
Abstract
Objectives:
To investigate the levels of change fatigue among clinical nurses in public hospitals and identify the potential contributing factors.
Design:
A cross-sectional, multi-stage sampling study was conducted in accordance with the STROBE guideline.
Methods:
This study surveyed 2,228 nurses in China from October to December 2023 using Wen Juan Xing (www.wjx.cn) and employed stepwise multiple linear regression analysis to assess factors associated with change fatigue.
Results:
The average change fatigue score of nurses was found to be at a medium to high level. Factors such as female, professional title, average overtime hours, workflow changes, workload increase, work-content changes, work pressure increases, new technology implementation and the change frequency were all identified as exacerbating nurses’ experience of fatigue related to change. Contrary to this, the support of change resources, communication and transmission of change information, distributed leadership, inclusive climate, readiness for change, change efficacy and workforce agility were found to alleviate the change fatigue to some extent.
Conclusions:
It is urgent and challenging for nursing managers to manage change fatigue. All of these identified predictors in study significantly contribute to the understanding of change fatigue among nurses and can provide valuable insights for health policies aimed at improving the effectiveness of nursing changes. Furthermore, they also offer a theoretical foundation for managers to develop targeted intervention programs for preventing and mitigating the negative impact of change fatigue on nurses and organizational outcomes.
Introduction
Rapid, ongoing organizational changes present various challenges to health-care providers, necessitating the adaptation of their work models to effectively implement and sustain multiple changes in the dynamic healthcare landscape.1,2 Nurses, a key group within the healthcare system, plays an indispensable role in facilitating successful changes in nursing practice. In order to deliver safer, more efficient, and cost-effective nursing services, nurses are currently experiencing a series of change initiatives, including technological innovation, restructuring and optimization of nursing resources, nursing performance system adjustment and other related aspects.3 -6 Nurses are often required to consistently adapt to changes and juggle multiple competing agendas alongside their demanding workload, which can lead to disengagement, apathy, and change fatigue.1,7,8
Change fatigue is understood as the overwhelming feelings of stress, exhaustion and burnout fuelled by feelings of ambivalence and powerlessness associated with rapid and continuous change in the workplace. 9 Previous studies have indicated that nurses are three times more likely to experience change fatigue than other healthcare professionals.2,10 Experiencing change fatigue negatively impacts nurses’ well-being, team commitment, job satisfaction and quality of patient care, but it can also greatly affect their decision to leave their profession. 9 Furthermore, it presents an equally serious threat to the successful implementation of organizational change.1,11 -13 However, the adverse effects of change fatigue on individuals or organizations are frequently overlooked. 13 Thus, investigating and comprehending the phenomenon of change fatigue and its influencing factors in nurses is critical to successfully managing change in healthcare organizations. Nevertheless, due to the novelty of this concept in the nursing field, there is a scarcity of relevant studies conducted on nurses, despite recent studies increasingly emphasizing the critical need to address change fatigue management.2,12,13 Therefore, drawing from the Social Ecological Model, we conducted a cross-sectional study to identify the change fatigue levels among clinical nurses in public hospitals and explore the possible influencing factors.
The Social Ecological Model is a framework that is widely used in occupational mental health that offers a multi-level explanation for the negative consequences of work.14,15 Given the multi-dimensional nature of factors influencing change fatigue, we consider these factors can be categorized into personal characteristics (e.g. gender, age, education level, professional title, etc.), individual level (e.g. readiness for change, workforce agility, felt obligation for constructive change and change efficacy), interpersonal networks (e.g. the communication, delivery and support of change information, etc.), organization level (e.g. characteristics of change, distributed leadership, organizational inclusive climate), community (different departments in hospital) and public policy (Figure 1). Considering that the extensive and profound influence of policies, certain difficulties exist in the assessment criteria and data acquisition. Moreover, the implementation of the policy varies among different hospitals. When evaluating the policy, it is highly challenging for nurses to undertake comprehensive and direct evaluations of the policy process and outcomes, especially those long-term and unquantifiable impacts. Consequently, we did not conduct an assessment from the policy perspective. 15 We hypothesized that high level of distributed leadership, inclusive climate, readiness for change, workforce agility, obligation for constructive change and change efficacy are crucial factors in mitigating the experience of change fatigue among nurses.
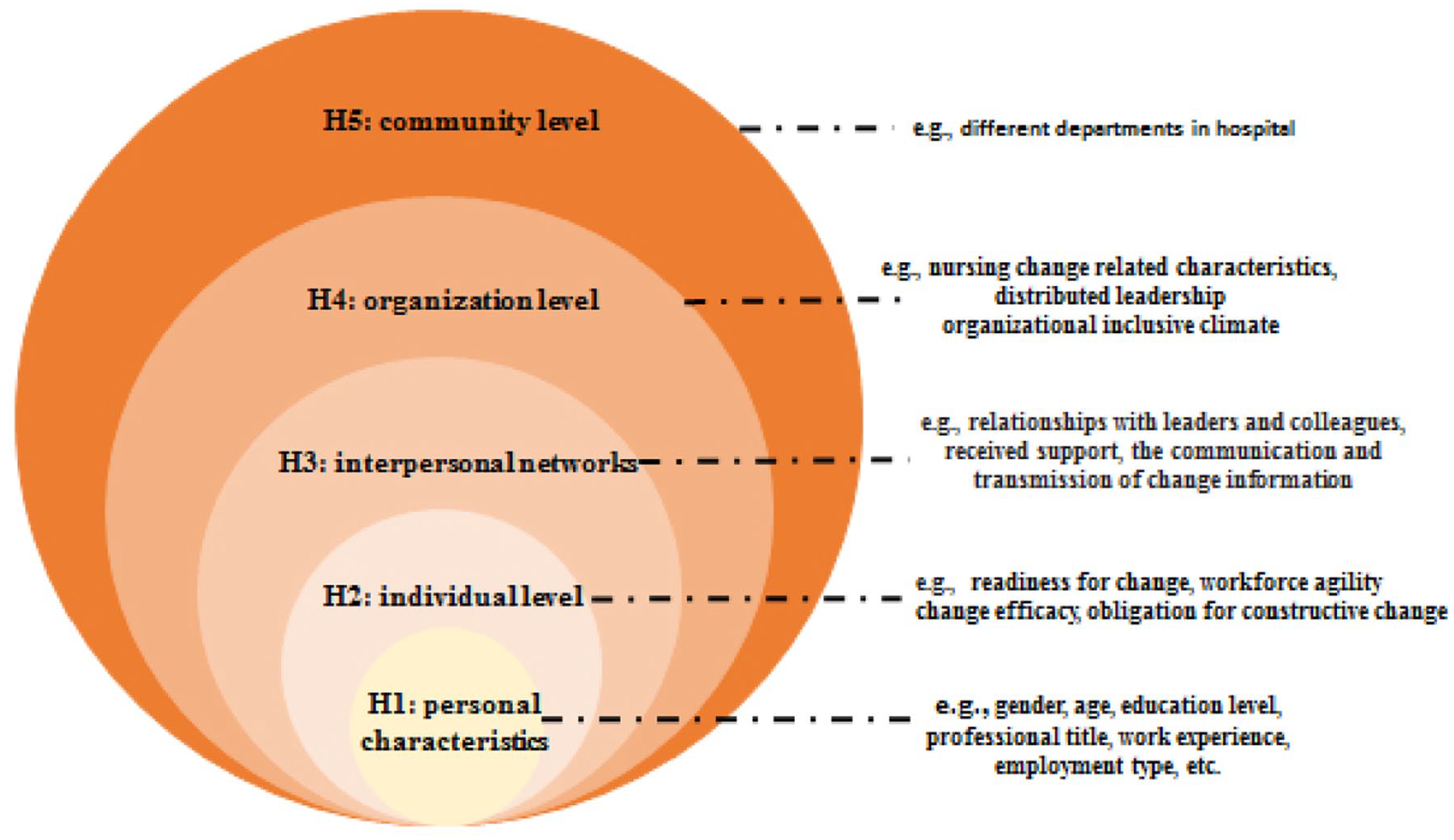
Hypotheses based on ecological model.
Methods
Study design and aim
We conducted a multicenter, cross-sectional design to assess change fatigue in frontline nurses and its associated factors. The study was reported according to the STROBE (see Appendix S1). 16
Participants and setting
This cross-sectional survey was conducted in Jinan City, Shandong Province, China, from October to December 2023. A multi-stage sampling method was used to ensure the sample’s representativeness. 14 Stage 1: we randomly selected three districts from six administrative districts based on economic development levels. Stage 2: One tertiary hospital (>500 beds) was randomly chosen from each districts. Stage 3: Cluster sampling was conducted for nurses meeting the inclusion criteria. Registered nurses with at least 6 months of experience in any position at the three hospitals were invited to participate in the study, excluding those not directly involved in patient care, such as those on sick leave, personal leave, or engaged in study or further training.
Sample size
The sample size estimation formula was calculated in study 17 was N = [Zα/2σ / δ] 2 , taking the mean scores (standard and deviation) of change fatigue as a base according to the study by Brown et al 12 In the formula, we set the value of Zα/2 to 1.96, σ to 8.97, and δ to 0.41, and the sample size is 1849 cases. Accounting for a 10%-20% invalid response rate, the final sample size was calculated as 2034-2219 cases. Therefore, a total of 2228 nurses participated in this survey.
Measures
Demographic characteristics
Data on unit worked, gender, age, work experience, professional title, professional position, educational level, employment type, average overtime hours per day, the number of night shift per month and the number of times that the rest time less than 11 hours between two shifts per week were obtained in the study.
Nursing change related characteristics
The relevant information regarding nursing change was developed based on previous literature, comprising three components: nurses’ prior experience with change (8 items), the impact of changes in job-related factors resulting from nursing reform on nurses’ responses to change (6 items), and the effect of changes in organizational factors on their response (7 items). Each item is responded to with either “yes” or “no.”
Change frequency
Change frequency was assessed using the 3-item Change frequency Scale,18,19 each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with higher total scores reflecting more frequent changes perceived by nurses at work. The scale of Chinese version was demonstrated with good reliability. 20 The Cronbach’s α for this study was .841.
Distributed leadership
The Distributed Leadership Inventory was employed to assess nurses’ perceptions of distributed leadership.21 -23 The scale consists of 20 items across four dimensions: vision motivation, trust culture, power sharing, and practical leadership. Each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), where higher scores indicate a better level of distributed leadership. It is reported that the Cronbach’s α for total scale was .857. 24 In this study, the Cronbach’s α for the overall scale was .975, with dimension-specific α values of .911, .914, .923, and .892, respectively.
Inclusive climate
The Inclusive Climate Scale comprises 15 items across three dimensions: policy fairness, difference integration, and decision-making fairness.25,26 Each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with higher scores reflecting a more inclusive organizational climate. The Cronbach’s α for Chinese version of the scale in previous study was .91. 27 In our study, the Cronbach’s α for the overall scale was .964, with subscale α values ranging from .891 to .916.
Readiness for change
The Readiness for Change Scale contains 12 items across four subscales: intention preparation, emotional preparation, cognitive preparation, and ability preparation.28,29 Each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). It is reported that the Cronbach’s α for total scale was .854. 30 In this study, the overall Cronbach’s α was .954, with subscale α values of .887, .849, .862, and .845, respectively.
Workforce agility
Workforce agility is conceptualized as the nurses’ ability to adapt to unexpected changes and to operate effectively under stressful conditions in a dynamic environment, and to adapt to new work demands. 31 We used the Workforce Agility Scale to gauge the ability to respond quickly and flexibly to task changes among nurses, and it have achieved excellent reliability and validity in nurses. 32 This scale consists of 25 items, which divided into three categories: proactivity, adaptability, and resilience. Each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with higher scores indicating higher nurses’ agility and vice versa. In this study, the overall Cronbach’s α was .956, with subscale α values ranging from .871 to .913.
Felt obligation for constructive change
In order to measure the willingness of nurses to take responsibility and obligation for organizational change and development, a five-item scale adopted from Liang et al 33 was used. Respondents rated a five-item scale on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). It is reported that the Cronbach’s α for total scale was .817. 34 The Cronbach’ α as .807 in the current study.
Change efficacy
The study adopted a four-item scale to evaluate nurses’ belief in their ability to achieve change goals and complete work tasks. 35 Each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), which higher scores indicate greater change-related self-efficacy. The scale was demonstrated with good reliability in previous study. 36 The Cronbach’ α as .954 in the current study.
Change fatigue
Change fatigue was assessed using the six-item Change Fatigue Measurement Scale (CFMS), 37 which has been validated and found reliable in nursing settings.1,12 Each item is rated on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree), which higher total score indicate greater change fatigue. In this study, the Cronbach’s α was .921.
Data collection
The survey was administered through Wen Juan Xing (www.wjx.cn), an electronic data collection tool. Firstly, we prepared an electronic questionnaire accompanied by informed consent. To ensure the questionnaire’s completeness, all items were made mandatory, while each IP address was restricted to a single response in order to prevent duplicate submissions. Prior to conducting the survey, an investigator was assigned to each hospital and underwent comprehensive training on the key concepts and guidelines involved, enabling them to provide accurate and consistent explanations. During the investigation, the QR code link was disseminated to nurses via the WeChat platform, with participation in filling it out being entirely voluntary. Before accessing the formal response interface, participants were required to sign an informed consent document. The completion of the questionnaire typically took between 10-15 minutes. To ensure data quality, we made a decision to exclude questionnaires that were completed in less than 5 minutes or more than 20 minutes, as well as those that exhibited regular patterns of response on either scale.38,39 These measures resulted in 2,228 nurses participating in the survey, with 2,029 valid questionnaires used for data analysis, achieving an effective response rate of 91.06%.
Ethical consideration
Research Ethics Committee approval for the study was obtained by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital. To ensure that participants are fully informed and willing to participate transparency, informed consent was set before the questionnaire to inform the attributes, purpose, benefits, and significance of the study. Confidentiality was guaranteed in the study by the anonymized data and the only use of the data for research purpose.
Statistical analysis
Data analysis was performed using SPSS 25.0 (SPSS Inc., Chicago, IL, USA) with a significance threshold of 0.05. The Kolmogorov-Smirnov test and the normal Q-Q plot were used to assess the normality of continuous variables.6,40 Continuous data were assumed to be approximately normally distributed. Descriptive statistics including mean, standard deviation (SD), frequencies and percentages were used for analysis the demographic characteristics, change related information, and main variables. The difference in total fatigue score variation between subgroups was examined using either independent sample t-test, one-way ANOVA, or Chi-square test. We then used the change fatigue score as the dependent variable, including statistically significant factors from the univariate analysis in a stepwise multiple linear regression to identify predictors. Additionally, Harman’s single-factor test was conducted via exploratory factor analysis to check for common method biases (CMB). Reliability was assessed using Cronbach’s α, with statistical significance set at P < .05.
Results
Participants’ characteristics and change fatigue
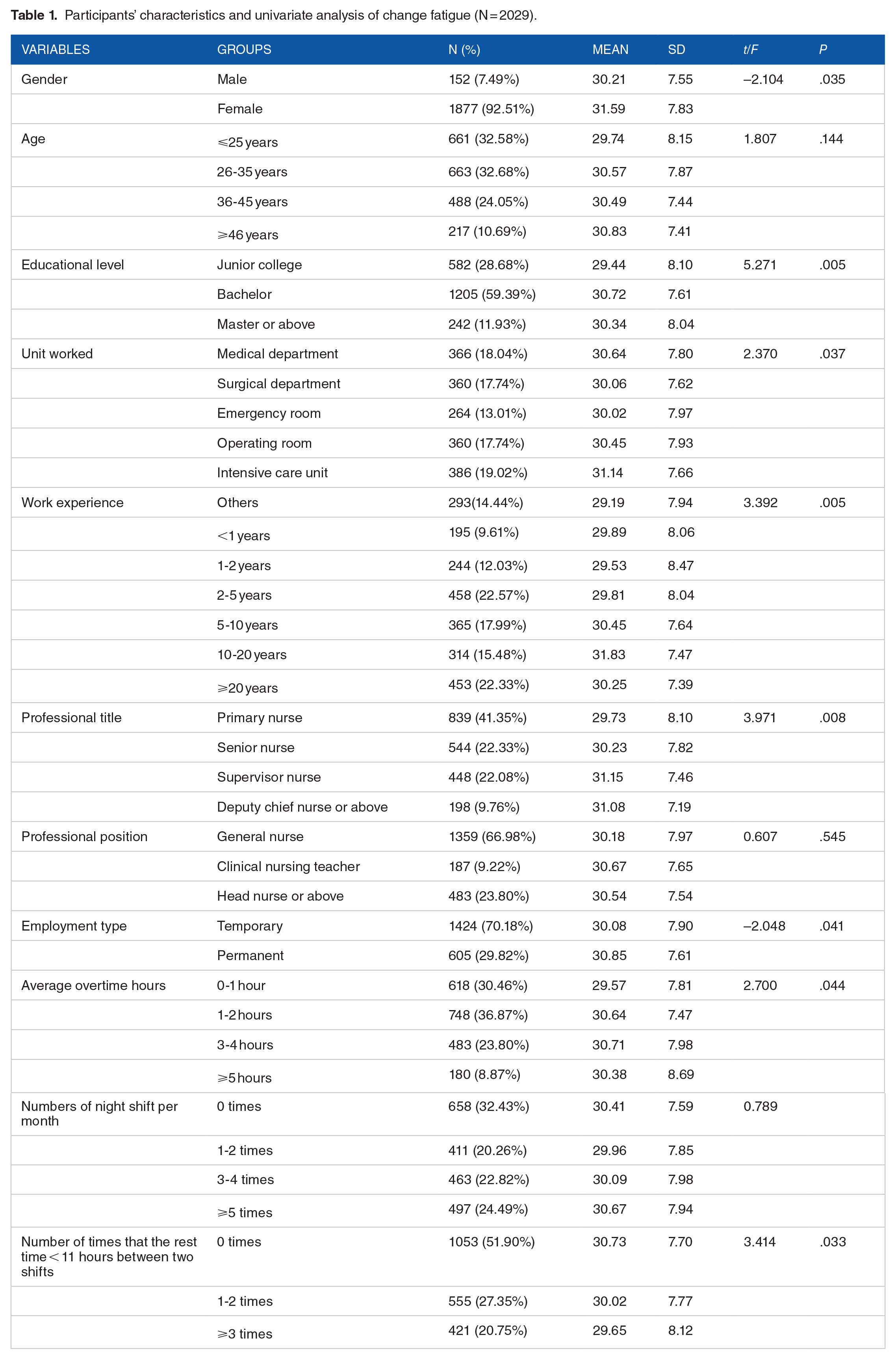
A total of 2029 nurses from three hospitals were enrolled in the study. The participants’ characteristics are presented in Table 1. Most of them were females (92.51%), less than 35 years of age (65.26%), and 71.32% of respondents had received at least a college education. One thousand and thirty-two nurses (55.79%) had worked for more than 5 years, and more than 66.98% were general nurse. The majority of the participants (70.18%) were contract nurse, and primary nurses accounted for 41.35% in terms of professional titles. Most nurses (69.54%) worked overtime more than 1 hours per day, and nearly half of them reported working over 3-night shifts per month. Furthermore, 48.10% of the nurses stated that they experienced the rest periods between two shifts lasting less than 11 hours at least once a week. All variables except age and professional position showed statistical significance using independent t-tests and ANOVA to compare means.
Participants’ characteristics and univariate analysis of change fatigue (N = 2029).
Nursing change related characteristics and change fatigue
The nursing change related characteristics are presented in Table 2. Regarding the experience of change, the main changes experienced by nurses were the reformation of salary system (36.62%), changes in service concept system (35.93%) and the introduction of new technologies (35.88%). The majority of nurses identified income (67.47%), workload (62.74%), and work-related stress (54.56%) as the main job-related factors affecting their change response. As for the organizational factors, most nurses considered that the duration (66.58%), climate (65.89%) and the communication and transmission of change information (64.46%). Univariate analysis found that the level of change fatigue was significantly associated with workflow changes, introduction of new technologies, major personnel changes, workload, work content changes, working pressure, goals of change, duration of change, the support with resources for change and the communication of change information.
Nursing change related information and univariate analysis of change fatigue (N = 2029).

Change fatigue and related variables
The overall score of change fatigue was 30.31 (SD = 7.82). Scores of distributed leadership were 70.53 (SD = 18.95). The highest subscale score was for power sharing (Mean = 21.05, SD = 5.84), followed by vision motivation (mean = 17.73, SD = 4.93), trust culture (Mean = 17.69, SD = 4.95), and while the subscale of the Practical leadership scored the lowest (Mean =14.07, SD = 3.99). Scores of inclusive climate were as follows: policy fairness (Mean = 17.21, SD = 4.87), difference integration (Mean = 21.05, SD = 5.76) and decision-making compatibility (Mean = 14.14, SD = 3.96). The participants exhibited a moderate level of change-efficacy (Mean = 13.93, SD = 3.84). The mean scores for proactivity, adaptability and resilience were 17.46 (SD = 4.67), 28.75 (SD = 7.19) and 31.27 (SD = 7.83) respectively. Scores of the change frequency (Mean = 10.23, SD = 2.99), the readiness for change (Mean = 41.99, SD = 10.94), and the obligation for constructive change (Mean = 17.37, SD = 4.08) were both at a moderate level (Table 3).
Descriptive statistics of change fatigue and related variables.

Influencing factors for change fatigue
A stepwise multiple linear regression was conducted to identify predictors of nurse change fatigue based on social-ecological systems theory. Figure 2 reports the results. In terms of demographic characteristics, female (β = .041, P < .05), professional title (β = .138, P < .01), and average overtime hours (β = .050, P < .05) were found to positively predict change fatigue. Similarly, in relation to nursing-specific change factors, workflow changes (β = .060, P < .01), workload increase (β = .058, P < .01), work-content changes (β = .056, P < .01), increased working pressure (β = .053, P < .01), and implementation of new technologies (β = .070, P < .01) were positive to change fatigue, while the support with resources for change (β = −.055, P < .01) and communication about change information (β = −.037, P < .05) were negative to change fatigue. Besides, change frequency may also be influential (β = .085, P < .01). What’s more, better distributed leadership (β = −.151, P < .01), inclusive climate (β = −.156, P < .01), readiness for change (β = −.060, P < .05), change-efficacy (β = −.147, P < .01) and agility (β = −.177, P < .01) could alleviate the change fatigue of nurses to some extent. The model was statistically significant (F = 56.858, P < .001) and explained 30.6% (adjusted R2) of the variance in change fatigue.

Hierarchical multiple regression analysis of the factors associated with change fatigue.
Discussions
This study explored the levels of change fatigue among clinical nurses and identify the potential contributing factors. Overall, the average change fatigue score of nurses was found to be at a medium to high level in our study. Factors such as female, professional title, average overtime hours, workflow changes, workload increase, work-content changes, work pressure increases, new technology implementation and the change frequency were all identified as exacerbating nurses’ experience of fatigue related to change. Contrary to this, the support of change resources, communication and transmission of change information, distributed leadership, inclusive climate, readiness for change, change efficacy and workforce agility were found to alleviate the change fatigue to some extent.
Specifically, the composite score of the change fatigue was 30.31 (SD = 7.82), which was above the mid-point, suggesting moderate to high levels of fatigue, basically consistent with early studies, 13 but higher than those reported by Brown et al 12 and Brown et al 41 Out of the 6 items, item that achieved the highest score was ‘I have made numerous sacrifices in response to a lot of change initiatives’ (Mean = 7.61, SD = 2.39), subsequently ‘I feel utterly exhausted by the rapid and continuous change initiatives’ (Mean = 7.56, SD = 1.17). This implies that nurses who have undergone change initiatives in their work often experience a certain level of fatigue. However, in such a rapidly and continuously changing environment, the change fatigue is easily overlooked by managers.2,5,6 Therefore, it is crucial to explore and understand the phenomenon of change fatigue. Nursing managers should focus on assessing change fatigue and thoroughly understanding its characteristics from the nurses’ perspective, including the timing of occurrence, severity level, duration, and influencing factors, so as to develop targeted intervention measures to reduce its occurrence.
Previous studies have identified several demographic factors that contribute to the occurrence of change fatigue.12,13,42 Accordingly, our study found that female participants were more prone to fatigue than their male counterparts. The finding has been inconsistently confirmed in studies.12,13 In comparison with men, women not only experience higher levels of work-related stress but also confront greater challenges in balancing their professional responsibilities with familial obligations, and they have to repeatedly sacrifice extra time and energy to cope with the change task, which leads them to feel the overwhelming stress, exhaustion, and burnout.11,14,43,44 The present study also verified a positive association between professional title and change fatigue, indicating that nurses with higher professional titles experience stronger feelings of change fatigue, which contrasts with the results reported by Ead 42 and Camilleri et al 13 This finding may be attributed to the fact that nurses holding high professional titles are often assigned additional responsibilities and tasks due to their strong working ability. 45 However, the process of organizational change is inevitably accompanied by an upsurge in workload and an expansion in the scope of responsibilities, which may lead to work-related stress and fatigue among nurses.1,7 Therefore, the finding imply that managers should allocate greater attention to the change fatigue experienced by nurses holding high professional titles. Furthermore, we also found that overtime hours positively predicted change fatigue, which is in line with previous studies.7,46,47 In times of rapid and continuous change, the intensification of care work, including longer hours and a faster pace, is particularly pronounced,48,49 and its negative impact on nurses is very worrying. Thus, the effective management of nurses’ workload and working hours is essential for ensuring their occupational health.
The work characteristic factors identified in the final model that may exacerbate nurses’ change fatigue are workflow changes, workload increase, work content changes, increased working pressure and the introduction of new technologies. Conversely, support with resources for change, timely communication and transmission about change information can effectively alleviate fatigue. These findings have been consistently confirmed in studies.2,50,51 The ongoing changes challenge nurses’ adaptability and coping mechanisms, making them susceptible to change fatigue.1,12,42,52 However, the effective support and communication can help alleviate this phenomenon, as evidenced in our study. Therefore, it is essential for managers to proactively establish a two-way communication mechanism during periods of change. Prior to the implementation of any change initiative, it is crucial to clearly communicate the purpose, goals, approach and benefit of the change, while also actively listening to the needs and suggestions of nurses, and provide timely feedback and support to help nurses cope with the difficulties, pressure and fatigue related change.
The findings of our study indicated that the frequency of change was a positive predictor of change fatigue, which was similar to reported in previous studies.11,53 -55 Frequent organizational changes will have a lasting impact on the original work process and tasks, leading employees to effectively cope with the uncertainty and changing needs.1,13,56 This indicates the importance for managers to reasonably grasp the frequency of changes and provide nurses sufficient recovery period after each change. On the other hand, when nurses experience inevitable frequent changes, managers should pay more attention to assess nurses’ change fatigue.
This study also provides strong evidence from organizational level that distributed leadership and inclusive climate can alleviate change fatigue. It is evident that leadership style and organizational culture are likely to serve as the pivotal factors in mitigating the adverse experiences encountered by nurses as a result of organizational changes. 1 In terms of leadership style, some researchers have indicated that encouraging nurses to jointly participate in management can effectively mitigate change fatigue.1,2,57 Distributed leadership precisely differs from other forms in that it emphasizes leadership as a practice centered on the role of nurses in driving change and offers significant benefits in terms of power sharing, hands-on leadership and shared decision making. 21 This leadership offers a platform and opportunity for nurses to actively engage in nursing development planning, reform initiatives, and decision-making processes, effectively increasing their willingness and satisfaction to engage in the change process and reducing change fatigue. As for the aspect of organizational climate, several researchers suggested that establishing a work environment featuring respect, support, and inclusiveness can effectively deal with the uncertainty of change, enhance nurses’ positive attitudes in responding to change, and alleviate their change fatigue.26,57,58 Inclusive climate reflects the working environment of fairness, equality, safety, and transparency, enabling employees to share their views and opinions as insiders and be valued and appreciated.5,26,59,60 Therefore, the inclusive climate can serve as a valuable work resource to alleviate resistance and fatigue related to change. In conclusion, it is essential for managers to demonstrate respect and acceptance towards the diverse abilities and needs of nurses, remain open to potential changes in the process, acknowledge the pivotal role of nurses as change leaders, fully empower them, and encourage their active leadership and participation in decision-making. This will ultimately enhance nurses’ psychological security and work engagement while reducing change-related fatigue.
According to the findings of this study, the readiness for change and change efficacy are significant negative predictors of change fatigue at the individual level. This suggests that nurses who more prepared for change and the stronger self-efficacy they have, the weaker the experience of change fatigue. According to previous research, the readiness for change is the key to successful organizational change.20,35,61 Adequate readiness for change enhances employees’ perception of their ability to navigate change. 28 When nurses are fully prepared for the changes, they are more likely to actively participate and contribute their ideas and suggestions. Meanwhile, some researchers have pointed out that nurses with a higher sense of change efficacy can adopt a positive attitude, better exert their subjective role in change work, increase their job participation and satisfaction, and reduce negative experiences related to change, such as change fatigue. 62 Therefore, prior to implementing the change, managers should strengthen the publicity of the change, establish effective communication channels, and implement incentive policies to stimulate the nurses’ intention to prepare for it. Additionally, there should be a focus on strengthening personnel training and capacity building so that nurses can gain confidence in adapting to changes through acquiring new knowledge, thereby reducing uncertainty and fatigue caused by the changes.
As anticipated, our findings reveal that workforce agility plays a crucial role in alleviating change fatigue. It indicates that nurses with high agility tend to exhibit positive emotional tendencies and are more inclined to accept, acknowledge, and engage with change, consequently, they are often comfortable with changes and less susceptible to negative emotions and fatigue associated with them.35,63 -65 To our knowledge, no previous studies have examined the relationship between workforce agility and change fatigue, so our results have an important theoretical contribution. Agility refers to an organization’s capacity to quickly sense and respond to environmental changes, an agile workforce offers numerous benefits to both the organization and its employees. 63 Not only is it critical to an organizations ability to survive in current hypercompetitive environments,63,66 but it also has the potential to enhance employee well-being, job satisfaction, and performance factors, which can effectively help alleviate stress and burnout caused by change. 63 Therefore, nursing managers should pay attention to the assessment and development of employees’ agility. First and foremost, they can utilize the measurement scale to identify the nurse group with high agility, who can serve as leaders and catalysts for implementing change practices. When delegating change tasks, it is advisable to prioritize them critical and complex work assignments. For nurses with low agility, it is imperative to enhance their agility. Drawing on the characteristics of agility, managers can intervene across the dimensions of proactivity, adaptability, and resilience to mitigate nurses’ fatigue associated with change. To foster proactivity, managers can enhance career counseling to promote role flexibility, 67 as well as establish an inclusive and supportive work environment, and empower nurses with a sense of autonomy and control. In terms of adaptability, nursing managers should effectively communicate accurate information about the work, clarify nurses’ roles and responsibilities, and consider implementing a tailored training system to enhance the adaptability of nurses at all levels. 65 Furthermore, resilience can be enhanced through training and learning interventions, such as mindfulness training, emotional resilience therapy, and solution-focused brief therapy. 68
Limitations
The present study has several limitations which should be taken into account. Firstly, the data we collected for testing our hypotheses was limited to Jinan City in China, which may restrict the generalizability of our findings due to geographical constraints. Secondly, our cross-sectional study design enables the identification of associations between variables but does not establish causal relationships. Future longitudinal studies are needed to evaluate the trajectory of change fatigue and its associated factors over time. Thirdly, the reliance on self-report measures may introduce reporting or recall bias. Additionally, we failed to find a targeted measurement for nurses’ change fatigue. Considering the time required for developing and validating a new scale, we decided to use the CFS, a universal scale suitable for assessing change fatigue in diverse populations. However, this decision may restrict researchers’ comprehensive understanding of change fatigue among nurses. Thus, developing an effective tool to assess nurses' change fatigue is essential. Finally, as a relatively new concept in the field of nursing, there have been few studies exploring the influencing factors of nurses’ change fatigue from both organizational and individual levels based on theoretical frameworks. It is therefore difficult to compare the results of this study with previous findings. Nevertheless, we believe that these findings provide valuable insights into understanding nurses’ change fatigue and also give valuable insights for health policies aimed at improving the effectiveness of change in nursing, as well as offering a theoretical basis to assist nursing managers in developing targeted interventions to mitigate change fatigue.
Conclusions
Based on the framework of Ecological Model, this study identified multidimensional factors predicting change fatigue among nurses through hierarchical regression analysis. Factors such as female, professional title, average overtime hours, workflow changes, workload increase, work-content changes, work pressure increases, new technology implementation and the change frequency were all identified as exacerbating nurses’ experience of change fatigue. Contrary to this, the support of change resources, communication and transmission of change information, distributed leadership, inclusive climate, readiness for change, change efficacy and workforce agility were found to alleviate the change fatigue to some extent. For managers, the change fatigue experienced by nurses is found to be at a medium to high level, presenting urgent and challenging tasks for their management, particularly in rapid and continuous organizational change. Our findings suggest that the ecological model is useful in identifying factors that influence change fatigue. Theories or conceptual frameworks are rarely used in the design or implementation of change fatigue management interventions, it is precisely the factors identified based on the Ecological Model that can guide nursing managers in the development of targeted intervention programs to prevent and alleviate the adverse impact of change fatigue on nurses and organizational change outcomes. Higher effects could be expected if the intervention is targeted on improving distributed leadership, inclusive climate, and readiness for change, change efficacy, workforce agility, and reasonable control of the frequency of change.
Relevance to Clinical Practice
This study has several implications to clinical practice. Firstly, nursing managers should pay attention to the evaluation of change fatigue, and gain a comprehensive understanding of its characteristics from the perspective of nurses, including the timing of occurrence, severity level, duration, and impact on both work and personal life. Additionally, managers also need to proactively engage in organizational change and identify the stages of change fatigue in advance by assigning change-related tasks and monitoring processes, and take appropriate measures to reduce its occurrence. Secondly, as this study has demonstrated, managers can develop strategies aimed at alleviating change fatigue from the organizational levels. On one hand, hospital administrators can promote the implementation of distributed leadership by fostering an inclusive climate that encourages and supports nurse managers in practicing distributed leadership. For example, develop the distributed leadership training programs and evaluation criteria. On the other hand, managers should demonstrate respect for and acceptance of the diverse abilities and needs of nurses, remain receptive to potential changes in the process, recognize the critical role of nurses as leaders of change, fully empower them, and encourage their active leadership and participation in decision-making as insiders. Thirdly, managers can also enhance nurses’ readiness for change and their efficacy at the individual level to alleviate their change fatigue by strengthening the publicity of the changes, establishing effective and equal channels of communication, and implementing incentive policies. Additionally, there should be a focus on strengthening personnel training and capacity building so that nurses can gain confidence in adapting to changes through acquiring new knowledge, thereby reducing uncertainty and fatigue caused by the changes. Lastly, nursing managers should pay attention to identify the nurse group with high agility, and prioritize them critical and complex work assignments when delegating change tasks.
Supplemental Material
sj-pdf-1-his-10.1177_11786329251318586 – Supplemental material for Change Fatigue Among Clinical Nurses and Related Factors: A Cross-sectional Study in Public Hospitals
Supplemental material, sj-pdf-1-his-10.1177_11786329251318586 for Change Fatigue Among Clinical Nurses and Related Factors: A Cross-sectional Study in Public Hospitals by Meng Lv, Jing Zhai, Li Zhang, Hong Wang, Ben-Hua LI, Ting Zhang and Paulo Moreira in Health Services Insights
Footnotes
Acknowledgements
We would like to thank all the participants who showed great patience in answering the questionnaires and express our deepest gratitude to all those who gave us help and support.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contributions
Meng Lv and Ting Zhang conceived the study; Meng Lv and Jing Zhai developed the study design; all authors contributed to the data collection, data analysis and interpretation. Meng Lv drafted the manuscript; Paulo Moreira, Ph.D and Ting Zhang critically revised the manuscript; all authors read and approved the final manuscript. Meng Lv is the guarantor of this review.
Ethical consideration
Research Ethics Committee approval for the study was obtained by the Ethics Committee of The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital (No.20221104). To ensure that participants are fully informed and willing to participate transparency, informed consent was set before the questionnaire to inform the attributes, purpose, benefits, and significance of the study. Confidentiality was guaranteed in the study by the anonymized data and the only use of the data for research purpose.
Data availability
The data set used in this research is available from the corresponding author upon a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.