
Abstract
Background:
Protecting healthcare employees and preventing infection transmission are paramount concerns during epidemics. Predicting healthcare employees’ behavior regarding the use of personal protective equipment (PPE) and identifying the related effective factors can guide educational and administrative strategies and enable timely interventions during outbreaks. This study aimed to predict factors affecting the healthcare employees’ behavior in the use of PPE at Shiraz University of Medical Sciences in Iran, based on Godin et al’s model.
Methods:
This was a cross-sectional and descriptive-analytical study. After reviewing the related articles and interviewing the experts and based on the model of Godin et al. (2008), a questionnaire was developed, validated, and tested for reliability using face and content validity as well as Cronbach’s alpha. Collected data were analyzed using SPSS v.21 and modeled by Structural Equation Modeling (SEM) via SPSS v.21 and Smart PLS v.3 software.
Results:
The questionnaire was valid (CVI = 86.42, CVR = 81.71) and reliable (α = .85). The model exhibited appropriate measurement, structural, and overall fit. Beliefs about consequences, social influences, habits/past behavior, role and identity, characteristics of employees, moral norms, and beliefs about capabilities indirectly and significantly influenced behavior (P < .001). Additionally, beliefs about capabilities (P < .001), habits/past behavior (P = .001), and intention (P = .001) directly and significantly influenced PPE use behavior during epidemics.
Conclusion:
The results emphasized the necessity of targeted interventions based on the studied model constructs within healthcare organizations. By promoting positive beliefs about PPE effectiveness and encouraging appropriate intentions and behaviors, healthcare organizations can significantly improve employee’s adherence to PPE use during pandemics.
Introduction
Understanding the behaviors of health workers, such as the use of appropriate personal protective equipment (PPE), is of particular importance in preventing epidemics. 1 Epidemics such as severe acute respiratory syndrome, Middle East respiratory syndrome coronavirus, Ebola virus, and COVID-19 were a global wake-up call2,3 and significantly changed the way of dealing with these emergencies and highlighted the importance of observing preventive standards in managing these complex situations. Epidemics that occurred in recent decades seriously challenged the capacity of national health systems to deal with them and showed the importance of preventive and protective systems in controlling threats caused by biological hazards. 4 In this situation, PPE is a basic principle of the health system and allows health system employees to perform their duties properly, 5 and protect themselves from the risk of contamination. 6 PPE includes items such as surgical masks, face shields, gloves, eye protection, and gowns. Such equipment is designed to protect the user and those who are in contact with these people, as well as to prevent the public from being exposed to such diseases. Although PPE is commonly used in clinical settings, it has become an essential commodity after the recent outbreak of the Coronavirus disease (COVID-19). 7
Diseases that are transmitted through breathing in closed centers such as government offices and hospitals can be transmitted quickly and spread easily by creating gatherings and inappropriate use of PPE. Based on this and to fight the spread of epidemics, many governments made the use of PPE mandatory in government and public places. 7 In epidemic and pandemic conditions, when most healthcare employees are required to use PPE, compared to normal conditions where only trained employees use them, the performance of the health system employees is affected by the use of PPE. 8 The use of PPE by healthcare employees ensures safe performance, but at the same time, it creates physiological and psychological stress due to the restrictions applied to reduce breathing, increase body temperature, etc.9,10
In the recent COVID-19 pandemic, to increase preparedness for its prevention and control among healthcare employees, the World Health Organization (WHO) issued several guidelines and recommendations 11 to reduce the prevalence of occupational infection among patients and healthcare employees. Adherence to such instructions is influenced by people’s perceptions. Disease risk perception is a critical determinant of health behavior. 12 Behavior is an overt action that takes place consciously or unconsciously. Due to the complexities of behavior, a change in awareness will not always lead to a change in attitude, and a change in attitude will not always lead to a change in behavior, because the environment may not allow the individual to develop the behavior. 13 Since behavior is a very complex phenomenon and affected by various variables, understanding the behaviors of healthcare employees in work environments and under the influence of colleagues in preventing the spread of epidemic diseases to achieve the successful implementation of preventive measures, including the use of appropriate PPE, is required. It is necessary to use behavioral theories to explain the behavioral dimensions of healthcare employees and to make policies to reduce the incidence of human resources to diseases in the health system. One of the theories that are used in various studies to investigate behaviors in the health and treatment sectors is the theory of planned behavior (TPB). The TPB is a fully functional model that can be effective in understanding better how and why people’s behavior changes. In this model, it is assumed that people’s behavior is planned and therefore their conscious behavior is predicted.14,15 Figure 1 shows the conceptual model used in the present study to predict the behavior of employees in the use of PPE during epidemics based on the study of Godin et al. 16

The study conceptual model.
According to the TPB, intention is the best factor to predict and explain behavior; Because the more a person’s motivation to engage in the behavior, the better his/her performance. 17 Behavioral intention is determined by the 3 factors of a person’s attitude toward behavior, subjective norms, and perceived behavioral control. A person’s attitude toward behavior is influenced by behavioral beliefs and expresses his/her positive or negative feelings about performing the target behavior. Subjective norms express the social pressure perceived by the individual to perform or not perform the target behavior. People often adjust their actions based on their perceptions of what others (friends, family, colleagues, etc.) think. Their intention to accept the behavior is potentially influenced by people who have close relationships with them. 15
In many studies, the planned behavior model has been used to predict the intention and behavior of healthcare employees. For example, in the study of Ismurdijahmitra et al, 18 the results showed that 48% of healthcare employees’ intention to use PPE could be well explained by the factors of attitude, subjective norms, and perception of behavioral control. Also, the model obtained from the study of Shubayr et al 19 showed that attitude and subjective norms significantly predicted the intention to perform preventive behavior in the COVID-19 epidemic. In the study by Li et al, 20 organizational climate had a direct and significant effect on preventive behaviors from COVID-19 among college students, and the constructs of the TPB, that is, attitudes, subjective norms, and perceived behavioral control, largely mediated the relationship between organizational climate and preventive behaviors from COVID-19. In the study of Öztürk and Dilek, 21 the results showed that attitude and perceived behavioral control had a positive and significant effect on the intention to purchase complementary and alternative medicine during the COVID-19 pandemic.
The protection of health system employees and prevention of infection transmission is one of the priorities and important aspects in response to epidemics. 22 Predicting the behavior of employees in the use of PPE in the occurrence of epidemics and knowing the factors affecting it can be helpful in educational and executive planning and timely intervention in times of epidemics.
The current study, conducted at Iran, Shiraz University of Medical Sciences, aimed to predict the factors affecting Iranian healthcare employees’ behavior in using personal protective equipment (PPE) during outbreaks of epidemic diseases based on Godin et al’s model. It should be noted that Shiraz is the fifth most populous city in Iran and the capital of Fars province.
Materials and Methods
This was a cross-sectional and descriptive-analytical study carried out at Iran, Shiraz University of Medical Sciences.
Sample size
One of the important issues regarding the validity of the estimates obtained from the Structural Equation Modeling (SEM) is related to the capacity of the model to identify differences between the observed relationships and the hypothesized relationships specified in the model. Therefore, the issue of sample size is of particular importance. Initial recommendations include having 10 samples per questionnaire item or variable.23-25
In the present study, the statistical population of the research included all employees of the central headquarters of Shiraz University of Medical Sciences. Considering that the questionnaire had 42 items and taking into account the average ratio of the sample size to the number of items, as well as taking into account the drop-out samples, the number of 440 samples was determined for the study. 26
Inclusion and exclusion criteria
The inclusion criteria included having at least 5 years of work experience in Shiraz University of Medical Sciences and willingness to participate in the study. The exclusion criterion was also the unwillingness to continue cooperation with the researchers in the present study.
Questionnaire design
In the current study, firstly, a comprehensive literature review was conducted to determine the factors affecting the behavior of using PPE. The keywords searched were “personal protective equipment,” “epidemic,” and also words related to different constructs of Godin’s model. The search was performed in databases such as PubMed, Web of Science, Scopus, Science Direct, ProQuest, and Google Scholar. The results of the comprehensive literature review were provided to experts, and the initial items of the questionnaire were designed based on the model of Godin et al 16 in 9 constructs. These 9 constructs included behavior, intention, habits/past behavior, beliefs about capabilities, beliefs about the consequences of using personal protective equipment, social influences, moral norms, role and identity, and characteristics of employees.
In the next step, the questionnaire was distributed among professors and experts to check its validity and reliability. The validity of the questionnaire was evaluated through face, content, and convergent validity, and the reliability of the questionnaire was evaluated using Cronbach’s alpha. 27
Both qualitative and quantitative methods were used to determine content validity. The opinions of 12 professors and experts in the fields of Infectious Diseases, Epidemiology, Health Education, Health in Disasters and Emergencies, and Health Services Management were used to check the validity of the content qualitatively, and the ability to integrate and overlap the items was checked. Professors and experts were included in the study if they had at least 3 years of research and executive experience at Shiraz University of Medical Sciences in the fields of community education, epidemics, and the use of personal protective equipment. The exclusion criterion was their unwillingness to participate in the study. It should be mentioned that the Lawshe method was used to quantitatively determine content validity. 28 The content validity ratio (CVR) was then calculated to determine the “importance” of each item. To determine CVR, experts were asked to determine the appropriateness of each questionnaire item based on the 3-part spectrum of “essential,” “useful but not essential,” and “not necessary.” In the Lawshe method, the minimum acceptable CVR is determined based on the number of experts. The minimum value of CVR for a panel of 12 experts is 0.56, and the items whose CVR is equal to or greater than this value were accepted, and the items that did not obtain the minimum validity value were removed from the questionnaire. To calculate the content validity index (CVI), experts evaluated each item of the questionnaire based on the 3 criteria of “relevancy,” “clarity,” and “simplicity” in a 4-part scale. If the item scored above 75% in terms of “relevancy,” its “clarity” and “simplicity” were also checked. If the CVI for each item was above 0.8, the item was accepted. 29
The answers to the items were coded and scored based on a 5-point Likert scale from 1 to 5 (completely disagree, disagree, somewhat agree, agree, and completely agree).
Data collection
After calculating the sample proportions in each deputy using the stratified random sampling method proportional to the size and based on the number of employees in the different vices of the university headquarters (Deputy of Development, Deputy of Education, Deputy of Health, Deputy of International Relations, Deputy of Research and Technology, Deputy of Student Affairs, Deputy of Treatment, Deputy of Food and Drug, and Presidency Office), the number of samples in each deputy was determined. Then, in each of the mentioned deputies, the required number of samples was selected from the employees using the simple random sampling method based on their personnel numbers.
Data analysis method
One-sample Kolmogorov-Smirnov test was used to check the normality of data distribution. The significance levels (P-value) obtained for all constructs were less than .05, which indicated their non-normality. The collected data were analyzed using SPSS v.21 and modeled by Smart PLS v.3 software.
One of the characteristics of the Partial Least Squares (PLS) method is its ability to model non-normal data. To test the conceptual model of the study with Smart Pls v.3 software, required analyses were done in 3 parts: measurement model fit, structural model fit, and overall model fit. In other words, first, the correctness of the relationships in the measurement models was ensured by using reliability and validity criteria, and then the relationships in the structural models were examined and interpreted, and in the final stage, the overall fit of the study model was checked.
In this study, to evaluate convergent validity, the Average Variance Extracted (AVE) criterion was used, in which values should be greater than 0.5 so that the model has a suitable convergent validity. To evaluate divergent validity, the Fornell-Larker test and HTMT ratio were used. According to the Fornell-Larker criterion, the average amount of extracted variance of each construct that is located in the houses in the main diameter of the matrix should be greater than the shared variance between that construct and other constructs (lower and left houses of the main diameter). The obtained values in the HTMT criterion also should be less than 0.9, so that the model has good divergent validity. The fit of the measurement model was evaluated through the Construct Cross-validated Communality (CV Com) index. The values of this index (Q²) which are above 0.5 indicate the appropriate fit of the measurement model. The positive values of this criterion indicate the appropriate and acceptable quality of the measurement model, and the closer it is to +1, the measurement model will be of good quality.
In examining the structural model, the relationships between the existing variables are analyzed and the criteria of significant coefficients, t-values, coefficient of determination (R
2
), effect size (f2), and construct Cross-validated Redundancy index (Q
2
) are examined to fit the structural model. The criteria of the significant coefficients of t-values based on the value of the confidence interval indicate the appropriate fit of the structural model. Also, the coefficient of determination R
2
(R Squares) is used to connect the measurement part and the structural part and expresses the effect of an independent variable on a dependent variable. The effect size (f2) determines the intensity of the relationship between the constructs of the model. In this criterion, the values of 0.02, 0.15, and 0.35 indicate weak, medium, and strong effect sizes, respectively. The redundancy index is also used for dependent variables and determines the predictive power of the model. The fit of the overall model controls both measurement and structural parts, and Goodness of Fit (GOF), Standardized Root Mean Square Residual (SRMR), and RSM-Theta were evaluated for the fit of the overall model. The overall fit of the model is equal to
Ethical considerations
This study was approved by the Shiraz University of Medical Sciences Ethics Committee (Code: IR.SUMS.REC.1399.1268). The participants were provided with necessary explanations of the purpose of the interviews and were assured of the confidentiality of the data and the anonymity of the interviewees. They were also allowed to withdraw from the interview at any time they wished, despite the initial agreement. All the individuals who were fully aware and willing to participate in the study completed and signed a written informed consent form. Also, the STROBE checklist was completed (https://www.strobe-statement.org/checklists/).
Results
In the present study, the overall relevancy of the questionnaire was estimated at 70.8, the overall simplicity of the questionnaire was 72.9, and the overall clarity of the questionnaire was 71.57. The average content validity index (CVI) was 86.42 ± 3.13 and the average content validity ratio (CVR) of the questionnaire was 81.7 ± 11.78, which indicates the appropriate content validity of the questionnaire (Table 1).
Quantitative assessment of the content validity of the questionnaire on the use of PPE during epidemics.

Also, the value of Cronbach’s alpha coefficient to evaluate the reliability of the questionnaire was calculated as .85, which indicated the appropriate reliability of the questionnaire. Cronbach’s alpha values for different constructs of the questionnaire were also above .8, which indicated the appropriate reliability of each construct of the questionnaire.
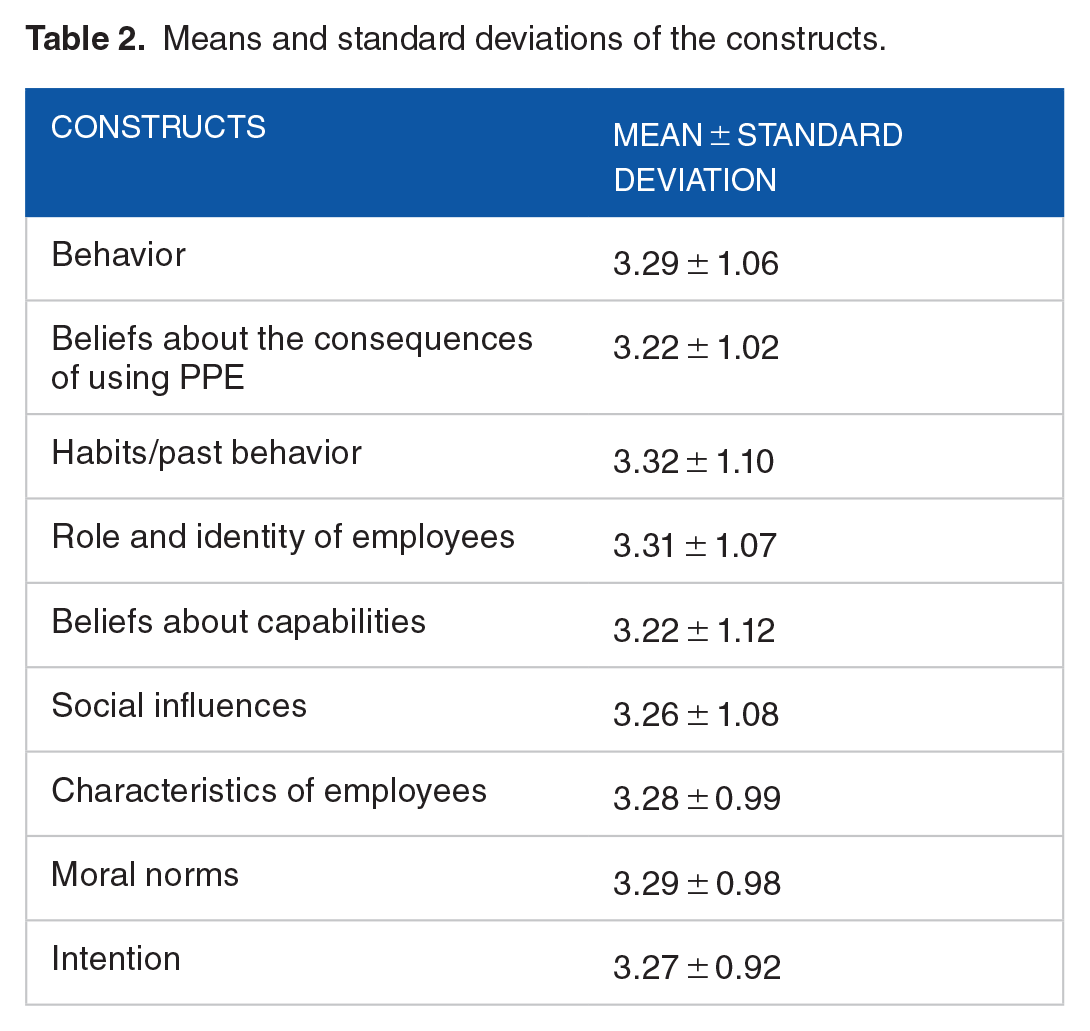
Moreover, the results showed that the highest means were related to the habits/past behavior (3.32 ± 1.10) and the role and identity of employees (3.31 ± 1.07), and the lowest ones were related to the beliefs about the consequences of using PPE (3.22 ± 1.02) and beliefs about capabilities (3.22 ± 1.12; Table 2).
Means and standard deviations of the constructs.
Measurement model fit
The measurement model fit includes checking the reliability and validity of the constructs. To check the fit of measurement models, 3 criteria of reliability, convergent validity, and divergent validity were used.
The results showed that Cronbach’s alpha for all constructs was above .7 and the Composite Reliability (CR) was above .7 (Table 3), indicating the appropriate reliability of the model.
The values of the Cronbach’s alpha, composite reliability (CR), and average variance extracted (AVE) for evaluating the reliability, and convergent validity of the model.

The factor loadings (Figure 2) also showed that the one-dimensional reliability was above 0.7 for all the items and the model had one-dimensional reliability. The obtained values of the factor loadings showed that all the items with a high level of correlation measured the variables of the study. Also, based on the results of Table 3, the Average Variance Extracted (AVE) values were greater than 0.5 and the model had a convergent validity.

Factor loadings for measuring the one-dimensional reliability of the model.
The model’s divergent validity was evaluated by the Fornell Larcker test and the HTMT ratio. Based on the Fornell-Larcker test (Table 4) and the HTMT ratio (Table 5), the model had divergent validity.
Fornell-Larker’s values to evaluate the divergent validity of the model.

HTMT ratio values for assessing the divergent validity of the model.

Based on the findings of Table 6, the values of the Construct Cross-validated Communality (CV Com) were above 0.5, indicating fit of the measurement model.
The construct cross-validated communality (CV Com) values for evaluating the fit of the measurement model.

Structural model fit
The t-values in Table 7 showed that the t-statistics at the 95% confidence interval for all constructs were above 1.96, indicating the significance of the paths and the appropriate fit of the structural model.
Direct relationships of model path coefficients.

H: The study hypotheses.
Therefore, the constructs of beliefs about the consequences, social influences, moral norms, the role and identity of employees, characteristics of employees, beliefs about capabilities, and habits/past behavior had significant relationships with intention. Also, beliefs about capabilities and habits/past behavior had significant relationships with behavior in the use of PPE during epidemics. These relationships were confirmed. Moreover, the significant relationship between intention and behavior was confirmed.
Furthermore, the results of investigating indirect relationships have been provided in Table 8, indicating that all indirect relationships had been approved and accepted.
Indirect relationships of model path coefficients.

The coefficient of determination (R2/R Square) of the structural model was 0.621 for the behavior variable and 0.489 for the intention variable. Considering that its values were between 0.33 and 0.67, the model had a structural fit.
In this study, the effect size (f2) for some constructs was above 0.35 and for some variables above 0.25. Therefore, the model had a moderate to strong structural fit (Table 9).
Effect size criterion values to determine the structural fit of the model.

It should be noted that in the present study, the values of the Construct Cross-validated Redundancy (Q2) were 0.350 for the intention and 0.355 for the behavior, indicating the predictive power of the model regarding the dependent variable and confirming the appropriate structural fit of the study model.
Overall model fit
Table 10 shows the Communalities values (Q²) of the studied constructs.
Communalities values of the constructs for the overall fit of the model.

Mean has been bolded to distinguish it from the constructs.
Also, according to Table 10, the mean of Communalities values was equal to 0.784, and considering that the value of

Given that the GOF value was above 0.35, the model had a strong overall fit. Also, in the present study, the SRMR criterion of the model (Saturated Model) was less than 0.08 and also between 0.08 and 0.1 (the Estimated Model), and therefore the model had fit.
The values related to the path coefficients in the final model of the study (Figure 3) showed that social influences (factor loading: 4.97), the role and identity of employees (factor loading: 4.88), moral norms (factor loading: 4.74), characteristics of employees (factor loading: 4.33), and beliefs about consequences (factor loading: 3.21) had predicted the changes related to intention. Beliefs about capabilities (factor loading: 4.29) and habits/past behavior (factor loading: 2.76) predicted the changes related to behavior. Also, the intention (factor loading: 2.79) had predicted the behavior of employees in using PPE during epidemics and had a significant and positive effect on it.

Values of path coefficients to evaluate the structural part of the model.
Discussion
Healthcare employees are at high risk of infection during the chain of epidemics, which is often due to their active role in controlling the situation. All over the world and especially in low and middle-income countries with limited resources and a lack of healthcare employees, it is necessary to keep them safe in the conditions of epidemics.30,31 Personal protective equipment (PPE) protects healthcare employees from pathogens by preventing them from being exposed to pathogens. Therefore, the proper use of PPE is one of the most effective strategies to protect healthcare employees against transmissible pathogens. This strategy is especially important when there is no effective treatment or prevention for a disease. 32 Using the TPB, the present study aimed to predict the factors affecting the behavior of healthcare employees of Iran, Shiraz University of Medical Sciences in the use of personal protective equipment (PPE) during epidemics based on Godin et al’s model.
The results showed that the model of the present study predicted 62% (32% through direct effects and 30% through indirect effects) of changes related to the employees’ behavior in the use of PPE during epidemics. The results of the studies by Ismurdijahmitra et al, 18 which showed that 65.1% of the health workers’ adherence to the use of PPE could be predicted using the constructs of the TPB model they had used, Shubayr et al, 19 which demonstrated that various constructs of the TPB such as attitudes and subjective norms had strong positive relationships with the dental healthcare workers’ use of personal protective equipment, and Gee et al, 33 which depicted that some TPB constructs such as subjective norm and perceived behavioral control had strong positive relationships with the workers’ use of PPE, are consistent with the results of the present study.
The results of the present study showed that intention positively affected the behavior of healthcare employees in the use of PPE, which means that the studied employees who were more familiar with epidemic diseases had better beliefs about the consequences of preventive habits and behaviors, and were more inclined to use PPE. Khaday et al 34 stated in their study that perceived behavioral control and attitude toward behavior had direct effects on the intention to follow the preventive measures, and the intention to follow preventive measures had a direct effect on the preventive behavior against COVID-19. In Blanaru’s 35 study, the results showed that employees who used PPE before the COVID-19 pandemic were more likely to agree that PPE was important and had a positive attitude toward its use. Zhang and Mu 36 also concluded in their study that people showed an optimistic attitude and intention to use PPE in order to minimize the risk of viral respiratory infections. Moreover, Johnson and Hariharan 37 showed the favorable effect of attitude and belief on the intention to use PPE. The results of these studies are in line with those of the present study.
Furthermore, the results of the current study showed that the social influences and the role and identity of employees directly predicted the changes related to the employee behavior toward the use of PPE during epidemics. The findings of the study by Trifiletti et al showed that social beliefs and influences were significant predictors of compliance with the principles of prevention in epidemics. These findings showed that behavioral intervention and strategies aimed at encouraging preventive measures during the COVID-19 pandemic had to be organized by considering several factors that were somewhat different depending on the role and position of employees and social norms in each organization. 38 In the study of Man et al, 39 the social influences of the safety climate and risk perception had a positive effect on the intention to use PPE. The results of Shwe et al’s 40 study also showed that implementing effective training programs, ensuring adequate access to protective equipment, and promoting a positive safety climate could improve adherence to safety protocols and the appropriate use of PPE. These results are similar to those of the current study.
Also, the results of the present study showed that moral norms, characteristics of employees, and beliefs about the consequences directly predicted the changes related to the behavior of employees to use PPE during epidemics. In Park and Oh’s 41 study, taking preventive behaviors against COVID-19 was indirectly associated with subjective norms, perceived behavioral control, and people’s intention. The results of the study by Gee et al 33 also showed that the 2 factors of moral norms and perceived behavioral control had a strong positive relationship with the use of PPE. Moreover, studies by Ezati Rad et al 42 and Ghobadi et al 43 indicated that the characteristics of employees had effects on their behavior. The results of these studies are consistent with those of the present study.
Finally, according to the results of the current study, strengthening factors such as social influences, role and identity of employees, moral norms, beliefs about the consequences, and habits/past behavior should be prioritized in health education for employees who need to use PPE. In this regard, health policymakers and hospital managers can significantly prevent the occurrence of diseases among employees by establishing disease prevention committees, informing about and educating about prevention behavior through the media, fostering a positive social and organizational safety culture, and defining clear safety rules and procedures.
Study limitations
Like other studies, this study had some limitations, such as its cross-sectional design, the employees’ self-reports, and predicting factors affecting the healthcare employees’ behavior only based on Godin et al’s model.
Conclusion
The model exhibited appropriate measurement, structural, and overall fit. According to the results, the constructs of Godin et al.′s model could predict 62% of the behavior and had direct and indirect significant effects on the healthcare employees’ behavior in the use of PPE during epidemics. Therefore, to encourage PPE use, especially during epidemics, policymakers and hospital managers should align organizational policies and strategies with safety goals, develop executive plans for employee safety, establish job-specific safety standards, provide adequate training, increase employees’ awareness through social media, and ensure the availability of PPE. By promoting positive beliefs about PPE effectiveness and encouraging appropriate intentions and behaviors, healthcare organizations can significantly improve employee’s adherence to PPE use during pandemics.
Footnotes
Acknowledgements
The present article was extracted from the thesis written by Saeed Ghanbari and was financially supported by Shiraz University of Medical Sciences grant No. 22791. The authors would thank all studied employees for their cooperation with the researchers in collecting the required data.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RR and PB designed the study. SGh, MAM, and ARM collected the required data. RR, ARM, and PF analyzed and interpreted the data. All authors read and approved the final manuscript.
Ethics Approval and Consent to Participate
This study was approved by the Shiraz University of Medical Sciences Ethics Committee (Code: IR.SUMS.REC.1399.1268). The participants were provided with necessary explanations of the purpose of the interviews and were assured of the confidentiality of the data and the anonymity of the interviewees. They were also allowed to withdraw from the interview at any time they wished, despite the initial agreement. All the individuals who were fully aware and willing to participate in the study completed and signed a written informed consent form.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.