistical software. 60 The statistical analyses were descriptive statistics of stakeholder self-reported/ self-rating of selected indicators to gauge levels of integration of each of the health system building blocks, and the results presented in the form of tables, charts, and frequencies. Means values of selected indicators were compared with cut-off scores of levels of integration to gauge perspectives of the three categories of respondents overall. Three levels of integration were assigned being ‘Fully Integrated’, ‘Partially Integrated’ and ‘Not Integrated’.
The qualitative method adopted a critical descriptive ethnography approach. Transcription and analyses of the interviews and discussions held were done alongside data collection. Analyses of the qualitative data took an initial analysis of listening to the audio recordings and poring through the notes recorded during the KIIs and FGDs. The procedure of thematic analysis provided by Braun and Clarke. 61 After the data collection, samples of the interviews were reviewed and new codes added to the codebook. Double coding was done after which it was compared. The inter-coder reliability index was computed as 0.87. The themes identified were applied, and then utilising NVivo 12 qualitative research analysis software package to extract codes from the transcripts.62–64 The extracted codes were used in the presentation of findings in the form of quotes of perspectives and experiences, as well as recommendations. As the results were based on self-reported scales/ rates, more weight was placed to the qualitative data.
Results
The results were presented by characteristics of study respondents followed by the indicators that determine levels of community participation and ownership as a key building block of the health system framework. A total of 830 study respondents fully completed the questionnaire giving a response rate of 75%). At total of 102 (53 female) participated in the qualitative data collection. They were made up of 27 (13 female) key respondents and 75 (40 female) focus group discussants.
Characteristics of study respondents
Majority of the survey respondents were female (56.6% [469/830]). Majority of the respondents (46.9%) [389/830] were within the age bracket of 28-37. More than two-thirds of them, [84.2% (698/830)], had formal education, at least, primary school level education, with 15.9% (132/830) with no formal education at all. As high as 72.7% (604/830) of the respondents had tertiary level education, mostly from medical/ health training institutions, teacher training colleges, polytechnics and other professional training bodies, colleges and universities. They were also employed, mainly in the agriculture and food processing sectors, handicrafts and artisanal ventures, petty trading, and services, including manual labour (head porters, cleaning).
Tables 2–4 provide details of findings of survey respondents. Table 2 detail results of the data analysed by the three broad categories that the survey respondents were grouped under. Table 3 details findings based on respondents’ location by the three geographical zones that the study areas were organised into. Table 4 presents total means scores indicating overall self-reported views of the levels of community participation and ownership in the integration of mental healthcare at the PHC.
Study participants’ (by category) responses on community participation and ownership in mental healthcare at the PHC level and extent of integration at that level (N = 830).

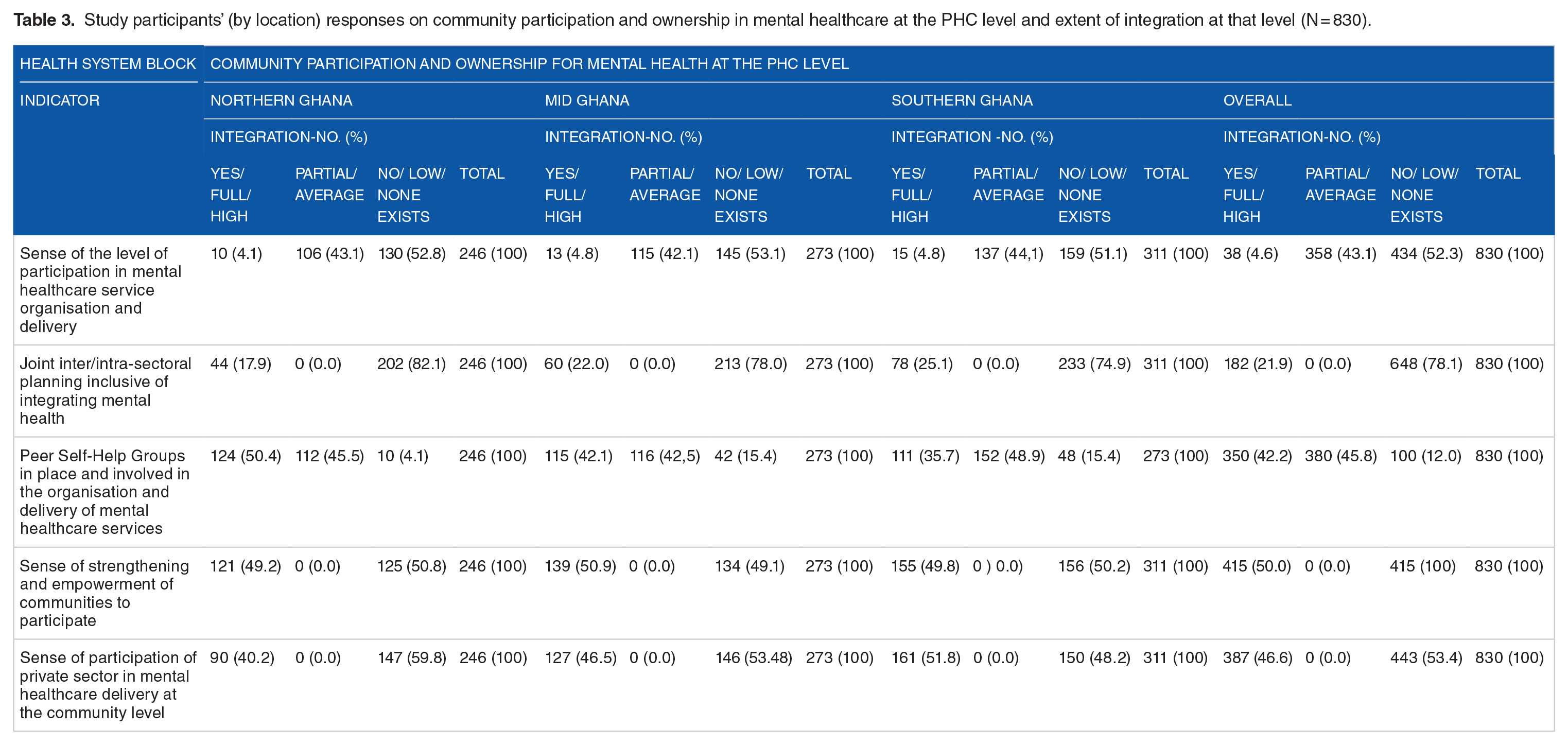
Study participants’ (by location) responses on community participation and ownership in mental healthcare at the PHC level and extent of integration at that level (N = 830).
Community participation and ownership in mental health development and integration the PHC by respondent category and geographical zone (N = 830).

NB: Mean value >3.0=Full integration; Mean value =2.0-3.0 signifies Partial integration; Mean value <2.0 signifies No integration.
Sense of the level of participation in mental healthcare service organisation and delivery
Survey respondents gauged the sense of community participation in mental healthcare service organisation and delivery at the PHC level as low, by 52.3% (434/830). Less than ten percent, 5.0% (41/830), of respondents indicated that there was a sense of community participation and ownership in mental healthcare service organisation and delivery at the community level. Mental health services users and caregivers, by 60.5% (279/461) were the category of respondents with highest percentage of the view that the sense of participation in mental healthcare service organisation and delivery at the community level was low. Similarly, a little over half, 50.4% (130/2568), of health policy officials/ health policy implementers and healthcare service implementers, found the sense of participation as low, for that matter an indication of inadequate involvement of communities in mental healthcare service organisation and delivery at the PHC level. The category of mental health / human rights advocates, development partners and donors, 63.1% (70/111), on their part gauged the level of participation as partial, for that case, just fair.
By the geographical location of the respondents (Table 3), sense of participation in mental healthcare service organisation and delivery was found to be low across the three zones by more than half, (52.3% [434/80]), of the study respondents. Respondents from Mid Ghana were the majority (53.1% [145/273]) of the three geographical zone holding the view that the sense of participation in mental healthcare service organisation and delivery was low, and followed by Northern Ghana, 52.8% (136/246, and Southern Ghana, 51.1% (159/11). Qualitative data analysed conveyed a mixed sense of community participation in mental healthcare organisation with respondents of the view that there was a sense of participation attribute that to engagements NGOs have with them.
There is no participation. You are given what is available. The nurses don’t ask how things can be improved for us. FGD, caregiver, mixed group of mental health service users. The NGOs do it. They hold meetings with services users, primary caregivers and families and they discuss with them how they can work together and improve their lives. The feel consulted and that is important. KII, mental health advocate We participate in annual district and regional review meetings, but we do not have joint planning sessions or meetings to discuss how the various units can collaborate to enhance mental healthcare at the community level. FGD, CPNs It is the NGOs who do invite the mental health workers for meetings about their programmes. Also, the Mental Health Authority invites stakeholders to their annual review meetings where they present what has been done for the year but there are no meetings to plan activities for the year. KII, mental health advocate.
Joint inter/intra-sectoral planning inclusive of integrating mental health
Another indicator to gauge the level of community participation and ownership in mental health care service organisation and delivery was understanding of joint inter/intra-sectoral planning that is inclusive of integrating mental health at the PHC level. More than two-thirds, 79.3% (658/830) of respondents did not find that to exist and so not engendering integration of mental healthcare at the PHC level. Mental health service users and caregivers/ families by 96.3% (444/461), and more than half of health policy officials, health policy implementers and healthcare workers, 63.2% (163/258) indicated a low level of joint and inter/intra-sectoral collaboration and planning inclusive of mental healthcare. However, the category of mental health/ human rights advocates, and health development partners and donors, (54.1% [60/111]), were of the view that joint inter/intra-sectoral planning inclusive of integrating mental health at the PHC level was happening. Less than a quarter of respondents, 20.7% (172/830), indicated that such joint and inter/ intra-sectoral planning happen.
While across all the three geographical zones, over 70% of the respondents held the view that joint and inter/ intra sectoral collaboration and planning inclusive of mental healthcare service organisation and delivery at the PHC was not happening, up to a quarter of respondents in southern Ghana, 25.1% (78/311) and mid Ghana, 22.0% (60/273), indicated collaborations exist that help to advance mental healthcare organisation and delivery at the community level. Qualitative data affirmed views of survey respondents that joint and inter/intra sectoral collaboration and joint planning at the PHC was absent.
It is not easy, but we try to ensure mental health is featured in our DHMT meetings and that makes it imperative to plan something. So, we do. Their nurses [CPNs/CMHOs] participate in immunisations and supportive supervision. This is to help make sure mental health is not forgotten and also the staff don’t feel left out. KII, District director of health We never hear of meetings called to plan for mental health service delivery. We are not invited. It is we the SHGs who go to the district assembly to present our challenges. Sometimes we are supported with funds under the district assembly disability fund and other times we are told is not there because central government has not released the Common Fund, FGD, mixed group of mental health and epilepsy service users and primary caregivers Such sectoral linkages will have been helpful for mental health for there are obvious synergies and mental health will have benefited from the other sectors. The other sectors could also at some point benefit from mental health. KII, development partner/ donor You know mental health has been left out in health matters for long. Despite the laws and policies, if there is no financial backing, it will really be a challenge to get the needed integration. Of course, with time things will change for the better. FGD, CPNs & CMHOs
With regards the stakeholders most actively involved in the organisation and delivery of mental health, Figure 2 presents the results from data of the survey respondents.

Perception of most consulted stakeholder in the development and delivery of mental health services at the Primary Health Service level.
NGOs/CBOs/CBOs were identified by survey respondents as the most actively engaged stakeholder(s), 41.8% (347), in the organisation and delivery of mental healthcare services at the PHC level. General healthcare workers were the next, 29.9% (247), then district/ regional directors of health services/ medical directors and in-charge(s) of health facilities, 12.5% (104), followed by caregivers of people with mental health conditions, 6.9% (57), and finally users of mental health services, 4.9% (41) and policy officials, 4.0% (33) with that view. The low level of involvement of mental healthcare service users most likely signals the low priority placed on the eliciting views from people with lived experience. Qualitative interviews emphasised the active involvement of civil society not-for-profit organisations involved in mental healthcare at the PHC level.
It is the NGOs who are more focused on mental healthcare services in the communities. They come around and talk about mental health services available, stigma and the need for families to take their relatives for treatment at the hospitals. KII, Regional Mental Health Coordinator
Peer Self-Help Groups in place and involved in the organisation and delivery of mental healthcare services
On the existence and involvement of Self-Help peer support Groups (SHGs) in the organisation and delivery of mental healthcare services at the PHC level (Table 2), the views of survey respondents were that it was low, 59.0% (490/830 of them), indicating a low level of involvement, with the rest, 41.0% (340/830), who gauged it as a high level of involvement. Mental health service users and caregivers the least view of involvement of SHG in the organisation and delivery of mental healthcare services, with a majority of them, 70.5% (325/461) indicating so. Mental health/ human rights advocates, development partners and donors were split, virtually equally, in their view(s) of the level of involvement of per support groups in the organisation and delivery of mental healthcare services at the PHC level. By geographical location (Table 3), respondents within the northern Ghana, by 50.4% (124/246), held the view that there was involvement of peer support groups in the organisation and delivery of mental healthcare services at the PHC level. Southern Ghana was close to half of the respondents, 48.9% (152/311), and mid Ghana being 42.5% (115/273), with similar views that SHGs were involved in the organisation and delivery of mental healthcare services at the community. Data from KIIs and FGDs attributed involvement of SHGs of persons with lived experience to the presence and operations of NGOs in the mental health sector.
These support groups are in place because of the activities of NGOs. With good organisation and support the support groups will be a key stakeholder to involve, especially that you can reach the caregivers and families through them. A good relationship can be developed in support of the mental health services user. KII, CPN
Sense of strengthening and empowering communities to participate in the development and delivery of mental healthcare services at the PHC level was yet another measure used to examine the level of community participation and ownership in the integration of mental health care at the PHC level in Ghana. Survey respondents viewed sense of strengthening and empowering communities be high by 56.8% (471/830), with 45.7% (379/830) indicating otherwise (Table 2). Health policy officials, healthcare policy implementers and healthcare workers were the category with majority of respondents, 74.8% (193/258), who indicated that there was a high level of sense of community strengthening and empowerment for mental healthcare service organisation and delivery at the community level. However, more than half of mental health / human rights advocates, development partners and donors, 54.1% (60/111), and mental health service users and caregivers, by 50.8% (234/461), held the view that there was low level of community strengthening and empowerment to enable them to participate in the development and integration of mental healthcare at the PHC level. Geographically, survey respondents were split with regards their sense of strengthening and empowerment of communities to be involved in the organisation and delivery of mental healthcare at the PHC level (Table 3). Respondents in northern Ghana, by 50.8% (125/246), considered the level of the sense of strengthening and empowerment to be low, just as with respondents in southern Ghana, 50.2% (156/311).
Qualitative data indicated that there is generally a low level of involvement of communities and stakeholder groups in the organisation and delivery of mental healthcare services at the district and the lower levels of care (PHC/CHPS).
We are not invited to discuss the services delivered in the hospital. Apart from the nurse asking you how are feeling when you go for your medicines, we are not consulted. The NGOs like BasicNeeds meet us. They encourage us to organise our groups so that we can support one another and help people to go for treatment. FGD, mental health and epilepsy service users
Sense of participation of private sector in mental healthcare delivery at the community level
Private sector involvement in mental healthcare service organisation and delivery at the PHC level of the health system of Ghana was found to be low by 53.4% (443/830) (Table 2). Mental health service users and caregivers were the majority of survey respondents, by 56.0% (253/461) indicating so, and closely followed by health policy officials, health policy implementers and healthcare workers, 53.9% (139/258). With regards to the geographical zones of the study locations (Table 3), northern Ghana had the majority, 59.8% (147/246), of respondents indicating absence of private sector involvement in the delivery of mental healthcare services at the PHC level, followed by mid Ghana, 53.5% (146/273). However, a little over half of respondents from southern Ghana indicated a sense of involvement of private sector in mental healthcare service delivery at the PHC level. Qualitative data of this study identified traditional healers as part of private sector with others indicating otherwise.
We can include traditional herbalists and faith-based healers as part of private sector so there is some involvement. However, if it is involvement of private orthodox / formal or western medical services, there is low involvement in mental healthcare service delivery at the local level. The few that are there are in the urban areas, and this includes the religious bodies that ran rehabilitation centres. KII, national mental health official
Table 4 details the composite means scores from the indicators and themes used to explore and assess community participation and ownership in mental healthcare at the PHC level. The general impression about community participation and ownership in the organisation and delivery mental healthcare services at the PHC level was viewed as partial with a means score of between 2.20 and 2.50 (Table 4 below) across the three respondent categories and the geographical zones. The category of mental healthcare service users, primary caregivers and families, and respondents of northern Ghana had the lowest means score (2.30).
Discussions
In this paper, we examined a number of engagement and involvement indicators that demonstrated a sense of community participation and ownership in mental healthcare service organisation and delivery at the PHC.
Community ownership and participation is most realised through the activities of community-based organisations and non-governmental organisations. They are organised and articulate the needs and interests of communities and groups and individuals with lived experience of mental health conditions. Family involvement in mental healthcare delivery is also important in engendering community involvement in the organisation and delivery of mental health policy and services. Effectiveness of mental health interventions are best achieved when there is high level of community involvement and sense of ownership of the service intervention, particularly by service users and caregivers as primary beneficiaries.
This study indicated partial to low level of community ownership and participation in the organisation and delivery of mental healthcare at the PHC. Qualitative data analysed identified the presence and activities of self-help groups of people living with mental health conditions and their primary caregivers as the key and positive factor to have brought about the sense of participation and ownership being partial by study respondents. Lempp et al 66 , in their study on mental health service user and caregiver involvement in mental health system strengthening across three countries, found varying responses that on the whole indicated limited engagement and involvement in mental health service strengthening at the primary care level. Except for a minority of service users in Nigeria and Ethiopia that felt consulted, there were hardly any respondents that had experience of being consulted or involved in discussions on expanding access to mental health care or integration of mental healthcare at primary health care settings in LMICs. In this regard, the partial involvement in Ghana is significant although a lot more effort is required to increase and sustain community participation and ownership in mental healthcare service organisation and delivery at the primary healthcare level. Involvement of users of mental health services which is considered essential can be said to have been addressed, even if somewhat, by the presence and activities of the self-help groups. This is especially so as it has been recognised that it is important to promote and ensure the active participation of service users in mental healthcare service organisation and delivery.
To realise this requires that there should be individually focused collaboration, consultation and inclusion of a cross-section of stakeholders in decisions they have to make in their encounters with the providers and the system. There should be recognition of the mental health conditions that people living with mental health conditions have and strive to facilitate their participation at service or system level as peer workers or advocates for policy and practice change.66,67 This supposes that even with the partial level of participation a real and meaningful level of participation reflecting these desirable aspects consolidates the sense of involvement and ownership. Similarly, Kohrt et al reiterate that community and user involvement enhances appropriateness and quality of the mental healthcare services delivered and also ensures that protection and promotion of the rights of people with mental health conditions. Kohrt et al 68 further mention that community ownership and participation should not be limited to accessibility of the intervention but community acceptability. The partial level of involvement from the study most possibly has most likely not attained total acceptability of the mental healthcare services delivered hence the need to strive to reach that optimal level.
Health policy officials, healthcare service managers, and healthcare service providers, along with patient/ human rights advocates, and donors/development partners in the study particularly gauged the level of community participation and ownership to be low and this can be attributed to the generally low governmental level priority placed on mental health and related issues. The engrained lack of attention to mental health has undermined the attention of state/governmental effort 69 to engage communities and user groups on improving mental healthcare service organisation and delivery at the PHC level as well as ensuring integrated mental healthcare services at that level. The low level of involvement also was pronounced in the northern Ghana area in five out of the eight indicator types of participation and ownership in mental healthcare service organisation and delivery at the PHC level and toward mental health integration at that level. A study conducted in northern Nigeria found similar limitations where the few individual level mental health services provided at the PHC level were not known to service users as a result of their non-involvement in the organisation and delivery of the mental healthcare services to the population. 70 This is an example of geographical inaccessibility challenges, especially as the northern part is further away from the national capital and more developed southern part of Ghana. The geographical inaccessibility challenge is attributed to limited number of mental healthcare providers involved in community level mental health awareness creation activities, and inadequate governmental level resourcing of mental health, as well as generally low levels of literacy of people.
It is necessary that the prevailing situation is improved for the better. As mentioned by a number of study respondents, the activities of non-profit non-governmental organisations, such as BasicNeeds-Ghana, have helped to give attention to mental health in the communities with a high potential of not just knowledge and awareness, but ensuring actual active involvement of individuals living with mental health conditions, families and indeed entire communities at large in the type and quality of services that are arranged and delivered at the community level. Such efforts complemented by the Government of Ghana (GoG) will ensure mental healthcare service organisation and delivery are adequate, responsive and inclusive. Activities of the SHGs are important and need to be supported to enhance participation and involvement of servicer users and caregivers in mental healthcare at the PHC level.
Limitations
This study employed a mixed method approach to maximise its scientific rigour and generalisability. The qualitative data collected had interviews and discussions conducted in the English and local language. Translating the local language(s) into English language usually resulted in use of terms that do not exactly express the equivalent of the local language. To address this, there was a focus on the main themes of the study. Secondly the purposive sampling adopted could have missed respondents with foreknowledge of the subject matter. These were addressed largely by ensuring individuals and institutions with stake in mental health were ensured using policy and stakeholder analyses. Financial and time constraints did not make it possible for a such large-scale approach to be applied in the study. COVID-19 and the restrictions and protocols to contain the spread and negative impact of the disease on people and society in general influenced community engagements.
Conclusions
There is inadequate community participation and ownership in the development of community mental health, for that matter limiting the integration of mental health care into general health care services at the PHC level. Every effort is needed to maximise community efforts and resources to achieve the synergies and health comes. The importance of political skills in fostering mental health reform has been well documented and this needs to be emphasised in Ghana. Being isolated, least prioritised, and even antagonised sometimes, nimble pollical manoeuvrings are needed to build support and sustain commitment for mental healthcare, especially at the community level. Political commitment to a process, taking advantage of windows of opportunities help in navigating the intricacies of the mental health sector and encouraging active community involvement and maximisation of community-based resources.
Recommendation(s)
It is imperative that mental health care services in Ghana need be organised and resourced. Engagement and involvement of communities, particularly persons living with mental health conditions and primary caregivers is essential in strengthening the development and scale-up of mental healthcare at the PHC. Realising this will require re-tweaking arrangements and processes for development of PHC systems with integration of mental health in mind. Mental healthcare services at the community level need to be less medicalised and more oriented to social medicine to enable participation and support. Existing health system structures do not encourage participation by community individuals and groups.
Supplemental Material
sj-docx-1-his-10.1177_11786329251318593 – Supplemental material for Stakeholder Perspectives on Community Participation and Ownership in Community Mental Health Policy and Services: Mixed Methods Study in Ghana
Supplemental material, sj-docx-1-his-10.1177_11786329251318593 for Stakeholder Perspectives on Community Participation and Ownership in Community Mental Health Policy and Services: Mixed Methods Study in Ghana by Peter Badimak Yaro, Philip Teg-NefaahTabong and Emmanual Asampong in Health Services Insights
Footnotes
Acknowledgements
Moses Sekyi Aikins
Graham Thornicroft
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PBY receives salary from BasicNeeds-Ghana, where he is Executive Director.
PTT, and EA have no financial interest(s).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by PBY, PTT, and EA. The first draft of the manuscript was written by PBY and all the authors commented on previous versions of the manuscript. All authors read and approved the final version of the manuscript.
Disclosures and declarations
EQUATOR Network guidelines for preparing manuscripts was used
Consent to participate and/ or Consent to publish
Consent was obtained from all individual participants included in the study
Authors affirm that human research participants provided informed consent for publication of images in Figure(s) 1, 2, and 3.
Ethical approval
Ethics review approval was received from the Ghana Health Service (GHS) Ethics Review Committee (ERC) numbered GHS-ERC018/12/19. Letters of permission were also secured from relevant government health agencies and political/ administrative institutions.
Informed consent from participants
Study respondents provided consent after the information brochure summarising the study was read by themselves of read to them in either English Language or the local language that they understood. Written permission was provided by institutions who were engaged, particularly the Ghana Health Service and Mental Health Authority of Ghana.
Data and/or Code availability
The data that support the findings of this study are available on request from the corresponding author [PBY].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.